
Abstract
Infants with severe neuromuscular disorders, presenting a birth, are often unable to move, communicate, breathe, and feed. Unlike infants with severe birth asphyxia and cerebral palsy, these neuromuscular conditions are often associated with presumed normal cognition. Supporting these very severely affected infants and maintaining life through medical intervention or re-orientating care to palliation is often debated, and decision-making can be extremely challenging. Although guidelines exist to help navigate this process (Nuffield Council of Bioethics and Royal Collage of Paediatrics guidelines) deciding what is in the child's best interest is fraught with difficulties. This article explores some of the unique issues that arise in infants with severe neuromuscular conditions and illustrates the challenges in determining best interest for these patients, using some of the cases in the legal literature and the authors personal experience.
Introduction
Infants born with some severe neuromuscular disorders are usually extremely hypotonic and weak and present with the inability to move, breathe, feed or communicate. What is unique about these conditions is that they are usually considered to have normal cognition in contrast to other infants, who present in a similar fashion but with an encephalopathy, where brain damage has occurred and there is little prospect of normal cognition.
In order for these infants to survive, a medical intervention, usually in the form of airway support, assisted ventilation and tube feeding will be required. The question that often arises is whether it is in the infants’ best interest to continue to receive medical intervention. This question is almost always challenging and often the answer lies in drawing up a balance sheet of benefits and dis-benefits/ burdens a of medical intervention.1,2 There is a wide body of literature addressing the exact nature and nuance of the best interest query3,4 which could lead to disagreements between treating clinicians and parents. Further difficulties in decision making may arise if there are also social, familial or religious dimensions to consider. This situation can exceptionally result in the conflicting parties making an application to the Courts for help in finding a way forward. 5
In the last decade a number of high-profile cases have come before Court which have generated a considerable amount of public interest. The cases of Charlie Gard, Tafida Raqeeb, Pippa Knight, Alta Fixsler and Archie Battersbee b have had major implications for case law and for paediatricians. A detailed review of these cases has recently been published in a Nuffield Council of Bioethics review by Kirsty Moreton c .
It can be argued that an important distinction needs to be made when undertaking the exercise of ascertaining best interest and calculating the benefits and burdens; the distinction being the degree of cognitive damage the infant brain may have sustained or whether cognition has remained intact. If the infant has brain damage and has severe cognitive involvement then usually the burdens of continued survival with medical intervention are said to be greater. This seems to be the case in that it appears to be widely thought by clinicians (and Courts) d that continued life sustaining treatment is less likely to be in an infant's best interests. However, in such cases it is not necessarily that the burdens of continued life are greater, rather that the benefits of continued life are so much less. 3 However, if cognition is said to be preserved then it can be argued that the benefits of continued life are greater but also conversely one may be able to experience the disbenefits or displeasures (usually considered to be pain and discomfort) of continued life. This argument is incorporated in the RCPCH framework e . There exists an entire body of ethical argument, surrounding death and disability, 6 which is in support of this line of thinking f .
Considerable weight is often given to the concepts of ‘futility’ and ‘lack of purpose’, although it is acknowledged that such terms can be problematic. An example of this is evidence from other countries, where it is certainly not technically futile or lacking in purpose (such children can live for many years and have lives that they themselves regard as worth living). It is therefore perhaps appropriate that the most recent RCPCH guidance 7 does not use either term.
There is a tolerability paradox 4 to consider, which states “that beyond a certain point more severe degrees of cognitive impairment may make life more tolerable rather than less tolerable”. In contrast, children with certain neuromuscular conditions, in whom cognition may be normal, the concept of suffering,8,9 or perhaps the uncertainty about the level of suffering, should be given much more weight in the calculation of the burdens.
It is important to recognise that since 2017, the advent of disease modifying treatments for SMA, 10 has resulted in paradigm shift of our consideration of the ‘best interest’ question. Prior to 2017, infants with SMA type 1 would virtually all die without medical support, 11 and the best interest question would maybe have to be determined by a court order. However, since 2017 and the introduction of disease modifying treatments, SMA still remains incurable but is no longer considered untreatable. This paper considers three historical cases involving infants affected by neuromuscular conditions.
