
Abstract
Aims and Objectives:
Ventilator-associated pneumonia is associated with increased morbidity and mortality. The aim of this pilot study was to determine the effectiveness of oral care with both tooth brushing and 0.2 per cent chlor-hexidine gluconate compared to 0.2 per cent chlorhexidine gluconate alone for the intubated patient in an intensive care unit (ICU).
Materials and Methods:
Patient screening was done over a period of two months. After taking informed consent, those ICU patients were divided into two groups. Only nine subjects were enrolled. During the study, the experimental group (N = 4) got oral care that consisted of both tooth brushing and 0.2 per cent chlorhexidine gluconate thrice a day. The control group got oral care with 0.2 per cent chlorhexidine gluconate alone thrice a day. The data were analysed by IBM statistical software SPPS, version 24.
Results:
Preliminary results suggest that the risk of ventilator-associated pneumonia in intubated patients can be reduced by maintaining thrice-daily oral care involving both tooth brushing and 0.2 per cent chlorhexidine gluconate.
Conclusion:
Thrice-daily oral care consisted of both tooth brushing and 0.2 per cent chlorhexidine gluconate might be a promise as a ventilator-associated pneumonia-reduction strategy in ICU. Furthermore, more studies are required for its application widely.
Keywords
Introduction
It is well documented or suggested that, oral cavity serves as a harbor for nosocomial respiratory pathogens.1,2 The prevalence rate of pneumonia enormously increases the morbidity and mortality and the length and costs of hospitalizations among ICU patients. As of now, ventilator-associated pneumonia (VAP) is the second most common nosocomial disease around the world. 3 At the most specific risk for VAP are ICU patients, who have been experiencing intubation for airway management. Basically, such infection occurs in 20–25 per cent of patients treated with mechanical ventilation and is connected with a death rate of 0.5–80 per cent. 4 Present concepts clarify the incidence of emphasis upon the sources of normal floral bacteria or nosocomial bacteria that colonize in the patient from the hospital environment and then the organisms are aspirated into the lungs.5,6 However, the concepts regarding these mechanisms show strong evidences for both nasopharyngeal and gastric colonization. So, this pilot study was designed based on the oral environment as it serves itself as the foundation of bacterial colonization.
ICU patients are highly susceptible for growing colonies of more infectious pathogens found in the typical oral atmosphere of a well individual. Pneumonia might be developed by microbial organisms which are not usually inhabitants of the oropharyngeal area, but that can enter the nasopharynx by inhalation from the ICU environment.1,7 8 Usually, a major portion of VAP cases is connected with increased age, previous medical status and respiratory condition, conceded immunological systems, and trauma.9,10 In an ICU patient, the hazard of ventilator-associated infection upsurges by intubation since this affects the primary reflexes of human body to dissipate those aspirated microbes. Facts suggest a relationship between VAP and deprived oral well-being for an individual over the age of 50 years, history of smoking, congestive cardiac failure, chronic obstructive pulmonary disease (COPD), uncontrolled diabetes mellitus, history of previous antibiotic treatment, length of days in mechanical ventilations, cross-infections, immune suppression, tube feeding, gastro-oesophageal reflux syndrome, preoperative hospital stay for a long time and also lengthy surgical events.1,2,11,12 Influencing conditions including xerostomia, dryness of mucosa, condensed immunoglobin status, nutritional deprivation, unadorned stress situation, mechanical injury while intubation from nasogastric and endotracheal tubes, and the cooperated immune system allow respiratory pathogen for creating inhabitants in the oral cavity. Quick pathogenic bacterial growth with oropharyngeal mucosal grip happens in the pharyngeal mucosal area. 5 These microorganisms are colonized at first in the oropharynx and then they consequently progress into the lungs.1,13,14 It seems that oropharyngeal bacteria are the key contributors and use of active oral antimicrobial agent with tooth brushing thrice daily may minimize the risk of nosocomial pneumonia which also decrease the rates of pneumonia in ICU patients. 15 Several studies showed fluctuating success in control of decontamination of the digestive tract by using systemic and topical antibiotics 12 ; but this extensive antibiotic application increases risk factor for the patient for emerging resistant microbial stains. 16 Hospitals have executed other approaches to reduce VAP incidence likely—thoroughly washing of hand by unit staff, recurrent suctioning, early extubation and semi-Fowler’s positioning of patients. Meanwhile, up-to-date research recommends that pathogenic bacterial colonization in the oral cavity leads to pulmonary colonization.2,7 Establishing an effective oral care practice for the intubated patients feasibly gives a protected, productive and practical approach to decrease the morbidity, mortality and total cost of VAP in ICU patients.4,17
The aim of the present study was to collect initial data based on a procedure for oral care of intubated patients. The specific question addressed was: Does thrice-daily oral care of intubated patients with both manual tooth brushing and 0.2 per cent chlorhexidine gluconate reduce the VAP rate within a hospital ICU to a greater degree than the thrice-daily oral care with 0.2 per cent chlorhexidine gluconate applied by the nursing staff? The tentative hypothesis was that intubated patients who receive the thrice-daily oral hygiene care with both manual tooth brushing and 0.2 per cent chlorhexidine gluconate will experience a lower incidence of VAP equated to those who get the oral care thrice a day as analysed by clinical pulmonary infection score (CPIS) and oral hygiene index (OHI) score for total VAP rates.
