
Abstract
Background:
Approved disease modifying treatments (DMTs) and the implementation of newborn screening for spinal muscular atrophy (SMA) have allowed individuals treated early to gain new motor abilities and achieve more typical motor milestones. In this changing landscape, current motor function outcome measures (MF-OMs) used in SMA clinical practice may no longer be sufficiently sensitive enough to optimally quantify new disease trajectories and evolving functional progression.
Objective:
To develop a consensus-derived recommendation for MF-OMs to be used in assessing infants and children living with SMA who were treated with DMTs very early in life.
Methods:
A modified Delphi methodology which included three web-based surveys and virtual conferences was conducted with an international group of multidisciplinary experts treating infants and children living with SMA who were treated early. Community input was also collected via semi-structured interviews.
Results:
A consensus-derived recommendation for MF-OMs to be routinely administered in early treated infants and children living with SMA was developed. Consensus recommendations included both SMA-specific and non SMA-specific MF-OMs for five age periods. MF-OMs were inclusive of Clinician-Reported, Caregiver/Patient-Reported, and Performance/Functional Outcome Measures. Recommendations on optimal assessment frequency varied across age periods from quarterly to bi-annually.
Conclusions:
Clinicians with expertise in SMA achieved consensus on establishing relevant MF-OMs to implement from infancy through childhood to track motor progress in early treated infants. Routine data collection using recommended MF-OMs will facilitate cohort comparison for research collaborations to better understand new disease trajectories and motor progression of this population.
Keywords
Background
Disease modifying treatments (DMTs) have significantly altered the course of SMA, especially in infants treated very early, allowing them to gain motor abilities and developmental skills not previously observed.1–5 Current commercially available DMTs for SMA modulate the splicing of SMN2 pre-mRNA to increase production of functional full length SMN protein (nusinersen and risdiplam) or by delivering a copy of SMN1 via gene therapy (onasemnogene abeparvovic-xioi).6–9 Although these DMTs compensate for reduced SMN protein levels and may slow disease progression, they are not curative, especially in individuals who are already symptomatic at the time of treatment. 10 Other DMTs currently in the clinical drug development pipeline include muscle-targeted treatments as well as higher doses and different administrations (intravenous versus intrathecal) of DMTs already approved. 7
Groundbreaking changes through the development of DMTs and the advent of newborn screening (NBS) have led to the ability to diagnose and treat infants with SMA at birth or very shortly thereafter.11,12 Infants diagnosed either clinically or via NBS may present, prior to initiation of DMTs, as 1) presymptomatic, presenting as clinically silent/asymptomatic, 2) presymptomatic, with emerging symptoms (prodromal to pauci-symptomatic), or 3) symptomatic shortly post pheno-conversion when early signs clinically manifest. 13 Hereafter, this manuscript will refer to this population as early treated infants. These early treated infants demonstrate varying differences in development and overall motor function than previously seen in SMA. Some present initially as clinically asymptomatic/presymptomatic and when treated early show considerable improvement and near typical development with only minor neurologic deficits.1–414,15 Others that present as symptomatic at birth respond less optimally to early treatments with DMTs and continue to present with functional impairments and significant delays. 14 In many countries, access to early diagnosis and early treatment remains limited, therefore progression proceeds according to historical descriptions. 10 Asymptomatic and presymptomatic infants derive the most benefit suggesting that early treatment is imperative14,16 and highlights the critical need for standardized assessment to guide management of this newly evolving phenotype over time.
Collaboration amongst the SMA community (academia, industry, advocacy, and individuals living with SMA and their families) has led to an evolution of natural history studies, phase 1–3 clinical trials, and real-world treatment/post commercialization registries of the first three DMTs for SMA. These efforts have included three clinical trials specific to treating the presymptomatic population (NURTURE, NCT02386553; SPR1NT, NCT03505099; and RAINBOWFISH, NCT03779334).1–4,17,18 In the aforementioned studies, primary, secondary and exploratory endpoints have included assessments of motor function, using both SMA-specific and non SMA-specific outcome measures.
Utilization of motor function outcome measures (MF-OMs) in early treated infants are critical for several reasons: 1) allows for accurate assessment of the effectiveness and impact of intervention(s) in improving motor function; 2) enables routine monitoring of motor skills and other relevant parameters to guide clinical management; 3) provides a comparison with typically developing infants; 4) facilitates characterization of this newly evolving phenotype to allow for long-term prediction of motor outcomes, identification of potential factors affecting progress, and more proactive identification of emerging comorbidities (highlighted in SMA-specific measures19–21); 5) informs healthcare providers about the specific needs of the infant which allows for personalized rehabilitation goals and treatment plans addressing their unique challenges and capabilities 22 ; and 6) provides valuable information to families about the expected developmental milestones and potential challenges their child may face. Collectively, this information would inform clinicians and families of the SMA individual's clinical status and motor trajectory and inform clinical decision making, counseling and referrals for intervention. Importantly, these MF-OMs should always be considered in conjunction with, and not in lieu of, the physician's neurologic assessment of signs and symptoms.
SMA-specific MF-OMs, including the Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND), Hammersmith Functional Motor Scale Expanded (HFMSE) and the Revised Upper Limb Module (RULM), were developed to quantify clinical changes and progression in the natural history over time across different SMA types and have demonstrated response to pharmacologic agents in clinical trials.19–27 Each of these MF-OMs have well documented reliability and validity in the symptomatic SMA population.19–27 Non SMA-specific MF-OMs, including the Hammersmith Neonatal Neurologic Examination (HNNE), the Test of Infant Motor Performance Screening Items (TIMPSI), the Timed Up & Go (TUG), and Timed Function Test (TFT)s, have been utilized more recently and have demonstrated emerging reliability and sensitivity in the SMA population.14,26,28–36 Current SMA-specific measures do not fully capture typical skill development, and thus early treated infants often reach the ceiling on SMA-specific measures.2–5 Experience with early treatment has necessitated the need to consider MF-OMs that are normative and criterion-referenced in nature, allowing for comparison of this newly emerging SMA phenotype to their typically developing peers and allowing for assessment of higher motor level skill competence.
A preliminary survey of clinicians managing early treated infants explored MF-OMs being utilized to discern consistencies and differences between institutions when measuring motor function across this evolving spectrum. 37 While most clinicians were still using SMA-specific MF-OMs, a variety of other outcomes were being utilized across clinics to better incorporate assessment of this early treated group. To best facilitate standardized, rigorous data collection across multiple clinical sites, consistency in the types of MF-OMs is necessary. A uniform and sensitive set of MF-OMs would also allow newer clinical sites to adopt appropriate measures at their centers.
To date there has been no guidance on selection of MF-OMs to assess this evolving population and obtaining consensus on recommended MF-OMs to understand the progression of this population over time is critically warranted. Therefore, the aim of this study was to establish consensus among international multidisciplinary experts in SMA regarding the prioritization of select MF-OMs to assess early treated infants and children. The primary goal was to provide clinicians and researchers with guidance on the most optimal MF-OMs selected to facilitate standardization in assessment over time. This will facilitate cohort characterization of this newly emerging phenotype, to proactively support their changing needs over time, and to facilitate research collaboration across centers.
