
Abstract
Objective:
To integrate current evidence and expert consensus on safe, effective exercise prescription in Duchenne and Becker muscular dystrophy (DMD/BMD), translating key pathophysiological principles into practical clinical guidance.
Methods:
Proceedings from the June 2025 Parent Project Muscular Dystrophy meeting, Translating Exercise Research in Dystrophinopathy to the Clinic, were synthesized. Faculty reviewed dystrophinopathy pathology and exercise physiology, analyzed data from clinical trials and pilot studies, summarized outcome-measure selection, and discussed pragmatic solutions to overcome barriers. Through interactive discussion, expert opinion on clinical management was aligned with exercise prescription frameworks (FITT) and clinic resources.
Results:
Exercise modality and dosing are understudied in dystrophinopathies yet represent critical factors for safe and effective interventions. In DMD, assisted low-intensity cycling can stabilize function and moderate isometric protocols can increase strength without evidence of injury. In BMD, aerobic training and supervised low-intensity resistance generally improve fitness/strength, whereas high-intensity loads may pose risks. Pragmatic assessments support monitoring and anticipatory care. Individualized prescriptions, supervised onboarding, and social engagement may mitigate dosing uncertainty, equipment access, and adherence barriers. The clinical framework should emphasize movement observation, postural strategies, oculomotor and cognitive-motor screening, and documentation for insurance coverage. Safety guidance emphasizes physician clearance, submaximal dosing, fatigue management, and clear “red flag” escalation pathways.
Conclusion:
Contemporary data and expert consensus support integrating conservative, systematically monitored exercise as an essential adjunct to DMD/BMD care. Available evidence indicates low-to-moderate aerobic activity and moderate-intensity isometric exercise appear feasible and safe when individualized and supervised. Further controlled studies should refine dosing and strengthen disease-stage-specific guidance.
Keywords
Introduction
On June 18–19, 2025, Parent Project Muscular Dystrophy (PPMD) convened a meeting on “Translating Exercise Research in Dystrophinopathy to the Clinic” in Las Vegas. Although exercise was historically discouraged in Duchenne and Becker muscular dystrophy (DMD and BMD) out of concern it might harm fragile dystrophic muscle, exercise is now being re-examined to counter disuse atrophy, protect strength, and support cardiopulmonary health. The meeting brought together rehabilitation clinicians and researchers from diverse settings, including physical therapists, occupational therapists, exercise physiologists, and neuromuscular specialists. Participants ranged from senior experts to early-career professionals specializing in either dystrophinopathies or more broadly across neuromuscular disorders, creating a dynamic environment for shared expertise and collaboration. Participants were engaged in discussion throughout the meeting to shape consensus on exercise in individuals with dystrophinopathy along with expert opinion of presenters.
The meeting was led by a core faculty group working in concert to align exercise evidence with clinical practice: Donovan J. Lott, PT, PhD (University of Florida), Tanja Taivassalo, PhD (University of Florida), Tina Duong, PT, PhD (Stanford University), and Claudia R. Senesac, PT, PhD (University of Florida). Their shared aim was to dispel persistent misconceptions that “any exercise is harmful” in dystrophinopathies and to delineate (based on available evidence) when, how, and how much activity can be prescribed safely and productively. The team noted that this is a critical moment for rehabilitation specialists; as disease-modifying treatments emerge, patients and families are increasingly advocating for the integration of exercise and rehabilitation into comprehensive care models.
The program opened with foundational concepts in pathophysiology and exercise science, introduced methods for safe monitoring and outcomes tracking and concluded with strategies for clinical translation.
Pathophysiology of dystrophinopathies
The field has shifted from skepticism to cautious acceptance regarding exercise in dystrophinopathies. Early exploratory studies of resistance exercise in boys with DMD (1960s–early 1980s) reported modest strength gains and maintenance of function—without any evidence of harm.1–3 Strengthening exercise programs in DMD were later dismissed as potentially harmful following mdx mouse experiments that used eccentric (lengthening) contraction protocols—a type of exercise known to damage muscle—to test dystrophic muscle membrane fragility.4,5 More recently, there is growing recognition that the type of exercise is critical, and selecting an appropriate regimen has become central to rehabilitation for this patient population.6,7
Pathophysiology and disuse
In healthy individuals without neuromuscular disease, stress from unaccustomed, higher-intensity, or eccentric exercise can produce small amounts of microdamage to muscle fibers. This triggers a cascade of repair events that restore integrity and, over time, result in hypertrophy—larger, stronger fibers capable of generating greater force.
In dystrophinopathies, muscle is vulnerable to injury during cycles of muscle contraction and relaxation. 8 The dystrophin-associated glycoprotein complex (DGC) is key for muscle repair. Dystrophin, a key element of the DGC, anchors the cytoskeleton to the extracellular matrix through the sarcolemma and stabilizes the muscle fiber during contraction. With DGC deficiency and the absence of dystrophin (as in DMD), the sarcolemma becomes fragile and highly susceptible to injury even under low force that leads to muscle being replaced by fat and connective tissue. 9 In BMD, in-frame mutations allow partial or reduced dystrophin function, producing a milder but still vulnerable phenotype. 10 In the absence of disease-modifying therapy, the lack of functional dystrophin in DMD leads to rapid disease progression, with most boys losing ambulation around age 12 years and experiencing a steep decline thereafter. In contrast, BMD follows a slower course, with significantly greater heterogeneity in clinical presentation than in DMD.