Methods and Ethical Approval
We got the ethical permission from Human Research Ethics Committee, USM (HREC/JEPeM-USM) for this study (JEPeM code: USM/JEPeM/16010014). JEPeM-USM is in compliance with the Declaration of Helsinki, International Conference on Harmonisation (ICH) guidelines, Good Clinical Practice (GCP) standards, Council for International Organizations of Medical Sciences (CIOMS) guidelines, WHO standards and operational guidance for ethics review of health-related research and surveying and evaluating review practices, Electronic Institutional Review Board (E/IRB) standard operating procedures (SOPs).
Each patient with oral and nasal intubation, who entered in the ICU during the months of May and June, had an opportunity to participate in this research. Verbal and written informed consents were collected from the patients or legally authorized representatives (such as parents, husband, wife, daughter and son). As most of the ICU patients were unconscious and unable to provide informed consent for participating in this study, we chose their legally authorized representatives for providing informed consent. After admission, probable subjects were checked and screened to determine the selection and the decision was made for the participant of the study. The following characteristics were excluded from enrolment in the present study:
Patients with acute respiratory distress syndrome (ARDS) and patients having cancer chemotherapy and immunosuppressive drugs. Post-obstructive pneumonia: Patients who already developed airway obstruction and developed pneumonia. Patients with chronic pulmonary