
Abstract
Duchenne muscular dystrophy (DMD) is a progressive, neuromuscular disorder with significant morbidity and mortality. This study aimed to quantify the socioeconomic burden of DMD in Belgium, assessing direct medical and non-medical costs, indirect costs and health-related quality of life (HRQoL) using the University of Leicester's 8-stage model for DMD. A descriptive, retrospective, cross-sectional burden-of-illness study was conducted at an expert DMD center in Belgium between 02-11-2023 and 16-06-2024. One pediatric and one adult neuromuscular specialist from the University Hospitals Leuven completed an electronic Case Report Form using patient electronic medical records capturing demographics, clinical data, and data on healthcare resource utilization over the prior 12 months. Patients under medical follow-up were invited to participate and provided written informed consent (N = 40). Costs were sourced through the Belgian National Institute for Health and Disability Insurance and the Belgian Center for Pharmacotherapeutic Information. A questionnaire was given to the participants and their parents to collect additional costs, HRQoL, and caregiver burden. The estimated mean annual societal cost per Belgian DMD patient was €134,337, with costs ranging from €115,336 in early disease stages to €153,339 in late disease stages. Direct non-medical costs were the largest contributor, followed by indirect costs, primarily due to loss of productivity. HRQoL declined with disease progression. Caregiver burden remained high across all disease stages. DMD imposes a significant socioeconomic burden on patients, caregivers, and society in Belgium. The findings underscore the importance of improving access to supportive therapies and interventions.
Introduction
Duchenne muscular dystrophy (DMD) is an X-linked recessive neuromuscular disorder caused by mutations in the dystrophin gene, primarily affecting males. 1 DMD is rare, with a global prevalence of 7.1 cases per 100,000 males and a birth prevalence of 19.8 per 100,000 live male births. 1 Incidence rates in Europe are consistent, with studies estimating 19.8 per 100,000 live male births. 2 The Belgian Neuromuscular Disease Registry (BNMDR) estimated in 2015 a prevalence of 4.5 patients per 100,000 male births. 3 DMD is characterized by progressive skeletal muscle deterioration, leading to significant morbidity and mortality. The disease typically progresses from loss of ambulation in early adolescence to severe respiratory and cardiac failure, culminating in premature death. Most patients become wheelchair-dependent by 10–12 years of age and require assisted ventilation by their 20 s. Weak respiratory muscles increase vulnerability to infections like pneumonia, while cardiac involvement results in cardiomyopathy and heart failure. 4
While there is no cure for DMD, multidisciplinary management has improved patient outcomes. 5 Current standard care includes corticosteroids such as prednisone or deflazacort, which delay disease progression, extend ambulation, and reduce the incidence of complications like scoliosis and cardiomyopathy.6,7 However, these treatments have significant side effects, including weight gain, osteoporosis, hypertension, impact on behavior and reduced quality of life.6–8 Emerging therapies for DMD include those that address its underlying genetic causes, such as gene therapy and exon skipping, as well as others that target the pathophysiological processes involved in muscle necrosis and fibrosis.9–12 Additionally, the development of the dissociative steroid vamorolone has the potential to transform the treatment landscape by reducing the side effects associated with long-term steroid use. Despite these advances, unmet needs persist, particularly in access to innovative therapies and their long-term efficacy.
The University of Leicester developed a natural history model of DMD through Project HERCULES, a collaboration aimed at supporting health technology assessments (HTAs) and reimbursement decisions (Figure 1). The model outlines eight disease stages, grouped into three phases: ambulatory, transfer, and non-ambulatory. It serves as a framework for evaluating the economic impact of new therapies by mapping the progression of DMD and its associated costs over a patient's lifetime. 13

Disease model of the natural history of DMD. This figure illustrates the 8-stage model of Duchenne muscular dystrophy (DMD) as originally developed by Broomfield et al. (2024), outlining the progressive loss of function from early ambulatory stages to full-time ventilatory support. To enable more robust analysis and ensure sufficient sample sizes within each group, the current study adopted a modified categorisation of disease severity. Specifically, the 8 stages were grouped into three broader categories—early (stages 1–3), middle (stages 4–6), and late (stages 7–8) disease stages.
DMD imposes a substantial Burden-Of-Illness (BOI) on patients, caregivers, and society. 4 A high-quality study by Schreiber-Katz et al. in Germany estimated the total annual economic cost of DMD at €78,913 (2013 prices), with direct medical costs accounting for 25%, informal care for 39%, and indirect costs for 36%. 14 Another study by Landfeldt et al. across four countries reported similar findings, estimating annual societal costs per patient between $80,120 and $120,910 (anno 2012 international dollars). 15 Indirect and informal care costs were the primary contributors to this total amount, while hospitalizations and medications represented minor expenses.
Health-related quality of life (HRQoL) declines significantly as the disease progresses, with the largest drop occurring between late ambulatory and early non-ambulatory stages.14–16
Despite this evidence, there remains a paucity of recent data on the BOI of DMD patients and their caregivers, including in Europe. Advances in treatment and care practices necessitate updated evaluations to capture the current landscape and address unmet needs. This study aims to provide real-world evidence on the socioeconomic burden of DMD in Belgium, focusing on costs and HRQoL across disease stages. The primary objective of this study was to quantify the cost of DMD in Belgium from a societal perspective, stratifying by the 8-stage model for DMD. 13 The secondary objective of the study was to estimate the impact of DMD on HRQoL in Belgium, from a patient and caregiver perspective, also stratified by the 8-stage model for DMD. 13
Methodology
Study design and procedure
This study employed a descriptive, retrospective, cross-sectional burden-of-illness (BOI) approach. Data were collected from an expert DMD center in Belgium between 02-11-2023 and 16-06-2024. Two neuromuscular specialists from the University Hospitals Leuven (one specializing in pediatric care and the other in adult care) completed an electronic Case Report Form (eCRF) using patient electronic medical records. The eCRF captured demographics, clinical data, and data on healthcare resource utilization (HCRU) over the preceding 12 months (see 2.3.1 for details). The consultation date on which the patient was recruited was designated as the index date.
