
Abstract
Youth and adults with muscular dystrophy (MD) face sexual and reproductive healthcare barriers shaped by the physical, social, and emotional impacts of a progressive neuromuscular condition. Despite sexual health being central to well-being, it remains understudied, as the needs of disabled individuals are often overlooked due to misconceptions and false narratives of disinterest. To address this gap, we conducted semi-structured interviews with thirty adults with various MD types, exploring their sexual and reproductive healthcare experiences. Using a hybrid inductive–deductive thematic analysis, we identified six themes related to barriers in care: patient discomfort discussing sexual health and insecurity about disability or inexperience; provider discomfort and overemphasis on medical puberty; lack of private, confidential time with providers; unaddressed fertility and reproductive concerns; provider invalidation or assumptions about sexual or romantic interest; and reliance on self-education from pornography or online sources. We also identified six themes for actionable improvements: patients desired increased provider-initiated conversations; practical sexual health information including hygiene and self-care; dating and relationship guidance; mental health support and resources to counter negative media messages; education on safe options for sexual fulfillment; and community and peer connection resources. Overall, participants expressed a strong desire for proactive, confidential, and affirming care addressing the full spectrum of sexual health needs while integrating mental health and peer support. Findings highlight the urgent need for inclusive, accessible, and holistic sexual and reproductive healthcare tailored to the lived experiences of people with MD.
Keywords
Introduction
Although sexual health is widely recognized as integral to overall well-being, it continues to be under-addressed in individuals with disabilities.1,2 The World Health Organization defines sexual health as “a state of physical, emotional, mental and social well-being in relation to sexuality.” 3 Despite this broader framework, sexual health discussions in disability care remain limited due to a variety of factors, including provider discomfort, lack of disability-specific training, and societal presuppositions. 4 These challenges are magnified in Duchenne muscular dystrophy (DMD), an X-linked recessive condition caused by mutations in the DMD gene, leading to loss of dystrophin protein and progressive muscle degeneration. Weakness begins in early childhood and continues to progress, typically resulting in the loss of ambulation before puberty, and ultimately progressing to respiratory and cardiac compromise in early adulthood. Sexual health in DMD is uniquely shaped by the effects of long-term corticosteroid therapy, which, while critical for slowing disease progression, often suppresses puberty and necessitates pubertal induction with hormone replacement therapy.5,6 As life expectancy for individuals with DMD continues to increase, through multidisciplinary management and emerging gene-targeted therapies, sexual and reproductive healthcare has become an essential component of comprehensive management in DMD.
Recent studies have begun to investigate sexual health experiences in neuromuscular conditions. In qualitative interviews with adults living with a range of neuromuscular diseases, Møller and colleagues found that participants frequently encountered societal assumptions of asexuality, limited representation of disability in sexual discourse, and reluctance among healthcare professionals to address sexuality in clinical encounters. 7 In the UK, semi-structured interviews with 20 individuals with DMD revealed aspirations comparable to those of nondisabled peers, such as marriage and family life, but also significant barriers to pursuing sexual and romantic relationships, including physical limitations, fewer opportunities for partnerships, and pervasive societal prejudices. 8 A more recent UK focus group study (n = 6) further explored men's perspectives on sexual health, testosterone treatment, and fertility, underscoring unmet needs for information, support, and individualized care. 9 Building on this work, Powell and Carlton developed a qualitative framework of health-related quality of life in DMD that emphasized autonomy, identity, and, in particular, social relationships, showing that sexual and reproductive health is inseparable from the broader lived experience. 10 Yet perspectives of adults with MD in the United States remain underexplored, despite potentially distinct barriers shaped by healthcare systems and social attitudes. In the U.S., the American Academy of Pediatrics has noted that youth with disabilities routinely receive substandard sexual and reproductive health education. 11 Our prior work showed that adolescents with DMD often miss critical opportunities for inclusive, disability-informed learning in both school and home settings. 1 Best practice calls for early, open, and ongoing communication about sexual health, tailored to developmental stage and medical needs within a multidisciplinary care framework, 12 yet little is known about how these principles align with the lived experiences of adults with MD in the United States. To address this gap, the present study extends our prior work by focusing specifically on sexual and reproductive healthcare and the relationship between patients and their medical teams. We conducted semi-structured interviews with 30 adults across the United States to explore lived experiences of sexual and reproductive healthcare and identify priorities for patient-centered, multidisciplinary care. Guided by an interpretivist approach that recognizes knowledge as socially constructed and grounded in lived experience, this study sought to answer the following questions: (1) How do adults with muscular dystrophies describe their experiences with sexual and reproductive healthcare? (2) What barriers do they identify in accessing comprehensive sexual and reproductive healthcare? and (3) How do they envision sexual and reproductive healthcare being delivered differently to better meet their needs?
Methods
Study design and sample size
We conducted a mixed-methods study with a qualitative emphasis to examine experiences of sexual and reproductive healthcare among adults with muscular dystrophies (MD). Participants contributed narrative data through either synchronous semi-structured interviews or written open-ended responses, with descriptive quantitative data collected to contextualize participant characteristics and care experiences. We recruited 30 adults (≥18 years) from clinical and community settings across the United States using purposive sampling through neuromuscular clinics and MD-focused community organizations, supplemented by convenience recruitment through online MD networks. Eligible participants were English-speaking adults with a confirmed diagnosis of any MD subtype who self-identified as having sufficient cognitive and communicative ability to participate.
Although recruitment was primarily conducted through DMD–focused channels, we included adults with other MD subtypes who expressed interest in participating. This approach aligns with prior work demonstrating overlapping healthcare barriers across neuromuscular conditions and reflects our aim to center lived experiences rather than diagnosis-specific clinical trajectories. Recruitment continued until thematic saturation was reached, defined as the point at which no substantially new codes or themes were created during ongoing analysis.
