
Abstract
Background:
Optoacoustic imaging (OAI) has emerged as a powerful modality for visualizing biological tissues with high spatial resolution and molecular specificity. When applied to skeletal muscle tissue, OAI provides unique opportunities to investigate muscle composition, function, and physiology beyond the capabilities of conventional imaging methods.
Results:
Literature search was conducted in PubMed using (“Optoacoustic” OR “Photoacoustic”) AND (“Muscle”), with relevant references additionally screened. Clinical studies include over 440 patients, mostly on skeletal muscle in neuromuscular disorders and peripheral artery disease. OAI detected structural changes such as fibrosis, and fatty infiltration, as well as functional impairments related to muscle perfusion and oxygenation. Preclinical studies demonstrate volumetric imaging of cardiac muscle, reflecting ongoing technological advances.
Discussion:
This review summarizes the fundamental principles of optoacoustic muscle imaging, technical implementations, and translational applications. Furthermore, it discusses approaches to signal quantification, artifacts, as well as translation into clinical practice. Emphasis is placed on applications in the field of neuromuscular disease, where OAI holds promise as a non-invasive, radiation-free, and bedside imaging modality for characterizing and monitoring disease-specific muscle alterations.
Conclusion:
OAI represents a rapidly evolving field with significant potential for advancing both fundamental muscle physiology research and the diagnosis and monitoring of (neuro-)muscular disorders.
Introduction
Muscle weakness - a common but nonspecific clinical symptom found in 5% of adults aged 60 and over in the US 1 – originates from a wide range of potential causes, including neuromuscular, metabolic, inflammatory, and vascular disorders.2,3 Current diagnostic approaches rely primarily on laboratory parameters and functional tests as well as electrophysiological and imaging studies.2–4 However, despite ongoing efforts for optimization and improved clinical standards, current diagnostic approaches may still yield inconclusive or nonspecific results. Therefore, muscle biopsy is often required to obtain a definitive diagnosis.5–7 This procedure is invasive, and its success is strongly dependent on the biopsy location, technique and combination with other diagnostic parameters; still, results may remain inconclusive.5,8,9 Due to advances in genetic testing muscle biopsy is increasingly avoided, especially in pediatric patients, allowing for diagnostic security without exposing them to additional risks, such as sedation or anesthesia. In adult populations, muscle biopsies are still frequently indicated due to highly variable phenotypes and vast differences in disease progression hindering clinical differentiation between suspected hereditary muscle disease and other causes of neuromuscular symptoms.10,11