disease, chronic hepatic disorder, chronic heart disease and chronic renal disease. Oral mucositis: It may cause local irritation and hypersensitivity. Legal incarceration (e.g., organ transplantation or patients having long-term steroid therapy): They have a chance of hypersensitivity reaction. Patients who died or were discharged within 48 hours of admission in the ICU.
Sample size number depended on the number of intubated patients who entered the ICU, met the inclusion criteria and agreed to participate here during the study period. At the end of the pilot study around May–June 2016, about 9 patients (5 male and 4 female) were included in the study (N = 9), although approximately 10 more patients had fulfilled the enrolment criteria but they denied to give informed consent and participate. The age range for the subjects were from 18 years to 81 years. These nine patients were randomly allocated to either the control or the experimental treatment group by using the computer-generated software ‘Research Randomizer’. This software generates random allocation for every patient for randomization where every patient has a possibility to being a control or experimental subject. Patients who were in the experimental group (N = 4) received the oral hygiene care with both manual tooth brushing and 0.2 per cent chlorhexidine gluconate thrice daily during their intubation period. The control group (N = 5) received a standard oral care with 0.2 per cent chlorhexidine gluconate thrice daily. The study plan was to evaluate a randomized, two groups and post-test-only experimental design. The thrice-daily oral hygiene care was