Historically treated as distinct conditions, dystrophinopathies are increasingly understood as a clinical spectrum of severity.11,12 This framing is especially relevant for exercise, since disuse atrophy is a universal phenomenon: without sustained activity, skeletal muscle weakens and shrinks, loses capacity for oxidative metabolism and becomes more fatigable. While concern about injury led to decades of discouraging activity in DMD and BMD,4,5 accumulating evidence indicates that moderate, carefully calibrated exercise may be protective for dystrophic muscle.13,14 In BMD, maintaining fitness is needed for heart health and longer survival, 15 and in DMD, “gentle exercise” is recommended to counteract disuse atrophy. 16
Early research on exercise for those with dystrophinopathy
Between the 1960s and early 1980s, small studies suggested that resistance training could be tolerated in boys with DMD. Vignos and Watkins reported gains in lifting capacity, 1 de Lateur and Giaconi found increased knee extensor torque without overload weakness, 2 and Scott et al. noted that manual resistance exercise helped maintain function without decline. 3 None of these studies reported any harmful effects from the exercise in these participants with DMD.
Then, in 1984, studies examining muscle fragility in the mdx mouse model led to extended delays in further exploring exercise as a therapeutic intervention. This was due to initial findings that eccentric downhill treadmill running in the dystrophin-deficient mice resulted in muscle damage, leading to broad generalizations that all exercise was harmful in human dystrophinopathies.
However, exercise is not monolithic—contraction type matters. Beginning in the 2000s, exercise specialists began reframing activity not as an inevitable trigger for injury but as a means to preserve strength, mobility, and quality of life. They highlighted significant gaps in research and called for studies to systematically assess the benefits of exercise in DMD, from structured training protocols to investigations of physiological outcomes. 17 Well-designed, controlled studies could identify safe and beneficial regimens while illuminating DMD pathophysiology.5,18
Emerging clinical evidence in DMD
The first randomized control trial (RCT) of exercise in DMD, the “No Use is Disuse” study, evaluated low-intensity, active-assistive arm and leg cycling, specifically designed to minimize eccentric contractions, performed five times per week for six months. 19 Functional scores (MFM-32) remained stable in the exercise group, while controls declined, demonstrating that even minimal activity can mitigate deterioration.
Building on the principle that mode selection is pivotal, University of Minnesota investigators examined the effects of isometric contractions in the mdx mouse, where the muscle generates force without changing length. Even at high intensity, isometric exercise did not exacerbate pathology, but instead improved force production and contractile performance. 14 These findings provided the biological and safety rationale for Dr. Lott and his colleagues to pilot carefully dosed isometric protocols in boys with DMD in two small studies. 13 The team started cautiously, testing a single bout of isometric exercise in ambulatory boys with DMD. Participants performed one session of four sets of six repetitions at 30% of maximal voluntary contraction, and then the protocol was progressed by having additional boys perform repeated sessions at 50% MVC. Both of these exercise paradigms were feasible and resulted in no elevation in CK (creatine kinase) or MRI changes providing supportive evidence of safety for these protocols in DMD. Encouraged by these results, the team implemented a 12-week, home-based program using a low-cost pediatric device adapted to ensure purely isometric contractions. Adherence was high, strength increased, and functional gains were maintained, all with no CK rise or negative MRI changes. While small and not randomized, these findings provide proof-of-concept and preliminary evidence that isometric training is tolerable and potentially beneficial in DMD and justify larger, controlled studies including home-based, remotely supervised interventions.
In addition to land-based exercise modalities, aquatic therapy is fundamental to rehabilitation given the hydrodynamic properties of water. 20 Despite an earlier pilot trial questioning feasibility of aquatic therapy in DMD, 21 more recent studies support its safety and efficacy.22,23 For example, dynamic, whole-body aquatic exercise prescribed using individualized heart rate targets to regulate intensity improved motor outcomes after 4 months, without evidence of increased muscle inflammation assessed by MRI. 23
Current exercise research in BMD
Complementary findings support the safety and efficacy of exercise in BMD.
These findings suggest that moderate-intensity endurance exercise and supervised low-intensity resistance training are safe and beneficial in BMD, while high-intensity regimens may carry higher risk. Importantly, study populations were limited to individuals with mild-to-moderate disease; generalizability to more advanced phenotypes remains uncertain.
Clinical takeaways
Exercise—long regarded as potentially harmful in dystrophinopathies—may be performed safely under carefully controlled conditions. Studies in DMD now suggest that assisted or low-intensity aerobic cycling may help delay functional decline, and that moderate-intensity isometric strengthening can improve force generation without evidence of muscle damage. In BMD, both endurance training and supervised low-intensity resistance programs have shown gains in strength and fitness without adverse effects. However, high-intensity training may be associated with exercise-induced damage in some BMD patients, underscoring the need for caution and careful monitoring. Although current findings are encouraging, further research is needed to characterize risks and to optimize exercise regimens to maximize benefit.
Practical considerations
While current findings are encouraging, there is convergence on several pragmatic points: Cycling has emerged as the most practical and widely studied modality, with other options such as aquatic therapy noted but limited by feasibility, particularly for individuals who are non-ambulatory. Questions remain about the optimal age to introduce exercise. Young children may not reliably understand exercise protocols or follow through; however, protocols are easily modified to accommodate to the developmental maturity level of the individual. For highly active boys soon after diagnosis, clinicians recommend allowing self-regulation while discouraging repetitive eccentric activities such as jumping. Across ages, individualized recommendations, inclusive environments at home and school, and explicit teaching children to recognize and communicate fatigue—are critical for balancing safety with sustained engagement in meaningful activity.
Exercise is medicine
The preliminary finding in DMD/BMD echo what has been seen in mitochondrial myopathies, where patients were once advised to avoid physical activity but were later shown to benefit from structured training. 26 The multisystem benefits of exercise have been demonstrated in numerous healthy and clinical populations. Beyond skeletal muscle, aerobic training improves cardiovascular, metabolic, immune, and even cognitive function, through circulating factors released during and after activity. 27 For DMD and BMD, where these same systems are compromised, the rationale for exercise as medicine is particularly compelling. The task now is to demonstrate how exercise can be prescribed in ways that are both safe and beneficial for individuals with DMD and BMD.