The study was approved by the Boston Children's Hospital Institutional Review Board. Informed consent was obtained verbally for interview participants and electronically for written participants.
Reflexivity
This study was developed by clinicians and researchers involved in the care of individuals with DMD and other neuromuscular conditions. Our clinical roles shape our awareness of how sexual health is often narrowly framed or omitted in neuromuscular care. We approached this work from an interpretivist perspective, recognizing experiences of disability and sexuality as socially constructed and shaped by healthcare interactions, power dynamics, and cultural norms.
To support reflexivity, the analytic team included clinicians, non-clinical researchers, and individuals with lived experience of disability. We engaged in ongoing discussion to examine how professional training, assumptions about disability and sexuality, and prior clinical experiences could influence interpretation. Analytic decisions were documented, disagreements were resolved through consensus, and participant language was prioritized in theme naming and description to center participants’ narratives rather than clinical interpretation.
Data collection
We developed a semi-structured interview guide focused on experiences with sexual and reproductive healthcare, informed by existing literature and multidisciplinary input from a clinical psychologist, a sexual health specialist, and researchers with expertise in endocrine and neuromuscular care. The guide included open-ended questions designed to support approximately one hour of engagement and was refined after the first three interviews for clarity and relevance.
All participants began with a brief demographic questionnaire (age, gender identity, MD subtype, race/ethnicity, living situation), followed by targeted prompts to establish shared language and reduce stigma around terms such as masturbation and pornography. Participants were then invited to reflect on their experiences using open-ended questions, including: “Is there anything your medical providers did not tell you about puberty or sex that you wish they had?” and “Please describe anything you wish your medical team had done differently.”
After completion of approximately six synchronous interviews, members of the MD community contacted the study team to ask whether alternative ways of engaging with the same questions could be offered for individuals with low vocal tone, fatigue, or difficulty sitting through a 45–60-min video interview. In response to this community feedback, we added an asynchronous written participation option designed to mirror the semi-structured interview as closely as possible while improving accessibility.
The written format used the same content domains, question order, and prompts as the interview guide, including demographic context, ideal sexual and reproductive healthcare, experiences with puberty, sex education, conversations with medical providers, fertility and parenthood, and recommendations for improving care. Open-ended text fields were used in place of verbal probes, allowing participants to respond in their own words and at their own pace, with the option to pause and return as needed. The intent of this format was not to replace the interview, but to function as an equivalent method for eliciting narrative responses while reducing physical and vocal demands.
Both formats were treated as complementary qualitative modalities designed to elicit comparable narrative content. Of the 30 participants, 11 participated in synchronous interviews and 19 completed the written REDCap format. We observed that synchronous interviews generally yielded longer narrative responses and allowed for probing and clarification, whereas asynchronous REDCap responses more often produced concise statements and a higher proportion of direct responses to structured prompts. The addition of the REDCap option improved accessibility by enabling participation for individuals who preferred or required an asynchronous format; however, we recognize that modality may influence the depth and elaboration of narrative detail. Interview transcripts were transcribed verbatim, de-identified, and formatted to align with the same question structure used in the written responses prior to analysis, allowing for integrated thematic analysis across modalities.
Data analysis
We conducted a reflexive thematic analysis, which is well suited to exploring lived experiences and meaning-making in under-studied populations. 13 This approach emphasizes reflexivity, transparency in analytic decision-making, and identification of patterned meaning across the dataset rather than quantification of responses. We used a hybrid, deductive-inductive analytic strategy. Deductively, analysis was organized around two a priori domains informed by prior literature and the interview structure: (1) barriers to sexual and reproductive healthcare and (2) recommendations for improving care. Inductively, we applied open coding within each domain to identify patterns of meaning emerging directly from participant narratives. Codes were iteratively refined through team discussion and grouped into candidate themes, which were reviewed and revised to ensure internal coherence and distinction between themes.
De-identified transcripts and written responses were imported into Dedoose (version 9.2.012) for data management and coding. Coding was conducted manually by the research team; no automated coding or algorithmic analytic functions were used. Transcripts were independently coded by team members with clinical backgrounds, lived experience with disability, and non-clinical research training to incorporate multiple analytic perspectives. Coding discrepancies were resolved through consensus discussion. At least two team members independently reviewed and synthesized themes.
We tracked repetition of topics within individual narratives as a descriptive indicator of salience for some participants, recognizing this as a content-analytic element; however, theme development was based on patterns of meaning across the dataset rather than frequency alone. Descriptive statistics were used to summarize participant demographics and clinical characteristics. Reporting followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 14
Results
Demographics
Participants’ mean age was 31.1 years (SD = 9.8). All were assigned male at birth; most identified with he/him pronouns (90%), with one participant each identifying with she/her and they/them, and one undisclosed. Most reported DMD (23/30, 77%), with smaller numbers reporting Becker Muscular Dystrophy (2/30, 7%) or an unspecified type (5/30, 17%). Two-thirds lived with parents (20/30, 69%). Racial/ethnic identity was predominantly White (19/30, 63%), with others identifying as Hispanic/Latino (3/30, 10%), Asian (3/30, 10%), or nondisclosed (5/30, 17%). A complete summary of demographic characteristics is provided in Table 1.
Demographic characteristics of study participants.