included as an independent variable with both manual tooth brushing and 0.2 per cent chlorhexidine gluconate (another variable) that the experimental group would receive and The thrice-daily oral hygiene care was included as an independent variable with both manual tooth brushing and 0.2 per cent chlorhexidine gluconate (another variable) that the experimental group received, and the control group received standard oral care with 0.2 per cent chlorhexidine gluconate thrice daily during their complete intubation time. The present study used thrice-daily experimental protocol because of the substantive nature of chlorhexidine and to accommodate investigator and dental surgeon efficacies. The VAP rate was the main outcome variable as it was determined by the attending medical doctor and recorded in patients’ medical charts. However, the study design and its pattern was remained intact, but the investigation was altered to a case study for the ultimate insufficient sample size. Based on the discharge of the patients, the nursing staff and principal investigator completed a demographic data sheet for each of the nine subjects who were enrolled in the study. These data were compiled to evaluate the characteristics of the participants in the sample descriptively. The ICU nursing staffs attended an educational session that was conducted by the dental researchers on the thrice-daily oral hygiene protocol, recruited case study participants at the time of admittance to the ICU, provided the thrice-daily oral hygiene care protocol with both manual brushing and chlorhexidine gluconate to the experimental group or the standard oral care protocol that the hospital already followed to the control group, and kept a record of the oral hygiene administration and adverse effects to the subjects. Every day, the principal investigator visited the ICU to monitor record-keeping and to note adverse effects. No adverse effects were found and noted. Each patient had a hospital chart where oral hygiene administration record was kept very consciously. The study equipment and materials used for the thrice-daily oral hygiene protocol included the standard oral paediatric toothbrush distributed by 1 Malaysia and 0.2 per cent chlorhexidine gluconate distributed by the ICPA Health Products Ltd. Some other materials were also used for the standard oral care protocol such as suctioning foam swab, chlorhexidine and oral lubricant. For the standard oral care protocol or a thrice-daily oral hygiene care regimen with chlorhexidine gluconate procedure, patients were requested to provide their informed consent. In the nursing care routine, there was no modification except the thrice-daily oral hygiene care thus provided to the nine intubated patients in both control and experimental groups. Both of these oral hygiene protocols were followed until day 11 for the 9 intubated patients staying in the ICU in HUSM. These intubated patients were a transient population; none of them was kept in the ICU for the entire month of the study period. For the nosocomial pneumonia, diagnosis was done by a physician and the ICU nursing staffs monitored each subject spontaneously. As the study sample size was too small, it prohibited the use of parametric statistical analysis