Illustrative cases
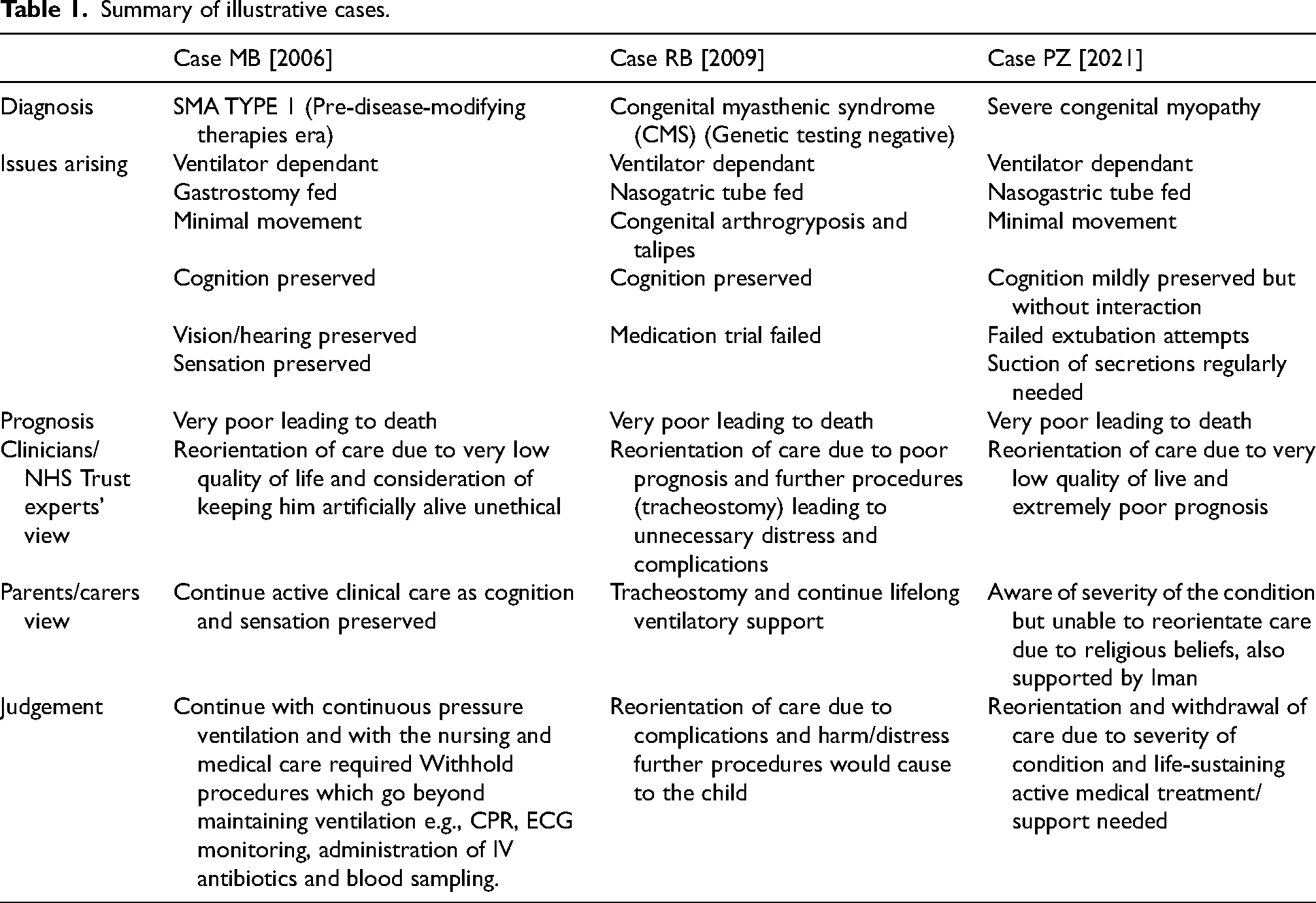
We present three cases involving patients with severe neuromuscular conditions that raise the issues and challenges clinicians face regarding best interest for these patients. A summary of the three cases is presented in Table 1.