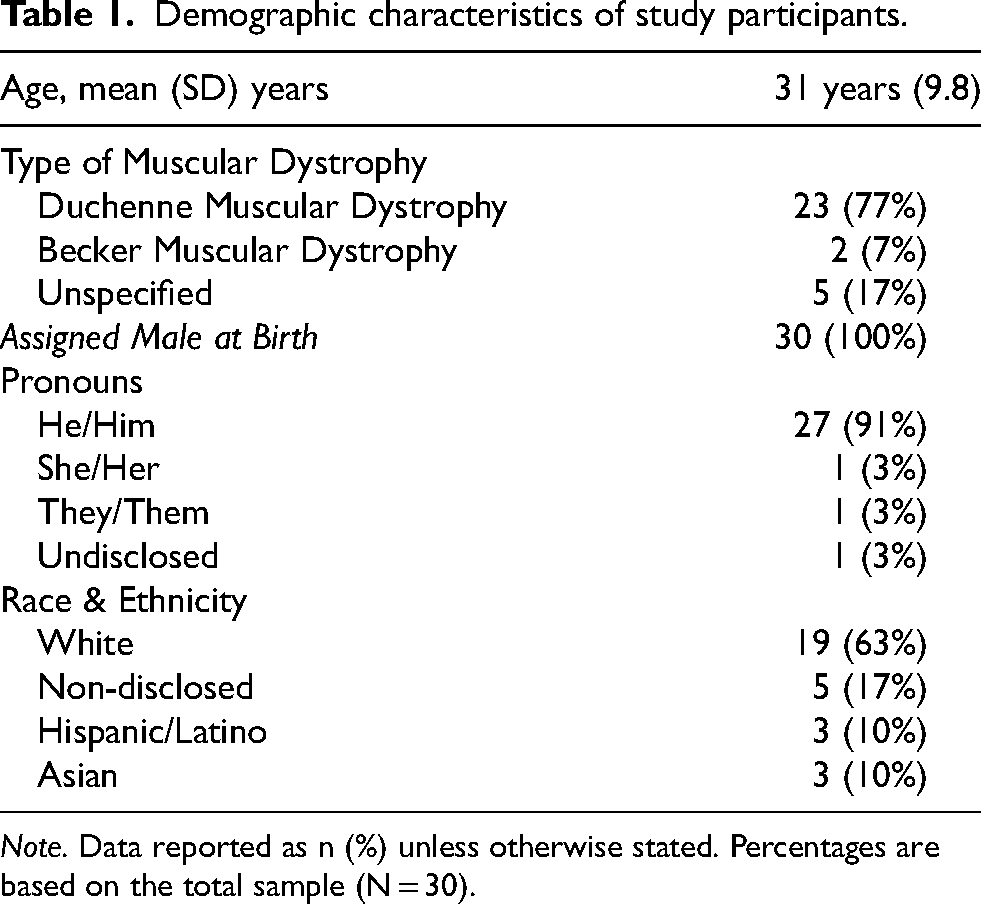
Note. Data reported as n (%) unless otherwise stated. Percentages are based on the total sample (N = 30).
Medical care background
To contextualize patient care experiences, we asked about primary care arrangements and prior discussions on sexual health (Table 2). Although all participants were adults, a sizable minority (17%) continued to see a pediatrician as their PCP, highlighting the persistence of pediatric care into adulthood for young adults with MD. Continued reliance on pediatric primary care in adulthood highlights ongoing transition-of-care needs in this population. Most participants reported never having discussed sexual health with a clinician (18/30, 60%); when discussions occurred, they were infrequent (8/30, 27%), with only 1 participant (3%) reporting frequent conversations. Among those with any discussion about sexual health, initiation was shared between physicians (n = 7) and patients (n = 5); one cited a partner; none cited parents/caregivers. Because of regional differences in medical practices across the United States, we also asked participants about the primary region of the country where they received medical care during childhood (Table 2). Our data show that we were able to collect perspectives from across the United States, with the highest representation from the Northeast and the Southern U.S.
Sexual education with medical providers.
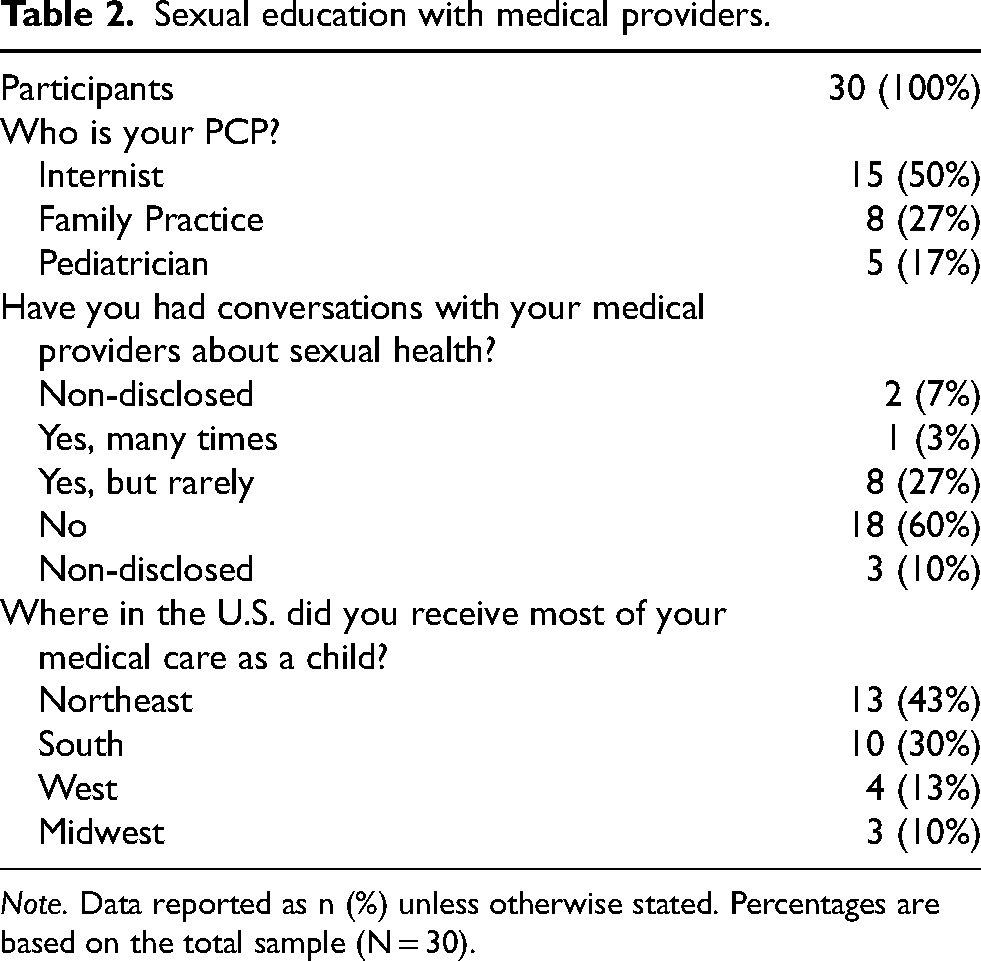
Note. Data reported as n (%) unless otherwise stated. Percentages are based on the total sample (N = 30).
