
Abstract
Background
Thymidine Kinase 2 deficiency (TK2d) is a rare, mitochondrial DNA (mtDNA) depletion/deletions syndrome leading to a severe and progressive myopathic disorder. Nucleoside supplementation (deoxythymidine and deoxycytidine) has been shown to favorably alter the disease's course, particularly in severe infantile-onset cases. Long-term data on efficacy and safety, especially in the adult patient population, remain limited.
Methods
This is a retrospective, long-term follow-up study of 14 TK2d patients (five children and nine adults with childhood-onset disease) treated with nucleosides. Patients were systematically evaluated over a period ranging from 9 to 36 months, with assessments conducted every 3 months during the first year of treatment, and every 6 months thereafter. Comprehensive functional assessments of motor, respiratory, and bulbar function were performed. Periodic measurements of liver and pancreatic function monitored safety and tolerability.
Results
All 14 TK2d patients showed beneficial effects across motor, respiratory, and bulbar function domains. Among pediatric patients, a rapid treatment response was observed early on, with functional gains sustained and continuing beyond 12 months of therapy. Adults experienced substantial improvements in motor and respiratory capacity but most of them reported severe gastrointestinal symptoms. Liver and pancreatic enzymes abnormalities were noticed mainly in adults.
Conclusions
Deoxythymidine and deoxycytidine were found to be safe and beneficial in this long-term cohort of TK2d patients, but elevation in liver and pancreatic enzymes were present and required regular monitorization. This study provided valuable evidence supporting this therapy as an effective and safe, long-term disease-modifying treatment option for both pediatric and adult patients.
Keywords
Introduction
Thymidine kinase 2 deficiency (TK2d) is a rare autosomal recessive mitochondrial disorder that causes a myopathic form of mitochondrial DNA (mtDNA) depletion/multiple deletions syndrome. The TK2 enzyme contributes to maintaining a balanced mitochondrial nucleotide pool by mediating the phosphorylation of pyrimidine deoxyribonucleosides, specifically deoxycytidine (dC) and deoxythymidine (dT). 1 Historically, TK2d has been primarily associated with rapidly progressive and fatal myopathy, typically observed in pediatric cases. 1 However, the clinical phenotype is highly heterogeneous, spanning aggressive presentations such as encephalomyopathy 2 and the milder myopathic phenotype characterized by adult-onset (symptoms appearing after age 12).3–5 Disease-onset between ages 2 and 12 is classified as an intermediate phenotype. 3 A recent publication from our group detailed the clinical features of 19 childhood-onset patients, reporting severe motor involvement in 30% and severe respiratory involvement in 75%, underscoring the debilitating nature of the disease in this group. 6
Nucleoside supplementation therapy using deoxycytidine (dC) and deoxythymidine (dT) for TK2d has been recently approved by the United States (US) Food and Drug Administration (FDA) for TK2d patients with age-at-onset ≤12 years and demonstrated significant potential as a disease-modifying therapy, positively influencing survival rates, motor, bulbar, and respiratory function,7,8 and also improving quality of life. 9 The treatment is generally reported as safe; however, drug suspension was followed by an increase in transaminases in two adult patients 10 Most of the literature data regarding the nucleoside supplementation come from case reports or small series and do not show clear how the liver monitoring was performed. In addition to that, most current efficacy and safety data involve children, leaving an higher gap in the understanding of long-term treatment efficacy, side effects, and liver function in adults.
Here, we present a long-term follow-up of 14 treated TK2d patients, including nine adults with childhood-onset disease, for whom comprehensive data are particularly scarce. This study detailed motor, respiratory, and bulbar outcomes, as well as adverse effects, and liver and pancreatic enzymes associated with the therapy in this patient cohort providing important clues about the management of those patients.
Methods
Patients
Retrospective and observational data from 14 patients with TK2d treated by dC and dT were collected. Medication was provided by UCB Pharma (Belgium) through the Compassionate Use Program (CUP). Patients signed a written informed consent form to receive the therapy and a separate written informed consent form to participate in the study. All patients were followed at the Hospital das Clínicas of FMUSP. Data was collected through chart review following the approval by the local ethics committee.
Dosage of medication and safety assessment
Dosage was escalated from 200 mg/kg/day (100 mg/kg/day for each compound) to a maximum of 800 mg/kg/day (400 mg/kg/day for each compound). The dose was increased by 200 mg/kg/day every two weeks, or more, depending on patient tolerance. Each envelope contained 4 g of the nucleoside compounds (2 g of dC and 2 g of dT) and was diluted in 100 to 200 mL of water, adjusted based on patient tolerance to the medication and the required total intake volume. Liver function tests were monitored before dosing, after the first month, at three months, at six months, and every six months thereafter. In cases where liver enzyme levels increased to greater than three times the upper limit of normal (ULN), the nucleoside dose was reduced, and tests were repeated weekly until resolution (defined as normalization or a maximum increase up to three times the ULN). The patients that presented with transaminases elevation underwent additional tests, including a liver ultrasound and comprehensive blood tests focused on the differential diagnosis for hepatitis (e.g., hepatitis serologies and antibodies). Pancreatic enzymes were not routinely monitored during the first six months of follow-up. After an incidental finding of elevated lipase in one patient, amylase and lipase regular screening was initiated for all others and included in the monitoring. If pancreatic enzymes were persistently (more than one measure) above three times the ULN, an abdominal computed tomography (CT) scan was performed.