With the growing importance of genetic testing and emerging gene therapies, there is a pressing need for sensitive, non-invasive biomarkers and imaging techniques to monitor disease progression and therapeutic response. Clinically established imaging methods include magnetic resonance imaging (MRI), which provides high-resolution structural and compositional information,12–18 and muscle ultrasound, a low-cost alternative enabling bedside imaging. 19 A promising yet not routinely available imaging modality is optoacoustic imaging (OAI), which combines optical contrast with ultrasound resolution. OAI enables the non-invasive, real-time detection of endogenous chromophores such as oxy- and deoxyhemoglobin, collagen, and lipids. 20 Multispectral optoacoustic tomography (MSOT), a hybrid optoacoustic and ultrasound modality has been translated in clinical studies to assess neuromuscular diseases,21–24 inflammation,25–30 tissue oxygenation,31–35 and vascular remodeling of muscle tissue.
This review provides an overview of current advances in in vivo characterization of muscle tissue using multispectral OAI. We discuss its principles, technical challenges, and clinical applications, with a focus on its ability to detect muscle remodeling and degeneration. We also explore how MSOT may serve as a sensitive and label-free tool to monitor disease progression and response to emerging therapies in neuromuscular diseases.
Technological background and concepts of optoacoustics
Optoacoustic imaging (OAI), also referred as photoacoustic imaging (PAI) is based on the photoacoustic effect: pulsed light absorption induces thermoelastic expansion and generates acoustic waves.20,36–39 While both refer to the generation of sound waves by light absorption, OAI is, very simplistic the broader term encompassing all light-induced acoustic phenomena, while PAI specifically focuses on those caused by pulsed or modulated light absorption in materials or tissues. Nevertheless, this is based on a much longer historical development, since the fundamental physical effect was described by Alexander Graham Bell in 1881 (Figure 1).36,40
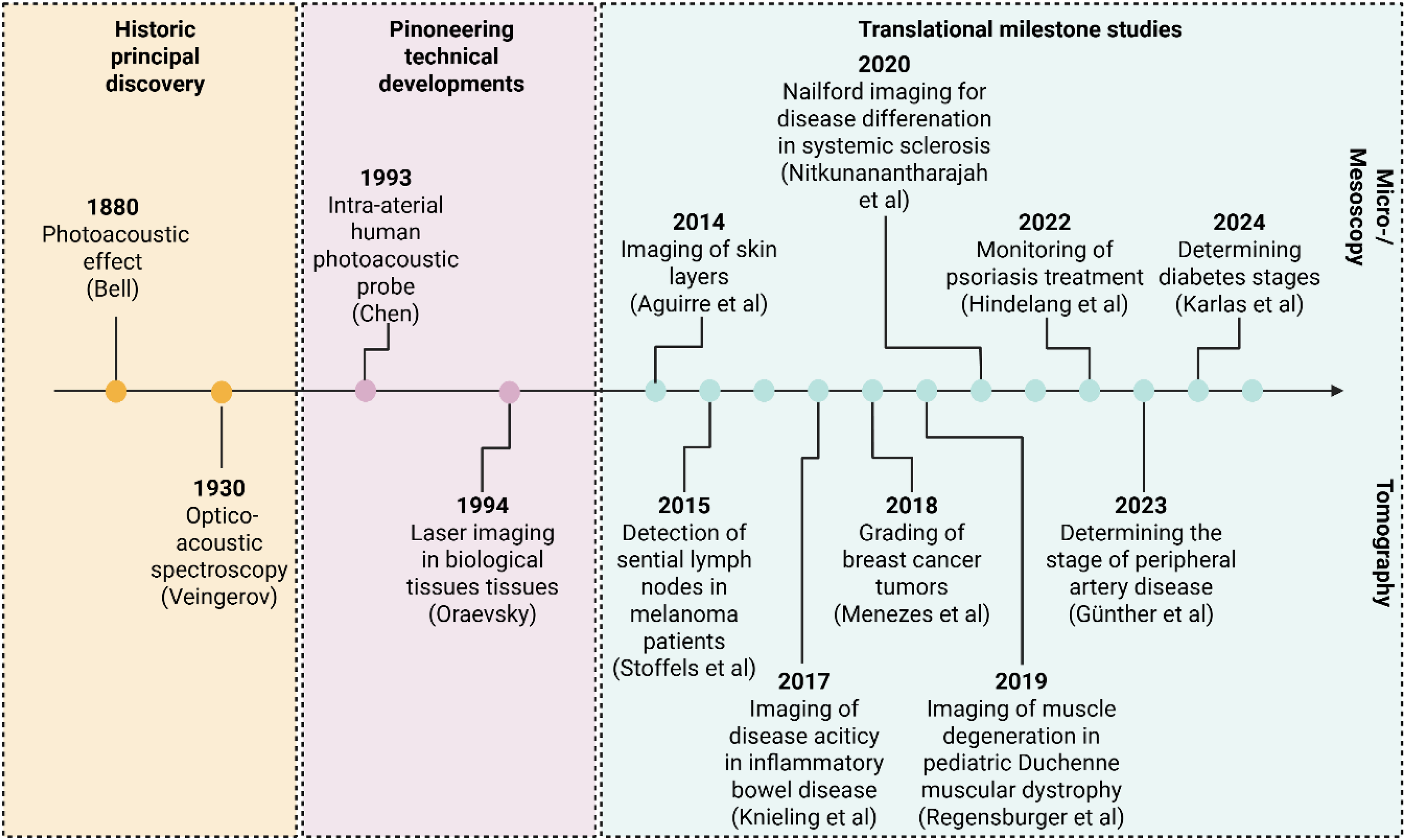
Timeline of key historical achievements and milestone studies in optoacoustic imaging with clinical translation. Created with BioRender released under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International license.
In OAI, excitation light is applied in the near-infrared (NIR) and extended near-infrared (exNIR) regions of the electromagnetic spectrum, typically spanning wavelengths from 700–900 nm (NIR) and 900–1600 nm (NIR-II) (Figure 2(a)).20,41,42 This “optical window” results from the wavelength-dependent absorption properties of biological chromophores: hemoglobin exhibits strong absorption at wavelengths below approximately 650 nm, whereas water absorption increases markedly above 1100 nm, thereby limiting light penetration at longer wavelengths.23,27,43 Consequently, the spectral range between 700–1100 nm is considered most favorable for biomedical optical imaging. 