and hypothesis testing. Hence, the descriptive statistics, in the form of frequencies, proportions and measures of central tendency, were used for this study. Demographic data were thoroughly described to the patients in the study. These played a role to verify subject groups’ equivalency and also helped to identify possible external influences that might have an association to the development of nosocomial pneumonia.
Results
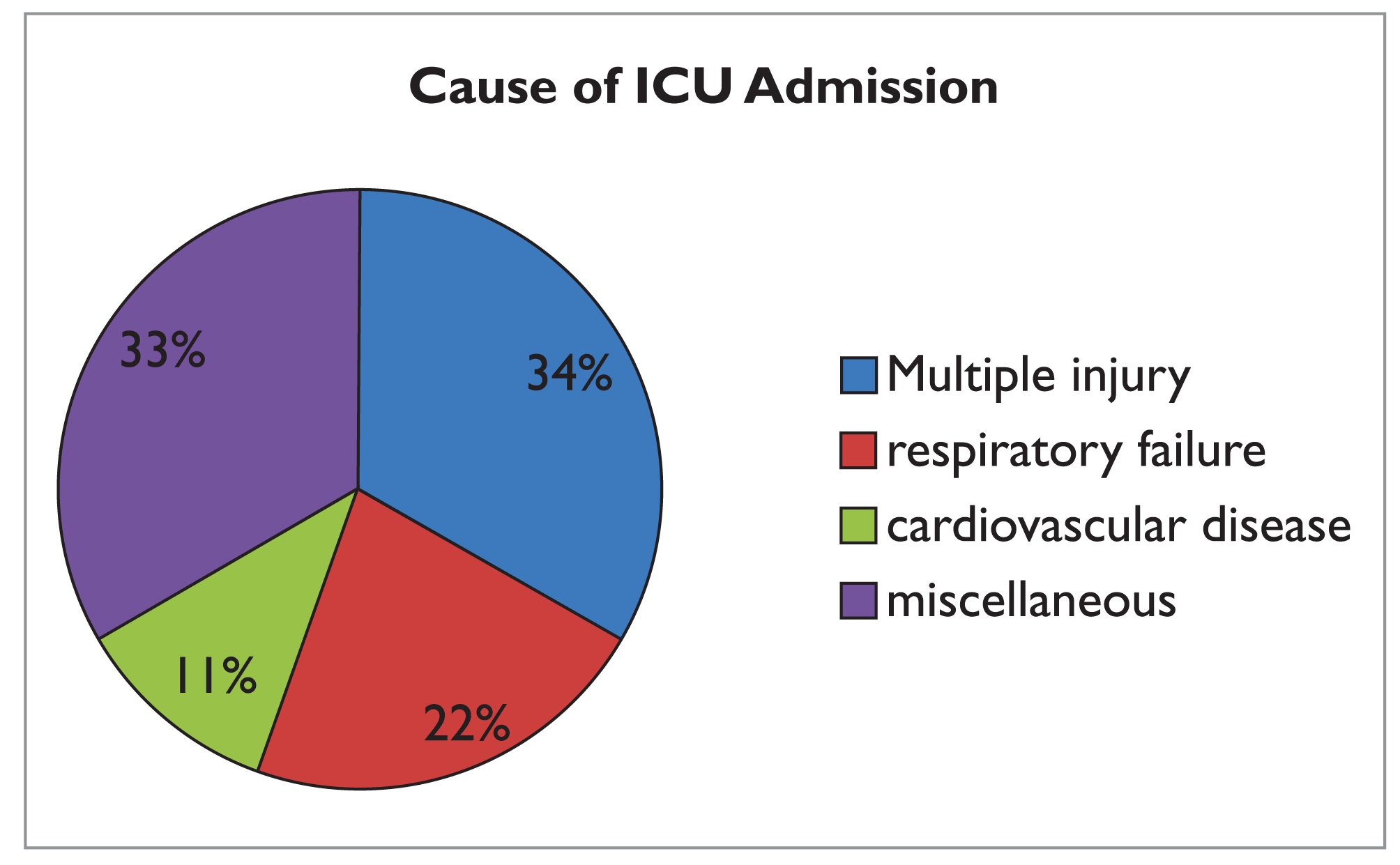
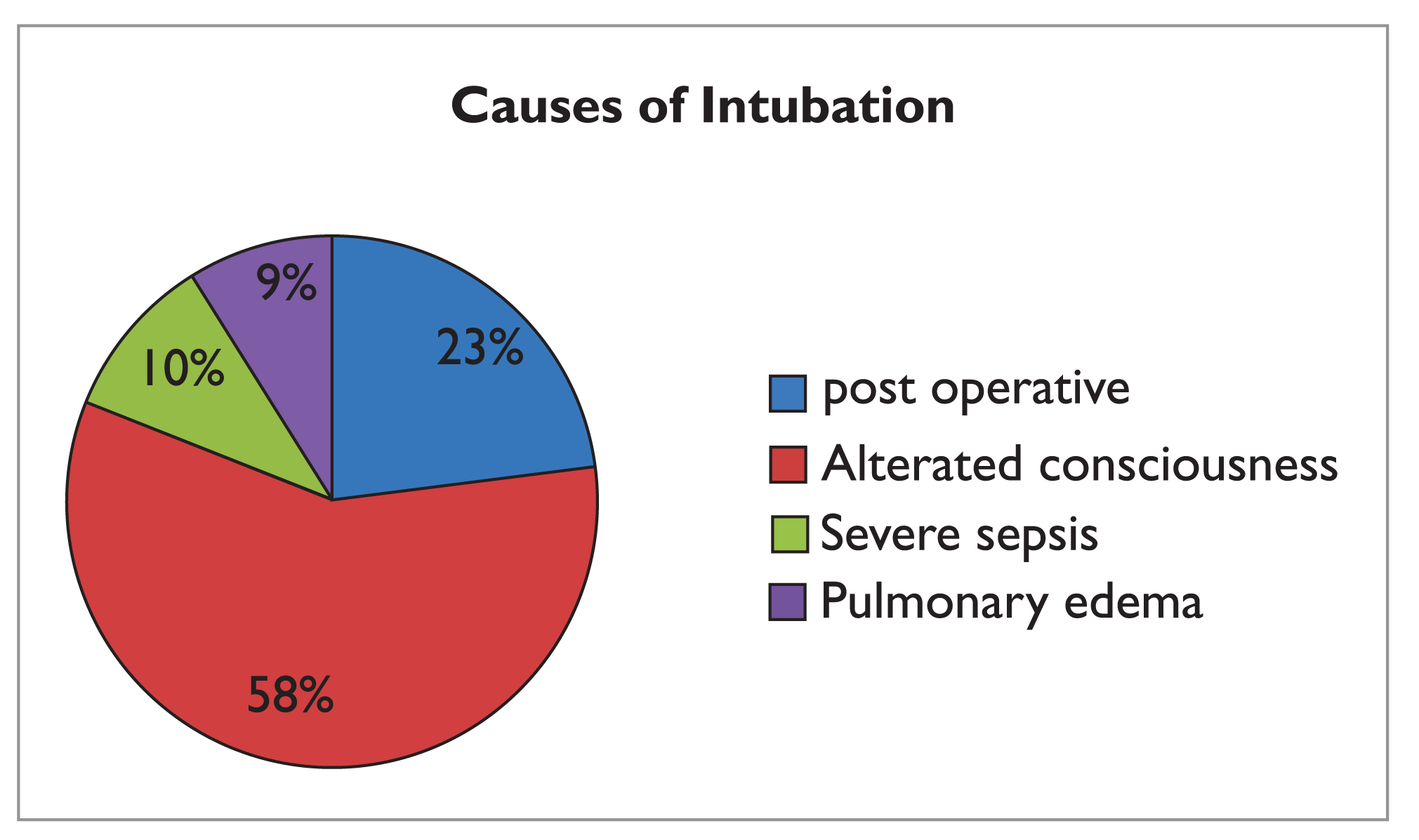
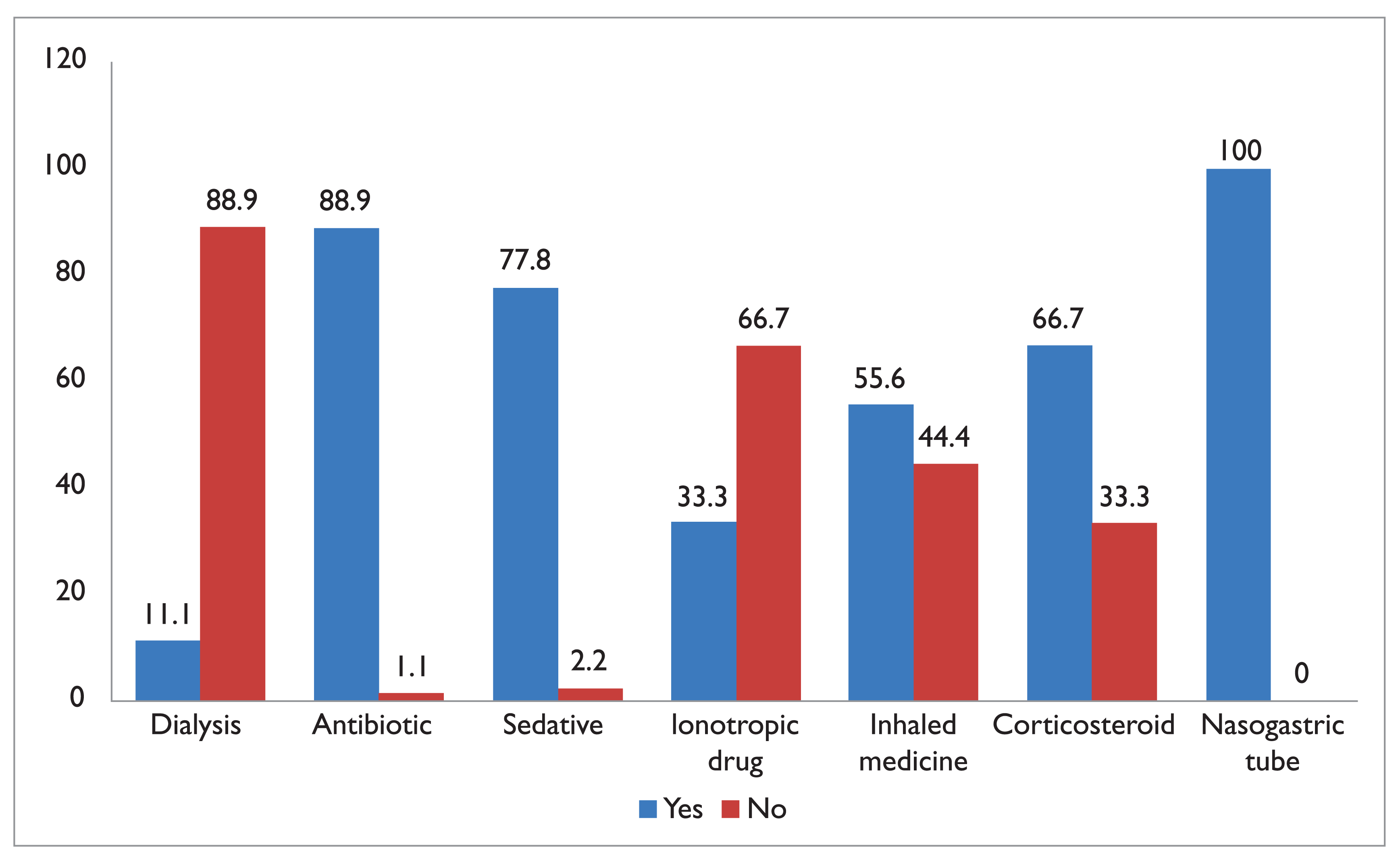
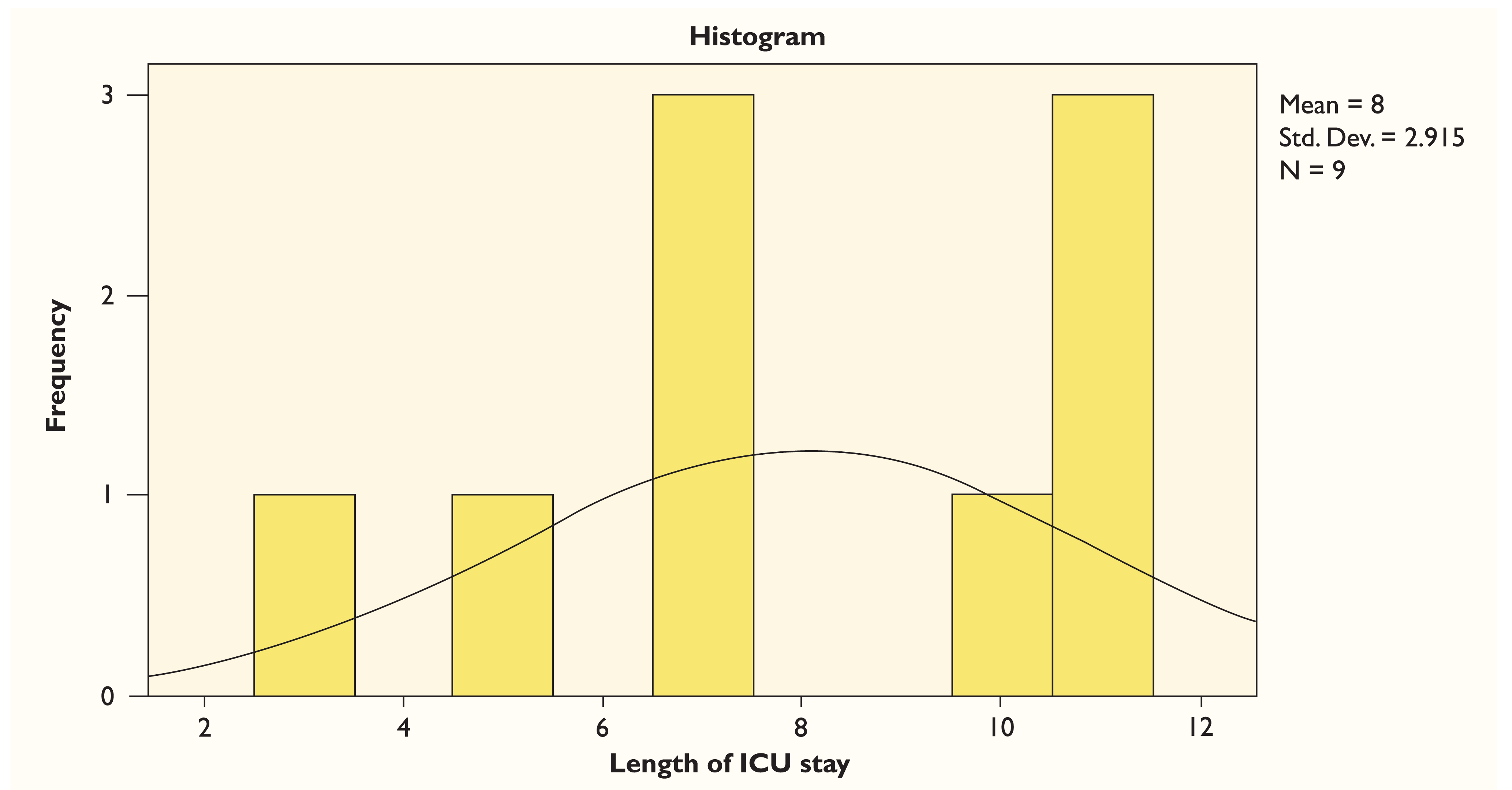
Based on the discharge of the patients from the ICU, the principle investigator completed a demographic data sheet for each of the nine subjects who were enrolled in this study. Remarkably, one of the subjects from the control group was diagnosed with VAP. In this study, males compromised 55.6 per cent and females compromised 44.4 per cent in overall (Figure 1). The mean age of the subjects was 45.67 years (Figure 2). Most of the subjects were admitted in the ICU with cause of multiple injuries and miscellaneous causes (33.3 per cent; (Figure 3). Alternated consciousness (58 per cent) was the most common cause for intubation (Figure 4). Most of the subjects were treated by antibiotics (88.9 per cent), sedatives (77.8 per cent) and with nasogastric tube support (100 per cent); (Figure 5). The number of days spent in the ICU ranged from 3 to 11, with mean length of 8 days in the ICU (Figure 6). While comparing the patient (OHI with CPIS, we found that the experimental group had lower mean score in both the scores (Table 1).