Clinical evaluation
Clinical evaluations were systematically performed at baseline, then every three months up to one year of treatment, and every six months thereafter. The assessment protocol included a neurological examination, measurement of weight and vital signs, and a comprehensive questionnaire gathering clinical and self-reported data. Motor and respiratory function assessments were performed on the same day by a trained physiotherapist. Motor function was evaluated using either the Motor Function Measure-32 (MFM32) 11 or the Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP-INTEND), 12 selected based on the patient's age and maximal motor function. For ambulatory patients, timed tests were also performed based on ability, including the 6-Minute Walk Test (6MWT), 5 Times Sit to Stand (5xSTS), timed Gowers’ maneuver, time to climb four steps, and time to descend four steps. All capable patients underwent seated spirometry and peak expiratory flow (PEF) testing prior to the motor examination. At each visit, patients were interrogated regarding food preferences and the feeding process (e.g., route and duration), and subsequently classified using the Neuromuscular Disease Swallowing Status Scale (NDSSS). 13 Patients were also specifically queried about changes in voice tone, fatigue during eating and speaking, and the frequency of choking episodes.
All statistical calculations were performed using R packages. Continuous variables were presented as mean and standard deviation (SD) or median and interquartile range (IQR). Discrete and categorical variables were presented as counts and percentages. To investigate the relationship between CK levels and transaminases, a multivariate analysis was performed to evaluate the correlation between hepatic enzymes (ALT, AST, and GGT) and CK using analysis of covariance in R package (rmcorr). Missing data was handled individually and the denominator for each variable was adjusted by subtracting subjects for whom data were not available. All patients performed all the pre-specified visits.
Results
We presented data from 14 patients (6 female and 8 male) with TK2d who were receiving dC and dT supplementation. Patients had a mean age of 20 ± 14 years and a mean disease duration of 17 ± 14 years. Three patients had infantile-onset disease (symptom onset before the age of two), while the remaining eleven patients had childhood-onset (symptom onset from 2 to 12 years of age) and a median onset age of 2 years. Nine of the eleven childhood-onset patients were adults at the time of follow up. A shorter follow-up from four of the children was previously published 6 ; this published data was included in the current analysis for comparison with a longer follow-up period.