23 Here, endogenous chromophores such as oxygenated (HbO2) and deoxygenated hemoglobin (HbR), collagen, and lipids present distinct absorption spectra:26,42,44–48 In the NIR range, Hb and myoglobin are most prominent absorbers in human tissues, 49 with lower wavelengths around 700 nm targeting HbR, and wavelengths above 850 nm detecting HbO2. The so called isosbestic point can be found around 800 nm, representing the equal absorbance of both HbR and HbO2 (Figure 2(b)). Lipids, water, and collagen can be detected in the exNIR range, with lipids showing peak absorption at 930 nm. 27 Indocyanine green (ICG) is an exogenous contrast agent50,51 and has its absorption peak around 800 nm.51,52 In previous contrast-enhanced OAI studies it successfully visualized the gastrointestinal transit52–54 and lymphatic vessels. 55 Figure 2(c) provides a comparative overview of optoacoustic tomography and established imaging modalities. Across preclinical and clinical studies, the single wavelength 800 nm as well as spectrally unmixed hemoglobin parameters have consistently demonstrated physiological relevance, reliably capturing muscle tissue integrity and perfusion (Table 1, Figure 3).23,35
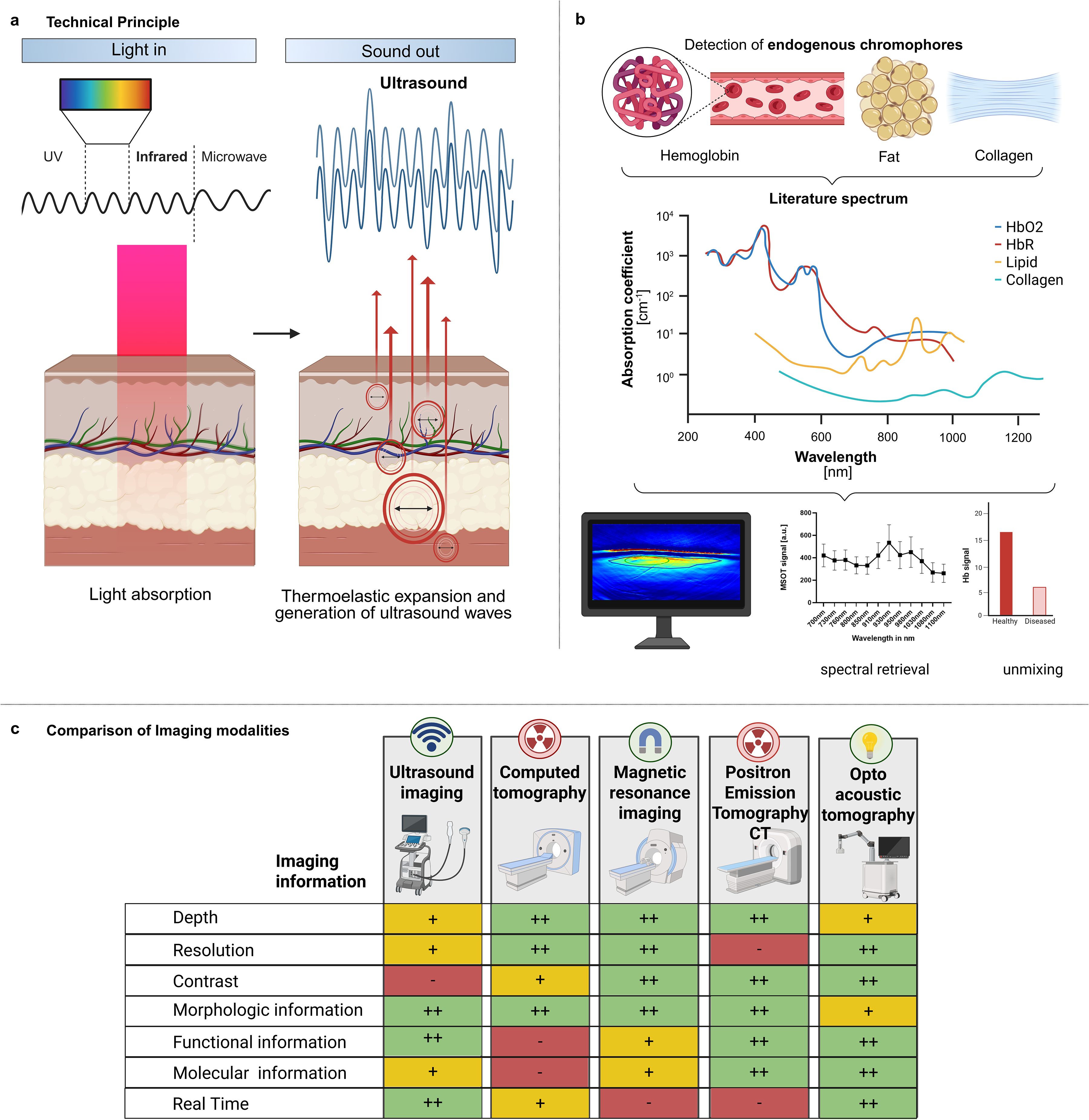
Principles and clinical context of OAI. a. Schematic illustration of the technical principle. b. Detection of endogenous chromophores based on molecular contrast arising from characteristic absorption spectra and post-processing quantification. Literature spectra for oxygenated hemoglobin (HbO2), deoxygenated hemoglobin (HbR), lipid, and collagen. Literature spectra are adapted from Regensburger A. et al., Biomedicines, 2021 c. Comparison of imaging modalities with respect to clinical applicability. Performance across individual parameters is indicated using color-coding (green: high, yellow: intermediate, red: low). CT: computed tomography. Created with BioRender released under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International license.
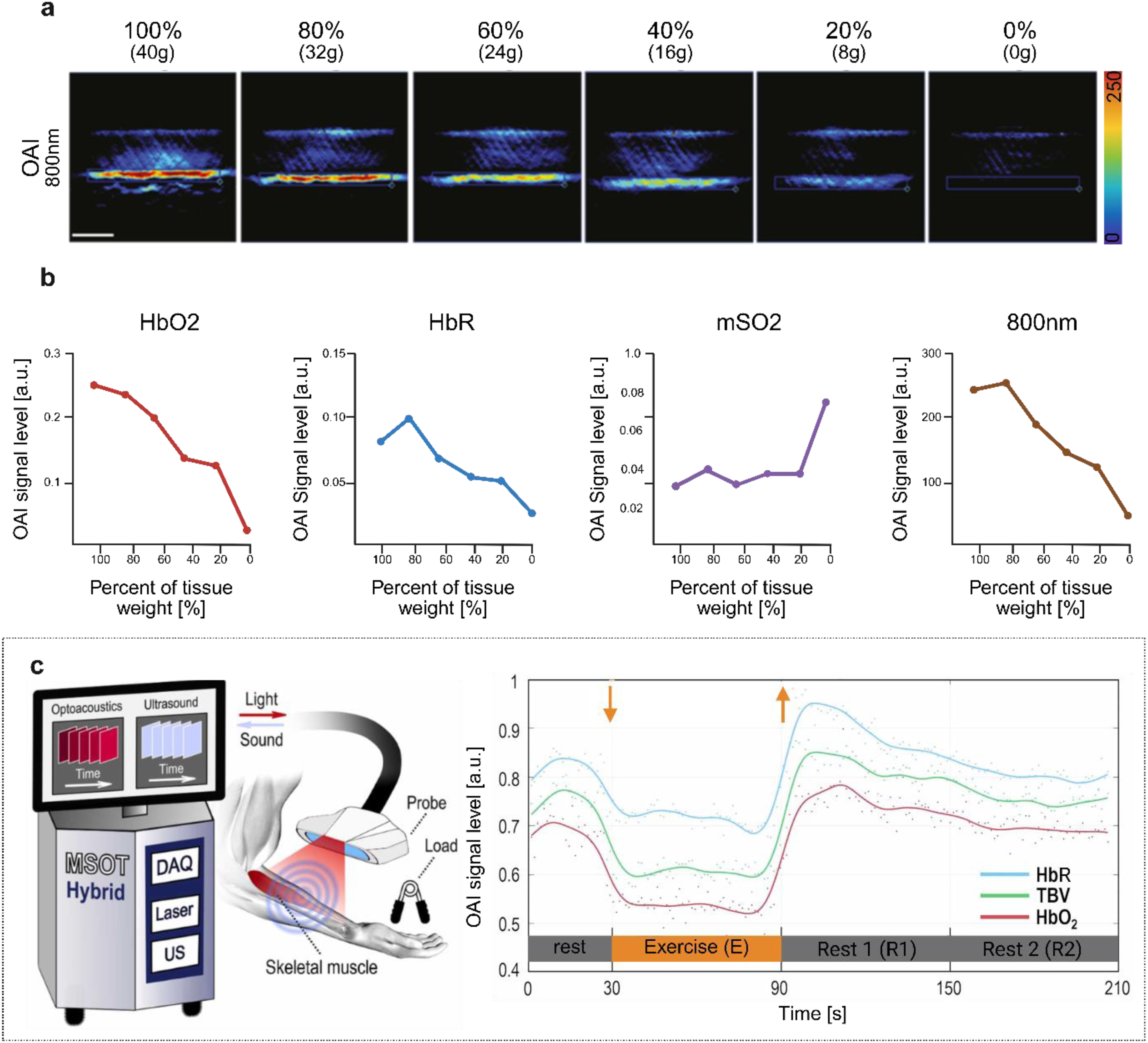
Validation of OAI sensitivity to muscle composition and oxygen metabolism. a. Representative titrated muscle phantom scans at 800 nm b. Quantitative measurements of titrated muscle phantom. From left to right: spectral unmixed oxygenated hemoglobin (HbO2), spectral unmixed deoxygenated hemoglobin (HbR), calculated oxygenation saturation (mSO2), and SWL 800 nm. c. Clinical exercise study of the brachioradialis muscle. Illustration of study setup and representative plot of the OAI signal under exercise. HbR: deoxygenated hemoglobin, TBV: total blood volume, HbO2: oxygenated hemoglobin, rest: 30-s baseline period before isometric exercise, E: 60 s period of isometric exercise, R1: first 60 s rest, R2: second 60 s rest. Adapted from Karlas, Photoacoustics, 2023. Created with BioRender released under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International license.