Ethical approval was obtained from the Ethical Committee in UZ Leuven (S67663). Patients under medical follow-up at UZ Leuven were invited to participate and provided informed consent. Each participant completed a corresponding Patient and Public Involvement & Engagement (PPIE) questionnaire, capturing demographics and HRQoL cross-sectionally. PPIE completion varied by patient age and cognitive ability: patients aged 18 + completed it independently, primary caregivers completed it for patients aged 4–7, and both patients and caregivers jointly completed it for those aged 8–18 years. Caregivers of patients with cognitive delay provided consent and completed the PPIE on behalf of the patient. They also completed a caregiver-specific section addressing their own HRQoL and any expenses incurred due to caregiving. Additional costs, including direct non-medical (e.g., travel) and indirect (e.g., productivity loss), were retrospectively assessed over the prior 12 months.
Participants
The study population included paediatric (under 18 years old) and adult patients diagnosed with DMD at least 12 months prior to the index date. The total target sample for this study was 40 patients, about evenly divided between pediatric (<18 years) and adult patients (18 years or older). To adequately represent the full spectrum of DMD (ambulatory, transfer, and non-ambulatory; see Figure 1), 13 measures were taken to ensure a balanced recruitment of ambulatory and non-ambulatory patients. The fieldwork agency continuously monitored individual physicians to understand the health state distribution of recruited patients. Weekly updates were provided from the fieldwork agency on the health disease stage distribution to minimise oversampling of ambulatory or non-ambulatory disease stages. For a patient to be considered for inclusion into the study, the patient had to meet the criteria below.
Inclusion criteria
1. Male 2. DMD diagnosis confirmed by genetic testing 3. Diagnosed with DMD at least 12 months prior the index date (i.e., the most recent consultation date in the last year) 4. Patients must have carefully read, understood, and signed the Informed Consent Form (ICF). For patients with a cognitive delay inhibiting them from deciding for themselves, support was provided by a caregiver giving consent on behalf of the patient.
Exclusion criteria
Patients with non-defined or other type of muscular dystrophies Patients participating or have ever participated in a clinical trial for an AAV gene therapy Patients and caregivers who cannot provide informed consent
Physicians were asked to stratify patients into one of the 8 health states as described below:
Early Ambulatory: patient can stand from supine and walk/run 10 m. Late Ambulatory: patient cannot stand from supine but can walk/run 10 m. Transfer: patient cannot stand from supine or walk/run 10 m but can remain standing (i.e., weight baring). Hand-to-Mouth Function (HTMF)/No ventilator: patient cannot remain standing (is non-ambulatory) but has HTMF and is not on a ventilator. No HTMF/No ventilator: patient has no HTMF but is not on a ventilator. HTMF/Night ventilation: patient has HTMF but is on night-time ventilation. No HTMF/Night ventilation: patient has no HTMF and is on night-time ventilation. Full Ventilation: patient is on full-time ventilation.
Due to small sample sizes per stage (N = 40 total), the eight disease stages were grouped into three broader categories for the primary analysis:
Early disease stages (Stages 1–3): patients with some ambulatory capacity or transfer function, Middle disease stages (Stages 4–6): non-ambulatory patients who either have no difficulties with hand-to-mouth function or do not require any form of ventilation, or experience a limitation in only one of these two domains Late disease stages (Stages 7–8): non-ambulatory patients without hand-to-mouth function in combination with night-time or full-time mechanical ventilation.
This grouping enables more robust analysis while maintaining the clinical relevance of disease progression.
Data collection
Electronic case report form (eCRF)
The eCRF collected information on sociodemographic characteristics, DMD disease-specific variables (e.g., DMD mutation type, fractures), comorbidities (current and since diagnosis), corticosteroid treatment information (including dosing, length of use etc) since diagnosis, types of non-corticosteroid treatment use (in the last 12 months), and HCRU (number of consultations, surgeries, hospitalisations). The time required to complete the survey was approximately 20 min per patient.
Patient and public involvement engagement form (PPIE)
A corresponding patient and caregiver survey (PPIE) was developed to collect patient-centric outcomes directly from patients and their caregivers, collecting sociodemographic information, HRQoL, and current disease stage questions. Additional questions covered sociodemographics, functional support needs (e.g., caregiver hours), and DMD-related resource utilization. Within the PPIE Caregivers completed the Work Productivity and Activity Impairment questionnaire (WPAI) to assess the impact of caregiving responsibilities on their ability to work. The WPAI measures four components: absenteeism (work time missed), presenteeism (impairment while working), overall work productivity loss (a combination of the former), and activity impairment. Data were collected with a 7-day recall period, and annual productivity losses were extrapolated by assuming 48 working weeks per year. The results informed the calculation of indirect costs due to caregiver absenteeism and reduced productivity. Most costs were captured retrospectively over the last 12 months from the index date, apart from caregiving hours and lost productivity which were captured with a recall period of 7 days. The PPIE also included several validated instruments to measure HRQoL:
EQ-5D-5L / EQ-5D-Y (self and proxy versions): These are generic preference-based measures of HRQoL. The EQ-5D-5L consists of five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each with five severity levels. The EQ-5D-Y is adapted for use in children and adolescents. Health states were converted into utility scores using the Belgian value sets, with scores typically ranging from < 0 to 1 (full health). A higher utility score reflects better HRQoL.
Costing sources
Costs of illness were categorised as direct medical, direct non-medical and indirect costs. 16 Direct medical costs included consultations (neurologists, cardiologists, pulmonologists, physiotherapists, occupational therapists, nurses, and social workers), hospitalisations, and a range of diagnostic tests (e.g., echocardiogram, ECG, forced vital capacity, sleep studies). Medications included corticosteroids (deflazacort, prednisone, vamorolone), supplements (vitamin D, calcium), and other therapies (e.g., ACE inhibitors, antidepressants, testosterone). 14 Direct non-medical costs encompass, professional and informal caregiving hours, use of various transport modes (private car, taxi, ambulance), home adaptations (e.g., ramps, hoists, wheelchairs, ventilators), and therapies (physiotherapy, speech therapy, nutritional counselling, psychological support, and alternative therapies such as massage or hydrotherapy). Indirect costs were estimated based on lost productivity among patients (e.g., inability to work) and caregivers (e.g., stopping work, absenteeism, reduced work performance).