Summary of illustrative cases.
Case MB g [2006]
Case summary
MB was diagnosed with Spinal Muscular Atrophy type 1 (SMA1). SMA is degenerative and progressive disease and in 2006 (pre-treatment era) this condition was considered life limiting. SMA type I infants would usually die by two years of age and death was inevitable without artificial ventilation.
MB was aged 18 months at the time of the application; MB's clinical condition was said to be extremely severe. MB had minimal movement of his eyes only. MB required positive ventilation via an invasive endotracheal tube; could not swallow at all and was fed through a gastrostomy tube. MB remained conscious, with a retained sleep-wake cycle. It was assumed that MB continued to be able to see, hear, to feel touch, and to have an awareness of his surroundings and the people most close to him. MB was thought to have normal thought processes. Although MB was able to make some very limited voluntary responses to environment, he was not able to make his wishes desires and choices known.
There was a presumption of normal cognitive function, as this is usually the case in SMA type 1, but it was considered very difficult to assess objectively. MB was not considered to have had any brain damage. It was felt that MBE would experience some discomfort and distress as interventions particularly blood sampling, deep endotracheal suction, physiotherapy and bagging are considered very uncomfortable. Reactions of distress and pain in that his heart rate would suddenly rise and he would produce tears.
Assessment of quality of life was very difficult. Prognosis was considered very poor and death inevitable. The journey ahead of MB was full of potential complications related to his condition.
Issues arising
The medical evidence suggested that although ventilation was keeping him alive, it was not restoring his health. All treatments were futile and would not have change the outcome. The treating team and the experts all agreed that withdrawing ventilation and re-orientating to palliative care would be in his best interest.
The benefits were considered as follows: MB had always been conscious and attained an age of 18 months old. It was assumed that MB had normal, age-appropriate cognition, power of thought and capacity for moods and emotions and feel pleasure from stimuli. MB could hear and see. MB did follow movement and was able to focus on objects or people of interest. MB could feel touch, and according to the parents could experience some pleasure.
The burdens were considered as follows: MB was being exposed to discomfort, distress and pain, due to the fact that he needed intensive care support. MB underwent medical procedures periodically which caused pain. MB was considered to have been in constant discomfort from the presence of an ET tube and localised infection around it. MB's inability to communicate, coupled with the vast range of early childhood pleasures/ moods /emotions which he was not able to experience (e.g., crawling, exploring, walking, etc) would have been hugely frustrating.
The NHS Trust considered quality of life for MB was so low and the burdens of living to be so great that it was unethical to continue to artificially keep him alive. They made an application to the Court to allow for the ET tube to be withdrawn which would have led to MB's death. MB's guardian-ad-litem's view supported the treating clinicians and experts in that it was not in MB's best interests for his life to continue to be artificially prolonged. MB's parents’ views were not in agreement with the Trust or the Guardian.
Judgement
The Judge was not persuaded even considering predicted future deterioration; he went further and considered that at the time it was positively in his best interests to continue with continuous pressure ventilation and with the nursing and medical care required.
The Judge did consider it to be in MB's best interest to withhold procedures which go beyond maintaining ventilation e.g., CPR, ECG monitoring, administration of IV antibiotics and blood sampling.
The parents had further applied for the doctors to undertake a tracheostomy (which the clinicians opposed). This application was dismissed as it was felt not to be a matter for the court but one for further discussion between doctors and parents.
In a commentary h by Jonas regarding baby MB, she considered medical decision making difficult in the context of uncertain infant suffering.
Case RB i [2009]
Case summary
The case RB was of a 10-month-old boy who had been born with profound muscle weakness, hypotonia, facial weakness, bulbar dysfunction, congenital arthrogryposis, very poor respiratory effort and talipes in the lower limbs and was ventilator dependent since birth. RB had multiple failed extubating attempts due to poor respiratory effort and copious secretions. Elective endotracheal tube changes resulted in collapse and the airway was deemed to be difficult to manage.