Discussion
VAP is highly related with the increased health care expenses, morbidity and mortality. Oral swabbing with chlorhexidine was effective in reducing early onset of VAP in patients staying in medical, surgical/trauma and neuroscience ICUs who did not have pneumonia at baseline. Tooth brushing did not alone reduce the incidence of VAP, and combining tooth brushing with chlorhexidine provided an additional benefit than chlorhexidine rinsing alone. This study was a randomized, controlled clinical trial which was planned to determine that the application of two oral care involvements–chlorhexidine alone and combining chlorhexidine with tooth brushing–would decrease the risk for VAP during the first week of intubation in critically ill patients receiving mechanical ventilation. The sample varied in race and included both males and females. The outcome of the present study that combines tooth brushing with chlorhexidine was beneficial on patients who had baseline CPIS values on day 3 in the ICU. Mostly, toothbrushes were observed as the best implement for mechanical oral care in healthy populations. 3 The tentative hypothesis for the present study was that the intubated subjects who received the thrice-daily oral care with tooth brushing with 0.2 per cent chlorhexidine gluconate encountered less VAP contrasted with the individuals who got the oral care with chlorhexidine only. Despite great enthusiasm among bedside nurses regarding the theorized effect of oral care on VAP reduction, few data support the effectiveness of mechanical oral care procedures. 18 More than seven days of intubation might have assumed a part in the subject getting VAP. Hixson et al. stated that the risk of VAP prolonged from 6.5 per cent in those 10 ventilated days to 28 per cent in those 30 ventilated days. 19 The patient was diagnosed with respiratory failure upon admission to the hospital, which is likewise a significant remarkable risk factor for the development of VAP. 20 The patient was in the control cluster, which did not receive tooth brushing. The control group got oral hygiene care with a foam swab and chlorhexidine gluconate, though a toothbrush is a more superior dental assistance to a foam swab. 21 The use of 0.2 per cent chlorhexidine gluconate rinsing with tooth brushing has appeared as extraordinary to diminish the bacterial colonization in dental plaque. 15 Chlorhexidine gluconate helps to decrease VAP incidence by 69 per cent. 18
Comparison of CPIS Score and OHI Score for Subject total by Independent t-test
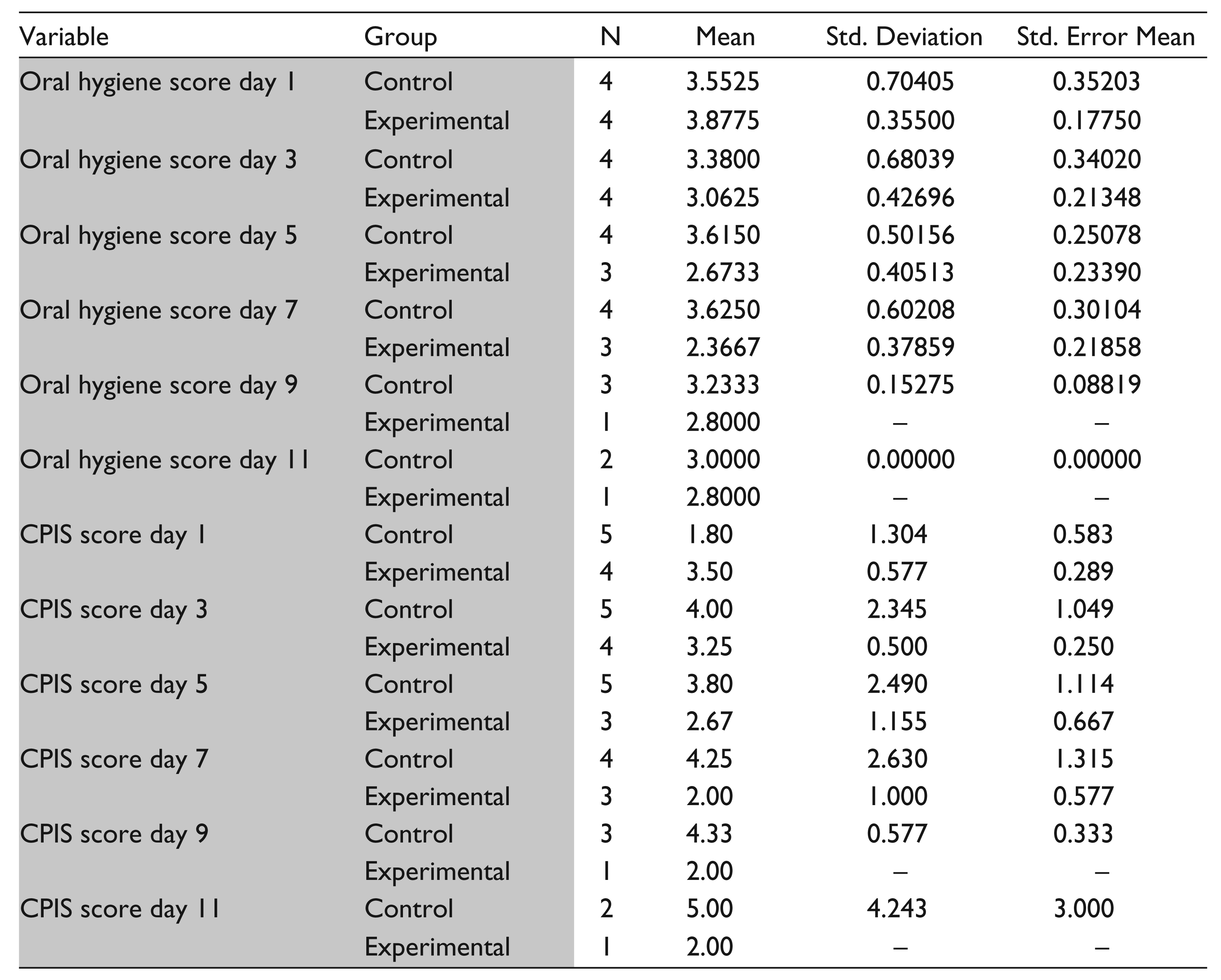
Our study revealed that the mean age of admitted patients was 45.67 years. While VAP can occur in all ages, elderly patients are especially vulnerable to it. 19 In our study, most of the subjects were admitted in the ICU because of multiple injuries and miscellaneous causes (33.3 per cent). A study on Asia-Pacific countries also got similar finding where most of the patients were in the ICU with multiple injuries, head injury and miscellaneous causes. 22 In the present study, alternated consciousness (58 per cent) was the most common reason for intubation. Barbier et al. also identified alternated consciousness as the most common reason for mechanical ventilation and prone to VAP. 23 Our study shows that most of the subjects were treated by antibiotics and sedatives. All the subjects got complete nasogastric tube support. This correlates with the study done by Goyet et al. 24 They found that most of the patients admitted in the ICU got antibiotics and sedatives along with nasogastric tube. Patient duration in ICU