Costs were sourced from a societal perspective, including patients and payers’ costs, through the Belgian National Institute for Health (www.riziv.fgov.be) and Disability Insurance and the Belgian Center for Pharmacotherapeutic Information (www.cbip.be) in 2024.
All treatment costs were calculated at an International Unit (IU) or mg level: the cost of the package was divided by the amount of IU or mg in the package to produce the unit cost. Many functional tests are captured during consultation and therefore have no unit costs as they are captured within the unit cost for consultation. In cases where multiple cost descriptions could apply to the unit cost required, an average was taken for imputation into the dataset.
Calculating the total cost of DMD
Direct medical costs
A “bottom-up” costing approach was used to calculate the direct medical costs (DMC) per DMD patient, which involves estimating individual costs on a per patient level through the multiplication of unit costs with HCRU over a specified period of time. 14 To estimate the DMC of DMD, HCRU (i.e., the number of times a health-related treatment, service, or procedure was utilised by the patient over the past 12 months) was multiplied by its unit cost providing a per patient total cost (TC).
Where, P is the unit cost, Q is the quantity of resource use, i indicates an individual, and j is the healthcare resource item. Equation (1) was applied to all resource use items per patient and aggregated across all patients to estimate the mean direct medical cost (MDMC).
Direct non-medical costs
Direct non-medical costs (DNMC) are defined as costs that are directly attributable to the disease but are non-medical in nature (e.g., formal and informal care, home adaptations, government allowances or benefits due to DMD, assistive aids, additional therapies, …). These were calculated by capturing use of non-healthcare DMD cost-related items in the last 12 months. Patients provided the cost per item, which was multiplied by the amount of times the patient had used the item in the last 12 months, to provide an annual cost per item per patient. In cases where patients were unable to provide the specific cost per item, unit costs were used to calculate annual cost. Informal caregiving hours reported via the PPIE were valued using the opportunity cost method, as described above. While caregiver productivity losses were captured separately using the WPAI, informal care costs reflect the economic value of unpaid time spent providing care. Informal and professional care hours, as reported in the PPIE questionnaire, were recorded as the average number of hours per week over the preceding 12 months. Given the limited number of DMD patients participating in the workforce, patient-level productivity losses were minimal or not applicable in many cases. As such, caregiver productivity losses represent a more prominent component of the indirect economic burden.
Indirect costs
Indirect costs were defined as expenses not directly attributable to the disease itself but resulting from its secondary consequences. For example, productivity losses due to an inability to participate in the labor market as a result of living with DMD. To calculate indirect costs (e.g., work productivity), the human capital approach (HCA) was used. 13 The opportunity cost of labour was approximated using mean gross wages (hourly, daily, and yearly), which were multiplied by time missed from work due to DMD to estimate productivity losses. For the purposes of this study, productivity losses were calculated assuming 46 working weeks per year (i.e., 230 working days). All work productivity costs were annualised to a 12-month period.
Data quality
The data collected in the eCRF were audited for completeness, accuracy, and clarity via a combination of automated logic checks and manual validation. Data queries were resolved in consultation with clinical sites. Data were cleaned and cross-checked for missing data. The frequency and percentage of missing data were quantified for all variables and the pattern of missing data across the sample was evaluated to identify whether data were missing at random.
To minimise bias and provide accurate estimates of burden, the study population was required to be representative of the entire DMD population. To achieve this, we ensured that patients were recruited from a representative sample of physicians that manage DMD patients and a soft quota system was applied to monitor and balance patient recruitment across the 8 disease stages, with weekly reports used to track stage distribution.
Statistical analysis
All data were analyzed using descriptive statistics. Continuous variables (e.g., age, cost, number of healthcare visits) were summarized using means and standard deviations (SD), while categorical variables (e.g., use of corticosteroids, type of comorbidity, caregiver support) were presented as counts and percentages. The total cost of illness per patient was calculated by summing direct medical, direct non-medical, and indirect costs.
To estimate mean costs per disease stage (early, middle, late), data were stratified according to the 8-stage University of Leicester model and grouped accordingly. No imputation was applied for missing cost data; only completed responses were included in cost analyses. For HRQoL measures (EQ-5D), utility scores were calculated using country-specific value sets, and results were reported per disease stage.
Due to the small sample size and exploratory nature of the study, no inferential statistical tests were performed. The results are intended to provide descriptive, real-world insight into the socioeconomic burden of Duchenne muscular dystrophy in Belgium.
HRQoL
EQ-5D
To calculate utility values for the EQ-5D-Y and the EQ-5D-5L (both self-complete and proxy versions) each patient's EQ-5D health state (e.g 1-1-3-2-2) was combined with a value set. The Belgian value set was used to calculate utility values in this study since value sets for both the EQ-5D-Y 17 and EQ-5D-5L 18 versions were available.
Used versions
The version of EQ5D completed by each participant depended on their age and cognitive ability. Self-completed versions were used by patients aged 18 years or older, while proxy versions were completed by caregivers for younger children (4–7 years) or patients with cognitive delay. For participants aged 8–17 years, both self and proxy versions were collected when possible. Full details on PROMs used across age groups and cognitive abilities are provided in Supplemental Table 1
Results
Patient characteristics
As displayed in Table 1, a total of 40 patients and their caregivers were recruited. All included patients completed the patient PPIE form. Only one caregiver (of a patient in the late disease stages) did not complete the PPIE form, resulting in 98% completion of the total sample. Mean age at diagnosis was 2.65 years (SD: 3.3).
Patient characteristics.