Data were collected from all patient visits, starting at baseline (1–2 months before treatment initiation), and were followed every three months up to one year, and then every six months thereafter. The duration of follow-up varied by patient, depending on their enrollment time in the compassionate use program (CUP): 36 months for one patient, 18 months for eight, 12 months for four, and 9 months for one patient.
At the pre-dosing visit (baseline), three patients were bed-bound, ventilator-dependent, and fed exclusively through a gastrostomy tube (G-tube). Of these three, two had only anti-gravitational movements, and one had no voluntary movements. Eight patients were able to walk. All ambulatory patients used non-invasive ventilatory support (NIVS)–BiPAP during sleep-time and were orally fed. Recurrent respiratory infections and recurrent myalgia were frequent symptoms reported by the patients (Tables 1 and 2).
Summary of clinical outcomes throught 24 months of treatment in patients aged 12 years old and below.
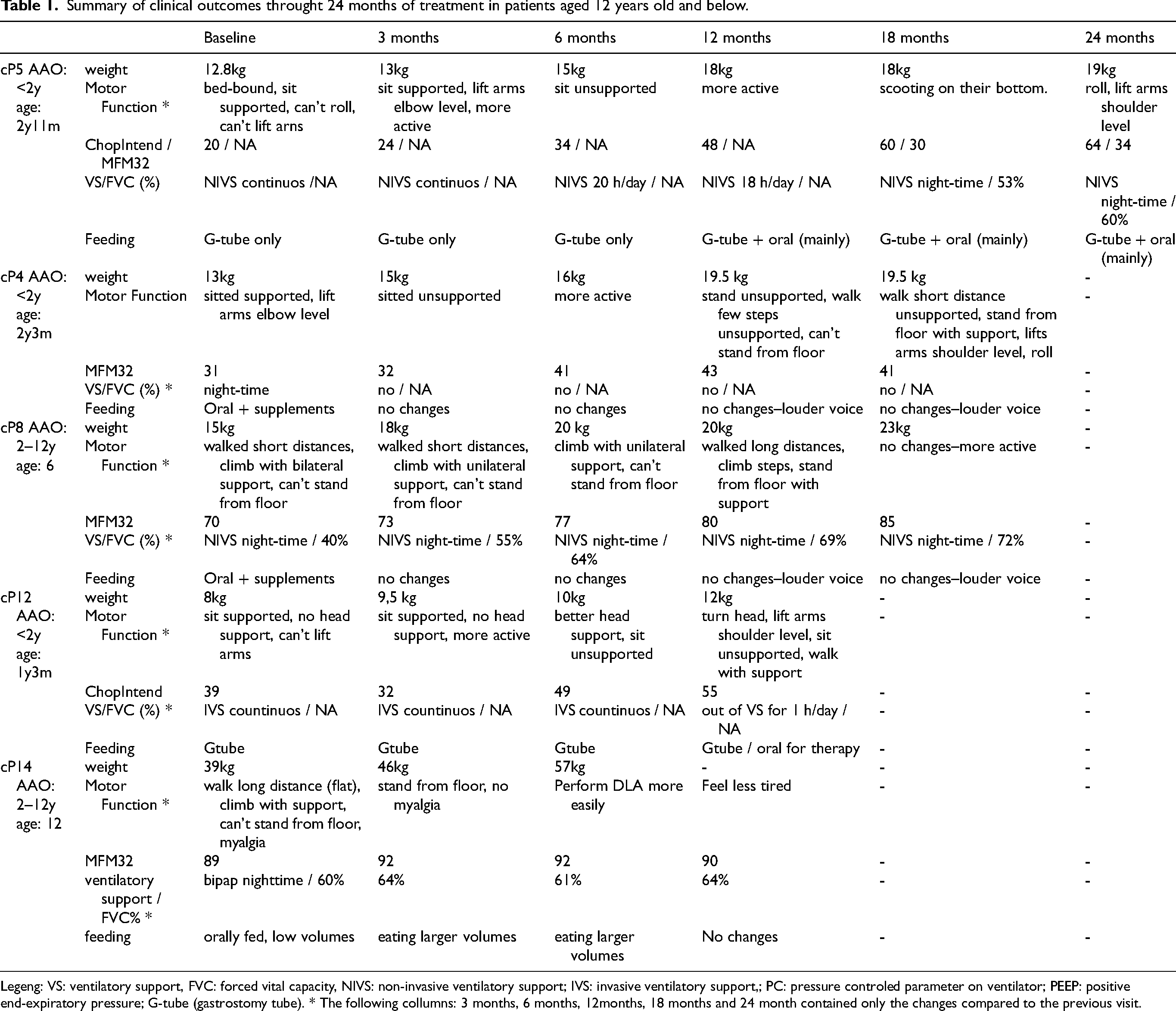
Legeng: VS: ventilatory support, FVC: forced vital capacity, NIVS: non-invasive ventilatory support; IVS: invasive ventilatory support,; PC: pressure controled parameter on ventilator; PEEP: positive end-expiratory pressure; G-tube (gastrostomy tube). * The following collumns: 3 months, 6 months, 12months, 18 months and 24 month contained only the changes compared to the previous visit.
Summary of clinical outcomes throught 12 months of treatment in patients aged above 12 years old.
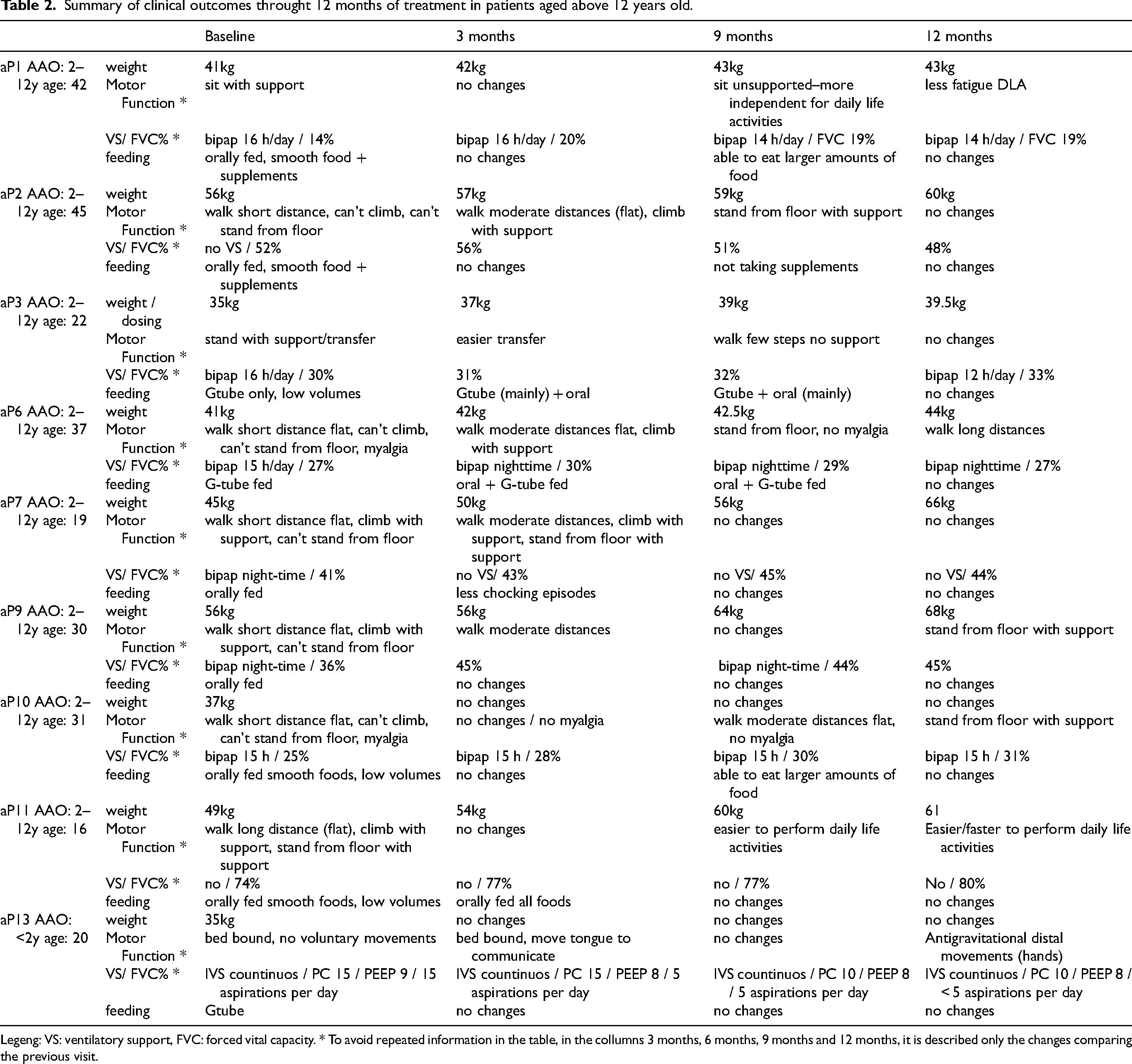
Legeng: VS: ventilatory support, FVC: forced vital capacity. * To avoid repeated information in the table, in the collumns 3 months, 6 months, 9 months and 12 months, it is described only the changes comparing the previous visit.
Adverse effects and tolerability