Methods
Pre-Delphi
SMA clinical experts involved in functional motor assessment were invited in April of 2022 to collaborate in providing guidance and consensus regarding MF-OMs from infancy through childhood for early treated infants. An initial virtual conference was held to agree on the best methods for achieving consensus on MF-OMs. After initial discussion amongst a panel of international multidisciplinary healthcare experts, it was determined that a web-based modified-Delphi approach would be the most appropriate methodology to achieve consensus. Delphi consensus is a technique commonly used in healthcare practice to reach collective agreement amongst a group of experts. It is a structured and iterative process that combines expert knowledge when evidence is limited and provides controlled feedback to generate consensus.38–40
Following the initial meeting, four additional virtual expert panel conferences included discussion to: 1) define the patient population, 2) determine meaningful age periods for MF-OMs, 3) identify the most appropriate MF-OMs for each specified age period, and 4) select a panel of multidisciplinary healthcare experts to survey. A thorough literature review was conducted, and a MF-OM Evidence Table was developed to be referenced during the Delphi survey (Supplemental File 1). The Steering Committee (KJK, SDY, EM) then developed the initial Delphi survey based on prior expert panel input to determine consensus on the items discussed above (Figure 1).
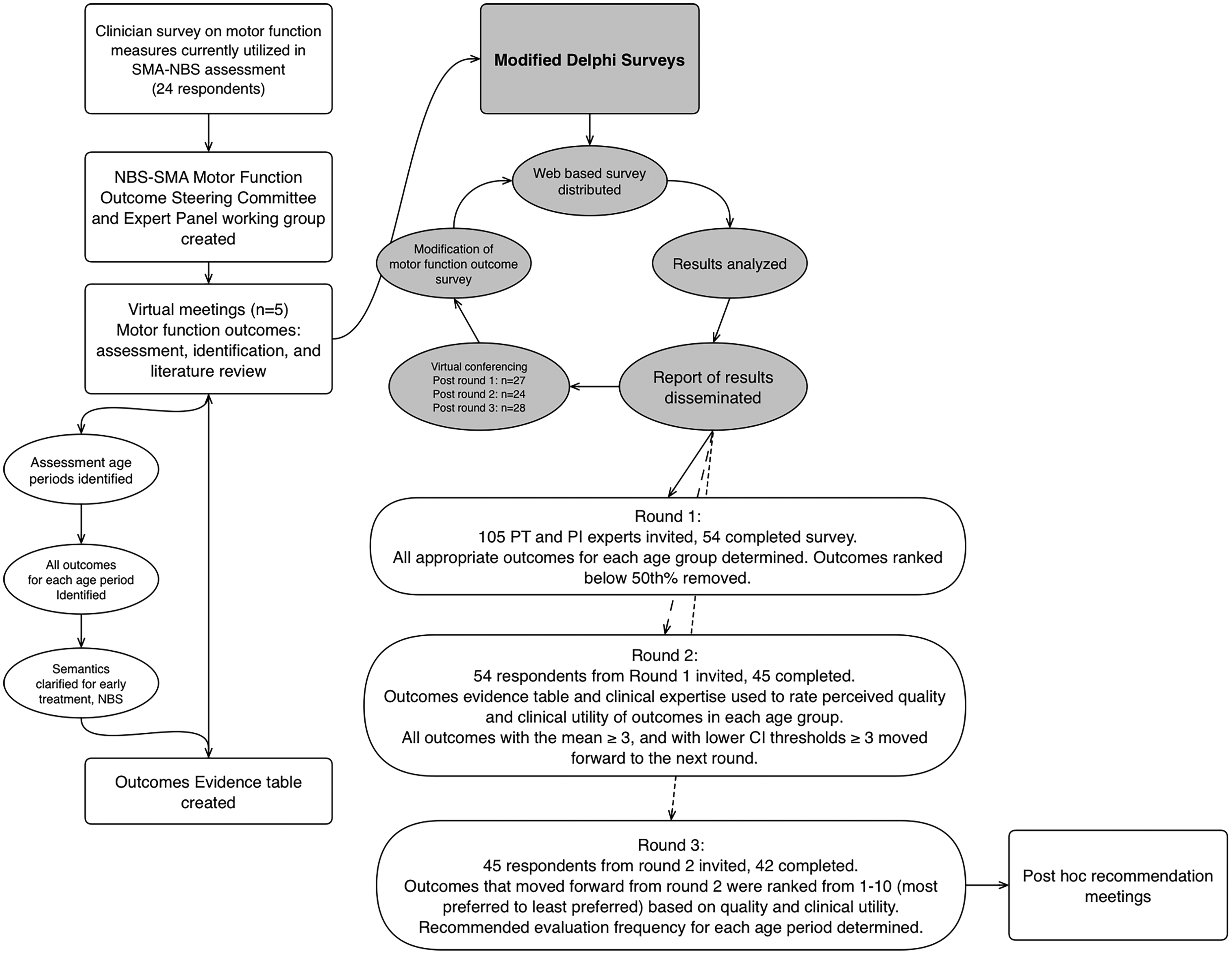
Modified Delphi methodology. SMA- spinal muscular atrophy; NBS- newborn screening; PT- physical therapist; PI- principal investigator; CI- confidence interval.
Delphi administration
Institutional IRB approval (Northwestern IRB # STU 00216184 and STU00221567) was obtained and a preselected expert panel was invited to participate via a REDCap survey in August of 2022. Expert panel members were selected using a broad email invitation list to healthcare professionals engaged in care of those with SMA in neuromuscular clinics across the US, Canada, South America, Europe and Australia. Expert panel members were English speaking healthcare professionals with expertise in SMA research and/or clinical care, familiar with newborn screening and MF-OMs in SMA. All participants who engaged in the survey were provided an electronic waiver of consent via REDCap. As each round progressed, those panelists who completed the prior round were invited to the next round. For each round the total number of expert panelists, practice specialty, years of experience, and country of practice were recorded. During each survey round expert panelists had access to the MF-OM Evidence Table (Supplemental File 1) and were asked to respond based on their knowledge of the evidence and their clinical expertise. Three web-based survey rounds were conducted prior to achieving a-priori consensus. After each Delphi round, results were tabulated and disseminated in formal reports to expert panelists and then discussed in virtual sessions prior to the next survey round commencing. Expert panelists completing each round were invited to these virtual discussions. While the survey and results were anonymized, panel discussions after each round were critical to obtain controlled feedback (Figure 1).
Consensus was examined after each round using descriptives (means (m), standard deviations (SD), and confidence intervals (CI)) for each outcome in each age period in addition to total number of respondents rating each MF-OM and percent agreement. Specifically, MF-OMs moved forward in each round based on a-priori consensus level of percent agreement in rounds 1 and 3. For round 2, a-priori mean ratings and lower CI threshold greater than or equal to 3 determined which MF-OMs moved to the next round (Table 1). In round 3, coefficients of variance were also calculated to determine agreement variance for the top 10 recommended outcomes in each age period.
Delphi round aims and A-Priori consensus/decision standards.

Legend: MF-OMs- motor function outcome measure; NBS- newborn screening; CI- confidence interval; %- percentage
Round 1
Expert panel demographics including medical profession/discipline, years’ experience overall, years’ experience working with individuals living with SMA, years’ experience with early treated infants, and country of practice were collected.
Expert panelists were asked if listed MF-OMs were appropriate to consider in the assessment of motor function when evaluating an early treated infant/child. Additionally, level of agreement was collected for several recommendations regarding MF-OMs in early treated infants including the type of measures to be considered, definition of the patient population, definition of baseline period, age periods for MF-OM assessment, factors driving assessment, and recommended frequency of assessment.