Clinical muscle studies on healthy subjects.
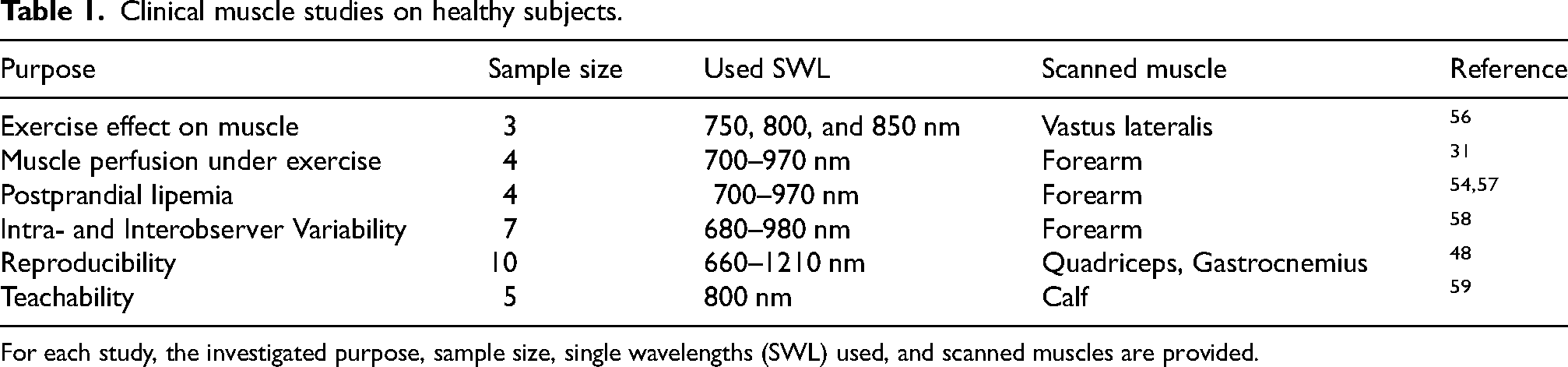
For each study, the investigated purpose, sample size, single wavelengths (SWL) used, and scanned muscles are provided.
Spatial resolution in OAI is determined not by the optical system, but by the ultrasound (US) diffraction limit and the bandwidth and geometry of the US detectors used. 44 This enables superior resolution at greater imaging depths compared to optical imaging.23,27,39,60 The OAI resolution is scalable from microscopic to mesoscopic and macroscopic imaging.61–64 For clinical applications, imaging is typically achieved using optoacoustic computed tomography, using linear or spheric detector geometries. 61 The resulting acoustic signals are reconstructed into cross-sectional or volumetric images using mathematical algorithms such as filtered back-projection or model-based approaches. 44 Following image reconstruction, spectral processing is performed to identify the specific signatures of intrinsic and extrinsic chromophores. 61 Spectral unmixing models the detected multispectral signal in each pixel as a linear combination of known absorber spectra and their respective contributions. With the use of multiple wavelengths, tissue can be examined, differentiated and quantified with respect to its endogenous chromophore composition. 61 A key technical limitation for spectral unmixing is the depth dependency: with increasing depth, the measured spectra are altered due to wavelength-dependent light attenuation (so-called “spectral coloring”), so that they no longer fully match the reference spectra.20,42,61 In addition, the signal intensity decreases with depth, which currently limits clinical applications mainly to superficially located tissue. Furthermore, laser power fluctuations and electronic noise can distort the measured spectra. For accurate quantification, the optical fluence, which is the light distribution in tissue, should be taken into account; however, this nonlinear optical approach remains a computational challenge. Current approaches to address these challenges include fluence correction methods, statistical modeling of tissue background, and subpixel target detection algorithms. 42 These technical limitations result in dependence of optoacoustic outcomes on biological factors such as sex, 65 skin pigmentation 66 and weight. Women were shown to exhibit generally lower MSOT signals, which may be attributed to higher body fat percentage. 67 Patients with darker skin tones (Fitzpatrick types IV-VI), or with dense body hair 27 presented lower signal intensities due to melanin-absorption in the lower wavelengths and reduced optical fluence. 67 As a result, OAI is currently best suited for slim individuals with lighter skin tones. However, within individuals, signal variations occurred between proximal, mid, and distal muscle regions, reflecting biological variability. 48 Nonetheless, studies have demonstrated high intra-rater and predominantly high inter-rater reproducibility.22,48,58
The approach of multiple wavelengths received different nomenclature such as Multispectral Optoacoustic Tomography (MSOT) or spectral photoacoustic tomography (sPAT). However, most clinical work has been performed on system termed MSOT Acuity (Echo) (iThera Medical GmbH, Munich, remark: Buisness discontinued). 68 Supportive for clinical use is the fact that the device is handheld, allows for simultaneous hybrid registration with B-mode ultrasound, and enables a short scanning time of approximately 10 s per image. 48
Optoacoustic muscle imaging
The ability of OAI to directly measure and visualize deoxygenated, oxygenated and total Hb 34 makes imaging of muscle a promising field of research. Quantification is typically reported as signal intensity in arbitrary units and compared to healthy controls. In this review, we discuss the major OAI studies focusing on skeletal muscle divided in neuromuscular diseases (NMD) and those of ischemic origin (e.g. peripheral artery disease). In addition, we discuss preclinical studies on imaging of beating murine hearts, considering it as a specialized muscular organ, to highlight the broader potential of OAI in imaging muscle-related pathophysiology across various systems. Table 2 summarizes selected OAI studies related to muscle.
Selected studies on muscle diseases.