Thematic analysis
Through 30 in-depth interviews, participants described both barriers to sexual and reproductive healthcare and priorities for improving it. We identified 12 recurrent themes grouped into two overarching domains: Structural and Interpersonal Barriers (6 themes; Table 3) and Calls for Improvements (6 themes; Table 4). Figure 1 summarizes the proportion of participants endorsing each theme. The following sections summarize each domain, highlighting participant quotations that illustrate how lived experiences shaped both the obstacles encountered and the improvements envisioned for high-quality, inclusive care.
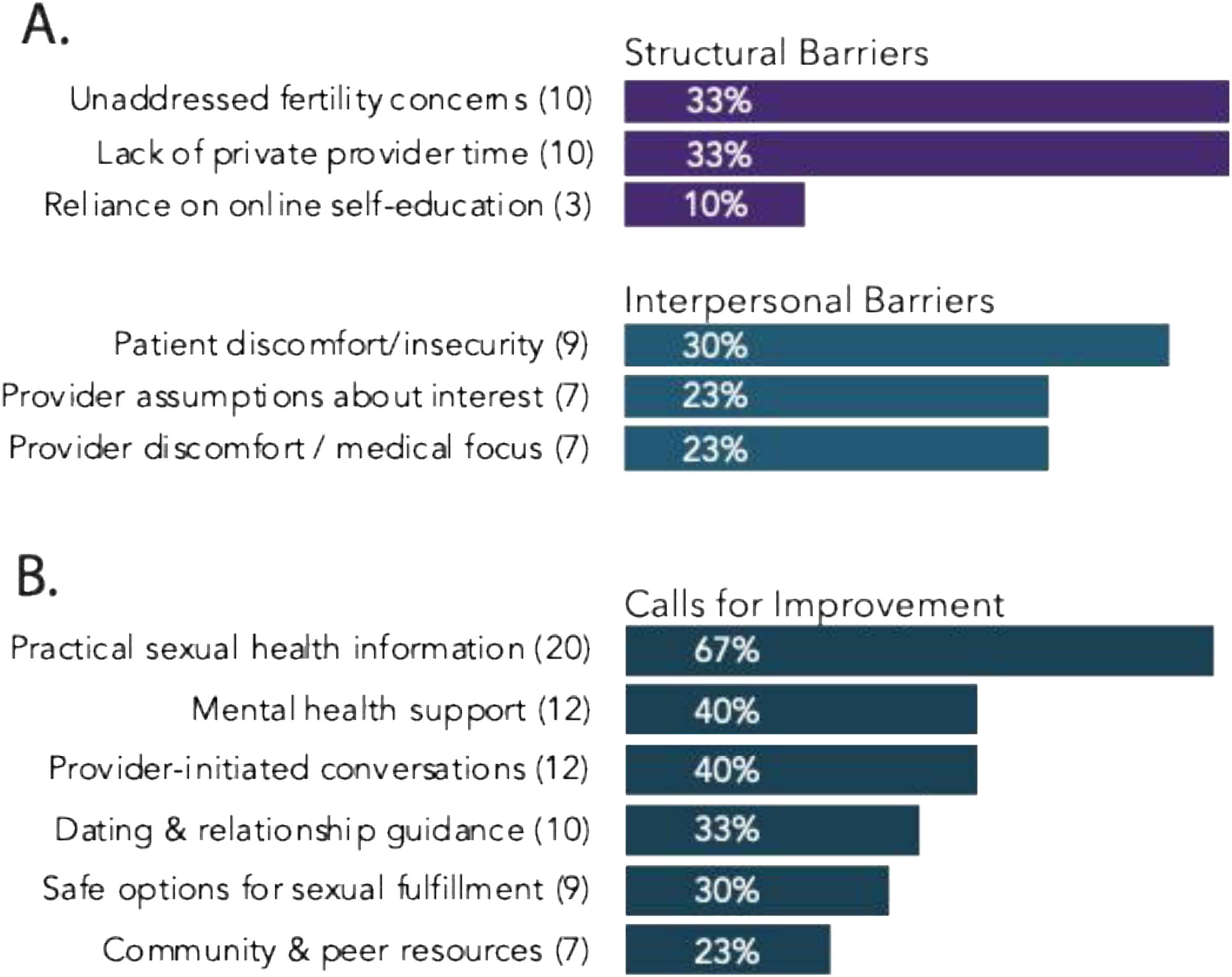
Endorsement of themes related to sexual and reproductive healthcare experiences and recommendations, including (A) structural and interpersonal barriers and (B) participant-identified priorities for improvement. Note. Bars represent the proportion of participants (n = 30) endorsing each theme. Numbers in parentheses indicate the number of participants who raised the theme. Themes were derived using reflexive thematic analysis; full descriptions and representative quotations are provided in Tables 3 and 4.