RB had a suspected clinical diagnosis of Congenital Myasthenic Syndrome (CMS) but a genetic cause was never found. Empirical trials of medications (Pyridostigmine, Ephedrine, and 3,4-Diaminopyridine) were conducted and showed no noticeable clinical change in RB.
By four months of age, it was clear that RB was not making any progress and would need to have full intensive care support to survive. This eventually led to different management options: a) Long term nasal endotracheal ventilation and PICU admission for the remainder of his life, b) Insertion of a tracheostomy and lifelong ventilation which would require an intensive care management package for home with support from domiciliary staff or c) reorientation of care towards palliation.
Issues arising
The medical and expert evidence suggested that it was not in RB's best interest to proceed with long-term ventilation and tracheostomy as was considered to be adding to his distress. All medical treatments had been tried and did not show any benefit for RB. The treating team and the experts agreed that withdrawing ventilation and re-orientation to palliative care would be in his best interest. RB's Guardian's views supported treating clinicians and expert's view.
In considering the RB's long-term best interest there emerged a difference in opinion between the parents and the treating medical staff. His parents preferred the option of a tracheostomy and lifelong ventilatory support; therefore, an application was made to the Court.
Judgement
In court, when the evidence was given, it was felt to be very strongly in favour of withdrawing care from RB and reorientation to palliative care. The parents eventually decided not to challenge the overwhelming medical view and position. The Judge therefore gave words of endorsement supporting the decision by the parents to no longer challenge the medical position.
In his judgement the issues that arose were firstly a clear recognition of the life RB would have experienced had he continued on the ventilator or received a tracheostomy j .
Case PZ k [2021]
Case summary
PZ was born with a severe congenital myopathic condition which resulted in significant hypotonia and muscle weakness. She was unable to move independently, communicate, swallow or cough. Through further genetic testing a gene mutation was found which confirmed the diagnosis. The prognosis was grave, especially as it had presented in the neonatal period. It was accepted that her condition would not improve, would continue to deteriorate and would ultimately, be life limiting. It was thought that PZ was cognitively aware but it was difficult to identify when she was in distress, other than by signs of an increased heart rate or when tears were observed.
She had care in the neonatal intensive care unit and required mechanical ventilation, tube feeding and regular suctions of secretions due to her inability to swallow or cough. All attempts to extubate PZ had been unsuccessful. PZ remained unable to communicate.
Many of PZ's procedures in the neonatal unit, such as suctioning, intubation, change of ET tube, intravenous cannulation and blood investigations, were observed to cause her pain and discomfort.
Issues arising
The parents agreed with the medical diagnosis and prognosis for PZ but felt very strongly that she should continue to receive the life sustaining medical treatment in accordance with their strong religious beliefs.
Judgement
The judgement was guided by what was considered to be in PZ's best interests, having regard to what her views may have been, her parent's wishes, including their religious and cultural beliefs (The advice of several Imams was taken into consideration), the benefits and burdens as a consequence of her medical condition and the views of her treating doctors. There was a strong presumption to preserve life. PZ's Guardian undertook a detailed assessment and sought the views of the infant, parents and the medical team.
The judgement concluded that it was in PZ's best interests for life-sustaining medical treatment to be withdrawn, and for a palliative care regime to be implemented.
Discussion
The key medical issue that arises from these cases are the severe neuromuscular conditions which have led to profoundly weak infants who are not able to move, communicate, feed, breathe or clear their own secretions. These disorders did not have a prospect of improvement or cure at the time of discussion. All these infants could have their life sustained through modern intensive care management with invasive ventilation, insertion of a tracheostomy, feeding through a tube and active management of secretions. The question that then arises is whether survival at all costs should be offered to these infants.
The infant with SMA, was from 2009 (pre-disease modifying treatment era). Since 2017, the management of SMA has gone through a paradigm shift as new treatments have emerged which have been very successful in changing the severity of the condition. 12 It is still however true, that despite these new treatments, SMA has not been cured but only made it milder with better survival. This presents us with a new possibility and dilemma in the management of SMA (especially severe SMA type 0 or 1) which, to our knowledge has not yet been challenged in court.
