
Abstract
Background:
Idiopathic inflammatory myopathies (IIM) are a group of autoimmune diseases characterized by skeletal muscle inflammation. Magnetic resonance imaging (MRI) is increasingly used in IIM diagnosis, yet standardized protocols and comprehensive datasets remain limited. This study aimed to characterize MRI findings across IIM subtypes, identify muscle involvement patterns, and assess correlations between imaging abnormalities and clinical severity.
Methods:
In this retrospective cohort study, 34 patients with IIM evaluated between 2012 and 2020 in Düsseldorf and Halle (Germany) were included: Inclusion Body Myositis (IBM, n = 9), Dermatomyositis (DM, n = 5), Polymyositis (PM, n = 6), Anti-Synthetase Syndrome (ASYS, n = 5), and Immune-mediated Necrotizing Myopathy (IMNM, n = 9). Clinical data (autoantibody status, creatine kinase [CK] levels, and muscle strength via Manual-Muscle-Testing-8 [MMT-8]) and muscle MRI findings were analysed. Muscle involvement patterns were characterized, and associations with clinical severity were evaluated using univariate linear regression.
Results:
MRI abnormalities were evident even in early disease stages (median disease duration: 7 months [IQR: 2–18]). Patterns of muscle involvement differed markedly across IIM subtypes; notably, ASYS and IBM showed minimal involvement of upper extremities. A significant correlation was found between MRI-visible pathology and MMT-8 scores (p = 0.027) as well as CK levels (p = 0.028).
Conclusion:
MRI reveals subclinical muscle involvement in early IIM and uncovers subtype-specific patterns. Given the heterogeneity of MRI findings, individualized imaging approaches are warranted. While MRI serves as a valuable adjunct in diagnosis and management of IIM, its utility depends on standardized protocols and integration with clinical and laboratory data to enable accurate interpretation and informed decision-making in clinical practice.
Keywords
Background
Idiopathic inflammatory myopathies (IIM) are a group of autoimmune conditions characterized by progressive muscle inflammation and weakness, often accompanied by varying degrees of systemic involvement. The primary subtypes of IIM include Inclusion Body Myositis (IBM), Polymyositis (PM), Dermatomyositis (DM), Anti-Synthetase Syndrome (ASYS), and Immune-Mediated Necrotizing Myopathy (IMNM).
Diagnosis traditionally relies on a combination of clinical evaluation, serological testing, and histopathological examination as diagnostic gold standard. 1 Magnetic resonance imaging (MRI) has emerged as a sensitive, non-invasive modality that can complement the diagnostic workflow.2,3 When integrated with clinical and histopathological criteria, MRI enhances the diagnostic accuracy, reduces the likelihood of false-negative muscle biopsies, and correlates with key clinical markers such as muscle strength and creatine kinase (CK) levels.4–6
Despite its advantages, a major limitation remains the lack of consensus on which anatomical regions should be targeted by MRI in the early diagnostic phase of IIM, limiting its standardized application in clinical practice. Moreover, existing literature predominantly addresses individual IIM subtypes in isolation, leaving a gap in comprehensive studies that evaluate all major subtypes within a unified framework, an essential step for translating MRI assessments into routine clinical practice.7–9
The aim of this study was to evaluate the clinical utility of muscle MRI in early disease stages of IIM. To this end, we systematically analysed muscle involvement patterns using whole-body MRIs (Wb-MRI) across the five major IIM subtypes: IBM, DM, PM, ASYS, and IMNM. Our primary aim was to identify subtype-specific imaging signatures and to investigate whether the severity of MRI-visible muscle pathology correlates with relevant clinical outcomes.
Methods
Study design and data collection
This retrospective study analysed clinical, laboratory, histological, and radiological data from 34 patients treated at the University hospitals of Düsseldorf and Halle, Germany, between 2012 and 2020. Patients were included if they had available Wb-MRIs and were diagnosed with IIM based on the European League against Rheumatism (EULAR)/American College of Rheumatology (ACR) criteria. 1 ASYS patients were included according to the 273rd ENMC workshop criteria. 10 For the antibody-negative ASYS patient, diagnosis was based on clinical/radiological phenotype consistent with ASYS. Of the nine IBM patients, four fulfilled the mandatory pathological criteria according to the 272nd ENMC workshop. 11 The remaining five patients were diagnosed in line with the ENMC classification as ‘clinically defined/probable IBM’, based on the typical age of onset, progressive clinical course, characteristic pattern of muscle weakness, and supportive MRI findings. Clinical and demographic data were retrieved from electronic medical records, and MRI data were obtained from the hospital's Picture Archiving and Communication System (PACS). All patients provided informed written consent, and data were pseudonymized and standardized for analysis. The study was approved by the local ethics committee (2016-2455_2) and was registered under the trial number: 2021-1417.