The multifactorial limitations observed in response to a single bout of exercise in DMD—across ventilatory, circulatory, and muscular systems—highlight why an integrated, structured training approach may be therapeutic. Dynamic exercise depends on the integrated functioning of ventilation, circulation, and skeletal muscle to deliver oxygen to mitochondria. 28 In dystrophinopathies, the primary impairment in muscle disrupts this cascade, leading to compensatory but inefficient responses upstream. Cardiopulmonary exercise testing (CPET)—the gold standard for assessing cardiorespiratory fitness (peak VO2) and identifying limitations in cardiovascular, ventilatory, and peripheral muscle systems—in DMD has revealed severely reduced peak VO2, often below the threshold associated with loss of independence, cardiometabolic disease, and early mortality. 29 Boys with DMD also demonstrate earlier reliance on anaerobic metabolism, elevated heart rates during submaximal work, and hyperventilation. 29 These findings suggest that a therapeutic exercise regimen should aim to normalize such pathophysiological responses.
Adaptation depends on overload: frequent, lower-intensity muscle activity (typical of aerobic exercise) promotes mitochondrial biogenesis, capillarization, and improved cardiorespiratory efficiency, while higher-intensity, lower-frequency loading (typical of strengthening exercise) induces hypertrophy. 30 For DMD and BMD, the challenge is identifying a “safe window” of overload that promotes adaptation without sarcolemmal injury. The Physical Stress Theory suggests both excessive overload and underload impair tolerance to activity, 31 but precise thresholds for optimal loading in dystrophinopathies remain undefined. The FITT principle (based on parameters of frequency, intensity, time, type) provides a general framework for exercise prescription, 32 but no tailored guidelines yet exist for muscular dystrophies, in contrast to the dozens of clinical populations where such protocols are well-established.
Pilot study: Home-based aerobic and strength training in DMD
Preliminary results from a six-month home-based intervention in ambulatory boys with DMD, presented by Dr Taivassalo, illustrate how FITT parameters might be applied in DMD (Taivassalo et al., manuscript in preparation). Training consisted of three months of moderate-intensity, motor-assisted cycling, followed by three months of isometric knee exercises combined with continued cycling, using a custom-engineered ergometer and the pediatric devices validated in Lott's work. Cycling intensity was personalized according to heart rate, 33 consistent with recommendations for deconditioned and heart failure populations. Every exercise session was remotely supervised by the research team to ensure safe intensity and correct mechanics. Adherence was high (over 85%), and there were no adverse events or signs of muscle damage on MRI or CK. Importantly, participants demonstrated gains in the cross-sectional area of the quadriceps muscles, cardiorespiratory fitness, bone density, and metabolic markers, reinforcing the multi-system benefits of exercise. One boy wished to continue training following completion of the 6-month trial due to the benefits gained and has been independently cycling on an adaptive tricycle for the past two years. Improvements in cardiorespiratory fitness and submaximal exercise heart rate have been maintained and cardiac MRI revealed normal ventricular function with no fibrosis after two years. These data suggest improved myocardial efficiency, providing reassurance that prolonged moderate training did not worsen cardiac status. This case exemplifies the potential for research protocols to foster sustainable, long-term physical activity in the real-world setting. Taivassalo cautioned that this was a case study and that future studies assessing long-term skeletal muscle and cardiac impact of exercise are needed to support these findings.
Translation to practice
Key implications are that exercise intolerance in DMD arises from both muscular and cardiorespiratory inefficiencies; that moderate, appropriately dosed aerobic and isometric exercise is safe and feasible; and that preliminary data suggest multi-system benefits extending beyond muscle. Future work will expand modalities for non-ambulatory patients and female carriers and examine cardiac outcomes more systematically. Exercise should not be seen as optional, but as an adjuvant to emerging therapeutics in rehabilitation. At the meeting, the Rifton adaptive tricycle (Rifton Equipment, USA) fitted with Garmin monitors (Garmin Ltd, USA) for heart rate, speed, and distance, was demonstrated, showing how research protocols could translate into community use.
Access to adaptive cycles like the Rifton or other models, despite clear therapeutic benefits is a key barrier to translating these findings into practice. Insurance providers frequently deny coverage. Practical steps include sharing successful letters of medical necessity, recognizing that appeals often succeed when they emphasize the clinical requirement for submaximal exercise. In addition, there are grants and scholarships that are available to fund adaptive equipment like the Rifton adaptive cycle that can be found online. For individuals unable to get an adaptive cycle there are other alternatives for an aerobic workout such as ergometers for arms and legs, stationary bikes and aquatic exercise. Given the limited experience monitoring safety outside research settings, practical safeguards are recommended: keep intensity within moderate heart rate zones and use perceived exertion as a guide, with careful attention to red flags (see Table 3). Adherence and engagement, especially for younger children, remain challenges best addressed through close supervision and strategies that make exercise both structured and enjoyable.