Types of motor function outcomes: Expert panelists were asked to indicate their agreement or disagreement regarding the classification of the types of MF-OMs to consider. Assessment types queried included: 1) SMA-specific criterion-referenced, 2) SMA-specific patient-reported outcome measure (PROM), 3) Non SMA-specific age normative, 4) Non SMA-specific criterion-referenced, 5) Non SMA-specific PROM, and 6) TFTs. MF-OM types ranked by the majority (>80%) were included in all rounds moving forward (Table 1).
Patient population: Expert panelists were asked to agree or disagree with the proposed definition of the patient population to be considered as relevant to this Delphi consensus on MF-OMs. The proposed definition for the patient population was stated as: “Infants and children with SMA treated asymptomatically or presymptomatically and/or who were treated early when they may have been in the prodromal/paucisymptomatic period or presented with early clinical symptoms. These infants may have been identified by NBS and/or identified clinically.” Agreement with the definition by the majority (>80%) was considered as consensus to move forward (Table 1).
Definition of baseline period: Baseline period definition was gathered from expert input and was proposed to be the time after a child is diagnosed via NBS or other means very early in life (may be pre-symptomatic, prodromal or symptomatic) until time of or very shortly after first DMT. Expert panelists were asked to agree or disagree with the proposed definition of the baseline period for this population.
Meaningful age periods for MF-OM assessment: As development is not linear and MF-OMs intersect a variety of ages with no one outcome encompassing all ages, we felt it was important to establish agreement on important age periods. Expert panelists were asked to agree or disagree with age periods for identifying MF-OMs based on age over time. Proposed age periods included: baseline (defined above), after baseline and < 1 year of age, 1 year to < 3 years of age, 3 to 5 years of age, and > 5 years of age.
Factors driving assessment: Expert panelists were asked to rank priority factors driving assessment from a pre-defined list generated from the panel: functional status, age at visit, SMA type, age at diagnosis, SMN2 copy number, insurance authorization, type of DMT, and other. If ‘other’ was chosen, they were given the option to write in additional factors that might drive assessment choice.
Recommended frequency of assessment: Expert panelists were asked to recommend frequency of assessment for two time periods: 1) during the first year of life and 2) after the first year of life.
Agreement on MF-OMs to consider across each time period: Experts selected outcomes they perceived to best fit for each age period. Those MF-OMs that reached 50% agreement were carried forward into the next survey round (Table 1).
Round 2
Those that responded to round 1 were invited to participate. This round was focused on rating the outcomes remaining after Round 1 based on experience and evidence within each specific age period. Each listed MF-OM was rated on a Likert scale: 5) Very Strong, 4) Somewhat Strong, 3) Neither Weak nor Strong, 2) Somewhat Weak, 1) Very Weak, or 0) Unfamiliar with MF-OM, unable to rate. To minimize skewed effects of respondents rating MF-OMs they were unfamiliar with, they were instructed to rate only the MF-OMs they were familiar with for each age period. Expert panelists had access to the MF-OM Evidence Table in REDCap (Supplemental File 1) and results from the prior round (Supplemental File 2) when completing the round 2 survey.
MF-OMs that reached a priori mean ratings ≥ 3/5 (neither strong nor weak, somewhat strong, or very strong) and lower bound CI thresholds ≥ 3 were moved forward to the next round.
Round 3
Prior to the start of round 3, some MF-OMs were grouped (tests with older and newer versions) or collapsed (due to similarity of construct, based on virtual conferencing after round 2). TFTs including the 10-meter walk run test (10MWRT), time to climb 4 stairs (TTC), and timed rise to stand from supine on floor (TTR) were collapsed into one TFT MF-OM.
In round 3, expert panelists ranked MF-OMs remaining after round 2 based on which they felt were the top 10 MF-OMs in each age period from most to least preferred. Expert panelists had access to the MF-OM Evidence Table (Supplemental File 1) and results from the prior round (Supplemental File 3) when completing the round 3 survey. Means and standard deviations (SD) were plotted and consensus determined with means a-priori ≥ 70% delineated as core, means a-priori ≥ 50% delineated as recommended and remaining MF-OMs in the top 10 ranked were delineated as exploratory. (Figure 2) Coefficients of variance were also calculated to determine agreement variance (Table 1). Additionally, they were asked to rate their familiarity with each ranked MF-OM as a binary (familiar/unfamiliar) and their clinic's current use of each ranked MF-OM (yes/no/unsure). Moreover, factors affecting decision-making and driving MF-OM selection were revised due to limited consensus in round 1 and expert panelists were asked to re-rank factors driving assessment. Finally, the recommended frequency of assessment from round 1 was revised to query the recommended frequency specific to each age period (baseline, after baseline and < 1 year of age, 1 year to < 3 years of age, 3 to 5 years of age, and > 5 years of age).
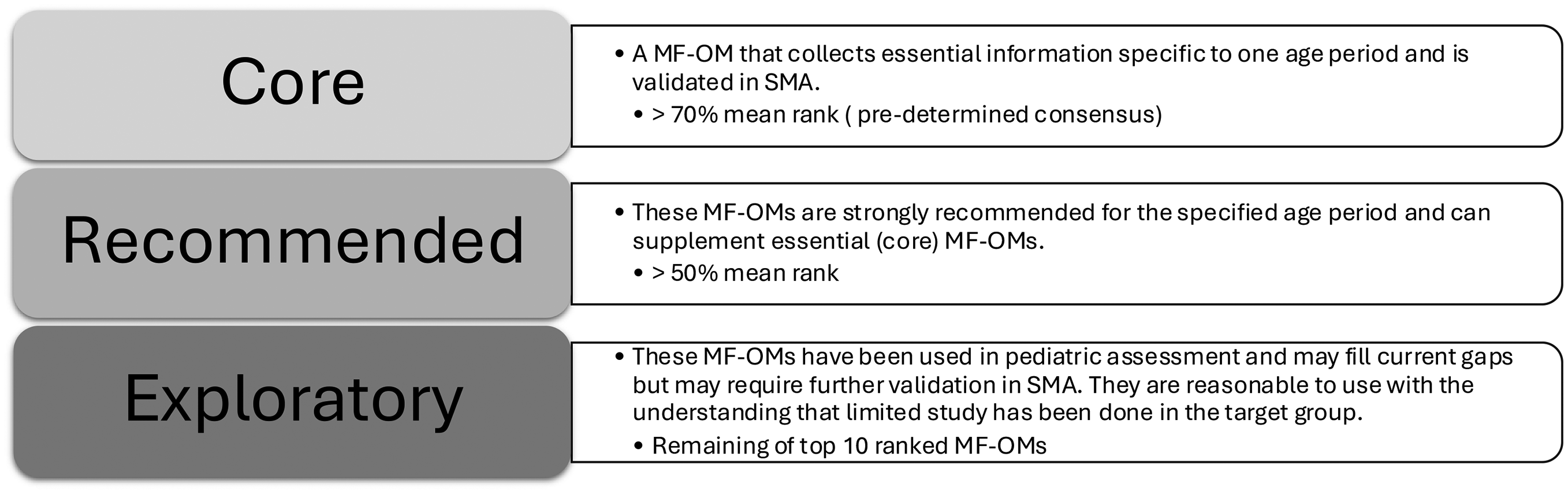
Core, recommended, and exploratory MF-OM categories for best practice. MF-OM- motor function outcome measure.