One of the other issues that frequently arises in such infants is about the futility/no purpose of any proposed medical intervention. The RCPCH guidelines 7 suggest that continuing medical intervention in the context of futility/no purpose will lead to increase in the burden (suffering, costs) faced by all parties concerned.
In the intensive care setting the management of these infants readily require their airways to be supported and for invasive ventilation to be commenced. The prospect of a long-term solution for ventilation, a tracheostomy, is often raised but it is considered a ‘red line’ by paediatric respiratory specialists. There is a perception that this may convert a reversible situation (where the prospect of a one-way extubation and reorientation to palliative care remain viable) to a situation which is irreversible. 13 This perception is however entirely unfounded and ethically incorrect. There is no fundamental barrier to providing palliative care to patients with a tracheostomy, including patients who are on a ventilator. Patients who are permanently ventilator dependent, such as children with neuromuscular disorders, can have ventilation weaned or stopped with provision of comfort treatment. This is a common occurrence in many NICUs l .
Perhaps uniquely in severe neuromuscular conditions is the fact that cognition may be preserved. This can then lead to a scenario where the infant is effectively ‘ locked in’ and experiencing stimuli, both pleasant and painful, without being able to respond to it. This is not something that it is usually considered in the context of severe hypoxic- ischaemic or acquired brain injury where there may be a very limited or no ability to experience stimuli in the first place.
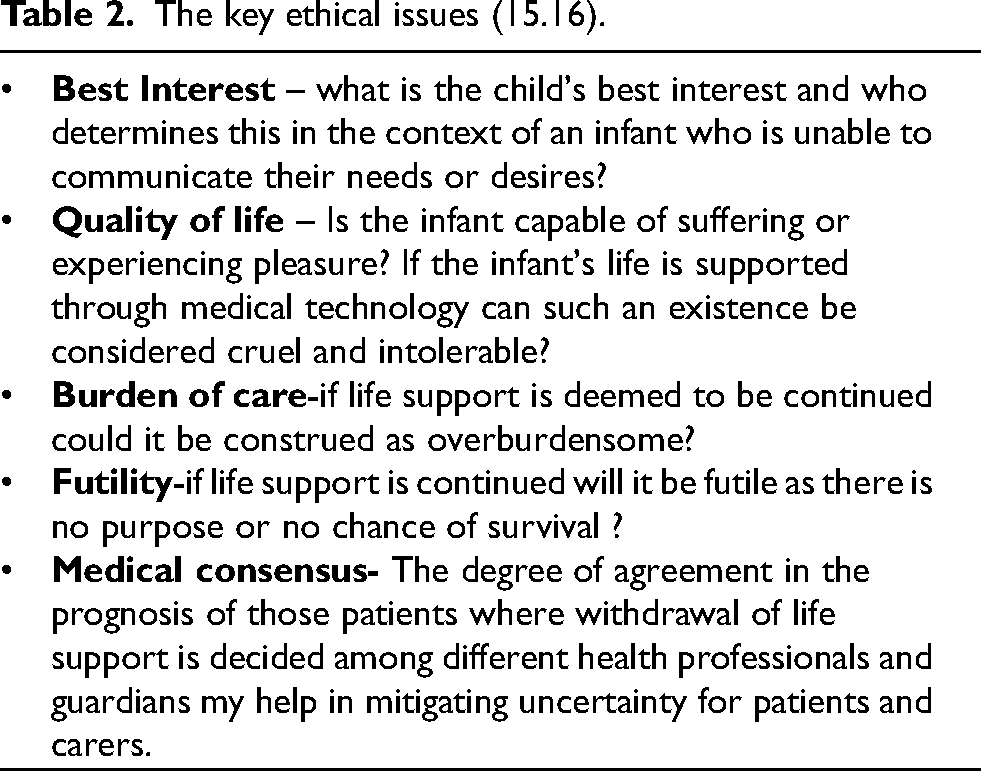
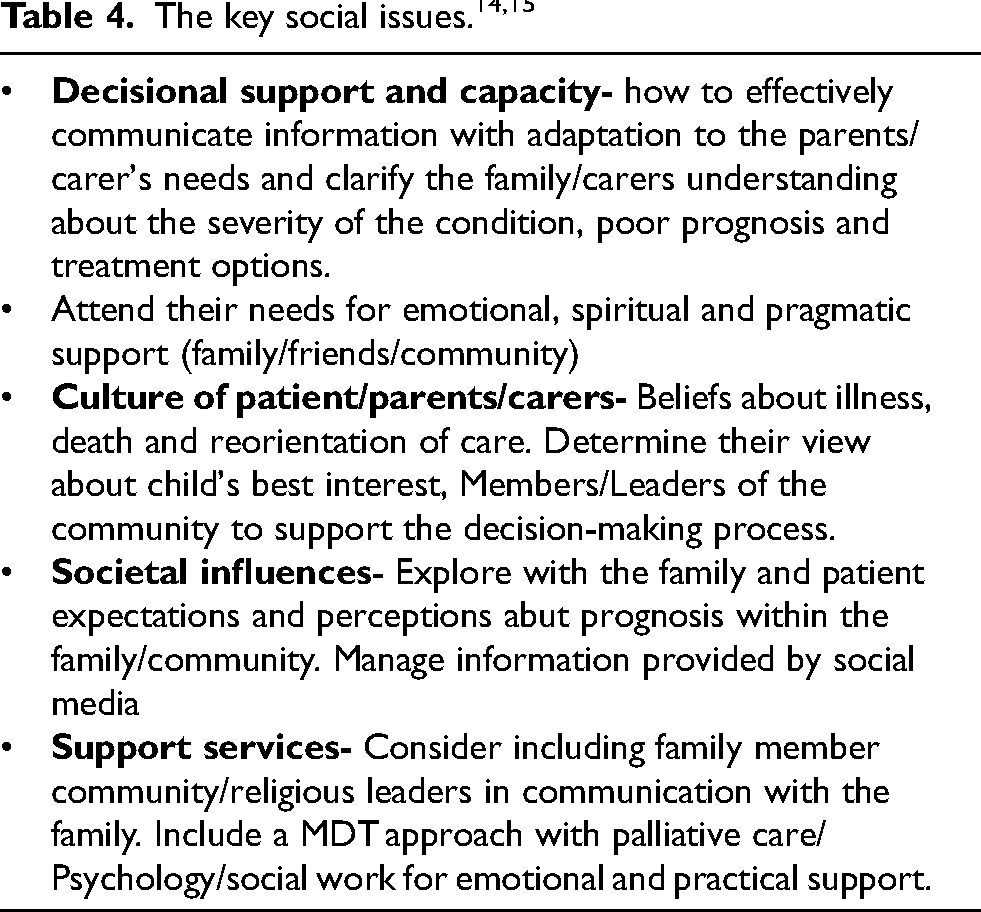
Due to the challenges in the management of this patients different ethical, legal and social aspects (Tables 2–4) need to be consider prior to discussion regarding limitation of therapy or withdrawal of life support.14,15
The key ethical issues (15.16).
The key legal issues (UK).