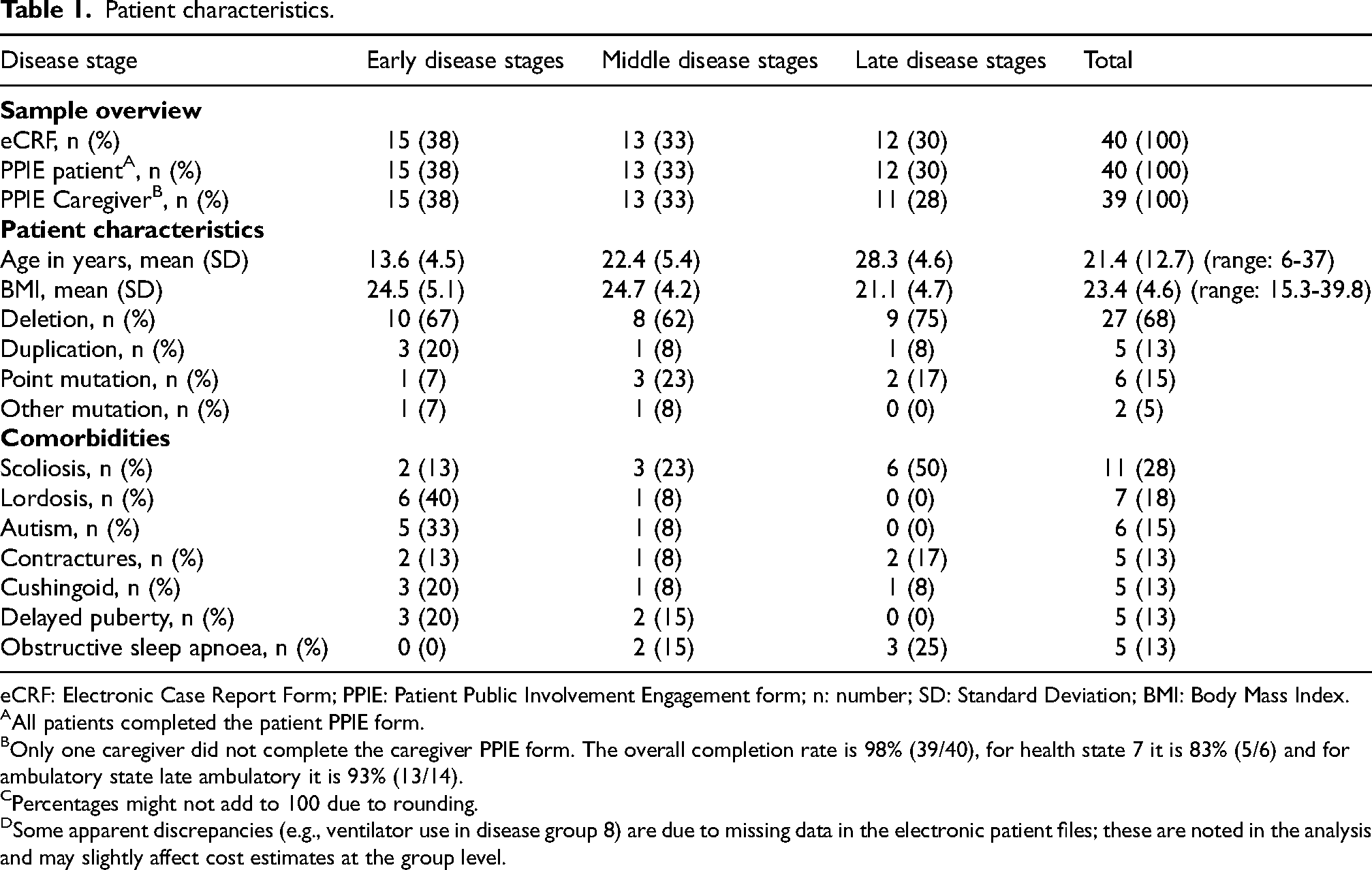
eCRF: Electronic Case Report Form; PPIE: Patient Public Involvement Engagement form; n: number; SD: Standard Deviation; BMI: Body Mass Index.
All patients completed the patient PPIE form.
Only one caregiver did not complete the caregiver PPIE form. The overall completion rate is 98% (39/40), for health state 7 it is 83% (5/6) and for ambulatory state late ambulatory it is 93% (13/14).
Percentages might not add to 100 due to rounding.
Some apparent discrepancies (e.g., ventilator use in disease group 8) are due to missing data in the electronic patient files; these are noted in the analysis and may slightly affect cost estimates at the group level.
Direct medical costs: HCRU variables.
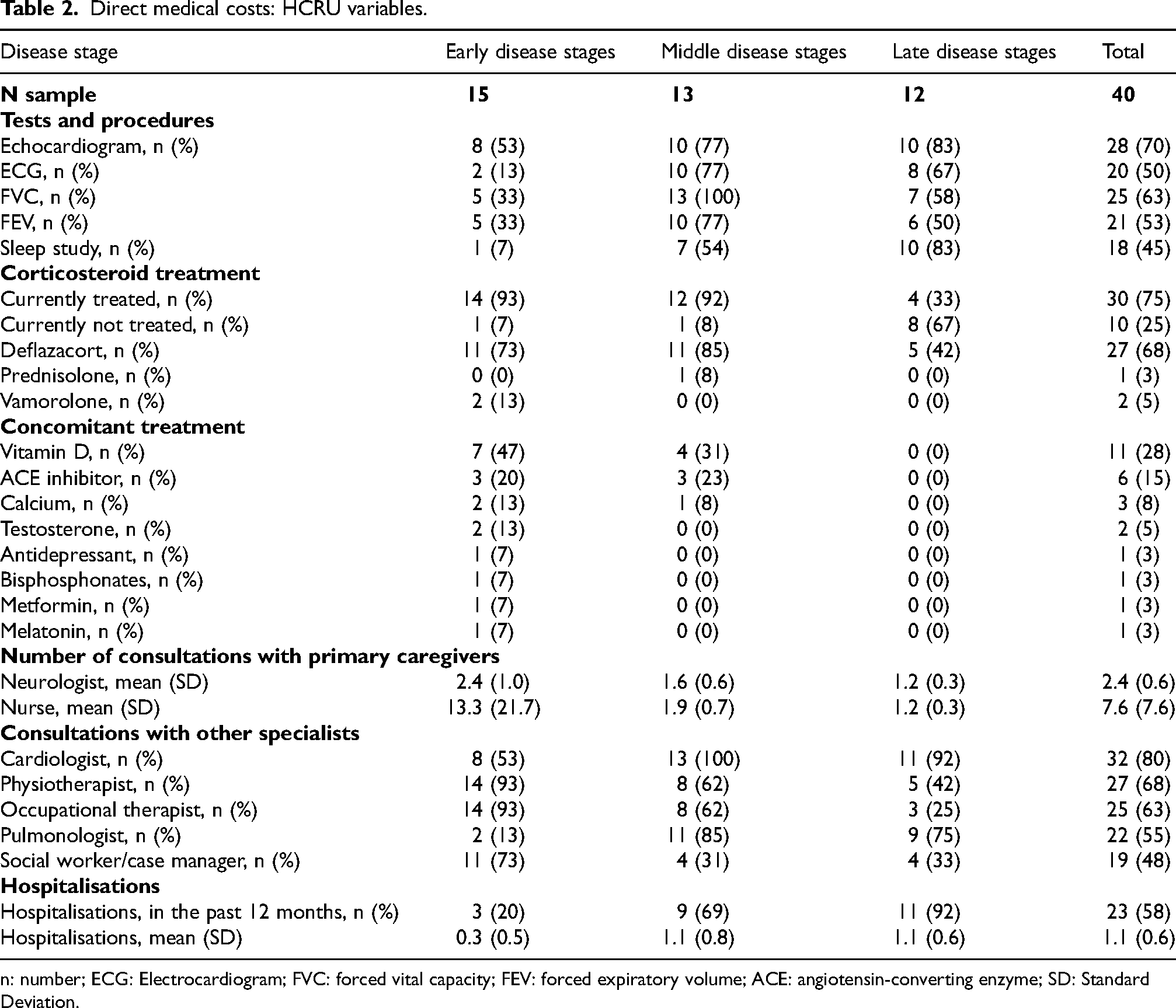
n: number; ECG: Electrocardiogram; FVC: forced vital capacity; FEV: forced expiratory volume; ACE: angiotensin-converting enzyme; SD: Standard Deviation.