Final virtual conference and community engagement
A post-hoc virtual conference was conducted after the final round. Round 3 data (Supplemental File 4) was shared and discussed. All the panelists recommended that the HFMSE and Revised Hammersmith Scale (RHS) as well as the Motor Function Measure-32 (MFM) and the MFM-20 be combined due to overlapping constructs. If they were ranked at the same level of core, recommended or exploratory, panelists recommended allowing users to select one versus the other as appropriate. Similarly, the Bayley Scales of Infant and Toddler Development 3 (BSID-3) and Bayley-4 assessments were collapsed into one Bayley MF-OM, the Peabody Developmental Motor Scales (PDMS)-2 and PDMS-3 were collapsed into one PDMS MF-OM and the Bruininks-Oseretsky Test of Motor Proficiency (BOT)-2 and BOT-3 were collapsed as the BOT MF-OM. This approach was adopted in part due to differences in the availability of these test versions across regions worldwide. Nevertheless, the use of newer versions was highly recommended, as validation of older versions typically become outdated one year after newer versions are published. 61 A final consensus-derived recommendation of MF-OMs delineated as core, recommended, and exploratory for each age period (Figure 2) was generated. Merits and barriers of each assessment were also discussed (Supplemental File 5).
Community Engagement: Five community participants in the US and Europe with an early treated infant who had participated in early motor function assessments were recruited to participate in semi-structured interviews which were conducted after the Delphi consensus to garner patient and family input. Families were recruited by word of mouth amongst panel members’ clinic participants and also using IRB-approved recruitment email and online social media messaging and the first five families to respond were interviewed. An iterative inductive process using open coding and DeDoose software was utilized to derive data driven themes from full text content of interviews. After initial coding, similar codes were grouped to form potential themes. Potential themes were then reviewed and iteratively refined against the coded data to come up with final themes that reflect the data.
Results
Demographics
One-hundred and five international multidisciplinary experts were invited to round 1, with the majority being physical therapists/physiotherapists (PTs) and physicians (MDs) (Figure 3). While the proportion of MD invitees was slightly higher than PT invitees, the response rate was higher for PTs for round 1 and that distribution occurred across Delphi rounds 2 and 3 as well (Table 2). The response rate for round 1 was excellent (51.4%, n = 54) and improved across subsequent rounds (round 2: 83.3%, n = 45, round 3: 93.3%, n = 42).
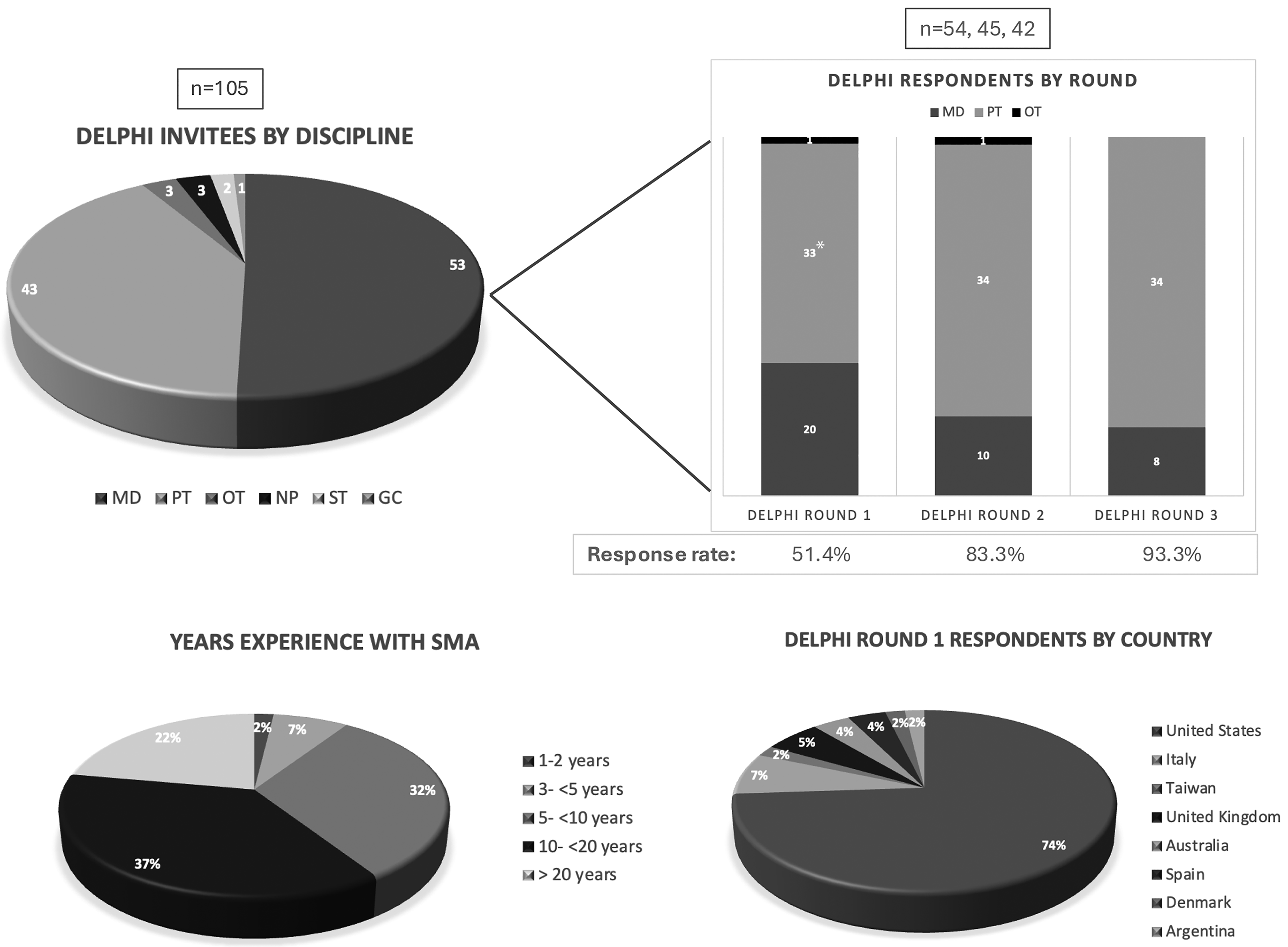
Delphi expert panelists demographics. MD physician, PT physical therapist/physiotherapist, OT occupational therapist, NP nurse practitioner, ST speech therapist, GC genetic counselor, *The initial group of PTs in Round 1 was reduced by one due to a data import issue in REDCap.
Delphi expert panelists.

Legend: MD physician, PT physical therapist/physiotherapist, OT occupational therapist; *The initial group of PTs in Round 1 was reduced by one due to a data import issue in REDCap
Expert panelists’ experience with SMA in round 1 ranged from one to greater than twenty years with the greatest percentage of respondents having between 10–20 years of experience. All had experience with infants with SMA, and the majority had experience with very early diagnosed infants, except two MDs (UK, Spain) and three PTs (one each from US, UK, and Denmark). Delphi expert panelists represented eight countries with the majority being from the United States. Ninety percent of panelists reported being SMA experts who had been or would be evaluating early treated infants (i.e., identified by early newborn screening or early clinical assessment or testing). Additionally, 79% reported involvement in decision-making, locally or within this SMA NBS Motor Outcomes Working Group regarding motor function testing in early treated infants with SMA. Several panelists represented countries that did not yet have fully established NBS at the time this survey was initiated in early 2022 (Argentina, Denmark, Spain, UK), however, regional pilots or partial implementations were underway in Denmark, Spain, and the UK. 41
Round 1
The number of MF-OMs included at the start of round 1 were rated and ultimately reduced based on a-priori agreement for each age period (Table 2). Specific MF-OM reductions can be found in Supplemental File 2.