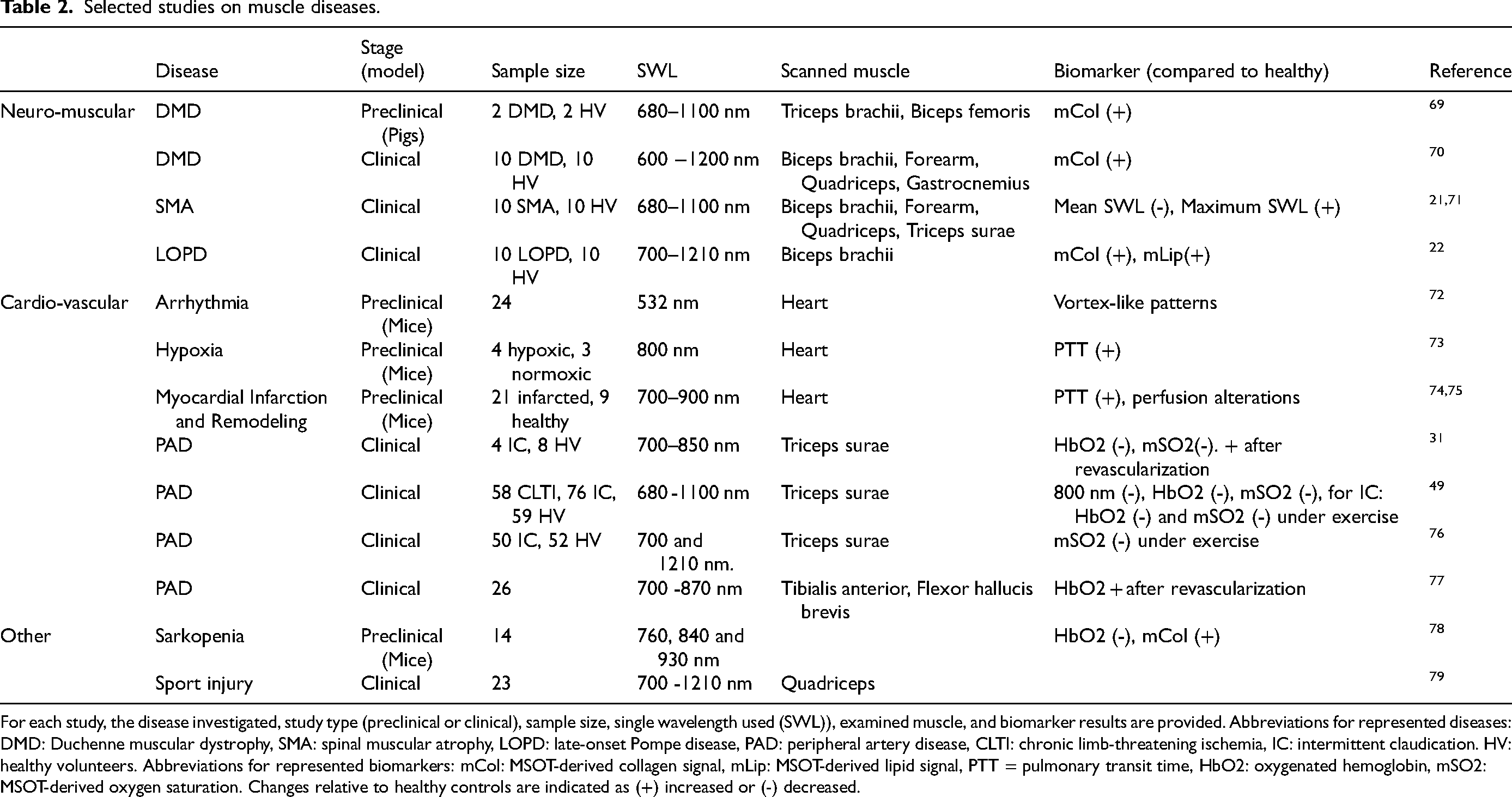
For each study, the disease investigated, study type (preclinical or clinical), sample size, single wavelength used (SWL)), examined muscle, and biomarker results are provided. Abbreviations for represented diseases: DMD: Duchenne muscular dystrophy, SMA: spinal muscular atrophy, LOPD: late-onset Pompe disease, PAD: peripheral artery disease, CLTI: chronic limb-threatening ischemia, IC: intermittent claudication. HV: healthy volunteers. Abbreviations for represented biomarkers: mCol: MSOT-derived collagen signal, mLip: MSOT-derived lipid signal, PTT = pulmonary transit time, HbO2: oxygenated hemoglobin, mSO2: MSOT-derived oxygen saturation. Changes relative to healthy controls are indicated as (+) increased or (-) decreased.
Neuromuscular disorders (NMD)
Considering the heterogeneity of (neuro)muscular diseases (NMD) and their diverse etiologies and pathophysiology, OAI may aid in the diagnostic evaluation of muscle weakness of unclear origin, disease severity and therapeutic monitoring. By assessing the molecular composition and hence visualizing specific changes in muscle structure and composition, it may contribute to more accurate differential diagnoses and enhance understanding of disease progression (Figure 4). Current clinical evaluations and endpoints for clinical trials primarily rely on functional muscle tests, which lack sufficient objectivity due to factors such as patient motivation, effort, and examiner dependency. 22 Laboratory tests, such as measuring creatine kinase levels, may not consistently show elevated values and can influenced by several other factors such as muscle mass and recent activity, limiting their diagnostic utility. Imaging techniques like ultrasound are limited in specificity, while MRI, although more informative, is not always easily accessible and not feasible for every patient. Muscle biopsy remains the diagnostic gold standard but is invasive and not ideal for pediatric patients or repeated assessments. 22 This underscores the urgent need for non-invasive, reliable techniques capable of directly and objectively assessing muscle pathology and disease progression.