Adverse events are detailed in supplemental table S1. Patients initiated therapy at 200 mg/kg/day, with the target total dose being 800 mg/kg/day. The most common adverse events reported were gastrointestinal (GI) symptoms, including diarrhea, abdominal pain, and nausea. While all patients presented GI symptoms within the first weeks of treatment, and some reported subsequent improvement, 64% of patients remained symptomatic at the final evaluation. In addition to that, some patients, particularly adults, also reported difficulties related to the high fluid volume of medication required daily and some patients were unable to reach the full target dose for this reason.
All pediatric patients presented with manageable GI symptoms and successfully achieved the maximum dose of 800 mg/kg/day within the first six months of therapy. Liver enzyme abnormalities were observed in only one patient (cP12) who presented an increase in ALT above 5× ULN with no increase of CK or bilirubin after a dose adjustment. The enzymes decreased to his baseline within 10 days of the adjustment (supplemental table s1, Figure 1C).
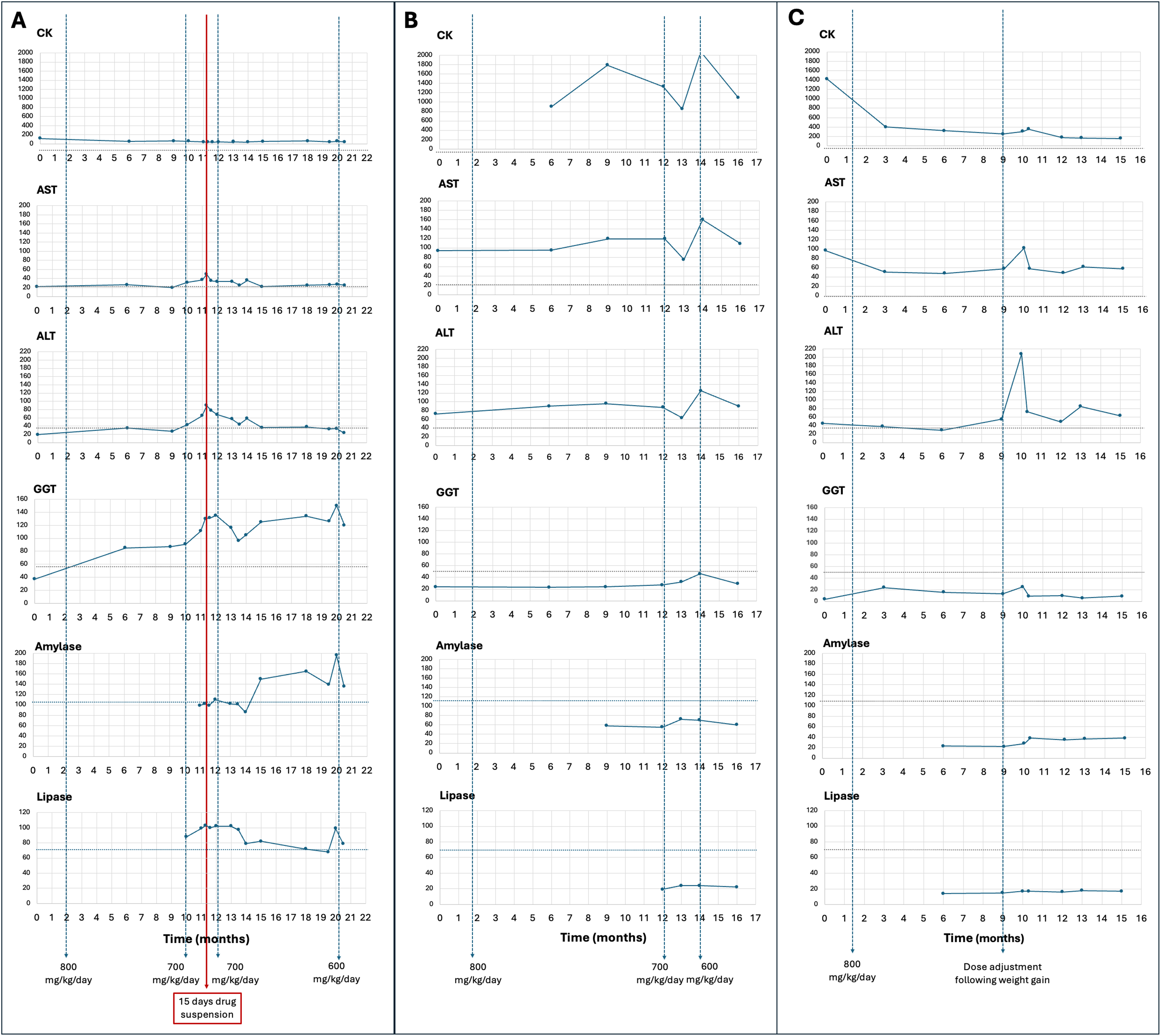
Longitudinal tracking of CK, AST, ALT, GGT, Amylase and Lipase for three patients aP1 (A), aP7 (B), and cP12 (C) over the course of their treatment month by month. Vertical dashed lines indicated clinical interventions or dosage adjustments.
The adult cohort experienced more pronounced GI symptoms. Of the nine patients, four already presented chronic diarrhea and intolerance to high fluid volumes on baseline. They presented severe GI symptoms and difficulties to reach the full dose of the supplementation. At the last evaluation, 6/9 patients were still experiencing daily episodes of diarrhea, and four of them were receiving lower doses of the nucleoside supplementation due to ongoing gastrointestinal intolerance (supplemental table s1).
Most of the adults (7/9) also manifested liver enzyme abnormalities during the follow up (detailed described in supplemental table s1) with no consistent pattern. Four patients presented high CK at baseline and all of them had elevation in AST and ALT. Amylase and Lipase were not accessed at baseline. Four patients had elevation of CK during the treatment and also presented elevation of AST and ALT. Two adult patients had ALT elevation above 2x ULN (aP1 and aP7). For those, blood tests were repeated every 10 days until returning to baseline. High ALT values were sustained for aP1 which also had elevation of GGT and lipase, which resulted in dose reduction for 700 mg/kg/day. Follow up exams showed that transaminases were still