Disease duration was calculated from symptom onset to diagnosis. The EUROLINE Blot Assay (Euroimmun, Lübeck, Germany) as well as Labor Limbach (for HMG-CoA-Reductase-Receptor-Antibodies) were used to detect IIM-associated and -specific antibodies. Antibody status is summarized in Suppl. Table 1. Muscle strength was assessed by Manual-Muscle-Testing-8 (MMT-8). The assessment was performed by the treating clinician and noted in the electronic patient records. The treating clinicians were not involved in this study to avoid investigator biases. Electromyographic examinations were performed prior to MRI (at least 3 months in advance to avoid invalid interpretation) as part of diagnostic workup. Different numbers of muscles were examined per region as specified in
Image analysis
All MRI examinations were conducted at the time of diagnosis, primarily using 1.5 Tesla systems with locally standardized protocols for myositis. The MRI protocols included at least a T1-weighted turbo-spin echo ([T1 TSE] TE 10–20 ms, TR 500–650 ms) as well as a Short-Tau-Inversion-Recovery ([STIR] TE 90–100 ms, TR 4000–13000 ms) sequence. Wb-MRIs were conducted in transverse orientation and analysed by an experienced radiologist blinded to the disease group. Upper extremities were not separately assessed using dedicated upper-extremity coils.
Muscle involvement, as assessed by MRI-visible pathology, was graded semi-quantitatively by an independent radiologist. Evaluation was based on STIR and T1 W sequences in alignment with the 255th European Neuromuscular Conference (ENMC) workshop.
12
Wb-MRI scores considered oedema, vascular engorgement, fasciitis as early morphologic disease markers, while fat infiltration as chronic change was evaluated in T1 W sequences. As our study primarily aimed to characterize broad pattern recognition across IIM subtypes rather than establish single-muscle diagnostic markers, parameters were scored according to the area of IIM-related changes in relation to their overall area on a joint scale from 0 to 2 (0 = no muscle involvement, 1 ≤ 50% of the muscle involved, 2 > 50% of the muscle involved). In our cohort, fatty infiltration was predominantly mild and almost exclusively colocalized with STIR hyperintensity. Given that isolated fatty replacement represents a nonspecific end stage of various neuromuscular disorders and is influenced by substantial inter-individual variability, a unified semi-quantitative score pooling STIR and T1 abnormalities was used. To further facilitate robust and reproducible detection and differentiation of muscle involvement patterns while also scaling to the limited sample sizes of individual subgroups, muscles were aggregated into functional groups for analysis, detailed in
Statistical analysis
Statistical analysis was performed using SPSS (Version 29.0.1.0 (171)), GraphPad Prism (Version 10.1) and Excel (Microsoft Office 365, Version 2025). Data are presented as medians and interquartile range (IQR) or mean and standard deviation (SD) if data showed a Gaussian approximation, or in n (%). The number of cases analysed is indicated when a full data set was not available. Univariate linear regression was conducted to assess the relationship between clinical indicators (MMT-8, CK level) and MRI-assessed muscle involvement. Kruskal Wallis Test was conducted to assess differences of muscle involvement within each muscle group among the IIM subtypes. Statistical significance was set at p < 0.05.
Results
We analysed a cohort of 34 IIM patients with available Wb-MRIs. Out of 34 patients, 9 were diagnosed with IBM, 5 with DM, 6 with PM, 5 with ASYS, and 9 with IMNM. The median age of the cohort was 71 years (IQR: 60–80) and the overall female to male ratio was 0.89: 1. Median disease duration was 7 months (IQR: 2–18), reflecting a relatively early disease stage in most patients. A disease duration of zero denotes patients whose symptom onset and diagnosis coincided, particularly in DM, where characteristic skin findings frequently enable a prompt diagnosis. Muscle strength, as assessed by the MMT-8 showed a median value of 139 (IQR: 121–142), with comparable scores across IIM subtypes. Serum CK levels varied by diagnosis, with the highest levels observed in patients with IMNM, followed by PM. Most patients were treatment-naïve at the time of MRI (IBM (6/8), PM (5/6), DM (4/5), ASYS (3/5), IMNM (9/9)). The clinical details are provided in
Patient characteristics (n = 34).