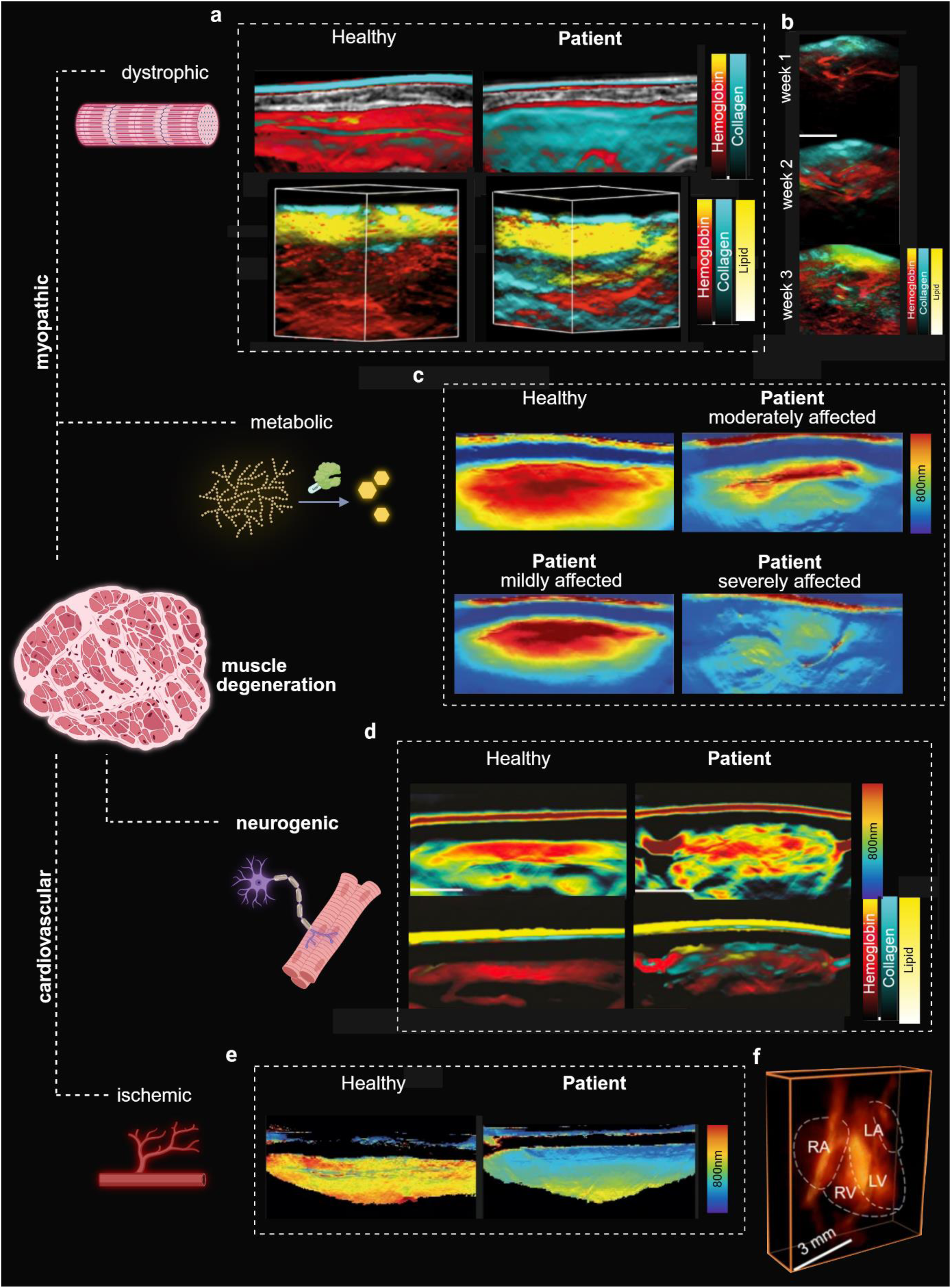
OAI applications in muscular diseases. Schematic overview of preclinical and clinical (boxed) OAI applications in various muscular pathologies.
Duchenne Muscular Dystrophy (DMD)
The first NMD to be investigated using OAI 70 was Duchenne muscular dystrophy (DMD), marking an important milestone in the application to NMDs. DMD is the most common X-linked inherited myopathy, caused by loss-of-function mutations in the dystrophin gene, the largest gene in the human genome. 80 Dystrophin is a cytoskeletal protein critical for muscle fiber stability; its absence leads to membrane instability, progressive degeneration, and fibro-fatty transformation in skeletal and cardiac muscle. Initial investigations in DMD pig models 69 showed elevated collagen signal intensities as early postnatally. The imaging approach demonstrated high diagnostic accuracy (AUC 0.98) for mean collagen signal intensity. Longitudinal imaging confirmed progressive collagen accumulation in dystrophic muscle, while wildtype (WT) animals showed stable signals. In human studies, DMD patients also displayed significantly increased collagen signal versus healthy volunteers (HV) with strong correlation to histopathological findings. 70
Spinal Muscular Atrophy (SMA)
A similar approach was subsequently applied to patients with spinal muscular atrophy (SMA), an autosomal recessive inherited disorder due to SMN1 deletions/mutations. 81 As part of the disease process, the lower motor neurons in the brainstem and spinal cord degenerate, leading to neurogenic muscle atrophy and weakness.71,82 Disease severity depends on the number of SMN2 gene copies, which partially compensates for the loss of SMN1. 83 MSOT imaging revealed a characteristic heterogeneous (“moth-eaten”) signal pattern, reflecting structural and compositional muscle degeneration. Spectral differences, especially at 800 nm, differentiated SMA from healthy muscle. SMA patients demonstrated lower mean but higher maximum signal values across all wavelengths, indicating focal tissue alterations. Elevated MSOT-derived lipid signal was observed in SMA, consistent with known patterns of fatty infiltration. MSOT also detected early changes in patients with preserved motor function and signal preservation was more evident in less severe subtypes.