ranged from 3 to 11 days with mean length of 8 days in the ICU. A study conducted in Malaysia indicated that a smaller pe-riod of mechanical ventilation significantly decreases the incidence of VAP and each extra day in mechanical ventilation rises the probability of VAP development about 4 per cent. 25 In that study, the significant difference in the duration of hospital stay between VAP (+) and VAP (–) groups of patients was remarkable. The most important finding of present study is that the experimental group had a lower mean score of OHI with CPIS score. We implied tooth brushing with chlorhexidine three times to the experimental group. A study done by Murno et al. with near to similar our method finds that chlorhexidine is better than tooth brushing. 26 He stated that combining tooth brushing with chlorhexidine has no additional benefit. In our study, we got a better result because we implied tooth brushing with chlorhexidine application three times while Murno et al. implied tooth brushing alone three times with chlorhexidine two times, not combined.
Looking back, the stringent exclusionary criteria kept excessively numerous patients from meeting all requirements for the study, hindering the accomplishment of a massive sampling estimate. It was reported by the intensive care staff that the patients admitted to the hospital ICU had several and multifaceted medical conditions. The essential exclusionary criteria that kept intensive unit patients from meeting all requirements for the study was diagnosis of uncontrolled diabetes mellitus, closely followed by admission with pneumonia and subsequent intubation and patient’s legal relative denied to give consent. This pilot study shows a positive impact of combining tooth brushing with chlor-hexidine oral care on an intubated patient for reducing VAP. A full randomized clinical trial is further needed for establishment of this standard oral care for the intubated patient.
Conclusions and Recommendations
The most significant conclusion for this study with contextual analysis was that no subject got the experimental action which identified with VAP. Outcomes propose that the thrice-daily oral hygiene care of intubated subjects with 0.2 per cent chlorhexidine gluconate as well as with tooth brushing might hold potential policy in reducing VAP in ICU; nevertheless, its uses need more testing. Suggestions for upcoming studies incorporate the utilization of 0.2 per cent chlorhexidine gluconate with tooth brushing at several hospital-based spots; thus, the sample size and assorted qualities may be improved and the discoveries could be more comprehensive. Moreover, rather than enlisting the subjects from the ICU, patients might be selected in a unit or a section where patients have less multifaceted medical situations. Using a reference population with a lesser amount of overwhelming medical circumstances would increase the size of the qualified subjects and, thus, the quantity of patients enlisted in the number of subjects enrolled, creating the study more substantial and dependable. The use of a pre-procedural rinse with 0.2 per cent chlorhexidine gluconate before the placement of endotracheal tube to decrease the risk of VAP requires additional research.
Footnotes
Acknowledgements
We are thankful to USM fellowship (December, 2015/2016) for supporting Mohammad Khan for pursuing his PhD. We are also thankful to ICU staff nurses, Shamima Easmin Nishi and Miz Hazrini, for their continuous support to this project.
Declaration of Conflicting Interest
We declare that there is no conflict of interest.
Funding
None.