increasing. The drug was suspended for 15 days, transaminases decreased and then treatment was restarted on 700 mg/kg/day. Transaminases increased again and the dosing was reduced for 600 mg/kg/day (figure 1A). Her lipase reached up to 3x ULN, but she remained with no symptoms of acute pancreatitis. She had an extensive investigation for the differential diagnosis regarding hepatic and pancreatic dysfunction including serum antibodies and abdomen imaging (CT-scan and ultrasound) which detected biliary stones (in the absence of signs of pancreatitis) and renal cysts (with normal renal function). Regarding aP7, the sustained elevation of transaminases and CK in addition to pronounced GI symptoms, leaded to a dose reduction to 600 mg/kg/day, followed by stabilization of blood tests (figure 1B). One additional patient had a mild and isolated increase of GGT. AP13 presented with non-related hyponatremia, which resolved after sodium supplementation and adjustments to the total fluid intake volume. At 12 month visit, she presented elevation of transaminases which returned to baseline after temporary drug suspension (supplemental table s1).
After aP1 showing also increases on lipase and amylase, these enzymes were screened in all remaining patients after that and then included in the regular routine tests. A mild increase of amylase was found in additional 4 patients, three of them had also a mild increase of lipase with no clinical signs or symptoms of pancreatic dysfunction.
A repeated measure correlation was performed to evaluate the correlation between transaminases (ALT, AST, and GGT) and CK. CK and ALT correlation was not significant (r = 0.15 and p-value = 0.23), CK and GGT correlation was not significant (r = 0.16 and p-value = 0.23), and CK and AST correlation was significant (r = 0.55 and p-value < 0.001).
Effect on bulbar function and weight
Before initiating treatment, five patients were fed by G-tube, and nine were fed orally. All patients, however, reported difficulties gaining weight and used supplements to achieve adequate nutrition. Two patients (cP5 and aP3), who were fed exclusively through a G-tube, regained the ability to eat orally at 12 and 9 months, respectively, though the feeding device was not removed. aP13 and cP8 reported a reduction in the frequency of daily aspirations. Of the eight patients who were orally fed at baseline, 50% reported fewer choking episodes.