Direct medical costs
Table 2 provides an overview of healthcare resource utilisation across disease stages. Corticosteroid treatment was reported for the majority of patients, with deflazacort as the most commonly prescribed corticosteroid. Various medications, such as vitamin D supplements, ACE inhibitors, and calcium, were also used. Scheduled healthcare contacts with physicians and nurses were more common than unscheduled visits, and no online consultations were reported. The majority of patients had contact with multiple specialists, and over half experienced at least one hospitalisation during the past year. Detailed frequencies and distribution across stages are presented in Table 2.
Direct non-medical costs
Table 3 summarises caregiving needs across disease stages. The majority of participants reported receiving caregiving support, either from family members or contracted professionals. Both the proportion of patients requiring support and the number of weekly caregiving hours varied by disease stage.
Variables for direct non-medical costs.
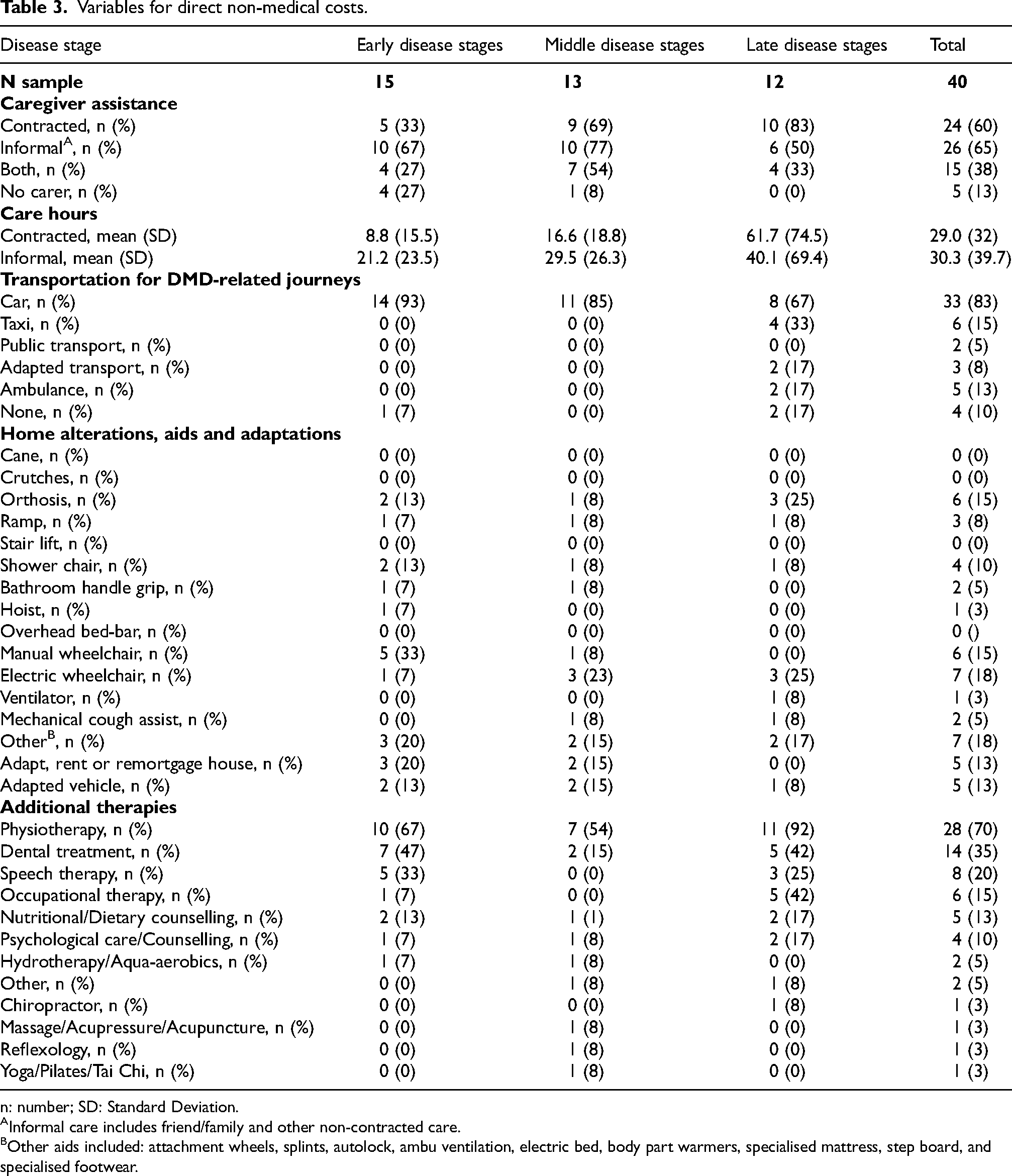
n: number; SD: Standard Deviation.