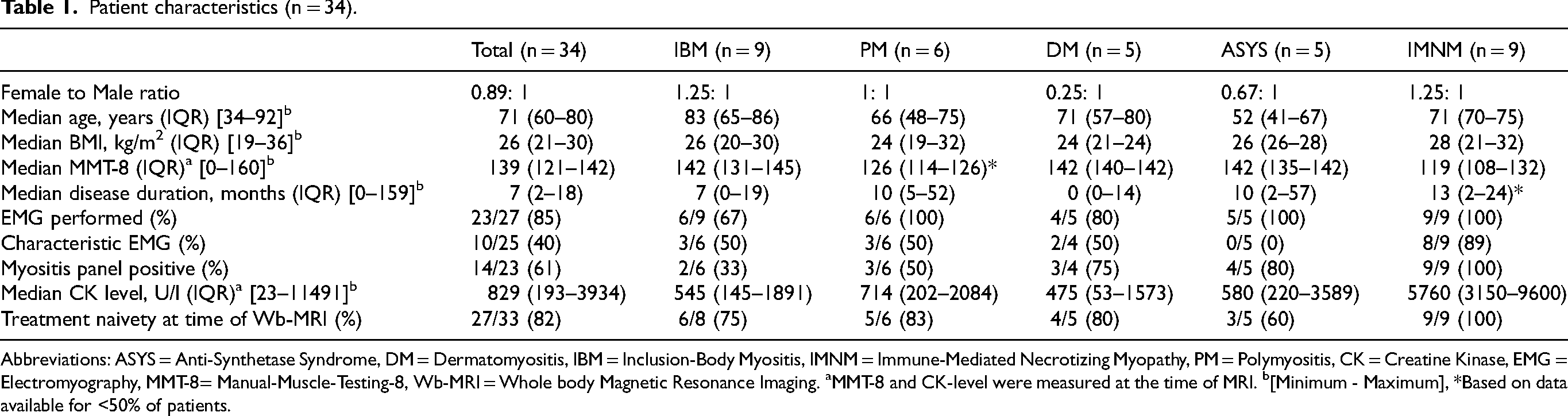
Abbreviations: ASYS = Anti-Synthetase Syndrome, DM = Dermatomyositis, IBM = Inclusion-Body Myositis, IMNM = Immune-Mediated Necrotizing Myopathy, PM = Polymyositis, CK = Creatine Kinase, EMG = Electromyography, MMT-8= Manual-Muscle-Testing-8, Wb-MRI = Whole body Magnetic Resonance Imaging. aMMT-8 and CK-level were measured at the time of MRI. b[Minimum - Maximum], *Based on data available for <50% of patients.
Muscle involvement patterns and MRI findings by IIM subtype
We observed distinct MRI phenotypes across IIM subtypes, each characterized by specific distributions of acute muscle affection, including preferential involvement of proximal or distal muscles and selective sparing or involvement of specific muscles (Figure 1). Figure 2 depicts representative examples of muscle involvement patterns of the thighs for each IIM subgroup.
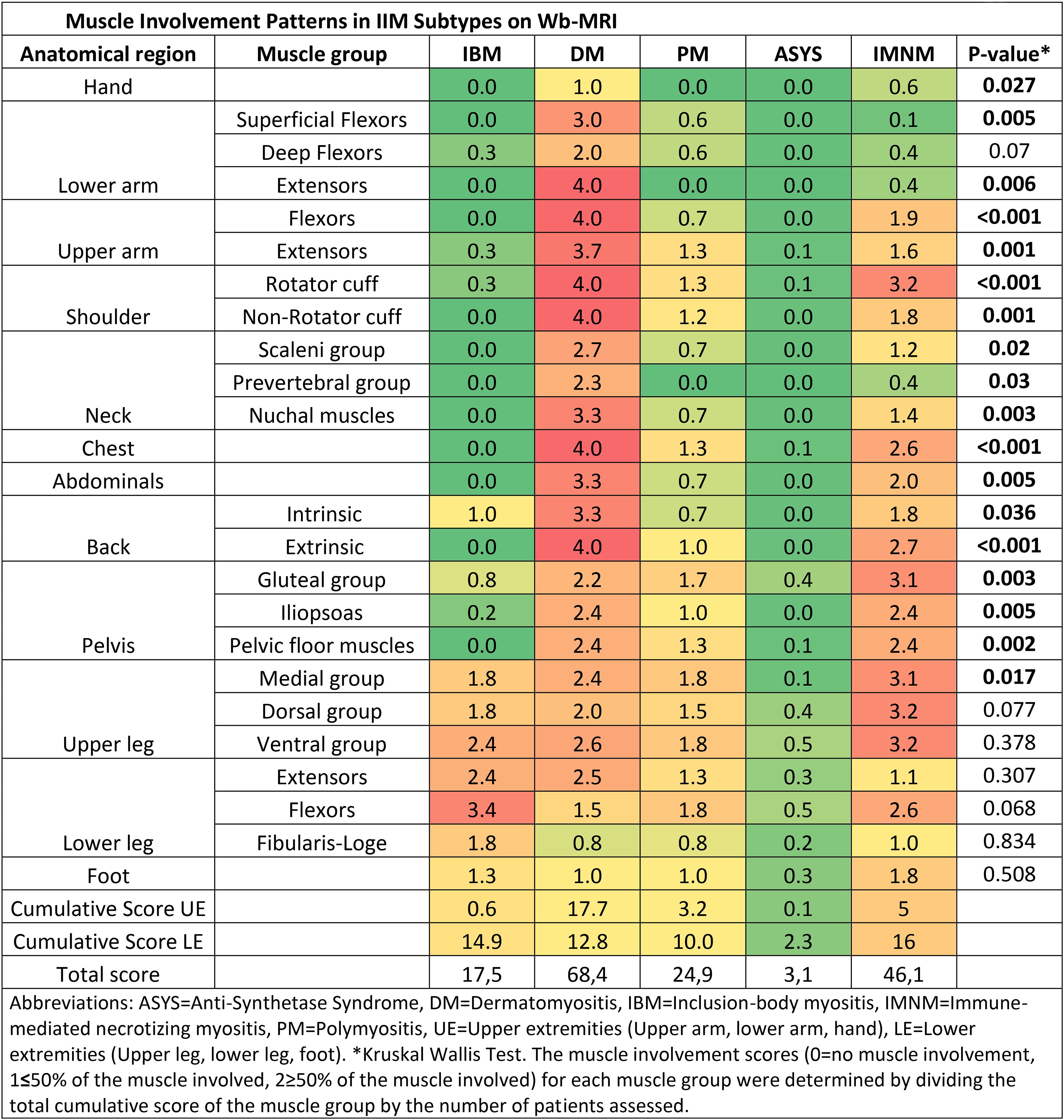
Muscle involvement patterns in IIM subtypes on Wb-MRI.
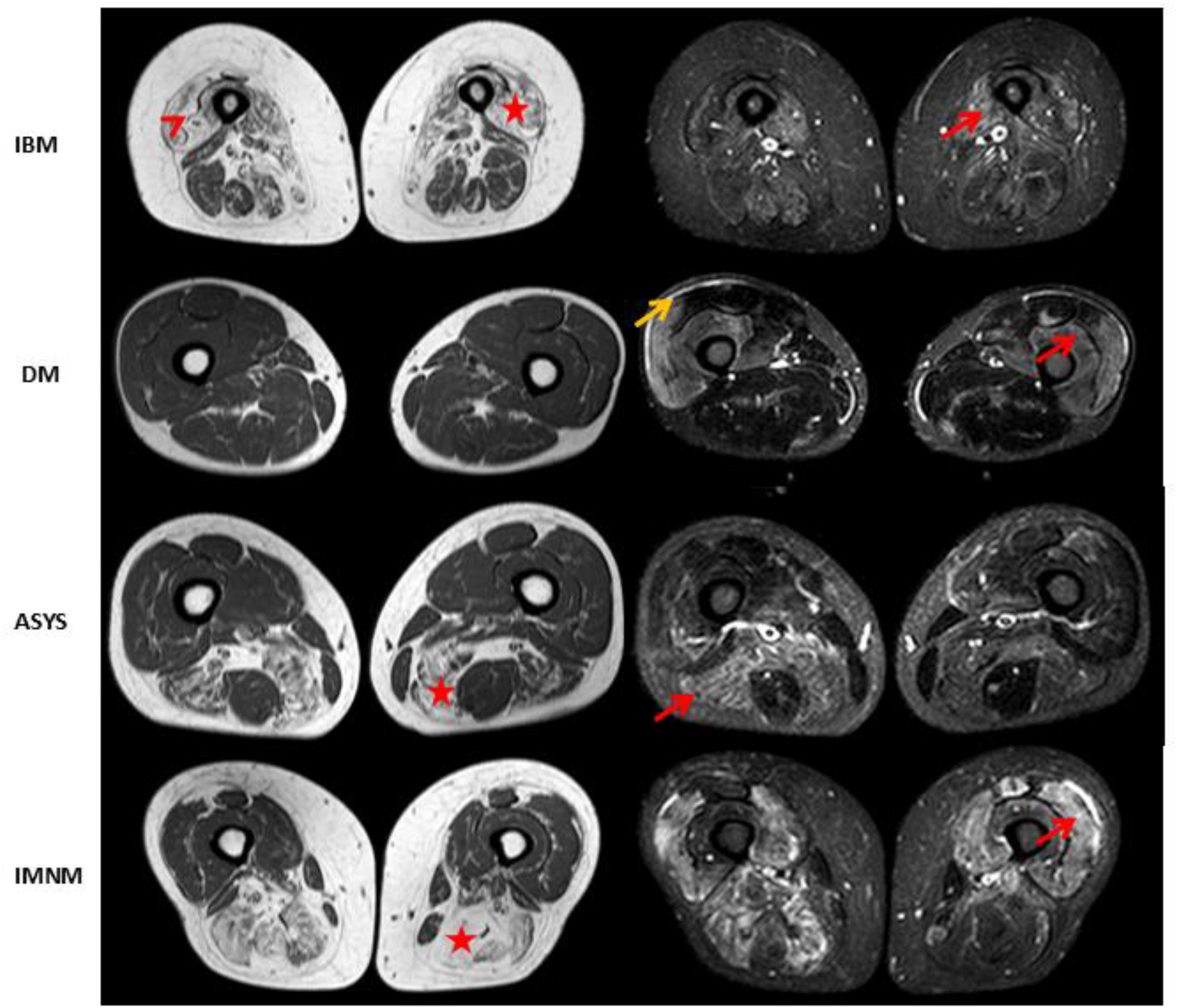
Examples of T1-weighted (T1 W) turbo spin echo (TSE) and short-tau inversion recovery (STIR) sequences showing muscle oedema (red arrow), fascial oedema (yellow arrow), fatty atrophy (red star) and the undulating fascia sign (red arrowhead) in patients with Inclusion-Body Myositis (IBM), Dermatomyositis (DM), Anti-Synthetase Syndrome (ASYS) and Immune-Mediated Necrotizing Myopathy (IMNM).