Similar to approach, volumetric (3D) optoacoustic imaging has been successfully applied in patients with DMD and SMA.21,70 Using a cup-shaped, high-frequency detector (8 MHz),84–86 3D imaging of muscles visualized and quantified disease-specific muscle degeneration. In DMD, collagen signals were significantly elevated, and hemoglobin-related parameters were reduced. Receiver operating characteristic (ROC) analysis demonstrated strong diagnostic power. 70 In SMA, reduced signal at 800 nm was found in proximal but not distal muscles, consistent with the SMA characteristic pattern of muscle involvement. 21
Late-onset Pompe disease (LOPD)
NMDs can be caused by metabolic disorders. Pompe disease is a rare glycogen storage disorder, caused by autosomal recessive GAA mutation.22,87–89 Deficiency of GAA results in glycogen accumulation in metabolically active tissues, particularly the heart, skeletal muscles, and liver. Given the underlying pathophysiology of PD, the optoacoustic behavior of glycogen was first studied in a preclinical phantom. Results indicated that glycogen itself does not generate a direct optoacoustic signal; however, its high water-binding capacity appears to contribute to increased signal intensity, particularly at wavelengths associated with water absorption. In clinical imaging, adult PD patients demonstrated globally elevated MSOT signals, particularly for lipid and collagen. These changes appeared spatially homogeneous within the imaged muscle regions. More severely affected individuals showed increased lipid but reduced collagen signals, reflecting fibro-fatty replacement. Moreover, MSOT-derived lipid signal correlated with clinical measures of pulmonary and skeletal muscle function. 22
Comparison with MRI showed that MSOT may match or even outperform conventional imaging modalities. In LOPD, MRI-based fat fraction failed to distinguish between affected and healthy biceps muscle, whereas MSOT-derived lipid and collagen signals did. 22 In DMD, increased MSOT-derived collagen signal paralleled elevated MRI sodium concentration, both indicating extracellular matrix changes. Additionally, the highest fat fraction corresponded to the strongest optoacoustic lipid signal at 920 nm. 70
Together, these studies demonstrate the potential of MSOT as an imaging modality to characterize muscle and NMDs possibly on subcellular level. Its independence from patient positioning or motor function allows application even in advanced disease stages. In DMD, collagen signal reflected fibrosis due to dystrophin deficiency; in SMA, signal heterogeneity matched neurogenic atrophy; in LOPD, MSOT differentiated affected from unaffected muscle even when MRI did not. Overall, MSOT represents a valuable complementary tool for early diagnosis, longitudinal tracking, and therapeutic evaluation in NMDs.
Cardiovascular diseases
Owing to the low prevalence of NMDs, further investigation of fundamental OAI principles in additional patient cohorts was required. Notably, previous findings were transferable to considerably more prevalent conditions, such as peripheral artery disease (PAD), in which patients frequently present with functional limitations, including reduced walking capacity. Conversely, the higher prevalence of these conditions offers the opportunity to recruit larger patient cohorts and generate more extensive datasets, which foster mutual advances in understanding across disease entities.
Peripheral artery disease (PAD)
Lower-limb PAD afftects around 230 million preple worldwide and is caused by chronic arterial occlusion and subsequent malperfusion and inadequate oxygenation of the affected limb.90,91 Since muscle metabolism and function critically depends on sufficient perfusion and oxygen supply, PAD results in structural alterations and muscle damage.49,92 Current diagnostics are based on clinical examinations, such as the ankle-brachial index (ABI), being complement by various cross-sectional imaging modalities. In this regard, precise characterization and localization of the vascular stenosis is the major imaging biomarker.93,94. However, the end-organ, which is the muscle, is not yet at the center of clinical interest and therefore none of these methods provide structural or functional information about this central organ.49,92
The first study using OAI in PAD 31 demonstrated real-time detection of functional muscle tissue changes induced by arterial occlusion. In addition, it was possible to detect the physiological reactive hyperemia phase by measuring a significant increase in HbO2 signal in healthy muscle. Furthermore, distinct differences allowing differentiation between patients with PAD, with chronic limb-threatening ischemia (CLTI), and HV were described. 31 Especially, the HbO2 signal and signal at 800 nm showed strong discriminatory ability to distinguish healthy from diseased muscle tissue, correlating well with angiographic grading. 49 In cases with inconclusive clinical examinations (i.e., ABI), OAI was still capable to detect the correct diagnosis, indicating its potential in also supporting diagnosis in inconclusive PAD cases. 49 Building on this high diagnostic sensitivity, it became possible to detect exercise-induced functional impairment in patients with intermittent claudication (IC). Consistent with the functional and clinical limitations captured during exercise, heel-raise testing revealed a more pronounced impairment of muscle oxygenation in affected patients. This was evidenced by a post-exercise decline in the HbO2 signal, reflecting an inadequate vascular response to increased demand. 76 Additionally, in patients undergoing intervention, OAI detected improved muscle perfusion and oxygenation post-intervention, indicating its potential utility for follow-up monitoring and predicting therapeutic response.31,77 This data could be a foundation model to understand early functional treatment responses in novel NMD therapies.
In summary, OAI may enhance diagnostic precision and disease staging beyond conventional clinical methods. Accurate assessment of perfusion would provide feedback on the extent of hemodynamic improvement. This is particularly critical for patients with peripheral ulcerations, as it helps verify sufficient perfusion necessary for effective wound healing. 77
Heart muscle
Coronary heart disease remains the leading cause of mortality worldwide. 95 To understand the pathophysiological mechanisms underlying myocardial injury and remodeling, it is essential to link molecular alterations with whole-organ function. 96 OAI has recently been applied to cardiac muscle imaging. In this regard, technical advances enabled real-time volumetric optoacoustic tomography of the entire beating heart. 97 This approach facilitates the assessment of dynamic cardiac parameters such as valve function and myocardial contractility, while also allowing for the evaluation of myocardial perfusion. Using ICG as a contrast agent, pulmonary transit time (PTT) can be quantified, which has shown to increase significantly in infarcted mice and correlate with both infarct size and reduced ejection fraction.74,96 In addition to myocardial infarction, MSOT has been applied to models of myocardial remodeling 75 and chronic hypoxia-induced pulmonary hypertension. 73 Recent advances include cardiac imaging of embryonic heart development in real-time and high-resolution. 98 This may enable imaging of the dynamic progression of congenital heart diseases in the future. On the technical side, advances include the use of machine learning methods to analyze high-frame-rate volumetric cardiac imaging. 99
Overview of other clinical applications
OAI has also found application in numerous non-muscle related clinical applications. While it is beyond the scope of the present review, this section provides a brief overview of some of these studies. Numerous studies have been conducted in the last decade to image vascular,31,100–102 inflammatory,25,26,45 and oncologic103–106 pathologies. In vascular imaging, OAI has successfully mapped blood vessels of vascular malformations, 100 arteries and microvascular structures of the lower extremities 101 and carotid arteries 86 based on optical absorption properties of oxygenated and deoxygenated hemoglobin. Postprandial increase of lipids not only in blood vessels skeletal muscle and adipose tissue was detectable with OAI suggesting applications for monitoring of biomarkers in cardiovascular disease. 57 Vascular pathologies, such as vulnerability of carotid plaques, was demonstrated with OAI.28,107–109 In Crohn's disease, elevated hemoglobin signals in the intestinal wall correlated strongly with inflammatory activity, allowing OAI to non-invasively differentiate between active disease and remission.25,26 In breast tissue, it detected hormone-related changes in healthy parenchyma 110 and visualized malignancy-associated features such as tumor vascularization and altered tissue composition, with increased hemoglobin signals in invasive cancer.104–106 In comparison to Doppler ultrasound, MSOT revealed precise visualization of hemoglobin-rich, tumor-associated vasculature which offers a promising advantage for improving cancer diagnosis. MSOT also showed promise in dermatology, successfully delineating non-melanoma skin cancers from healthy tissue85,103 and enhancing sentinel lymph node imaging in melanoma using indocyanine green, offering a radiation-free alternative to conventional scintigraphy.111,112 In patients with systemic sclerosis, MSOT revealed significantly reduced oxygenated and total hemoglobin levels in finger tissue compared to healthy controls, reflecting microvascular dysfunction as a possible disease activity marker. 113 In addition, early detection and visualization of inflammation using MSOT has been demonstrated in psoriatic arthritis, potentially enabling earlier diagnosis. 30 The ability to detect lymphatic vessels in patients with lymphedema makes MSOT a promising tool in the field of lymphatic surgery. 114 A pilot study has introduced imaging of peripheral nerves with MSOT, with MSOT allowing visualization of the vasa nervorum by observing intraneural vessels in healthy nerve. 115 These feasibility data provide a baseline for further detection of peripheral nerve characteristics healthy tissue as well as neuropathies.