Structural and interpersonal barriers to sexual healthcare delivery.
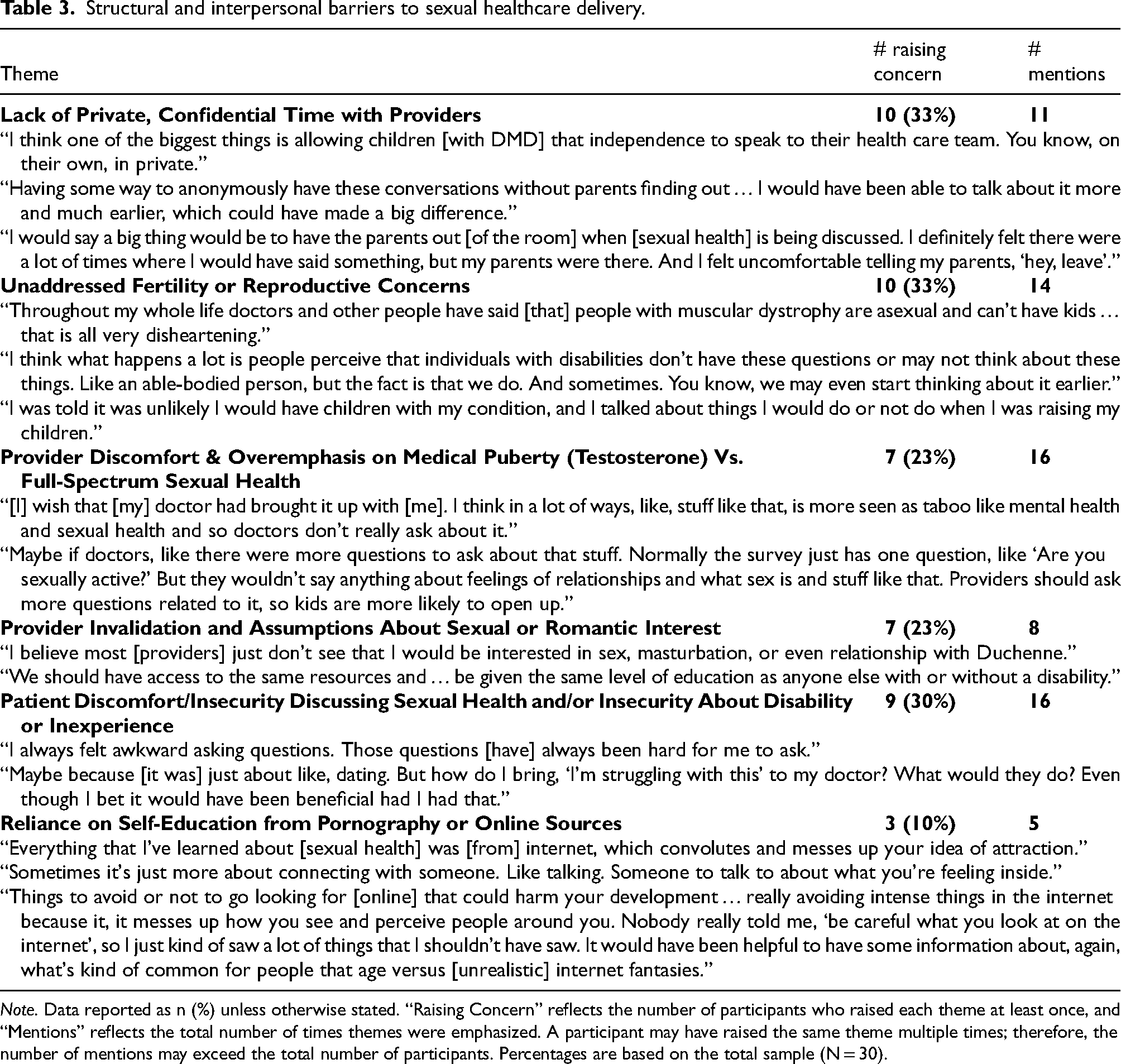
Note. Data reported as n (%) unless otherwise stated. “Raising Concern” reflects the number of participants who raised each theme at least once, and “Mentions” reflects the total number of times themes were emphasized. A participant may have raised the same theme multiple times; therefore, the number of mentions may exceed the total number of participants. Percentages are based on the total sample (N = 30).
Calls for improvements in sexual healthcare.