Types of motor function outcomes: All proposed MF-OM types reached consensus with > 80% agreement: 1) SMA-specific criterion-referenced (98.1%), 2) SMA-specific, PROM (98.1%), 3) Non SMA-specific, age normative (94.1%), 4) Non SMA-specific criterion-referenced (86.3%), 5) Non SMA-specific PROM (80%), and 6) TFT (92.3%). MF-OM types ranked by the majority (>80%) were included in all rounds moving forward.
Definition of baseline period: There was 100% agreement with the proposed definition (see methods) of the baseline period after round 1.
Definition of population: There was 100% agreement with the proposed definition of the patient population (see methods) after round 1.
Meaningful age periods for MF-OM assessment: All proposed age periods for MF-OM assessment (baseline, after baseline and < 1 year of age, 1 year to < 3 years of age, 3 to 5 years of age, and > 5 years of age) reached 100% agreement in round 1.
Factors driving assessment: Factors felt to be driving assessment choice were prioritized as follows: functional status (100%), age at visit (100%), SMA type (67%), time (63%), age at diagnosis (59%), SMN2 copy number (47%), insurance authorization (37%), type of DMT (27%), and other (14%). Only two factors (functional status and age at visit) achieved consensus > 80%. Fourteen percent of expert panelists provided additional factors including country mandated assessments, prior assessments completed, and ability to follow commands/cognitive status. Lack of consensus on ranking of factors driving assessment in round 1 supported an additional round of querying which occurred in round 3.
Recommended frequency of assessment: Expert panelists (n = 51) recommended frequency of assessment for two age periods: 1) During the first year of life, 53% recommended quarterly assessments, and 22% recommended follow-up assessments occur every 2 months. The remaining expert panelists varied between once every 4 months (14%), once a month (6%), once every 6 months (4%), and other (1%); 2) After the first year of life, 57% recommended every 6 months, 20% recommended once every 4 months, and 16% recommended quarterly. The remaining expert panelists varied between once per year (4%) and 4% (n = 2) stated other. For both age periods those selecting other noted they would follow 2 copy babies more often, and follow-up schedule would be at increasing intervals with age. Lack of consensus in round 1 supported an additional round of querying which occurred in round 3.
Round 2
The MF-OMs included at the start of round 2 were rated and the number of MF-OMs was ultimately reduced for each age period. Remaining outcomes each met a pre-determined cut-off mean score of ≥ 3. Rating results and specific MF-OM reductions can be found in Supplemental File 3.
Round 3
MF-OM rankings from most to least preferred: Ranking of the top 10 MF-OMs delineated a-priori as core, recommended and exploratory (Figure 3) for each age period using mean ranks are represented in Figure 4. In both the baseline and after baseline to < 1 year of age period one core, four recommended and two exploratory measures reached consensus. In the 1 to < 3 years of age period one core, four recommended and four exploratory measures reached consensus. From 3–5 years of age three core, three recommended and three exploratory measures reached consensus. In the > 5 years of age period two core, five recommended and two exploratory measures reached consensus. Coefficients of agreement variance were mixed dependent on MF-OM. (See Supplemental File 4 for additional detail).
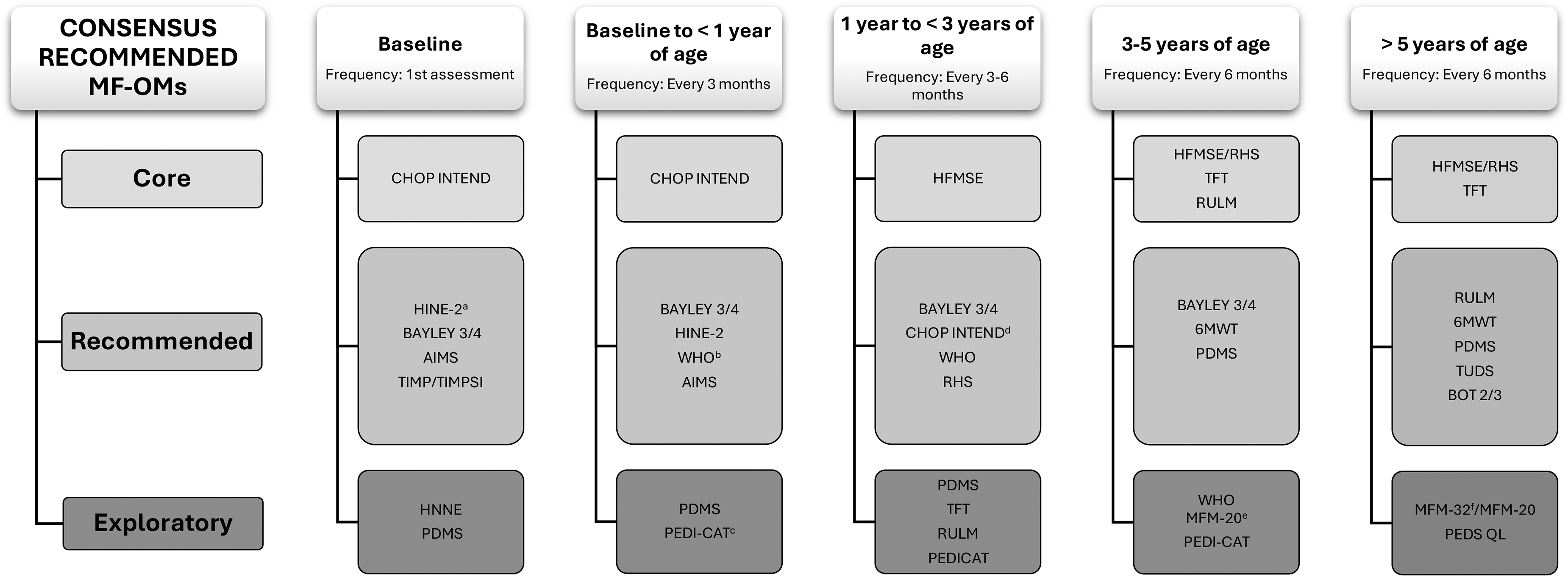
Consensus recommended MF-OMs delineated by core, recommended and exploratory for each age period. Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND); Hammersmith Functional Motor Scale Expanded (HFMSE); Revised Hammersmith Scale (RHS); Timed Function Test (TFT); Revised Upper Limb Module (RULM); Hammersmith Infant Neurologic Exam- Motor Section (HINE-2); Bayley Scales of Infant Development (BAYLEY 3/4); Alberta Infant Motor Scales (AIMS); Test of Infant Motor Performance (TIMP); Test of Infant Motor Performance Screening Items (TIMPSI); World Health Organization Motor Milestones (WHO-MM); Six Minute Walk Test (6MWT); Peabody Developmental Motor Scales (PDMS); Timed Up and Down Stairs (TUDS); Bruininks-Oseretsky Test of Motor Performance (BOT 2/3); Hammersmith Neonatal Neurological Exam (HNNE); Pediatric Evaluation of Disability Inventor- Computer Adaptive Test (PEDI-CAT); Motor Function Measure-20 (MFM-20); Motor Function Measure (MFM); Pediatric Quality of Life (PEDS-QL); a. Start at 2 months of age; b. Start at 4 months of age; c. Start at 1 month of age; d. Only continue if has not achieved full score at a previous visit; e. Start at 3 years of age and continue until transitioned to MFM-32 at 6–7 years; f. Start at 6 years.