Bridging research and clinical practice: Measuring progress, transitions and meaningful outcomes in-clinic
Moving from theoretical research to practical clinical assessment and patient management, there is a critical need to capture exercise metrics beyond currently validated clinical outcome tools to better monitor and personalize exercise programs and progression. A rigorous evaluation framework is central to successfully integrating exercise into DMD and BMD management. Selecting outcome measures sensitive enough to detect subtle, clinically meaningful changes—whether resulting from disease progression or therapeutic intervention—is essential for guiding individualized care and improving long-term patient outcomes. Sharing such evidence with families can also strengthen motivation and adherence by demonstrating that effort translates into measurable gains. 34
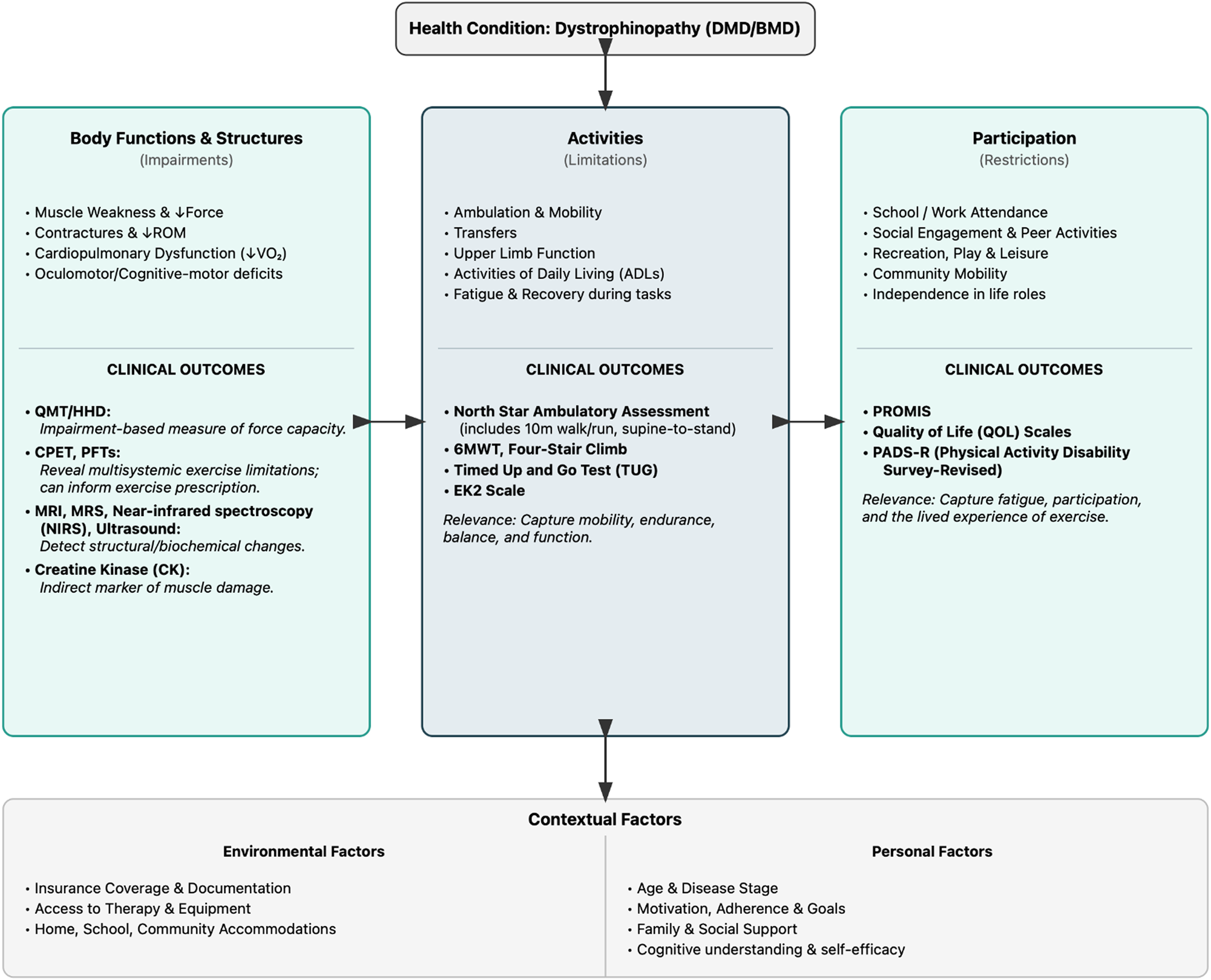
ICF based framework for exercise in dystrophinopathies.
A rigorous approach to measurement is the foundation of effective management. Intra-rater consistency typically exceeds inter-rater reliability; while utilizing the same clinician for longitudinal follow-up is ideal to maximize sensitivity to change, it is often practically difficult in a clinical setting. To mitigate the ‘noise’ of poor inter-rater reliability, which can obscure subtle functional change, clinical teams should standardize testing methods and equipment. This ensures that longitudinal fluctuations in scores reflect true changes in clinical status rather than variability between examiners or tools.
Beyond ensuring reliability, a thorough understanding of an assessment's psychometric properties, including its predictive value and floor/ceiling boundaries, directly informs clinical goals and treatment decisions. By selecting measures sensitive to a patient's specific functional stage, clinicians can transition from reactive monitoring to anticipatory care. This paradigm shift allows the team to forecast major milestones, such as the loss of ambulation, thereby reducing the logistical hurdles and addressing the psychological impact associated with functional decline.
Families also rely on outcome data to make informed treatment decisions— a need that is increasingly critical as advances in the DMD treatment pipeline and improvements in standards of care delay disease progression and extended survival.48–53 With disease-modifying therapies now available or in late-stage trials, the field is approaching a turning point: moving from a largely palliative model focused on slowing disability toward a rehabilitation model aimed at safe, restorative interventions. This shift should be undertaken gradually and guided by careful monitoring to ensure safety. Generating and sharing evidence on how exercise interventions can be introduced is essential to empower clinicians to prescribe them with confidence.
Barriers to integration of exercise interventions
Despite growing recognition of the importance of exercise—and the and pilot work led by Lott and Taivassalo evidence supporting submaximal exercise —significant barriers hinder its translation to the clinic. Research indicates that while 81% of neuromuscular providers support incorporating aerobic exercise into care, 77% cite uncertainty regarding screening and dosing as a primary obstacle. 54 Consequently, clinical implementation is driven less by skepticism than by a lack of evidence-based guidance to mitigate safety concerns such as overwork weakness. Among patients, limited ability to perform at a specified training level, decreased motivation, and fatigue were also identified as major hurdles. 54 These challenges highlight the need for clearer guidance, practical tools, and evidence that exercise can be dosed and monitored as rigorously as any other clinical intervention. Addressing these barriers requires a shift toward individualized, realistic planning that accounts for physical, social, environmental, and cognitive constraints. This multidisciplinary framework aligns clinical management with the patient's functional level and lifestyle to ensure sustained adherence.