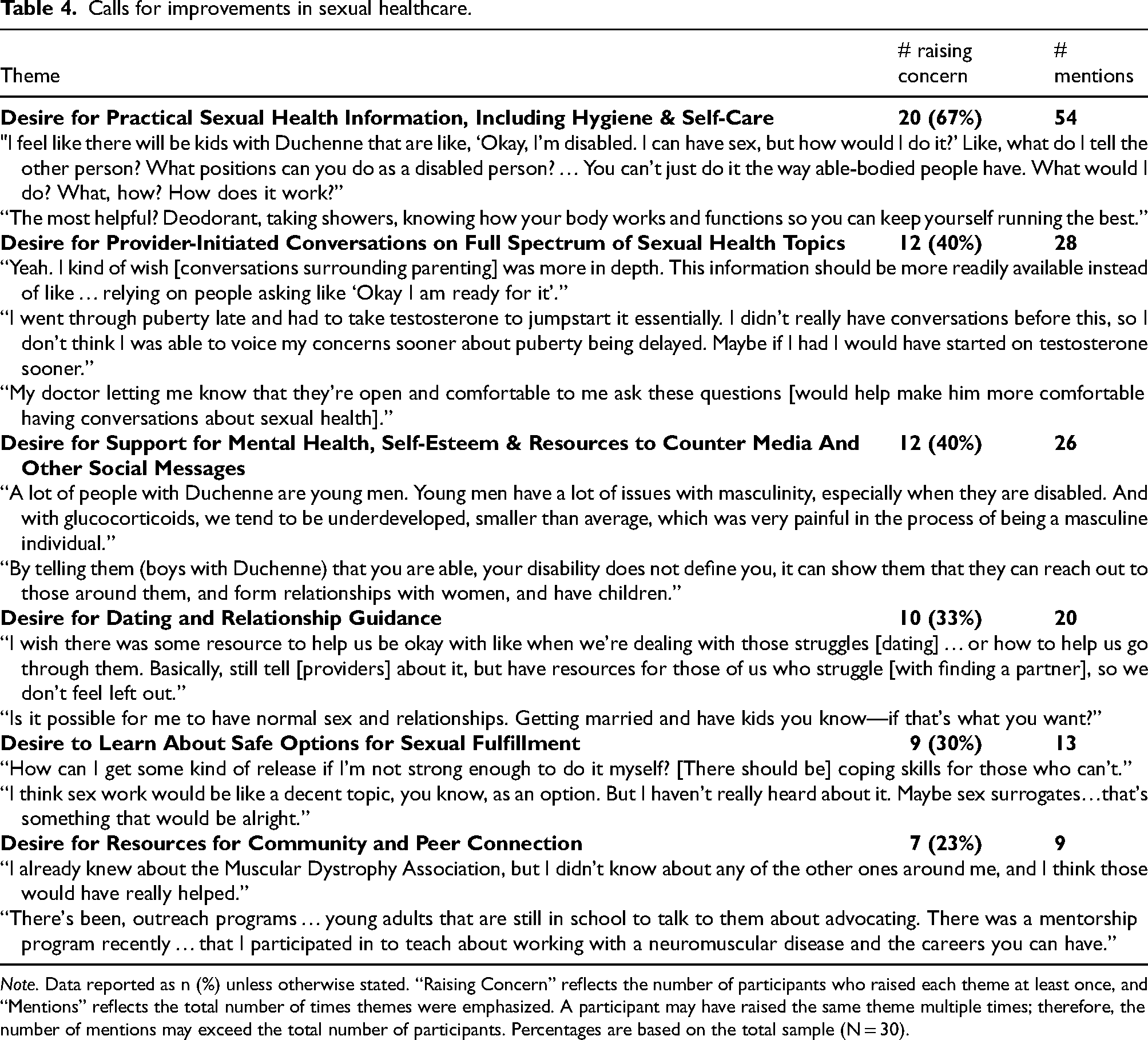
Note. Data reported as n (%) unless otherwise stated. “Raising Concern” reflects the number of participants who raised each theme at least once, and “Mentions” reflects the total number of times themes were emphasized. A participant may have raised the same theme multiple times; therefore, the number of mentions may exceed the total number of participants. Percentages are based on the total sample (N = 30).
Structural and interpersonal barriers to sexual and reproductive healthcare
Participants described multiple barriers to receiving comprehensive sexual and reproductive healthcare (Table 3).
Lack of private, confidential time with providers
A frequently raised concern was the absence of private, confidential time with clinicians (n = 10; 33%). Participants described how the presence of caregivers during visits limited their ability to ask questions or disclose concerns about sexual health. Several participants emphasized that while caregiver involvement was often necessary for daily care, it created barriers to discussing sensitive topics. One participant explained, “I would have said something, but my parents were there. And I felt uncomfortable telling my parents, ‘hey, leave’.” Another noted that the ability to speak privately with clinicians “would have made a big difference.” These accounts illustrate how structural aspects of pediatric care may unintentionally limit opportunities for confidential sexual health discussion.
Unaddressed fertility or reproductive concerns
An equal proportion of participants (n = 10; 33%) described receiving messages that people with muscular dystrophy were unlikely to have children. Several participants reported that clinicians or others had suggested that reproduction was improbable or irrelevant, which discouraged fertility-related discussions during clinical visits. Over time, some participants described beginning to internalize these messages. One participant explained, “Throughout my whole life doctors and other people have said [that] people with muscular dystrophy are asexual and can't have kids … that is all very disheartening.” Another reflected that assumptions about disability often shape clinical conversations, noting, “I was told it was unlikely I would have children with my condition.” Together, these accounts suggest that assumptions about reproductive potential may contribute to the absence of fertility counseling in clinical care and shape how individuals with neuromuscular conditions view their own reproductive futures.
Provider discomfort and narrow focus on medical puberty
Provider discomfort and an overemphasis on medical puberty (e.g., testosterone initiation) rather than holistic sexual health were identified by seven participants (23%) and emphasized multiple times across their interviews. One participant noted, “It was definitely more in sort of a medical sense … they were mostly focusing on starting puberty… not that much about dating or relationships.” Participants described clinical encounters in which conversations prioritized biomedical milestones while leaving broader topics such as dating, relationships, and emotional wellbeing largely unaddressed. “Normally the survey just has one question, like ‘Are you sexually active?’ But they wouldn't say anything about feelings of relationships and what sex is and stuff like that.” Together, these accounts suggest that sexual health discussions in clinical care are often framed narrowly around endocrine management rather than encompassing the broader relational and psychosocial aspects of sexuality that participants identified as important.
Provider invalidation and assumptions about sexual or romantic interest
Seven participants (23%) described feeling invalidated by providers or encountering assumptions that they had no sexual or romantic interests, with one participant sharing, “I believe most just don’t see that I would be interested in sex, masturbation, or even relationships.” These perceptions discouraged participants from raising sexual health concerns, further limiting opportunities for comprehensive care.