Informal care includes friend/family and other non-contracted care.
Other aids included: attachment wheels, splints, autolock, ambu ventilation, electric bed, body part warmers, specialised mattress, step board, and specialised footwear.
Table 3 presents additional non-medical resources used during the study period, including home adaptations, assistive devices, and therapeutic services. Common adaptations included wheelchairs (manual and electric), orthoses, and other assistive equipment. A subset of families reported making home or vehicle modifications due to disease-related needs. Use of different transport modes for DMD-related purposes, such as private car, taxi, or ambulance, was also captured and is summarised in Table 3.
Indirect costs
Among the 40 participants enrolled in the study, 24 (60%) were 18 years or older at index date. Out of these 24 patients, 22 have never been able to work due to DMD, and none of the participants were working at index date (missing data in two patients).
None of the caregivers had to retire due to the DMD diagnosis of their son, although 15% of caregivers reported that they had ceased working to attend to the patient's needs, half of whom were carers of patients in stages 8 (n = 3). Overall impairment for the entire sample was 46.4% (SD: 36.0), and presenteeism (31.5%, SD: 29.3) was more influential than absenteeism (17.2%, SD: 37.1).
Total annual cost of DMD
Table 4 presents the total annual societal cost of DMD per patient, stratified by early, middle, and late disease stages. The breakdown includes direct medical costs (e.g., corticosteroids, consultations, devices), direct non-medical costs (e.g., caregiving, home and vehicle adaptations, therapies), and indirect costs (e.g., patient and caregiver productivity losses). Across all categories, cost components and their relative contributions varied by disease stage. Direct non-medical and indirect costs together represented the majority of the total societal burden. Full details of the cost breakdown and standard deviations are shown in Table 4.
Total costs of DMD for society.
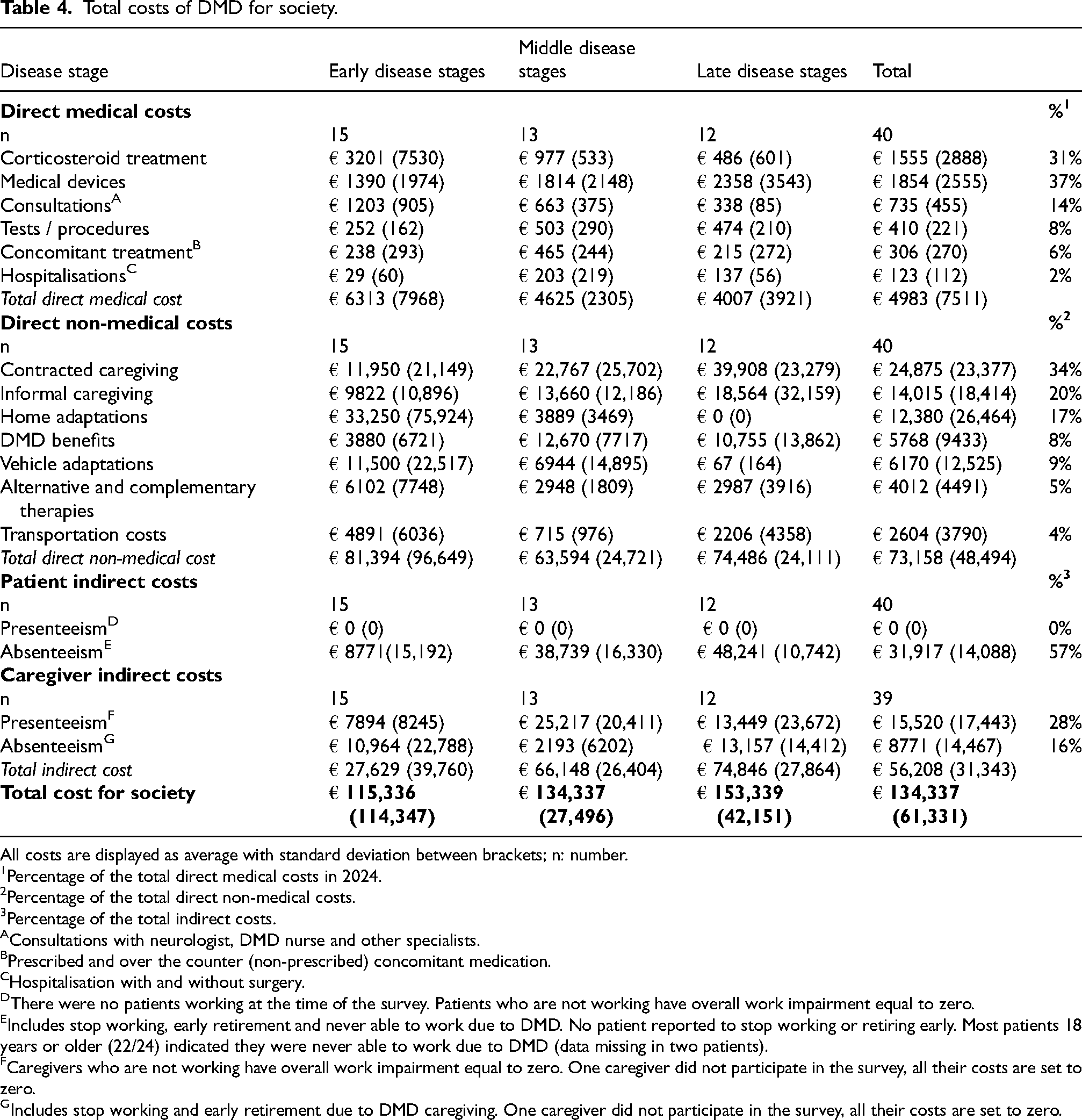
All costs are displayed as average with standard deviation between brackets; n: number.
Percentage of the total direct medical costs in 2024.
Percentage of the total direct non-medical costs.
Percentage of the total indirect costs.
Consultations with neurologist, DMD nurse and other specialists.
Prescribed and over the counter (non-prescribed) concomitant medication.
Hospitalisation with and without surgery.
There were no patients working at the time of the survey. Patients who are not working have overall work impairment equal to zero.