Translational limitations
Despite its successful application to many different muscle pathologies, the clinical application of OAI remains constrained by various methodological, and translational challenges. 116 OAI studies on NMD often rely on small and heterogeneous cohorts due to the rarity and clinical variability of these diseases,22,23,70,71 limiting the generalizability of results. Further validation through large-scale, multi-center clinical trials is required to establish impact on routine diagnostics. Furthermore, longitudinal studies are needed to validate the role of OAI in disease monitoring and progression. Another important area in need of development is the standardization of MSOT imaging protocols, especially for quantitative analysis in clinical settings.22,23,27 For interpretation of OAI data complex analysis is needed, revealing results only subsequently after examination, limiting its use in time-sensitive cases. Additionally, no reference values are available yet due to only few studies in NMD with small cohort sizes therefore interpretation of results is only feasible in comparison to matched healthy volunteers. To facilitate clinical use, norm values for OAI parameters are needed to allow data interpretation. The high cost of OAI systems presents a further barrier to clinical adoption.23,117 Many commercial systems rely on costly components such as OPO, dye-based, or Nd:YAG lasers, with some platforms costing up to one million dollars. Currently, only two CE-certified systems, Imagio (Seno Medical Instruments, USA) and MSOT Acuity (iThera Medical GmbH, Germany), are available for clinical use.23,61 Notably, hardware by iThera Medical is not marketed any longer. Increasing the number of commercially available systems and expanding competition may help drive down costs and facilitate broader clinical integration.23,61,117 Even though studies on teachability have demonstrated that MSOT can be reliably performed even by inexperienced operators. 59 with current handheld systems two examiners are required to obtain optimal images. Specific safety requirements due to laser safety regulations for currently marketed OAI systems can pose considerable structural challenges for OAI implementation, particularly regarding facility availability and personnel.
Future perspective
A promising application of optoacoustic imaging lies in its integration with emerging gene therapy approaches in neuromuscular disease. With recent advances in gene replacement, antisense oligonucleotide and RNA-targeted therapies, OAI could serve as a valuable tool for non-invasive molecular assessment of disease processes and monitoring treatment response. A technical advancement is the integration of deep learning algorithms into OAI data analysis. These algorithms have the potential to improve the efficiency and precision of optoacoustic data evaluation by enabling more accurate identification of specific patterns. Initial studies suggest that deep learning can fully exploit the spatial information contained in OAI data, resulting in more accurate, consistent, and efficient analyses. 33 In the future, the application of deep learning may further enhance the interpretability and reproducibility of results, thereby improving the reliability of diagnostic assessments.
Conclusion
Since its first clinical applications, optoacoustic imaging and more specifically multispectral optoacoustic tomography has demonstrated promising diagnostic capabilities for muscle diseases of various etiologies, providing findings that align with underlying disease mechanisms. As a non-invasive, radiation-free imaging modality, it enables sensitive characterization of muscle tissue at the molecular level. It may thus complement clinical diagnostic and molecular genetic testing by contributing to more detailed phenotypic characterization. In the context of emerging gene therapies, it holds potential as a valuable tool for longitudinal monitoring of disease progression and therapeutic response. Its high reproducibility, short acquisition times, and point-of-care applicability make it particularly suitable for use in large and vulnerable patient populations, including pediatric cohorts.
Footnotes
Acknowledgements
FK received funding from the EUROPE European Research Council ERC Starting Grant No 101115742-IsseG.
Author contributions
Conceptualization, L.T., F.K.; writing, original draft preparation, L.T., F.K.; writing, review and editing, L.T., S.M., J.Z., F.K.; visualization, L.T., F.K.; supervision, F.K. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the EUROPE European Research Council ERC Starting Grant, (grant number 101115742-IsseG).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.K. and U.R. were members of the advisory board of iThera Medical GmbH (Munich, Germany). F.K. received travel supports from iThera Medical GmbH (Germany) and Sanofi Aventis (Germany). F.K. reports lecture fees from Sanofi Genzyme. SM received speakeŕs honoraria for lecturing from Argenx, and travel, accommodation and congress fees from Biotest, Kedrion, Alnylam Pharmaceuticals, Argenx and Janssen. J.Z. received speakeŕs honoraria for lecturing from Alexion, Amicus, Argenx, Kedrion, Roche, Sanofi and UCB and travel, accommodation and congress fees from Alexion, Argenx, Janssen, Kedrion, Sanofi and UCB. Research was granted by Argenx and UCB. JZ is board member of the German Myasthenia Association and member of the German Muscle Society. The other authors declare no competing interests.