Patient discomfort discussing sexual health
Patient discomfort discussing sexual health, often linked to insecurity about disability or limited sexual experience, was identified in nine interviews (30%). Several participants described feeling uncertain about how to raise sensitive topics with clinicians or questioning whether such concerns were appropriate to discuss in a medical setting. One participant explained, “I always felt awkward asking questions. Those questions [have] always been hard for me to ask.” Another reflected on the difficulty of initiating these conversations, noting, “Maybe because [it was] just about like, dating. But how do I bring, ‘I'm struggling with this’ to my doctor? What would they do?” These comments suggest that discomfort and uncertainty may prevent patients from seeking sexual health guidance even when they believe such conversations could be beneficial.
Reliance on self-education from pornography or online sources
Three participants (10%) reported relying on pornography or online resources for sexual health information. While they noted the convenience of these resources, they also described them as misleading, with one participant explaining: “Everything that I’ve learned about that was the internet, which … messes up your idea of attraction.” Another stated, “Nobody really told me, ‘be careful what you look at on the internet’, so I just kind of saw a lot of things that I shouldn't have seen.”
Calls for improvements in sexual and reproductive healthcare
Participants also articulated clear priorities for improving sexual and reproductive healthcare delivery across multiple themes. These described not only the type of information they felt would be useful, but how it would have been most useful to learn from their providers (Table 4).
Desire for practical sexual health information, including hygiene and self-care
The most frequent request was for practical sexual health information, including education on hygiene, self-care, and adaptive strategies for sexual activity. This theme was raised by 20 participants (67%). One participant explained the need for basic guidance, noting a desire to learn about “deodorant, taking showers, knowing how your body works and functions so you can keep yourself running the best.” Others requested more concrete, disability-specific guidance related to sexual activity, including positions, assistive devices, and safe movement strategies. As one participant stated, “If you’re [physically] limited, like what things can you do?”
Desire for provider-initiated conversations on full Spectrum of sexual health topics
Provider-initiated conversations about sexual health were requested by 12 participants (40%). Participants expressed a desire for clinicians to normalize discussions across a broad range of sexual health topics rather than waiting for patients to raise these issues themselves. As one participant explained, “My doctor letting me know that they’re open and comfortable for me to ask these questions [would] help make [me] more comfortable having conversations about sexual health.” Another participant noted, “Yeah. I kind of wish [conversations surrounding parenting] were more in depth. This information should be more readily available …” These accounts suggest that proactive clinician engagement may help normalize sexual health discussions and ensure patients receive timely information and support.
Desire for support for mental health, self-esteem & resources to counter Media and other social messages
Requests for mental health support and resources to counter negative or misleading social and media messages were raised by 12 participants (40%). Participants described how cultural narratives about disability shaped expectations around relationships, sexuality, masculinity, and self-worth. One participant explained, A lot of people with Duchenne are young men. Young men have a lot of issues with masculinity, especially when they are disabled. And with glucocorticoids, we tend to be underdeveloped, smaller than average, which was very painful in the process of being a masculine individual.
Desire for dating and relationship guidance
Guidance on dating and relationships was requested by 10 participants (33%). Participants described uncertainty about how to initiate relationships, navigate dating, and discuss disability with potential partners. One participant reflected, “I wish there was some resource to help us be okay with like when we're dealing with those struggles [dating] … Basically … have resources for those of us who struggle [with finding a partner], so we don't feel left out.” Participants also raised broader questions about the possibility of long-term relationships and family life. As one participant asked, “Is it possible for me to have normal sex and relationships … getting married and have kids, you know—if that's what you want?”
Desire to learn about safe options for sexual fulfillment
Education about safe options for sexual fulfillment was raised by nine participants (30%), particularly among individuals with physical limitations affecting sexual function. Participants described uncertainty about how to achieve sexual release safely or independently given reduced dexterity. One participant explained, “How can I get some kind of release if I'm not strong enough to do it myself? [There should be] coping skills for those who can't.” Others suggested that clinicians could discuss a broader range of options, including assistive devices, sexual surrogacy, or other supportive resources. As one participant noted, “I think sex work would be like a decent topic, you know, as an option. But I haven't really heard about it.”
Desire for resources for community and peer connection
Opportunities for peer connection and community-based resources were raised by seven participants (23%). Participants described how connecting with others who share similar lived experiences could provide emotional support, practical guidance, and a sense of belonging. One participant highlighted the impact of peer forums, noting, “The PAAC [Parent Project Muscular Dystrophy Adult Advisory Committee] is a bi-weekly meeting… about 30 different people… and we talk about advocating and careers you can have.” Others described how greater awareness of community organizations and mentorship opportunities would have been helpful earlier in their lives. As one participant explained, “I already knew about the Muscular Dystrophy Association, but I didn't know about any of the other ones around me, and I think those would have really helped.” Another participant described participating in outreach and mentorship programs connecting young adults with neuromuscular conditions, noting that these initiatives help individuals “learn about advocating… and the careers you can have.”
Discussion
This study highlights significant gaps in sexual and reproductive healthcare for adults with MD, revealing both structural and interpersonal barriers, and outlines clear participant-generated recommendations for improvements in their medical care. These findings echo prior research on disability and sexual health. Similar barriers have been reported in UK-based DMD cohorts, 9 and in qualitative studies of disabled men navigating gender and sexuality, 8 suggesting that these challenges are persistent across contexts and diagnoses. Participants emphasized that sexual health needs, including fertility, dating, and peer connection, do not end with puberty but persist well into adulthood, highlighting the importance of continuing sexual health discussions beyond adolescence within neuromuscular and endocrine care. Across interviews, participants consistently described a lack of private, confidential time with providers and the perception that certain topics—particularly fertility and reproductive health—were considered inapplicable to them. Our findings extend this literature by showing that, in the U.S. context, providers often underestimate or overlook the sexual and reproductive needs of people with disabilities, reinforcing stigma and limiting access to essential information and care.