Familiarity and clinical use: Familiarity with and clinical use of final ranked MF-OMs varied and is reported in Supplemental File 4. Familiarity varies with MF-OM and age period being queried. Overall greater familiarity and use was reported for MF-OMs that were ranked higher in each age group. In general, there appeared to be more familiarity with SMA-specific MF-OMs that have been used in SMA clinical trials and less familiarity with norm-referenced outcomes in the younger age periods (baseline through < than 1 year of age) and in those older than 5 years of age.
Factors driving assessment selection: Factors driving assessment selection ranked in round 1 were reworded and surveyed again in round 3 due to limited consensus in round 1. Priorities ranked (in order of frequency) were: functional status (97.6%), presenting symptoms (85.7%), age at follow up (81%), insurance authorization requirements (42.9%), age at diagnosis (38.1%), SMN2 copy number (28.6%), type of SMA (23.8%), pharmacologic treatment (19%), and other (14.3%) which included time and equipment availability, knowledge of outcomes, continued symptoms, etc. Time available for assessment administration, as well as effects of government mandates on outcomes selection, while not explicitly surveyed, were reported as “other” as additional elements that continue to drive assessment selection.
Recommended frequency of assessment: Expert panelists (n = 42) achieved a-priori consensus (> 70% agreement) for frequency of assessment at different age periods in round 3 (Table 3). During the first year of life, 76% suggested assessment frequency a minimum of every 3 months. After the first year of life, 95.2% assessment every 3–6 months was suggested until age 3. From age 3 to 5, and > 5 years, 90.5% and 83.3% respectively, suggested assessment was at least once every 6 months.
Age periods and suggested frequency of assessment for early treated infants.

Legend: y = years; m = months; < = less than; > = greater than:* Baseline assessment timing should not delay treatment initiation. These are suggested treatment intervals and reflect an ideal-scenario, consensus informed guide to be adapted based on patient needs, local resources, and feasibility.
Final Recommendation
A final post hoc meeting occurred after round 3, in February 2024, to synthesize and finalize MF-OM consensus-derived recommendations and discuss potential ways to facilitate implementation. Final MF-OMs including core, recommended and exploratory (Figure 4) are additionally represented in Figure 5 by construct, priority level, and age period. Both schematics collapse MF-OM versions (e.g., BSID-3 and Bayley-4, PDMS-2 and PDMS-3, etc.) and related measures (e.g., HFMSE and RHS, TFTs) when they were recommended at the same level of priority (core, recommended, exploratory) within an age period. To additionally support the expert panel's consensus-derived recommendations, an Outcome Merits and Barriers Table (Supplementary File 5) was created as a useful reference to support clinical decision-making and guidance for selecting and prioritizing MF-OMs. Ninety percent of meeting participants felt implementation would be feasible within their settings. Review of these recommendations, once formally implemented, was also discussed and half (50%) agreed revising every 2 years was appropriate, while 17% felt MF-OM recommendations should be reviewed annually and 33% felt every three years would be adequate.

Final NBS consensus based MF-OM recommendation by construct, level of priority, and age period. Measure selection should be guided by 1) clinical judgement, 2) ranked factors (functional status, presenting symptoms, and age at follow up), 3) priority level of measures, 4) the Merits and Barriers table (Supplemental file 5), and 5) resources and time available. Spinal muscular atrophy (SMA); Test of Infant Motor Performance Screening Items (TIMPSI); Hammersmith Neonatal Neurological Exam (HNNE); Hammersmith Infant Neurologic Exam- Motor Section (HINE-2); Alberta Infant Motor Scales (AIMS); Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND); Bayley Scales of Infant Development (BAYLEY); Peabody Developmental Motor Scales (PDMS); World Health Organization Motor Milestones (WHO-MM); Pediatric Evaluation of Disability Inventor- Computer Adaptive Test (PEDI-CAT;) Hammersmith Functional Motor Scale Expanded (HFMSE); Revised Hammersmith Scale (RHS); Timed Function Test (TFT); Revised Upper Limb Module (RULM); Six Minute Walk Test (6MWT); Motor Function Measure-20 (MFM-20); Motor Function Measure-32 (MFM-32); Pediatric Quality of Life (PEDS-QL); Timed Up and Down Stairs (TUDS); Bruininks-Oseretsky Test of Motor Performance (BOT): Patient Reported Outcome Measure (PROM).
Community input
Family and caretaker input was deemed important to obtain prior to achieving final consensus. Of the five families who participated two families were involved in MF-OM assessment within clinical trials and were also treated with secondary DMTs commercially, while three families’ experiences were with MF-OM assessment pre- and post-dosing in a clinical setting with commercial drug. Current ages of participants’ children ranged from 2 months to 8 years. All had diagnostic confirmation and initial treatment within two weeks of life except for one participant who initiated treatment after two months of age. Overall, participants appreciated the newly designed structure for consensus-derived MF-OM recommendations and felt there was a clearer focus on MF-OMs that may be more comprehensive and meaningful for early treated infants.
Common themes that emerged from family interviews included:
1. Communication, information sharing, support and parent education
Input centered around making the testing experience informative, comprehensive and supportive for both the child and family. Providing parental education, such as a brief document in lay language explaining the assessments and what they measure, was recommended to assure families understand the purpose of repeated testing and what to expect at each evaluation. Clear communication of findings was also recommended as most felt they did not have access to assessment scores, especially when involved in clinical trials. The importance of providing detailed feedback to parents to help them understand their child's progress and areas for improvement was noted to be of value by multiple participants. The supportive and engaging approach of the therapists was also reported to play a crucial role in the success and effectiveness of testing sessions.
2. Challenges with standardized testing, compliance, and testing conditions
Challenges of unfamiliar environments and frequency, length, and timing of assessments were discussed. Several participants were concerned with perceived over testing as their children had repeated MF-OM testing in short intervals to meet the separate needs of providers, insurers, and clinical trial protocols. Participants also felt the need for a better balance between standardized MF-OM testing and capturing overall developmental growth. Participants did observe flexibility and the PT's ability to adapt in the moment to accommodate their child's needs and behaviors.
3. Parental observation, assessment and monitoring
Participants reported understanding the comprehensive nature of testing as well as the benefits of more intensive early testing with a decrease frequency over time. Their feedback also emphasized the need to assess skills that are more in line with age-related peers versus continued utilization of SMA-specific measures, which they feel their child no longer needs. Several stated that a better understanding of what to expect next from a developmental perspective would be of value.
Discussion
Consensus-derived recommendations for use of a standardized set of MF-OMs to track early treated infants were established via modified Delphi. Providing consensus-derived recommendations for MF-OMs to use in evaluation of early treated infants also supports the observation that a better understanding of outcomes is critical to improve care. 42 In conjunction with early neurologic signs and symptoms, use of these consensus-derived MF-OMs will enable a more complete understanding of motor development, functional abilities and impairments. 13 These selected MF-OMs may more clearly elucidate patterns of developmental progression over time and may potentially lead to earlier prediction of long-term motor outcomes for parents and caretakers. 43 Additionally, an informed understanding of motor trajectories will allow practitioners to have more meaningful interactions with families and providers regarding rehabilitation recommendations. Future implementation of these consensus-derived recommendations will also facilitate improved monitoring and data sharing across SMA clinics. Our methodology to get consensus for NBS MF-OMs parallels that used recently in Delphi panels considering outcomes to assess adults with SMA 44 and bulbar function in those with SMA, 45 and supplements recommendations for other SMA types and ages44,46–53 for both treated and untreated SMA populations.