Inclusion body myositis
Wb-MRI in IBM patients revealed pronounced asymmetrical fatty atrophy predominantly affecting the lower extremities. The distal lower leg flexors were most severely involved, followed by lower leg extensors and ventral thigh muscles. The medial gastrocnemius and anterior thigh showed maximal atrophy, alongside marked changes in the intrinsic back muscles. Oedema was minimal or absent. Notably the upper extremities, including the flexor digitorum profundus, showed no substantial involvement, which diverges from typical muscle involvement patterns in IBM.
Dermatomyositis
DM patients displayed severe, symmetric muscle oedema with predominant involvement of proximal muscles in both upper and lower limbs. The most affected areas included the lower arm extensors, upper arm flexors, shoulder girdle (non-rotator cuff), chest wall muscles, and extrinsic back muscles. Significant oedema was also observed in the medial and ventral groups of the thigh while the dorsal group was relatively spared. Extensive oedema was observed in nearly all affected muscle groups, while fatty infiltration and atrophy were minimal, suggesting a primarily inflammation-dominant phenotype in DM patients.
Polymyositis
PM exhibited primarily proximal, symmetric involvement, predominantly affecting the lower limbs more than the upper limbs. The medial and ventral thigh, gluteal muscles and lower leg flexors exhibited the highest MRI scores. While less severe than DM, PM was characterized by a heterogenous pattern of involvement of upper arm, gluteal and thigh muscles. Oedema was infrequently detected, and in several patients, muscle architecture remained largely preserved, suggesting variable disease activity or chronicity.
Anti-synthetase syndrome
In ASYS, a predominantly distal and symmetric pattern was observed, primarily affecting the lower leg flexors, the ventral and dorsal thigh, and gluteal muscles. The most affected regions were the medial gastrocnemius, soleus, flexor digitorum longus, and quadriceps femoris. Fatty atrophy was prominent, while muscle oedema was minimal. ASYS exhibited the mildest overall muscle involvement among all subtypes, potentially reflecting shorter disease duration or a less aggressive muscle phenotype.
Immune-mediated necrotizing myopathy
IMNM patients demonstrated extensive, symmetric involvement of proximal muscle groups, particularly the gluteal region, thigh and rotator cuff muscles. The medial and ventral thigh muscles exhibited pronounced oedema, while the dorsal group was characterized by marked fatty atrophy. Notably, MRI revealed the coexistence of pronounced muscle oedema and fatty infiltration within the same individuals, suggesting concurrent, muscle-dependent inflammatory and degenerative changes indicative of different disease stages.