Thirteen patients or their guardians completed a questionnaire to evaluate bulbar function (swallowing and speech) at six months of therapy, capturing the patients’ self-perception. After treatment, 11 patients/guardians reported positive changes in their feeding process: nine patients reported being able to eat larger volumes and experiencing fewer choking episodes, and eight patients reported feeling less tired during meals, while nine patients reported eating faster. Nine patients reported changes in their voice and speech, noting they felt less tired when speaking. A total of 11 patients noticed they were being understood more easily by others.
During treatment, all patients presented with weight gain. They had an average increase in total body weight of 6% at the three-month visit and 16% at the nine-month visit. At the six-month visit, seven patients (six of whom were adults) reported positive changes in their speech, including an increase in voice tone, being better understood, and feeling less tired when speaking.
Effect on motor function
Eleven patients were followed using the MFM32 scale, which showed an 8% increase in the total score. Two patients were followed initially with the CHOP-INTEND scale: cP5 showed a pronounced increase from a baseline of 20 points to 39 at 9 months, 48 at 12 months, and 64 at 24 months, then he was followed with MFM20 For cP12, the score decreased initially from 39 to 32 due to a severe pulmonary infection in the first month of therapy but then rebounded to 52 at the twelve-month visit.
Eight patients were able to perform the 5xSTS test and had a reduction of 40% in the time required to complete the task. Eight patients were able to ascend and descend four steps, demonstrating a 64% decrease in time to ascend and an 14% decrease in time to descend. Three of these eight patients were only able to perform the task after the three-month visit. Seven patients were able to perform the 6MWT at baseline, and one patient was able to perform it after the first three months of treatment. The follow-up revealed an improvement of 71 ± 40 meters at nine months and 85 ± 35 meters at 12 months (Figure 2).
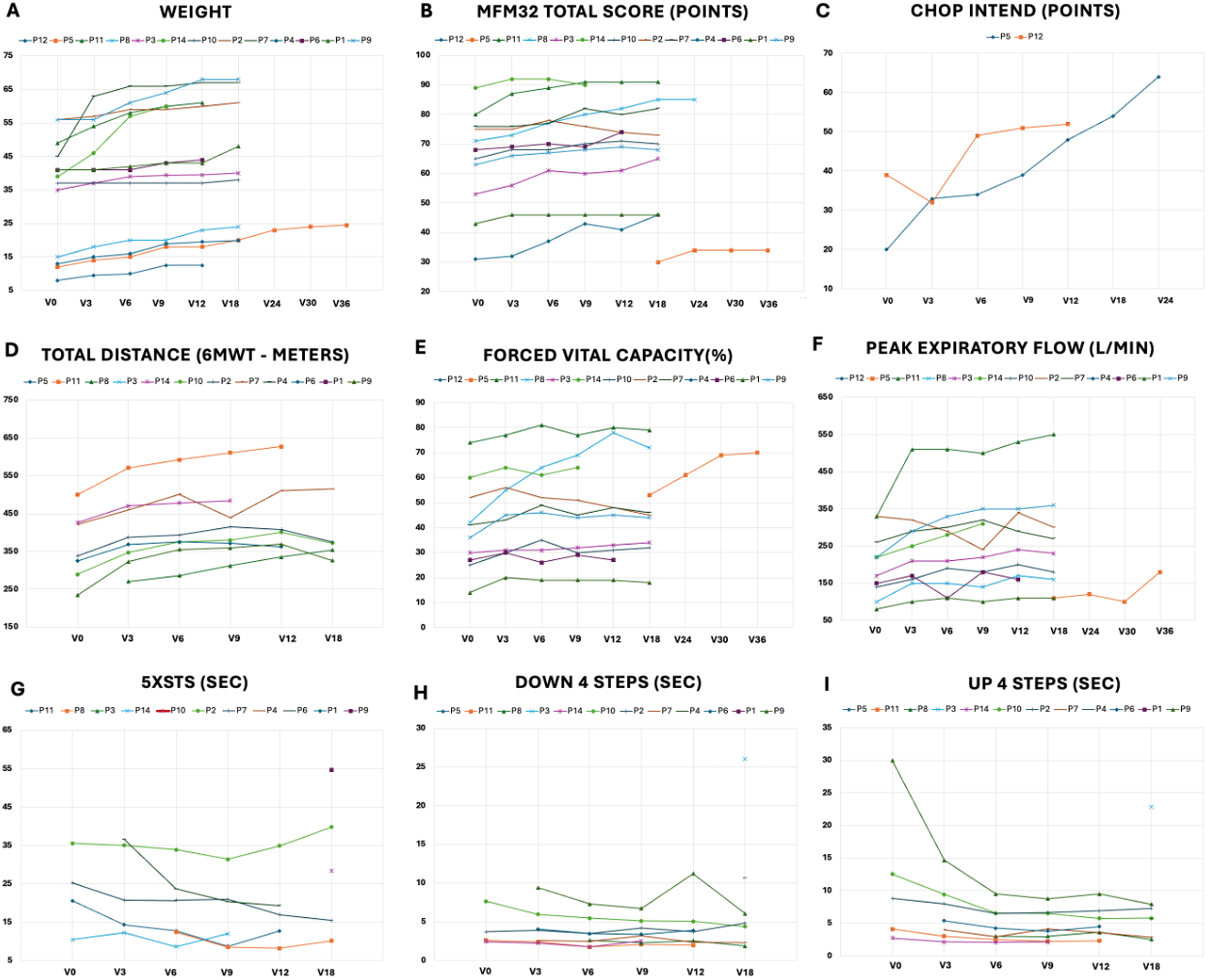
Functional measures of TK2d patients treated with nucleosides supplementation across visits: V0 = baseline; V3 = 3-months visit; V6 = 6-months visit; V9 = 9-months visit; V12 = 12-months visit; V18 = 18-months visit, V24 = 24-months visit, V30 = 30-months visit and V36 = 36-months visit. Variables included in this analysis were weight (A), total score of Motor Function Measure-32 (B); total score of Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (C); the total walked distance in the 6 min walking test (D), the percentage of seatedforced vital capacity (E), the seatedpeak expiratory flow measure (F), the time in seconds to perform 5 times sit to stand test (G), the time in seconds to climb up four steps (H), and time in seconds to climb down four steps.