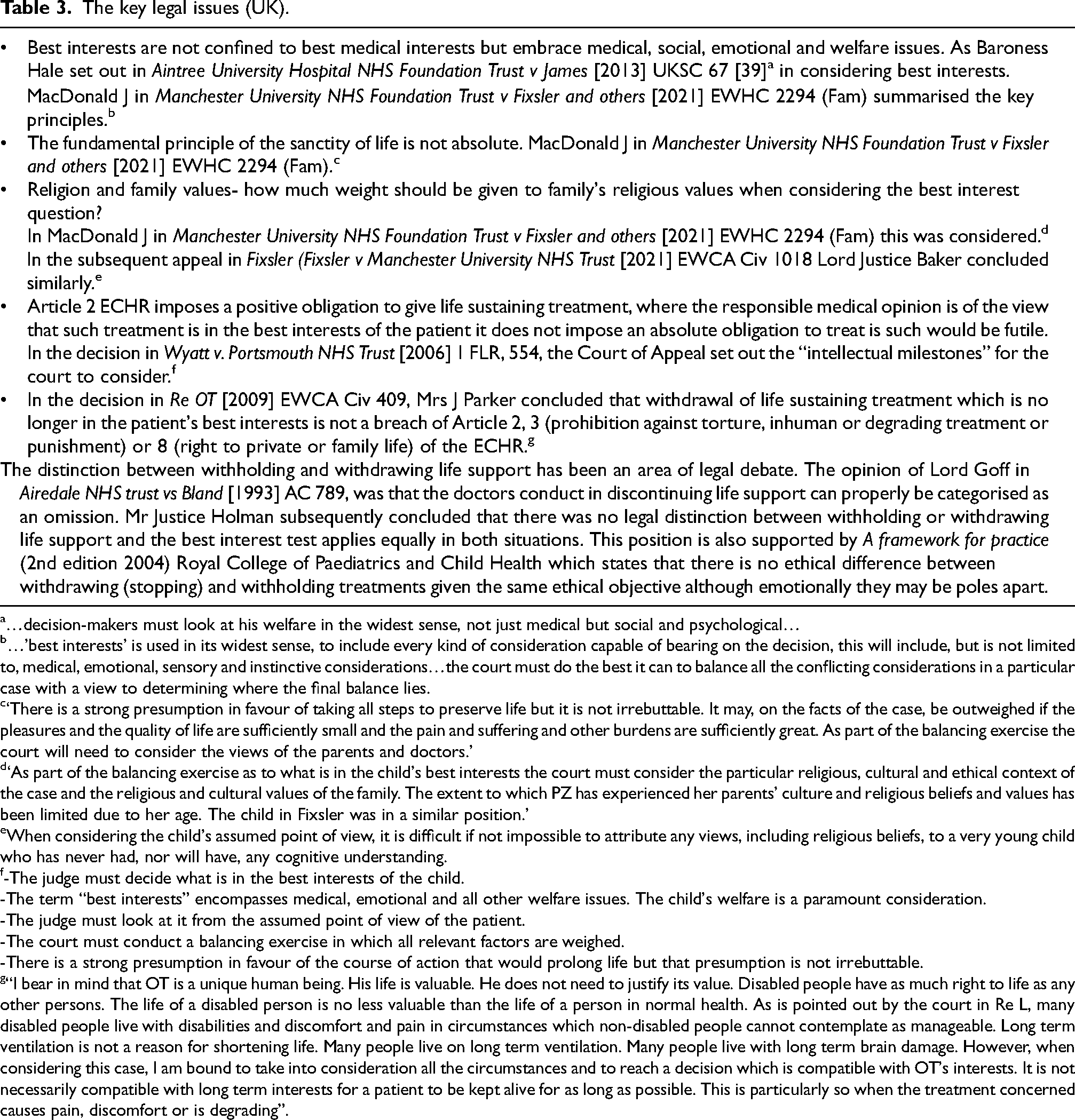
…decision-makers must look at his welfare in the widest sense, not just medical but social and psychological…
…’best interests’ is used in its widest sense, to include every kind of consideration capable of bearing on the decision, this will include, but is not limited to, medical, emotional, sensory and instinctive considerations…the court must do the best it can to balance all the conflicting considerations in a particular case with a view to determining where the final balance lies.
‘There is a strong presumption in favour of taking all steps to preserve life but it is not irrebuttable. It may, on the facts of the case, be outweighed if the pleasures and the quality of life are sufficiently small and the pain and suffering and other burdens are sufficiently great. As part of the balancing exercise the court will need to consider the views of the parents and doctors.’
‘As part of the balancing exercise as to what is in the child's best interests the court must consider the particular religious, cultural and ethical context of the case and the religious and cultural values of the family. The extent to which PZ has experienced her parents’ culture and religious beliefs and values has been limited due to her age. The child in Fixsler was in a similar position.’