Monitoring and measuring exercise
Translating exercise interventions into routine care, requires practical tools for monitoring safety, effectiveness, and progression beyond the current functional outcomes. Standard strength and function tests are still cornerstones, but each has limitations. Although access to CPET is limited, it is valuable and relevant to DMD/BMD because it can identify physiological limitations as well as secondary deconditioning, an often-overlooked determinant of exercise tolerance. By quantifying these baseline characteristics, clinicians can personalize prescriptions that reflect both the patient's disease stage and their current functional level, ensuring the program is tailored to maximize individual benefit. This information also helps patients monitor intensity more accurately, supporting their adherence to safety parameters while maximizing efficacy. Practical recommendations include activity calendars, heart rate bands/watches, and the Talk Test (able to talk but not sing) to gauge moderate exercise intensity. This provides accessible metrics to help guide safe exercise dosing and progression. Additionally, fit-for-purpose remote measures such as physical activity monitors and wearables offer a practical and valuable means for patients to track and compare their own progress over time. Taken together, these modalities allow clinicians to begin applying the FITT-Volume, Progression (FITT-VP) framework in practice. 32
Developing a home exercise program
From a clinical standpoint, exercise should be regarded as a key component of overall health in DMD and BMD. Before starting any exercise program, patients should undergo physician clearance, including cardiac evaluation. Interventions should begin conservatively “start low 55 and go slow” with gradual progression as tolerated. Even small amounts of consistent activity can be beneficial, particularly when activities are meaningful and enjoyable to patients, which should improve adherence. While the published guidance (e.g., 30 min of moderate aerobic activity 5 days per week plus resistance training twice weekly) can seem daunting, even cumulative bouts of 20 min spread across the day confer meaningful benefit. 56 The key is to avoid inactivity, which remains highly prevalent among people with disabilities. A home exercise program should follow the FITT-VP framework, while emphasizing fatigue management, energy conservation, frequent rest periods to prevent over-exertion, and quality of movement over quantity.
Clinicians should also be mindful of disease stage, degree of deconditioning, and the need for adaptations. Preparing the body through stretching, passive range of motion, or massage may improve comfort and readiness to exercise. 57 Clinicians are also encouraged to leverage community and accessible technologies to improve adherence: online resources (e.g., National Center on Health, Physical Activity and Disability [NCHPAD]), adaptive equipment (such as assisted cycles or low-cost hand supports), and collaborations with personal trainers or community programs that provide social reinforcement. Assistive devices such as the Neater Arm Support (Neater Solutions, UK) can double as both functional and exercise tools, sometimes offering greater improvements in function than costly drug therapies.
Early supervision is often essential to ensure both safety and compliance, especially as patients and families adapt to new routines. Practical strength regimens may include isometric exercises performed two to three times per week at moderate-intensity, or progressive resistance programs beginning at low load with cautious progression. For children, incorporating elements of play or gamification (e.g., integrating iPad breaks) can help sustain participation over time. The goal is to balance safety with therapeutic benefit, providing structured activity that maintains function and quality of life while minimizing the risk of injury.
Exercise recovery is an essential but under-recognized part of a home exercise program. Compromised recovery can prolong fatigue and hinder adaptation, so knowing how patients return to baseline is critical. At Stanford, Dr Duong's group compared recovery dynamics in individuals with neuromuscular disease versus healthy controls, 58 finding significantly blunted and delayed recovery responses following exercise—underscoring that boys with DMD recover physiologically and functionally at a significantly different, slower rate than their peers. Further research is needed to guide more precise recommendations on the timing and duration of recovery in this population.
Overall assessment and setting priorities
Collecting information - holistic approach
To weave these threads into practice requires a solid understanding the pathophysiology and the exercise physiology of dystrophinopathies. With that foundation comes the therapist's challenge of bridging the gap between the research setting and clinical practice—drawing on established clinical skills to provide care to individuals with neuromuscular conditions that may be less familiar. In doing so, many skills honed with other populations could be further mastered when applied in DMD/BMD using the principles shared at the meeting, allowing more precise individualization of care. Clinicians should collect information holistically, while building rapport, for each individual with DMD or BMD and their families, to develop a comprehensive overview of their current situation. Recognizing the multisystemic nature of dystrophinopathies and the spectrum of disease, it is essential to understand where patients are in their care and what they know about their condition.
Before detailed assessment, clinicians should find out what brought the patient in to set the stage for the time spent together. Is the patient receiving multidisciplinary care, and if so, which specialists are involved? Knowing the names and contact information of cardiologists, pulmonologists, neurologists, and coordinators can help therapists avoid working in isolation and bridge the knowledge gap on the latest medical updates. It is also important to note participation in a clinical trial or a natural history study, as this may influence both expectations and available resources. All this information can be gathered organically over the course of a visit, alongside routine clinical assessments such as range of motion. Treating the patient as a whole rather than as a collection of body parts allows the therapist to make a connection vital to building trust.
Regardless of the patient's age, therapists should document daily routines and family structure to understand where exercise might realistically fit. Practical questions include what time their day begins, school or work schedules, typical physical activity in a day (walking distances, prolonged sitting or periods of both, etc.). Family arrangements for children—such as whether parents are separated or whether caregiving rotates—can affect consistency. For adult patients, does the person live alone or with someone? Learning strategies, behavioral issues, fatigue patterns, a child's play preferences or adults’ leisure activities all provide context for designing an exercise program that will be both sustainable and enjoyable. Therapists can also help families and individuals structure snack and hydration breaks to support exercise and avoid fatigue — important for both children and adults. Exercising muscle requires fuel so diet is an important topic to discuss. This is also an appropriate time to note behavioral challenges in children and how these are managed at home. Observations of family dynamics and the patient-therapist interaction during the assessment will provide valuable context for successful team building and should begin to shape the management approach during treatment.