Motor milestones were attained or regained by seven patients. Three patients regained the ability to sit without support (cP4, cP5 and cP12). One patient regained the ability to walk (cP4) while another reached this milestone for the first time (cP12). Additionally, cP8 gained the ability to jump and hop, and four patients aP3, cP4, aP6 and aP10) achieved the ability to stand from floor using a chair support.
Five patients reported chronic/daily myalgia and exercise intolerance; all of them reported improvement of the symptoms.
Effect on respiratory function
Ten patients were able to perform spirometry and the PEF . Patient cP5 was able to perform these tests only after 18 months of treatment due to his age and the severity of his weakness in the beginning of the treatment. At baseline, patients had a mean FVC of 40%±18% and a mean PEF of 200 ± 90 L/min. These measures improved with the therapy showing a mean increase of 15% for FVC (absolute value reaching 45%±21%) and a mean increase of 25% for PEF (absolute value going from 200 ± 87 L/min (10 patients) to 265 ± 118 L/min (9 patients) at 12 months of follow up, sustained at 18 months (Figure 2). Time on VS also decreased. At the baseline visit, seven patients required VS. Four of them reduced the total daily hours of use, while the remaining patients continued to use VS only during sleep hours. Patient aP13 was on continuous ventilation via tracheostomy. At baseline, the patient required suctioning approximately 15 times per day and used ventilator settings of pressure control (PC) of 15 and positive end-expiratory pressure (PEEP) of 9. By the twelve-month visit, the frequency of suctioning decreased to 4–5 times per day, and ventilator parameters were successfully decreased to a PC of 10 and a PEEP of 8.
At baseline, eleven patients reported recurrent infections; all of them subsequently reported a reduction in both the frequency and severity of pulmonary infection episodes.
Discussion
Here, we present motor, respiratory, and bulbar outcomes from a large cohort of patients with TK2d receiving nucleoside supplementation (dC and dT), including 9 adult patients with childhood-onset disease. Our results provide compelling evidence for the positive effects of the therapy in both children and adults. Furthermore, a detailed data on liver and pancreatic enzymes was presented and reinforced the safety profile of nucleoside supplementation in this patient group.
In infants, open-label data have previously shown that the therapy not only reduced mortality rates but also enabled the attainment or regaing of developmental motor milestones. 7 The long-term data presented here corroborate these findings. The children in our study demonstrated substantial gains in developmental milestones, strength, respiratory, and bulbar function with mild or absent side effects; all were able to reach the full target dose and none of them presented significant permanent transaminases abnormalities. Positive effects were observed early in treatment, within the first three months of therapy. They continued to show gains over time, even after 12 months.
With respect to adults, data regarding treatment efficacy and side effects in the literature are limited, especially among the ones with childhood-onset disease, such as the patients presented here. The effects of nucleosides on respiratory function were previously explored in a cohort of six adult-onset patients, suggesting stabilization of the disease. 14 Subsequently, two isolated case reports showed not only stabilization but also improvement in fatigue, motor, respiratory, and bulbar functions in one patient with adult-onset disease 15 and in one patient with childhood-onset. 16
Here, we describe data for 9 treated adults with childhood-onset disease, significantly expanding the existing evidence base. There was substantial gain in motor function, evidenced by functional evaluation scales and timed tests for those capable of completion. Regain of developmental milestones, which is rare is historical untreated controls, 8 was observed in some patients, notably the ability to walk unsupported for short distances in one patient and the ability to stand from floor in three. Beneficial effects on respiratory function were also observed with a 15% increase in FVC and a 25% increase in PEF, alongside with a reduction in the severity, in the frequency of pulmonary infections, and in the time on VS. Regarding the use of a feeding devices, no changes were noted during the follow-up period in adults, however, all of them gained substantially weight. They also reported additional features, including positive changes in speech, and reduction of myalgia, exercise intolerance, and fatigue, which warrant further investigation. Benefits of the therapy were also seen in late-stage disease, as exemplified by patient aP13. At 12 months of follow-up, improvements in respiratory parameters, as well as distal and tongue mobility, were beneficial for communication and care management.