Includes stop working, early retirement and never able to work due to DMD. No patient reported to stop working or retiring early. Most patients 18 years or older (22/24) indicated they were never able to work due to DMD (data missing in two patients).
Caregivers who are not working have overall work impairment equal to zero. One caregiver did not participate in the survey, all their costs are set to zero.
Includes stop working and early retirement due to DMD caregiving. One caregiver did not participate in the survey, all their costs are set to zero.
HRQoL burden of patients and their caregivers
Table 5 summarises EQ-5D utility scores completed by patients and caregivers across early, middle, and late disease stages. EQ-5D-Y proxy scores showed a decline in health-related quality of life from early to middle stages. Similarly, patient-completed EQ-5D-Y and EQ-5D-5L scores were lower in the middle stages compared to early stages. Caregiver EQ-5D-5L scores remained relatively stable across all stages.
HRQoL burden of patients and their caregivers.
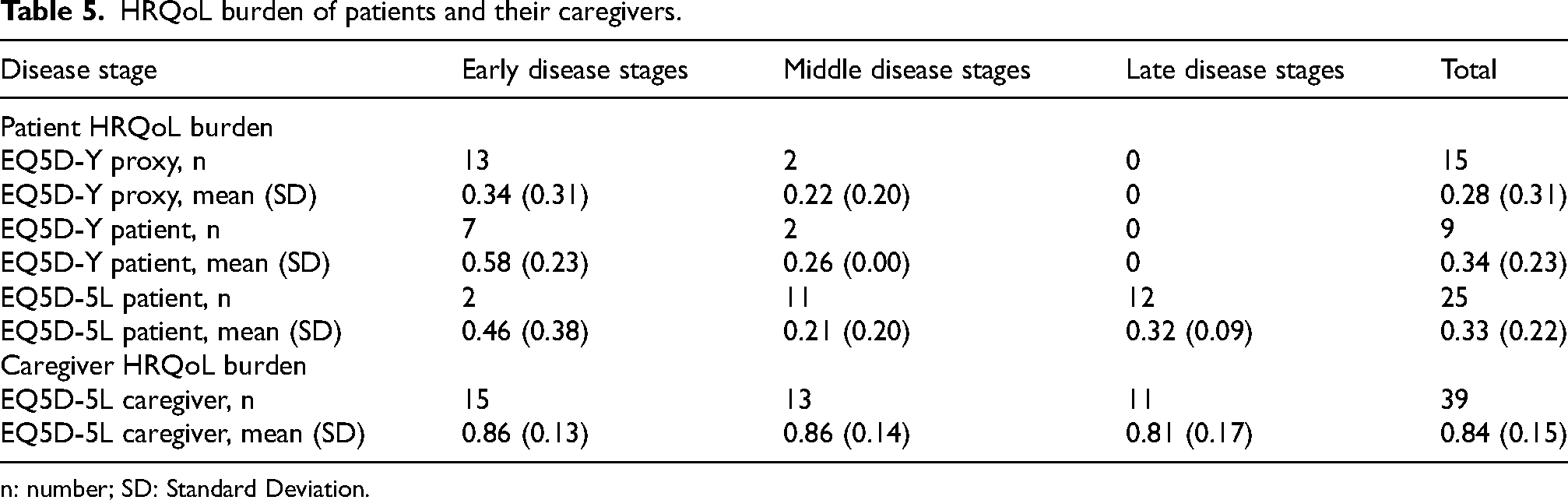
n: number; SD: Standard Deviation.
Discussion
This study aimed to provide a detailed assessment of the health-economic burden and quality-of-life implications of DMD in Belgium, utilizing the University of Leicester's 8-stage model for DMD. 19 To ensure robust results and sufficient sample size, we additionally grouped the results into three disease stages: early (stages 1–3), middle (stages 4–6), and late (stages 7–8).
The findings revealed a substantial societal cost, averaging €134,337 per patient annually. In general, societal costs increased with disease progression. On average, costs were estimated at € 115,336 in early disease stages, € 134,337 in the middle disease stages, and € 153,339 in the late disease stages.
Among the different cost components, direct non-medical cost constituted the largest share of the societal burden, accounting for 54% of the total cost. Within this category, professional care (34%), home adaptations (17%), and informal care (20%) represented significant contributors. Indirect costs comprised 42% of the total, primarily driven by patient unemployment (57%) and reduced caregiver work productivity (28%). While informal care and caregiver productivity losses were treated as distinct components, we acknowledge the potential for partial overlap between these categories; however, both were retained to capture complementary aspects of the societal burden of DMD. By contrast, direct medical costs were relatively minor, representing only 4% of the societal burden. Because the use of other healthcare resources (such as diagnostic procedures, non-steroidal treatments, and hospitalisations) was limited, corticosteroid therapy and medical devices, though low in unit cost, accounted for the largest proportion of total direct medical costs (31% and 37%, respectively).
This is the first study to investigate the financial burden of DMD in Belgium. Although limited resources allowed for the inclusion of only a small sample (N = 40), efforts were made to ensure balanced and representative recruitment across different disease stages. Nonetheless, certain stages within the 8-stage DMD health state model were underrepresented.
In the Belgian context, we believe our sample reflects the broader DMD population. By governmental regulation, all patients with neuromuscular disorders must receive follow-up care within recognized neuromuscular reference centers, all of which are affiliated with university hospitals. Moreover, the procedures for accessing reimbursed medications, adaptive aids, therapies, and other services are uniform across the country.
All participants in this study were recruited from the largest neuromuscular center in Belgium, which follows the country's largest DMD cohort. The recruitment process was carefully supervised to ensure the inclusion of patients from various stages of disease progression. Therefore, we believe our findings provide a meaningful estimate of the actual financial burden of DMD in Belgium. Nonetheless, future studies should aim to include larger cohorts to enhance representation across all disease stages.