Therapists should determine whether accommodations have been made at home, school, or in the workplace. Understanding support systems is critical: do they have local friends or relatives who can provide help if needed? Activities of daily living (such as eating, drinking, showering, and dressing) should be explored to gauge independence and identify needs for adaptation. Together, these details both shape therapy goals and enable therapists to fit exercise into routines that are realistic and aligned with each person's circumstances and personal goals.
Several factors cut across both pediatric and adult populations. Insurance status is an essential consideration, since coverage depends on documentation and coding. Medications (cardiac and others), supplements, nutrition, hydration, and sleep all affect exercise tolerance and recovery, and each should be addressed explicitly. Asking about adaptive and electronic equipment can uncover other needs, while questions about past and current exercise routines can guide program design. Quality of life and psychosocial wellbeing should be kept in mind throughout interactions, since these shape motivation and engagement as much as any clinical measure. Clinicians can weave questions related to mental wellness into the general conversation—such as “how well do you sleep,” “what is your favorite food,” “what do you like to do in your spare time,” “do you have time for exercise,” “are you exercising,” “do you ever get anxious?” 59 Careful listening can reveal surprisingly useful information.
Clinical evaluation – setting priorities
In Dr Senesac's experience, the clinical evaluation of patients with DMD/BMD should begin with close observation of movement and transitions. Watching how patients move through space, plan and sequence tasks, and control their joints can reveal as much as formal outcome measures. Therapists should note when assistance is needed and recognize the predictable patterns of weakness seen in dystrophinopathies, especially around the pelvis, shoulder girdle, and trunk. For those new to the field, video resources from PPMD, Child Muscle Weakness, and ImagingNMD can provide useful reference points for identifying these characteristic patterns (see Table 1: Supplemental Online Resources).
Supplementary online resources.
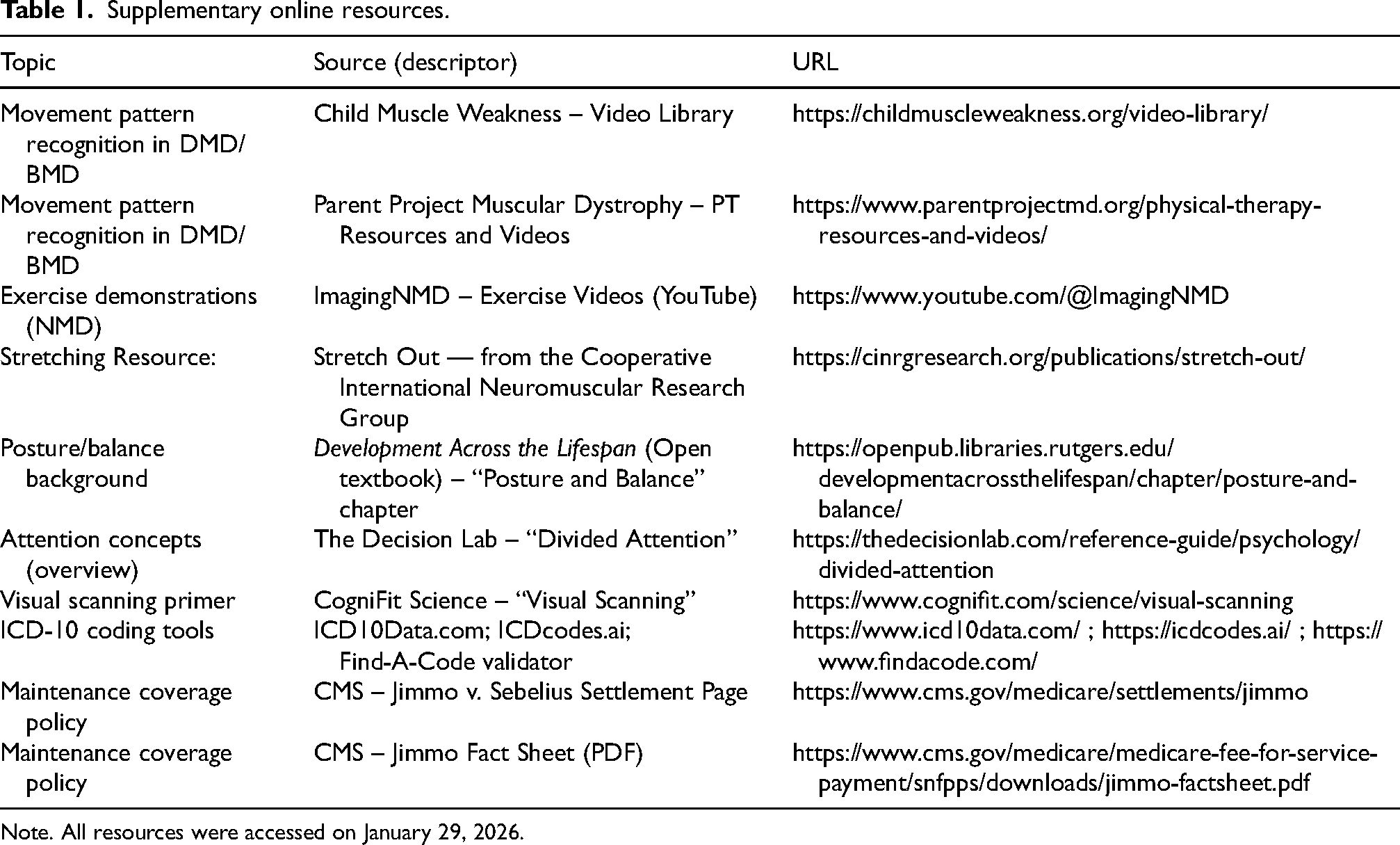
Note. All resources were accessed on January 29, 2026.