Current MF-OMs being utilized in most clinics to assess early treated infants with SMA describe functional improvement but, anecdotally, may miss issues of importance related to everyday care as reported by parents and caregivers. Use of additional MF-OMs, recommended by consensus and appropriate to both age and motor abilities, would allow for development of an international repository of MF-OMs that would enrich our understanding of this population over time, describe motor function trajectories, and allow us to optimize our care and therapeutic approach to individual children. Understanding motor function trajectories over time and the relationship of these trajectories to DMT intervention (timing and type) could also potentially lead to the ability to predict outcomes and better prognosticate need for additional interventions.
The progressive loss of motor neurons in SMA underscores the importance of early intervention, which allows the stabilization and rescue of a larger pool of neurons. 54 Thus a sense of urgency exists to initiate treatment as soon as diagnosis is confirmed. Treatment started in the earliest stage of the disease has been clearly demonstrated to dampen disease progression,1–4 with those treated in the clinically silent phase reaching the highest levels of motor development.12,43 Monitoring disease progression and understanding evolution of how motor function emerges in early treated phenotypes may assist in clinical decision-making regarding intervention and referral. While an assessment of motor function at baseline should never delay treatment initiation, it can be informative in understanding progression over time.
In addition to SMA-specific MF-OMs the final consensus also included an array of non-SMA-specific normative and criterion-based measures that improve the ability to assess development in light of typical expectations and to compare with age-related peers. Community participants cite this addition as relevant and meaningful to their child and family. Additionally, the final recommended set of MF-OMs overlap across ages and contain similar functional items that will be important in tracking longitudinal progress. Several measures that did not reach consensus (Supplemental files 2–4) may still be considered as the field evolves and additional evidence accumulates. While the final consensus-derived MF-OM recommendations are comprehensive of motor ability, other domains (bulbar,45,55 speech and swallowing, 56 cognition,57,58 respiratory, 56 quality of life, 59 and activity using inertial measurement units (IMUs) 60 ) remain important to include in any comprehensive assessment of early treated infants to cover all aspects of relevance in multidisciplinary care for the individual and caretaker. Cognition in particular could impact motor assessment and one should be mindful of such in selecting the appropriate MF-OM for an individual child. Capturing dates of basic motor milestone achievement separate from MF-OMs using parental report or developmental checklist also remains important, since many milestones are achieved between actual clinic visits.
Recommended suggestions for frequency of assessment were initially difficult to determine. In Round 1 assessment frequency was based on the early treated population as a whole without considering differences in recommendations based on the child's age and timing of treatment and therefore the panel was unable to come to consensus. After rewording the question in Round 3 to focus on frequency recommendations based on individual age periods consensus was achieved. Suggestions for frequency of assessment are provided from baseline through greater than five years of age. These suggestions are in line with what is currently occurring in neuromuscular disease follow-up clinics relative to insurance reimbursement requests (US, AUS, UK) and expected developmental skill acquisition across the early years of life. Although more frequent assessment is suggested early in life, a reduction in frequency with age should reduce the burden on the individual, family and clinicians. Additionally, while suggested frequency of visits is important for optimal follow-up, one must also consider impact of unforeseen family, child and life events, as well as insurance/payor requirements and other resources that may alter visit timing.
Consensus recommendations support frequency of assessments at three-month intervals during the first year of life. This aligns with established clinical standards and trial protocols and is considered essential for capturing rapid developmental changes and differentiating motor improvement from regression. While this frequency may present feasibility challenges in resource-limited settings, flexibility is encouraged. SMA-specific MF-OMs currently serve as the core assessments, reflecting their historical role in defining untreated phenotypes and providing a critical comparator for early-treated populations. However, as early treated infants often demonstrate more robust and typical motor development, integration of normative measures is warranted to enable age-appropriate comparisons and inform the evolving new natural history of this phenotype.
In the US, barriers to new or continued treatment access may include insurance/payor or other regulatory authorization requirements. Payor requirements continue to drive MF-OM selection, as most insurers and regulatory agencies rely on published evidence from previous SMA clinical trials for assessment for drug re-approvals. Similarly, providers in both the UK and Australia report the need to select MF-OMs mandated by health governing agencies. However, MF-OMs currently recommended by these parties for re-evaluations may not effectively depict change over time or target intervention needs (rehab or pharmaceutical) being that they emerged from use in those treated later in their disease course. Thus, a consensus driven approach to selection and utilization of MF-OMs in the early treated population with additional real-world evidence will be most impactful to characterize new motor function trajectories. It behooves us as clinicians and experts in motor function to continue to educate these authorities on the need for changes in assessment based on clinical presentation. It also remains important as clinicians to prioritize factors such as functional status, presenting symptoms and age at follow up in the selection of outcomes from the consensus-derived recommendations.
Decisions regarding selection of core along with recommended and or exploratory assessments should consider: 1) clinical judgement, 2) ranked factors deemed relevant in influencing outcome selection (functional status, presenting symptoms and age at follow-up), 4) the merits and barriers table (Supplemental Table 5), and 5) resources and time available. Specifically, selection of MF-OMs should be guided by such when time or resources are constrained. Typical assessment visits range from 30 to 90 min, and clinicians are advised to exercise clinical judgment in balancing comprehensiveness with feasibility. Consistency in use of MF-OMs across time points may enhance understanding of longitudinal trajectories, particularly as treated natural history data are accumulated for future trials. Due to the nature of overlap of various MF-OMs in ages covered and endpoints captured, one might choose the MF-OM that they are most familiar with and that could be tracked over a longer period. One should use their clinical judgement in continuing administration across age periods if a MF-OM is still deemed of value, is valid, and the child has not met the ceiling of the assessment (e.g., TIMPSI, HINE-2, AIMS). Utilization of the Merits and Barriers table (Supplemental Table 5) as a resource to assist with clinical decision-making regarding continuation or discontinuation of a tool over time is recommended as it provides guidance on MF-OM validation ages. For those who may score the maximum on any SMA-specific scale pre or post treatment (including those with > 4 copies of SMN2) one should absolutely consider prioritizing normative MF-OMs that may identify more minor deficits. It is also expected that as we gain more experience with MF-OMs ranked as exploratory they may also move up in priority level and fill current gaps for this population. Most exploratory level MF-OMs were deemed newer to SMA in general (HNNE, PDMS) or were known, but required exploration of validation in younger ages (RULM, TFT, etc.) as this early treated population presents as stronger with higher levels of function earlier. Overall, these recommendations aim to provide adaptable resources for diverse clinical contexts, emphasizing flexibility in MF-OM use.
Parental input supports consensus recommendations. As advocates for their children and stakeholders in the assessment and treatment process, parents provided important input regarding the value of the newly derived MF-OM recommendations for early treated infants and parental/family buy-in will remain important to consider moving forward. Additionally, their input regarding early testing experiences, frequency and duration, and suggestions to improve testing sessions will be valuable and inform implementation recommendations and adoption of MF-OM recommendations across sites. Thematic analyses underscore the value of consensus-derived recommendations and the need for comprehensive MF-OM assessments. The impact of repeated PT testing for research and clinical care on family burden needs to be considered. Additionally, the importance of clear communication and information sharing to support the family and provide education to promote optimal experiences and personalized outcomes should remain at the forefront of continued conversations in this area.