A notable pattern that emerged from our analysis was that participants with later-onset disease (e.g., Becker muscular dystrophy) appeared to describe somewhat greater satisfaction with their sexual education and experiences compared with those whose disability manifested earlier in adolescence (e.g., DMD). Although limited by the small number of Becker participants in our sample, individuals with later-onset disease may have had more opportunities to explore sexuality during adolescence prior to the progression of physical limitations, which could influence sexual confidence and experiences. While prior work has suggested that individuals with congenital disabilities often report greater adaptation in domains such as self-esteem and disability identity,15,16 sexuality may represent a distinct domain where early-onset disability can limit opportunities for exploration. The relationship between timing of disability onset and psychosexual development warrants further investigation.
Although this study presents the lived experiences of those with MD, similar themes have been documented in adults with spinal cord injury, 17 cerebral palsy, 18 and other physical disabilities 19 where sexual health is frequently deprioritized in clinical encounters and is overshadowed by biomedical management. 20 Studies across disability populations consistently describe de-sexualization, infantilization, and limited access to sexual and reproductive counseling, including fertility-related guidance, suggesting that these barriers reflect systemic patterns in healthcare rather than diagnosis-specific challenges. Our findings reinforce that adults with MD encounter many of the same structural and attitudinal barriers observed in other disability communities, particularly assumptions of asexuality and the absence of private, developmentally appropriate discussions.
Importantly, gaps in sexual health communication are not unique to disability. Even among nondisabled adolescents and adults, providers often focus narrowly on risk reduction, while omitting relational, identity-based, and pleasure-oriented discussions. 21 However, for individuals with MD, these gaps appear compounded by disability-related assumptions, limited privacy in pediatric care models, and uncertainty regarding fertility and parenthood. Thus, while inadequate attention to sexual health is well documented across healthcare settings,20,21 the consequences may be magnified for people with disabilities due to intersecting structural and social barriers.
One salient observation was that although the majority of participants identified as cisgender men, and all were assigned male at birth, three participants described gender identities outside the male binary. This demonstrates that gender diversity exists even within predominantly male MD populations, and particularly DMD, reinforcing the need for providers to address gender identity during pubertal and sexual health discussions. Although sexual orientation was not brought up explicitly during our interviews, it would also be reasonable for providers to discuss it during this time.
Participant recommendations provide a clear roadmap for provider improvement. The most frequently cited need—practical, accessible sexual health information—reflects a desire for concrete, actionable guidance that addresses both general topics (e.g., hygiene, self-care) and disability-specific considerations (e.g., adaptive sexual positions, assistive devices). Calls for provider-initiated conversations further emphasized that proactive engagement from clinicians can normalize these discussions and create safer spaces for disclosure. Together, these findings underscore the importance of disability-inclusive training in medical education and continuing education, so that providers are equipped to address sexual health across the lifespan.
Participants also emphasized the need for mental health support, relationship and dating guidance, and peer/community connection. These recommendations highlight the interdependence of sexual health, emotional well-being, and social participation. Addressing these areas will require not only provider education but also interdisciplinary collaboration with mental health professionals, peer networks, and disability advocacy organizations.
Importantly, these findings point toward actionable strategies for clinical practice: integrating routine, private discussions about sexual and reproductive health into MD care; providing developmentally and disability-appropriate educational materials; and embedding psychosocial and peer support into primary care models. Our study underscores the need to dismantle the structural and interpersonal barriers that have historically marginalized sexual health in the context of neuromuscular disorders. Engaging with community perspectives and implementing community-driven priorities is essential to delivering equitable, person-centered sexual and reproductive healthcare. Future research should evaluate the effectiveness of such interventions in improving sexual health knowledge, reducing stigma, and enhancing quality of life for people with MD.
Limitations
As a qualitative study with 30 participants, our findings cannot fully capture the diversity of lived experiences among people living with muscular dystrophies. Our sample was predominantly cisgender male and largely composed of individuals with DMD, reflecting both the X-linked inheritance of DMD and the recruitment channels used in this study. This limits representation of women, gender-diverse individuals, and people with other muscular dystrophy subtypes whose experiences with sexual development, independence, and relationships may differ due to variation in disease onset and progression. Participants were also predominantly White, with representation from Asian and Hispanic groups. Eligibility was restricted to English-speaking adults with sufficient cognitive and communicative ability to discuss their sexuality. Although autism spectrum disorder (ASD) and other neurodevelopmental conditions are more common in individuals with DMD (reported prevalence 6–21% in DMD22,23), none of our participants identified as neurodivergent. Future research should intentionally examine how neurodivergence, including ASD, may shape perceptions and experiences of sexual and reproductive healthcare. Finally, the use of both synchronous interviews and written responses may have influenced how participants expressed their experiences. Despite these limitations, this study provides novel insight into the sexual and reproductive healthcare needs of U.S. adults with muscular dystrophies.
Conclusion
Adults with MD described significant barriers to optimizing their sexual health, including lack of privacy, provider discomfort, and assumptions of disinterest, while also outlining clear priorities for improvement. Participants emphasized the need for proactive, practical, and affirming guidance that extends beyond puberty to address sexuality, relationships, fertility, and self-image. By centering the perspectives of U.S. adults with MD, this study underscores the importance of integrating sexual health into multidisciplinary care and highlights the need for provider training and clinical resources that are co-created in partnership with individuals with muscular dystrophies and other lived experience stakeholders to ensure relevance, respect, and shared agency across the lifespan.
Footnotes
Acknowledgements
The authors would like to acknowledge support from our colleagues in the Neuromuscular Clinic at Boston Children's Hospital, as well as the patients and families in our clinic, and Parent Project Muscular Dystrophy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sexual Medicine Society of North America,
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.