In addition to the standard outcome measures used with patients with BMD and DMD (see Figure 1), there are several screening domains that can shape therapy plans for individuals with dystrophinopathies:
Understanding the way a person functions in an environment through movement and through processing skills can help the therapist in building exercise programs for success by providing an integrative whole approach beyond skeletal muscle weakness.
Navigating insurance
Billing insurance relies on documentation of assessments and measurable goals in a way that supports sustained coverage. For patients with DMD or BMD in the United States, the primary diagnostic code is G71.1, typically accompanied by secondary or tertiary ICD-10 code such as M62.81 (muscle weakness, balance/coordination) or R26.89 (gait instability, postural weakness, toe walking) (see Table 1). To ensure reimbursement, the evaluation must clearly link these codes to measured outcomes and written goals—for example, documenting weakness in the assessment, use of acceptable outcome measures, and setting goals for improvement. Measurable progress is essential for continued coverage (progress can often be “slowing decline”), and therapists should explicitly state that the patient would benefit from skilled Physical Therapy or Occupational Therapy services. Small, incremental goals are more defensible and reminded participants that under the Jimmo v. Sebelius ruling 2013, maintaining function against expected decline also qualifies as improvement. In other words, document medical necessity of services for maintenance or slowing decline of the condition and get the referring physician's signature. Insurers are increasingly receptive to this approach (see Table 1).
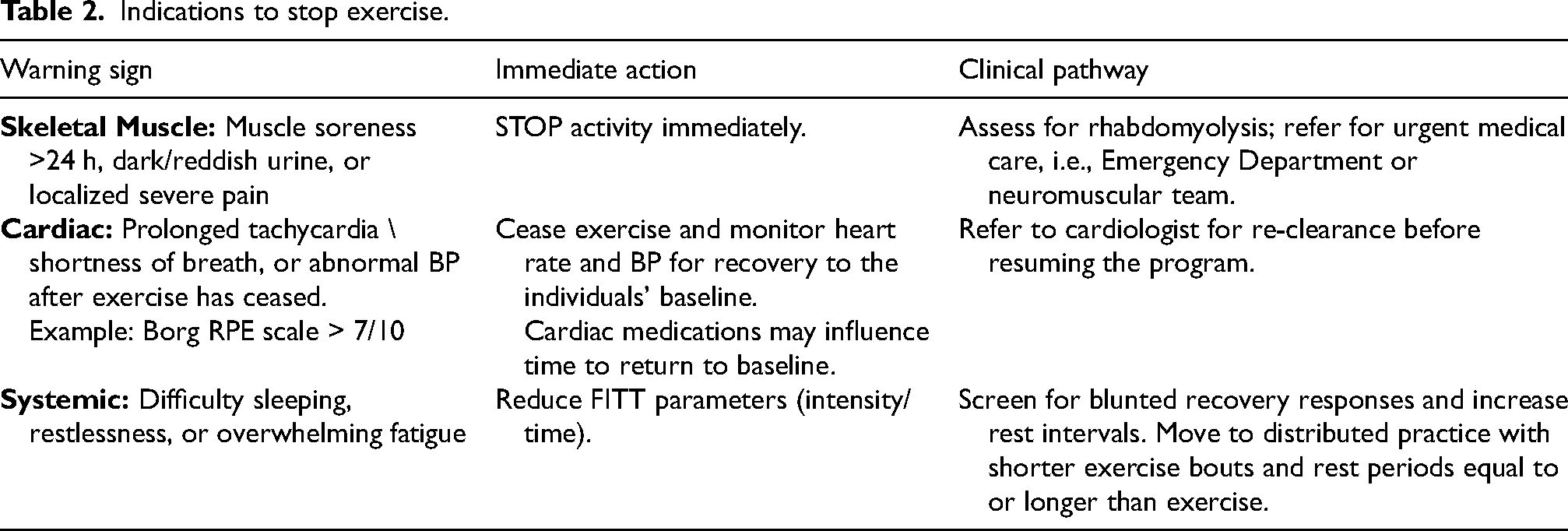
Indications to stop exercise.
Consensus regarding exercise for individuals with dystrophinopathy.
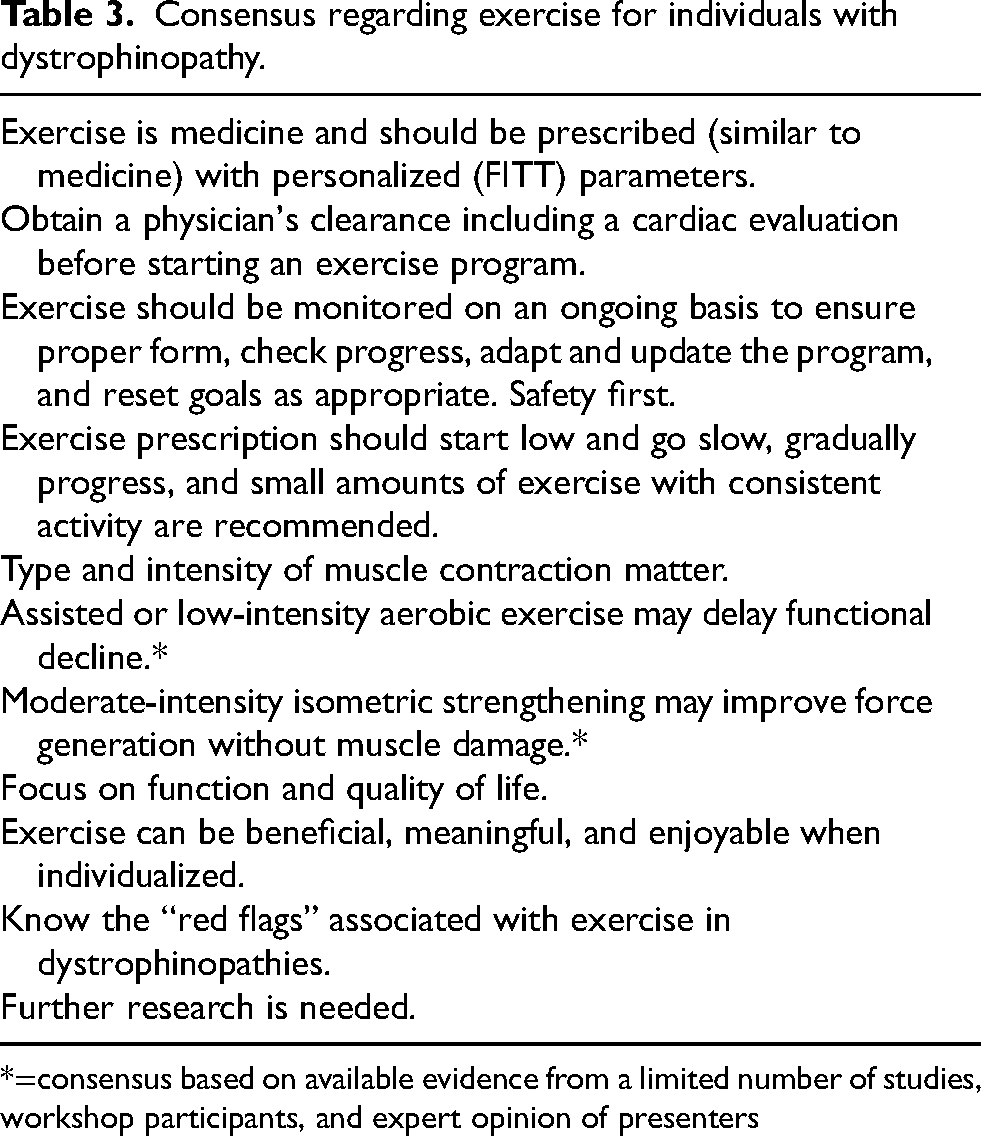
*=consensus based on available evidence from a limited number of studies, workshop participants, and expert opinion of presenters
Safety thresholds and red flags
Finally, before specifying dose and progression, programs should be gated by clear safety thresholds. It is particularly important to monitor heart rate and identify early warning signs that indicate overexertion, exercise progression too difficult, or inadequate recovery, including overwhelming fatigue, pain during or after exercise, or muscle soreness lasting more than 24 h after exercise; difficulty sleeping or restlessness (inability to get comfortable); prolonged shortness of breath or tachycardia (rapid heart rate) after exercise; abnormal blood pressure responses for the individual; and most seriously, dark or reddish-brown urine suggesting possible rhabdomyolysis. Rhabdomyolysis, while rare at low activity levels in typical populations, may occur disproportionately in BMD or DMD individuals after low to modest exertion and usually presents with muscle pain, weakness, in addition to dark urine. 62 To ensure safety, clinicians should implement a ‘Stop-and-Escalate’ protocol triggered by these specific clinical indicators (see Table 2). Under this framework, immediate cessation of activity and specialist assessment are required and should prompt cessation of exercise, or an immediate reduction in intensity and a reassessment of recovery intervals.
Bringing it all together for the clinic