Total muscle involvement scores were highest in DM (68.4), followed by IMNM (46.1), PM (24.9), IBM (17.5), and lastly ASYS (3.1). Notably, in all subtypes except DM, Wb-MRI revealed greater cumulative muscle involvement of the lower extremities compared to the upper extremities. The Kruskal–Wallis test revealed significant differences in muscle involvement across IIM subgroups for most muscle groups. Unexpectedly, within the lower extremities, significant differences were detected only in the medial thigh group, while no differences were observed in the remaining lower extremity muscle groups.
Relationship between MRI severity and clinical severity
To investigate whether the extent of muscle involvement on Wb-MRI reflects clinical severity, univariate linear regression analyses were performed comparing MRI severity scores with MMT-8 scores and serum CK levels.
In the overall cohort, a significant negative correlation was observed between MRI severity scores and MMT-8 scores (R2=0.202, p = 0.027), and a significant positive correlation was found between MRI severity scores and CK levels (R2=0.166, p = 0.028) (Figure 3(a) and 3(b)). To explore potential subtype-specific associations, separate analyses were conducted for the IBM and IMNM subgroups, which were the only subgroups with sufficient sample sizes for statistical analysis. Both in the IBM and IMNM subgroups, no significant correlations were observed between MRI severity and MMT-8 scores (IBM: R2=0.017, p = 0.73, IMNM: R2=0.129, p = 0.42) or between MRI severity and CK levels (IBM: R2=0.183, p = 0.39, IMNM: R2=0.04, p = 0.60).
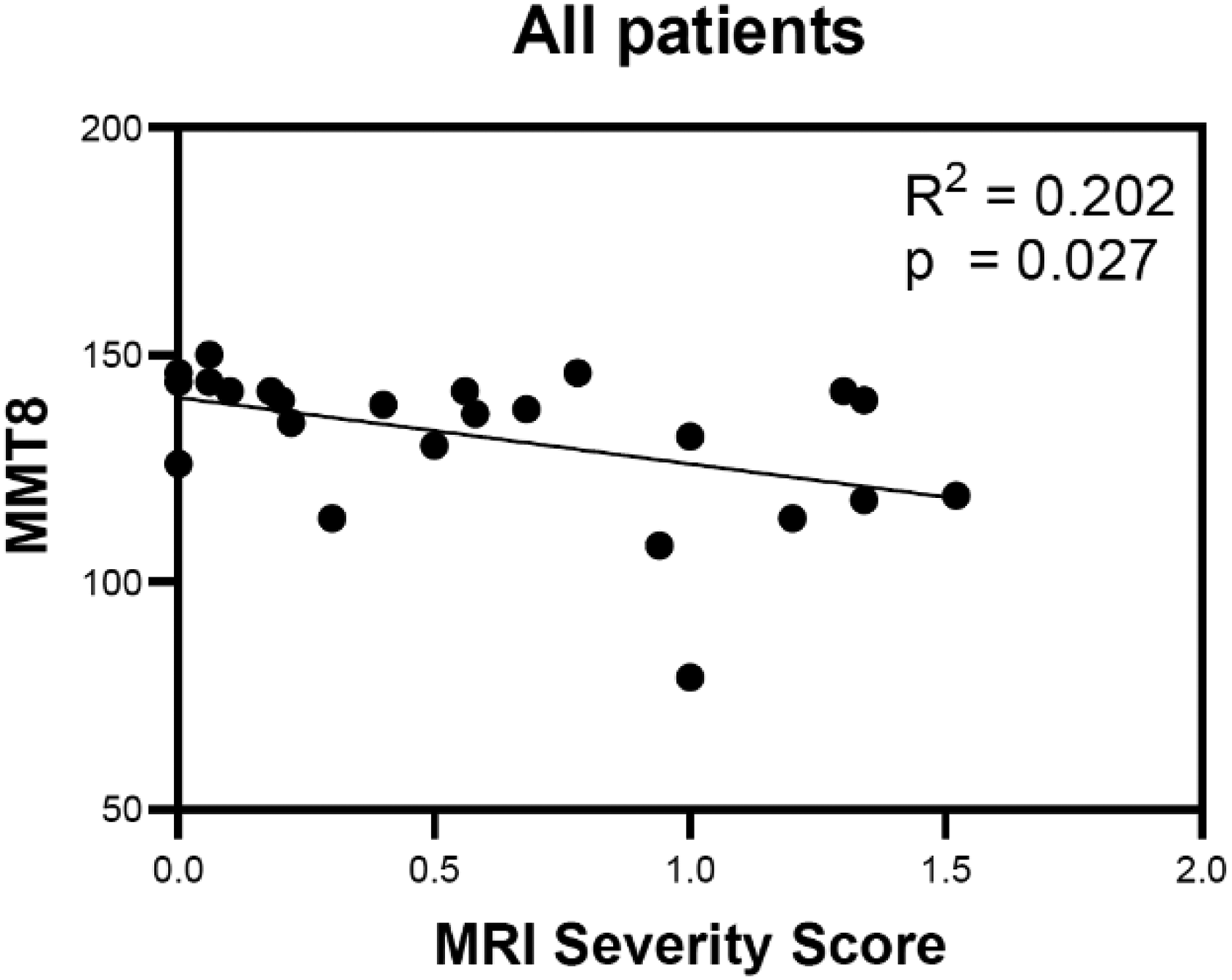
MRI severity score and MMT-8.