Although no prior studies have evaluated the health-economic burden of DMD in Belgium, comparable data are available for the UK, Italy, Portugal and Germany.2,20 Among these countries, Belgium exhibited the highest total societal cost (€128,180), with the UK ranking second with €98,857. While direct (medical and non-medical) costs were similar between Belgium (€77,308) and the UK (€73,845), Belgium's indirect costs were nearly twice as high as those observed in the UK and other European nations. This discrepancy may be attributable to the inclusion of productivity loss due to work cessation. 15
In terms of the proportional distribution of the total societal cost, direct costs in Belgium (58%) closely aligned with direct costs in Italy (54%) and Germany (67%), whereas the UK demonstrated a relatively higher proportion of direct costs (83%). Scheiber-Katz et al. (2014) provided alternative cost estimates for DMD in Germany, reporting direct (€74,284, 2024), indirect (€42,419, 2024), and total (€116,704, 2024) costs. 14 These values exceed those reported by Landfelt et al. (2014) but align more closely with the estimates from this Belgian study, particularly regarding the proportion of direct costs (Germany: 63% versus Belgium: 60%) and overall societal burden (Germany: €116,704 vs. Belgium: €128,180). Compared with the study by Cavazza et al. (2016), the Belgian cost estimates rank among the highest in Europe, supporting our findings. 21 Particularly in comparison with Eastern European countries, Belgian costs are several times higher and are more closely aligned with those reported in Germany. Cavazza et al. also emphasize that cross-country differences in cost reflect the diverse healthcare pathways adopted, shaped by varying policy choices, resource allocation strategies, and identified care priorities. 21
HRQoL was assessed across the study cohort with different version of the EQ-5D, with full data available for 34 patients. Utility scores had an average of 0.34 across the cohort. Despite small sample sizes and absence of formal statistical analyses, EQ-5D results consistently indicated a decline in HRQoL as DMD progressed.
Strengths
This study employed a site-based methodology, ensuring high data quality due to the validation processes applied to all eCRFs. This resulted in a robust dataset for 40 patients and their caregiver, including comprehensive HCRU data. Additionally, the methodology facilitated a 100% completion rate for patient-reported information, allowing for full linkage between eCRF and patient-reported outcome data. This enabled the calculation of total societal cost and the examination of healthcare utilization and patient-related outcomes in all cases. The use of a soft quota system for pediatric and adult patients ensured a relatively balanced distribution across the 8-stage DMD model, permitting more detailed analyses of cost and HRQoL trends. This approach was particularly valuable for assessing indirect cost, societal cost, and HRQoL utility scores derived from the EQ-5D. Furthermore, this study is among the first to apply the University of Leicester's 8-stage model for DMD to assess the economic and HRQoL impact of DMD at a national level, enabling a more granular analysis of disease progression.
Limitations
Despite efforts to achieve a balanced sample distribution, the overall sample size was limited (n = 40), resulting in particularly low representation in certain disease stages and prohibiting formal statistical analyses to compare different groups. Expanding the sample size would likely enhance the robustness of findings and improve the identification of trends in costs and HRQoL outcomes. The small sample size, made it particularly challenging to detect trends in EQ-5D-Y and EQ-5D-Y proxy results. Additionally, cost estimates for earlier disease stages may not fully reflect actual expenditures at that stage, as patients and families may anticipate future needs by purchasing equipment such as wheelchairs in advance. Similarly, reduced use of additional therapies in later stages may reflect declining motivation or increased fatigue rather than a lack of necessity. Moreover, recruitment was limited to a single study site, restricting the geographical scope. A multicenter approach across Belgium could enhance representativeness and provide a more comprehensive estimate of the actual societal cost of DMD. Finally, the societal perspective adopted in this study necessitated a focus on the most relevant cost elements, potentially omitting some indirect costs.
Further research
As the first study to assess the burden of illness associated with DMD in Belgium and among the earliest to apply the University of Leicester's 8-stage model, further research is warranted to expand upon these findings. A broader investigation could refine cost and HRQoL estimates, particularly for underrepresented disease stages (stages 2, 3, 5, and 6). Additionally, further exploration of caregiver-related quality of life is needed. A more detailed domain-level assessment of existing measures could elucidate their limitations, or alternatively, the use of broader instruments such as the ICECAP-A could provide a more holistic understanding of caregiver burden beyond specific health-related attributes.
Conclusion
This is the first study to provide an estimate on the socio-economic burden of DMD in Belgium, and the first to provide data across the University of Leicester 8-stage model of DMD. In combination with other recent and ongoing studies, this dataset can help identify the key drivers of disease burden in DMD, especially as the disease progresses.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261432406 - Supplemental material for Burden of illness of Duchenne muscular dystrophy in Belgium: A retrospective, descriptive, cross-sectional study
Supplemental material, sj-docx-1-jnd-10.1177_22143602261432406 for Burden of illness of Duchenne muscular dystrophy in Belgium: A retrospective, descriptive, cross-sectional study by Sam Geuens, Lauranne Beeckman, Stephen Dukacz, Jonathan Evans, Eva Gielis, Cheryl Jones, Nikita Lamaire, Nate Posner, Thomas Van Stappen, Yunchou Wu, Liesbeth De Waele and Kristl G. Claeys in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
We genuinely thank all participants for contributing to this study.
This work is generated within the European Reference Network for Rare Neuromuscular Diseases ERN EURO-NMD; Project ID No. 739543.
Author contributions
TVS, LB, NP, SD, LJ, JE, YW, CJ, LDW and KGC were involved in the conception and design of the study. TVS, JE, JC, YW, LB, LDW and KGC were involved in the acquisition and analysis of the data. TVS, LB, NP, SD, LJ, JE, YW, CJ, LDW and KGC played an important role in the interpretation of the results. SG, JE, YW, CJ, LDW and KGC drafted a significant proportion of the manuscript. All authors reviewed the final manuscript.
Funding
The study was sponsored by Pfizer, meaning Pfizer was legally responsible for the study design, conduct and oversight on the study. Pfizer provided funding for the study.
Conflict of interest
LDW has received a research grant from Pfizer, honoraria paid to the KU Leuven for a lecture during a symposium for Dyne Therapeutics and for advisory board roles for Italfarmaco, Roche, Pfizer, Dyne Therapeutics, Santhera Therapeutics, Entrada Therapeutics, Wave Lifesciences and Genethon. TVS, NP and LJ are employees of Pfizer and hold stock/stock options.
Data availability statement
The data supporting the findings of this study are available within the article and/or its supplementary material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.