Concerns regarding liver dysfunction following nucleoside supplementation stem from a previous report of a marked increase in transaminases in two adults, which lead to treatment suspension. 7 However, there is no reported data showing a regular assessment of these parameters in a larger group of patients as described in this current study. Data from routine measures of liver enzymes, liver function, pancreatic enzymes and CK are presented. An elevation in ALT (1.1×-2.5× ULN) and AST (1.1×-2.5× ULN) was observed in the majority of the patients (10/14), primarily in adults, most of whom also presented elevated CK levels. Pronounced (>3x ULN) but transient ALT elevations occurred in four patients (aP1, aP7, cP12 and aP13); however, serial testing demonstrated that values returned to baseline following a 25% dose reduction. GGT elevations were infrequent and typically presented as mild and isolated findings. Bilirubin levels remained normal in all patients. Although multivariate analysis indicated no correlation between CK and ALT or GGT, and dose adjustments mitigated the liver enzymes abnormalities, it remains challenging to determine whether the treatment directly impacts hepatic function or if these findings reflect purely muscle damage. Further investigation is needed for stronger conclusions.
Interestingly, a mild increase in pancreatic enzymes (lipase and amylase) was detected in four asymptomatic patients during ancillary investigation – the first such report in TK2d patients receiving nucleosides. It remains unclear, whether this finding was solely attributable to the medication, as no baseline data for these enzymes were available, but it highlights the need for further studies to evaluate potential pancreatic dysfunction.
Gastrointestinal symptoms were indeed the most common side effect reported in this cohort, and their management proved complex for most adult patients. During the initial months of therapy, 70% of them experienced diarrhea, abdominal pain, and intolerance to the high-fluid-volume required for weight-adjusted medication. While more diluted formulation reduced the intensity of diarrhea, individual adjustments were necessary due to large volumes intolerance reported by most of the patients. A progressive improvement in GI symptoms was noted over the following months for all patients, but even with individualized management, full dosing was achieved in only 50% of the adult cohort. Nevertheless, beneficial effects were observed even in those receiving suboptimal doses.
Of the four patients in the pediatric group, two (cP12 and cP5) presented with a severe and aggressive early-onset form of the disease. At the start of treatment, both were bed-bound and dependent on feeding device and ventilatory support. They were enrolled in therapy after a disease duration of 4 months and 2 years respectively. By the 12-month visit, cP12 showed more substantial gains than cP5, achieving independent gait. This data suggest that earlier treatment initiation may yield greater benefits, consistent with previous report. 7 In the adult group, although heterogeneity limits further speculation, patients with a shorter disease duration tended to present with milder symptoms and experienced more pronounced treatment gains.
The primary limitation of this study is the lack of a controlled, double-blind design, which is the gold standard for evaluating drug efficacy and adverse effects. This limitation is inherent to the study of rare and progressive diseases like TK2d, which carry high morbidity and mortality, particularly when evaluating a promising treatment that is altering the natural history of the disorder. Despite these limitations, the data presented here is novel and it was collected by a single and specialized team. It demonstrated for the first time that deoxycytidine and deoxythymidine supplementation significantly improved motor, respiratory, and bulbar outcomes in a large cohort of adult patients with childhood-onset TK2d while reinforcing the dramatic clinical benefits in the pediatric population. Furthermore, this study also supports the safety of the supplementation by providing detailed data on liver function and enzymes during the treatment, though it suggests that pancreatic function should be more carefully evaluated in future studies.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261432401 - Supplemental material for Nucleoside therapy for thymidine kinase 2 deficiency: Long-term outcomes from a Brazilian cohort
Supplemental material, sj-docx-1-jnd-10.1177_22143602261432401 for Nucleoside therapy for thymidine kinase 2 deficiency: Long-term outcomes from a Brazilian cohort by Cristiane Araujo Martins Moreno, Tatiana Ribeiro Fernandes, Clara Gontijo Camelo, Gabriel Keller, Filipe Di Pace, Gabriella Corrêa Dousseau, Alulin Tácio Quadros Santos Monteiro Fonseca, Eliene Dutra Campos, Ana Paula dos Anjos Lança, Mariana Cunha Artilheiro, André Macedo Serafim da Silva, Michelle Abdo Paiva, Andres Nascimento and Edmar Zanoteli in Journal of Neuromuscular Diseases
Footnotes
Ethics standards
The study was approved by the Ethics Committee of the São Paulo University (87649625.6.0000.0068). Written informed patients’ consent for participation in the study was obtained. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data is available upon request respecing local ethical regulation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.