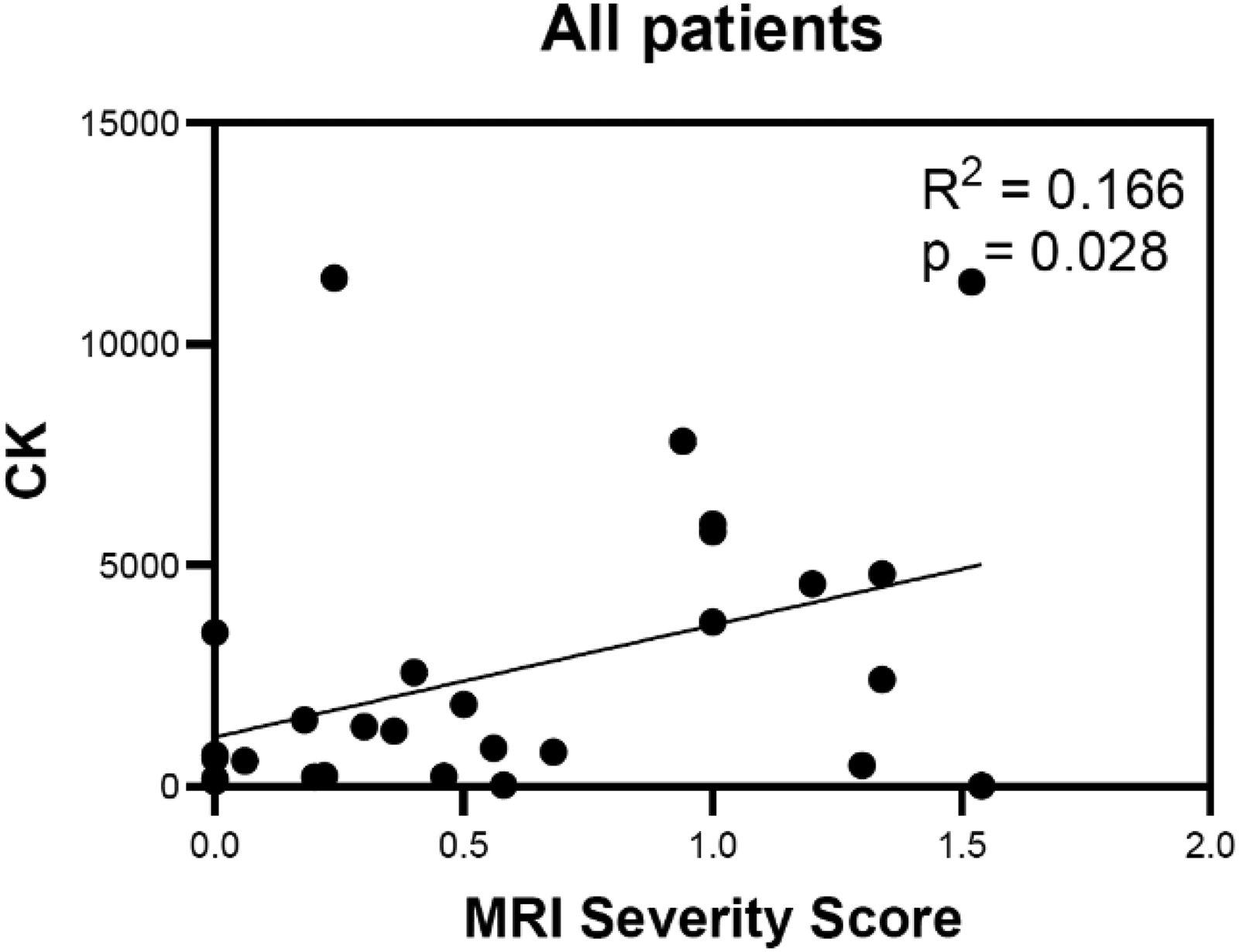
MRI severity score and CK level.