The current understanding of exercise in dystrophinopathy is to begin at low intensity and build up gradually, with current but limited studies demonstrating aerobic and isometric strengthening benefit muscle endurance and strength. Clearance from a physician is essential before initiating any program, to confirm cardiac safety. Given impaired physiological responses to the increasing oxygen demands associated with physical activity and exercise, applying the FITT principle is critical to design dynamic exercise programs that safely overload the system at submaximal levels readily available in clinics and at home. Monitoring these programs not only ensures safety but also provides information that families can use to anticipate future needs, while documenting measurable progress toward patient goals. Patients can also learn to monitor their own exercise and health.
The workshop underscored both the challenges and opportunities in exercise prescription for dystrophinopathies. Discussion was initiated after each topic with expert opinions of presenters and participants to reach a consensus on key factors regarding exercise with individuals with dystrophinopathy. Each time the clinician sees the patient is an opportunity for ongoing evaluation and observation—tracking signs of success while remaining alert to red flags. The meeting emphasized that careful monitoring and incremental goal setting are key to successful exercise programs for people with DMD/BMD. In addition, adhering to principles established through our understanding of pathophysiology, the exercise literature in dystrophinopathies, and general exercise guidelines is important for establishing effective exercise programs that are individualized and sustainable for individuals with dystrophinopathies (Table 3).
Further work needs to be done in exercise in dystrophinopathies however, we now have a starting point to strategically prescribe exercise under supervision. Moving forward, it will be critical that further verification explore the long -term effects on skeletal muscle, cardiac function over several years, optimal intensity/dose, and stage-specific protocols. Future studies should branch out to non-ambulatory individuals and carriers which present other challenges.
Footnotes
Acknowledgments
We thank Theodore Smart for writing assistance and manuscript preparation, and Lance Sherriff for transcription and editing assistance; both received payment for their services from Parent Project Muscular Dystrophy (PPMD), which also convened the meeting. We also express our appreciation to Merrill Landers, PT, DPT, PhD; Lisa Taylor, PT, DPT, PCS; Ryan Resnik, PT, DPT; the Department of Physical Therapy at the University of Nevada, Las Vegas; Rifton Equipment (New York, USA); and Caesars Entertainment for the loan of exercise equipment used in the interactive meeting.
TD: Advisory board: Actigraph, Biogen, Scholar Rock, Roche, Novartis, Dyne, PPMD, CureDuchenne, CureSMA, Catalyst
Consultancy/speaker: Sarepta, Biogen, Somite, Roche, Dyne, Astellas, Trinds, NMDPharma, Novartis; Received research support from Biogen, Ionis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Parent Project Muscular Dystrophy (PPMD) provided funding for the meeting, including covering the travel and hotel costs for faculty as well as for the patients participating in workshop demonstrations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.