When considering the child's assumed point of view, it is difficult if not impossible to attribute any views, including religious beliefs, to a very young child who has never had, nor will have, any cognitive understanding.
-The judge must decide what is in the best interests of the child.
-The term “best interests” encompasses medical, emotional and all other welfare issues. The child's welfare is a paramount consideration.
-The judge must look at it from the assumed point of view of the patient.
-The court must conduct a balancing exercise in which all relevant factors are weighed.
-There is a strong presumption in favour of the course of action that would prolong life but that presumption is not irrebuttable.
“I bear in mind that OT is a unique human being. His life is valuable. He does not need to justify its value. Disabled people have as much right to life as any other persons. The life of a disabled person is no less valuable than the life of a person in normal health. As is pointed out by the court in Re L, many disabled people live with disabilities and discomfort and pain in circumstances which non-disabled people cannot contemplate as manageable. Long term ventilation is not a reason for shortening life. Many people live on long term ventilation. Many people live with long term brain damage. However, when considering this case, I am bound to take into consideration all the circumstances and to reach a decision which is compatible with OT's interests. It is not necessarily compatible with long term interests for a patient to be kept alive for as long as possible. This is particularly so when the treatment concerned causes pain, discomfort or is degrading”.
These infants and the dilemmas that they present us with, brings to light the relationship between the paediatrician, the parent and the court. As stated by Lord Donaldson in Re: J (A Minor) (Wardship: Medical Treatment)[1991] 1 FLR 366: “no one can dictate the treatment to be given to the child – neither the courts, parents nor doctors. There are checks and balances… The inevitable and desirable result is that choice of treatment is, in some measure, a joint decision of the doctors and court or parents.”
If the situation is such that there is a disagreement about treatment options between the doctors and parents, then the concept of ‘the doctor's conscience’ needs to be considered. There is a large body of literature m , which considers these disagreements that may arise. The judgement of Mr Justice Sedley in the case of Charlotte Wyatt (2005) EWHC 2293, considered that a doctor could not be required to act contrary to his conscience.
In the opinion paper by Powell 8 discusses the judgment of Mr Justice Holman in the case of MB[2006] EWHC 507(Fam) and how it had raised concerns amongst paediatricians at the time that they would be compelled to treat a child against their conscience. His paper cites the well-known judgements of Lord Donaldson in Re J (A Minor) (Wardship: Medical Treatment)[1991] 1 FLR 366 and judgment of Mr Justice Sedley in the case of Charlotte Wyatt [2005] EWHC2293 (Fam) n .
Although it is beyond the scope of this manuscript, the economic aspect of the end of life and palliative care in those children and adolescents with complex clinical conditions is a factor to consider.
In this sense, some studies have found evidence that palliative care at the end of live has a reduction in health costs, indirect savings by protecting the patients from undergoing procedures or surgical interventions that can lead to suffering at the end of life without any clinical benefit.16,17 Nevertheless, the economic studies regarding palliative care and end of life have several limitations due to the ethical impossibility of being prospective, higher costs in complex palliative patients compared to the control group, different ways of providing palliative care and the uncertainty of the end-of-life period that can vary from minutes to days.16,17
Conclusion
Children with severe neuromuscular conditions who present to our neonatal units needing full intensive care support, where the lack of prospect of improvement and where cognition is said to be intact, provide the parents and medical team with enormous challenges. Often these situations will lead to differences in opinion and conflicts in determining what is in the infants’ best interest. Sometimes, they can be irreconcilable which usually results in an application to the Court.
In this context, the medical, social and ethical frameworks should be considered, together with the concept of possible suffering by the infant due to preserved cognition, in order to determine what is truly in the infant's best interest. Further consensus in how to manage these patients along with clear guidelines should be implemented by the different health boards to facilitate decision making by different professionals.
Footnotes
Abbreviations
Acknowledgments
I am grateful to Dr T Hilliard, Dr P Cairns, Miss H Squires, Professor D Wilkinson, Dr P Jardine and Dr L Rosenbloom's comments on this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.