Limitations to the study must be considered in interpretation of results. The survey was initially developed in the US and was primarily driven by the SMA newborn screening initiative. In an effort to be inclusive, the survey was originally distributed to a large population of SMA experts internationally; however, the majority of respondents were from the US (74%). Additionally, despite instructions to consider evidence and experience in selection of outcomes at selected age periods, inherent bias in selection, likely influenced by a participant's experience with MF-OMs currently used in clinical trials, cannot be ruled out. Clinical sites with experienced PTs and prior experience with the recommended MF-OMs have demonstrated the ability to initiate use within their current clinical settings and the majority reported feasibility regarding implementation. This may be biased as most participants were from larger academic and research centers where support and resources are more available. Further experience within and outside these centers will be important to consider.
Further study regarding implementation and efficacy in real-world practice is underway. The potential for remote and digital assessments in the future should also be considered. Future studies to harmonize data sets across centers will support the need for reevaluation of these recommendations of the motor trajectory in early treated infants and children.
Final consensus-derived MF-OMs were selected with thoughtful consideration of the supporting evidence across five specific developmental age periods. Feasibility of use, time to administer within the clinical setting, necessary equipment and resources, and overall experience with the MF-OMs were considered in the selection across each time-period. Measures were delineated as core, recommended, and exploratory, and a Merits and Barriers for Use Table (Supplementary File 5) was created to aid in clinical decision-making in selection of MF-OMs across age periods. Factors driving assessment, including functional status, presenting symptoms, and age at follow up, were key in MF-OM selection and should continue to be considered in personalizing selected MF-OMs for each individual. Importantly, adoption of these consensus-derived MF-OM recommendations will increase our understanding of disease trajectories and will add to improvements in clinical care.
Supplemental Material
sj-zip-1-jnd-10.1177_22143602261433638 - Supplemental material for Navigating new motor function trajectories: Consensus recommendations for assessment in the era of newborn screening and early treatment in SMA
Supplemental material, sj-zip-1-jnd-10.1177_22143602261433638 for Navigating new motor function trajectories: Consensus recommendations for assessment in the era of newborn screening and early treatment in SMA by Kristin J Krosschell, Sally Dunaway Young, Elizabeth Maczek, Laurey Brown, Katie Hoffman, Chiara Corbo Galli, Robert Muni Lofra, Giorgia Coratti, Meghan Moore Burk, Elise L Townsend, Carolyn Kelley, Christa Weigel, Matthew Civitello, Cara H Kanner, Melissa McIntyre, Leslie Nelson, Vamshi Rao, Diana Castro, Michelle Farrar, Nancy L Kuntz, Susan D Apkon, Zarazuela Zolkipli-Cunningham and in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
We thank all clinicians who participated in the Newborn Screening Spinal Muscular Atrophy Motor Function Working Group (NBS-SMArt): Giovanni Baranello, Enrico Silvio Bertini, Russell Butterfield, Terri Carry, Manu Chawla, Claudia Chiriboga, Wendy Chung, Emma Ciafaloni, Anne Connolly, Thomas Crawford, John Day, Adele D’Amico, Roberto De Sanctis, Darryl De Vivo, Tina Duong, Katy Eichinger, Richard Finkel, Wolfgang Mueller Felber, Richard Gee, Melissa Gibbons, Allan Glanzman, Antonia Goels, Soledad Gomez, Wuh-Liang Hwu, Megan Immarino, Elizabeth Kichula, Katie Kundrat, Courtney Lucken, Marion Main, Kaitlyn McGrattan, Julieta Medina, Julie Miller, Jackie Montes, Julietta Mozzoni, Amy Pasternak, Julie Patterson, Maria Fragala Pinkham, Matteo Pirinu, Kristy Rose, Lindsay Pietrruzewski, Crystal Proud, Carol Tesi-Rocha, Anne Marie Rohwer, Abigail Schwaede, Jessica Schwieterman, Molly Stark, Anne Stratton, Charlotte Sumner, Eduardo Tizzano, Jessica Trenkle, Ralph Rodriquez-Torres, Aravindhan Veerapandiyan, Keri Vela, Victoria Ward, Laura Watne, Julie Wells, Ulla Werlauff, Amelia Wilson
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded in part by support from Northwestern's NUCATS which is funded in part by a Clinical and Translational Science Award (CTSA) grant from the National Institutes of Health (NIH), UL1TR001422, for REDCap support. Its contents are the authors’ sole responsibility and do not necessarily represent official NIH views. KJK was supported by the Department of Physical Therapy and Human Movement Sciences, Feinberg School of Medicine and SDY and EM were funded, in part, by the Pediatric Neuromuscular Clinical Research Network (PNCRN) infrastructure grant from Cure SMA. ZZC was funded by the Pediatric Neuromuscular Clinical Research Network (PNCRN) infrastructure grant from CureSMA.
Disclosure of conflicts of interest
KJK: Advisory Boards/Steering Committee for Biogen, Scholar Rock and Cure SMA, Consulting for Biogen, Scholar Rock, Novartis, and Cure SMA. SDY: Advisory boards for Biogen and Scholar Rock, consulting for Biogen, Roche, and Cure SMA. RML: Advisory boards for Biogen, Roche and Novartis and consulting for Roche. GC: Steering Committee/Ad Board/Consultancy with Roche, Biogen, Novartis, Scholar Rock, Solid Biosciences. MMB: Advisory boards/consultant for Biogen, Scholar Rock, and Cure SMA. ELT: Consultant and Advisory Board for Biogen. MC: Advisory board for Biogen. Consultant for Novartis, Roche, IONIS. LN: Advisory board for Scholar Rock, Biogen. Consultant for Novartis, Roche, Biohaven. Speaker Bureau for Genentech. DC: Research with Biogen, SRK, Genentech, NMD Pharma. Steering Committee with Novartis; Advisory Boards with Biogen, Novartis, Scholar Rock, and Genentech. MF: site principal investigator for Roche, and Novartis Gene Therapies, Inc., SMA clinical trials, and the institution has received funds for contract research related to the conduct of these trials. MAF has received honoraria for advisory board participation and participation in educational events from Biogen, Novartis, and Roche, speaker's fees from Biogen and Novartis and serves as a medical director on the board of Muscular Dystrophy NSW (not-for-profit). NLK: Medical Advisory Boards for Argenx, Astellas, Biogen, Catalyst, Genentech, Sarepta, Scholar Rock; Institution receives funding for clinical research from Argenx, Astellas, Biogen, Catalyst, Genentech, Novartis, Sarepta, Scholar Rock and Solid Biosciences. SDA: Institutional PI on Biohaven and Scholar Rock. ZZC: Has previously been or is currently engaged with several companies involved in mitochondrial disease therapeutic clinical stage development as a paid consultant (Reneo Therapeutics, UCB Pharma), a sponsored research collaborator (United Mitochondrial Disease Foundation, US Department of Defense, North American Mitochondrial Disease Consortium, National Institutes of Health, Pediatric Neuromuscular Research Network Consortium), and/or under a sponsored research agreement with Khondrion, Astellas [formerly Mitobridge] Pharma Inc., Imel Therapeutics, Reneo Therapeutics, Stealth BioTherapeutics, Precision Therapeutics, Thiogenesis Therapeutics, Ribonova Inc., BPGBio, Inc, Tisento Therapeutics and Pretzel Therapeutics). EM, LB, KH, CCG, CK, CW, CHK, MM, & VR have nothing to report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.