Discussion
In this study, we employed Wb-MRI to characterize early signs of muscle involvement across the major IIM subtypes; IBM, DM, PM, ASYS, and IMNM. Using a simple semi-quantitative scoring system, we were able to capture the extent and distribution of MRI-visible muscle pathology. Even in a cohort with relatively short disease duration (median disease duration of 7 months [IQR: 2–18]), Wb-MRI revealed subtype-specific patterns of muscle pathology across IIM subtypes. In all subtypes except DM, Wb-MRI revealed greater cumulative muscle involvement of the lower extremities compared to the upper extremities. Additionally, significant correlations were identified between MRI severity scores and clinical measures, including MMT-8 and CK levels, in the overall cohort, whereas no significant associations were observed within individual subgroups. Our findings highlight the sensitivity of Wb-MRI to detect early muscle involvement and its potential to differentiate between IIM subtypes. 16 In DM, PM and IMNM, the observed patterns of muscle involvement were consistent with previous reports, reinforcing the diagnostic value of MRI in phenotyping these subtypes.6,8,17–19 In contrast, IBM and ASYS patients showed less upper extremity involvement than expected, particularly of the deep forearm flexors, diverging from earlier reports.9,20–23
For ASYS, the limited upper extremity involvement may reflect a milder phenotype or variability related to antibody status, disease duration, and treatment status. 24 Although most ASYS patients (3/5) were treatment-naive, some received immunosuppressive therapy at the time of MRI which may have attenuated visible pathology. Additionally, the small sample size may have restricted the ability to detect subtle upper extremity involvement. One ASYS patient was seronegative but included based on characteristic clinical presentation and the known occurrence of seronegative cases due to assay limitations or undetected autoantibodies.25,26 Despite most patients with IIM typically being treated promptly, the predominance of treatment-naïve patients at the time of MRI in our cohort likely reflects real-world clinical pathways, including delayed referral, diagnostic uncertainty, or initial assessment at external institutions.
In IBM, the absence of deep forearm flexor involvement contrasts with established clinical patterns.27,28 This may be attributed to early disease stage, small muscle size, or limited MRI resolution, emphasising the need for standardized, subtype-specific imaging protocols. 29 Alternatively, disease progression may not yet have reached these regions in our IBM cohort.
Interestingly, no significant differences in muscle involvement were observed in the lower extremities, except for the medial group of the thigh, despite these being the muscle regions most consistently and severely affected across all subtypes. This likely reflects a ceiling effect, as high overall disease burden reduces intergroup variability. Moreover, subtype-specific patterns appear to involve distinct muscles within these regions rather than the overall extent of involvement, which may not be fully captured by the semi-quantitative group scoring approach.13,30
Although significant correlations between MRI severity scores and clinical measures such as MMT-8 and CK levels were evident in the overall cohort, these associations did not reach statistical significance in the IBM and IMNM subgroup analyses, likely reflecting insufficient statistical power due to the small sample sizes. This observation is consistent with previous studies reporting associations between MRI findings and functional assessments, including MMT-8 and Myositis Disease Activity Assessment Tool (MDAAT).18,27 Together, these results support the notion that MRI-derived measures capture clinically meaningful aspects of disease activity, even when traditional biochemical or functional parameters show limited sensitivity. 31 The lack of significant correlations within subgroups further highlights the need for larger, adequately powered studies to confirm these relationships and to explore disease-specific patterns. In IBM in particular, CK levels are frequently within the normal range, limiting their usefulness as indicators of disease activity or progression, which underscores the potential value of MRI as a complementary biomarker in this context.
Collectively our findings highlight the importance of interpreting MRI results within the clinical and serological context of the suspected IIM subtype. Wb-MRI provides valuable insights into early muscle pathology, but a multimodal approach remains essential for comprehensive disease evaluation as MRI may complement but not replace antibody or biopsy-based classification. Given that cumulative MRI scores were consistently higher in the lower extremities across all subgroups except DM, focusing MRI assessments on the thighs may offer a pragmatic, cost-effective strategy for diagnostic purposes, particularly relevant given the limited accessibility and high resource demands of Wb-MRI in routine practice. Although MRI-based classification supported clear differentiation between most IIM subtypes, PM cases lacked a distinct imaging pattern, consistent with the evolving understanding and reclassification of this heterogenous group. 32
Limitations
This study has several limitations. The small sample sizes reduce statistical power and limit the generalizability of the findings. The absence of a matched control group precludes definitive differentiation between disease-specific and nonspecific MRI findings. In addition, some patients were not treatment-naïve at the time of MRI, which may have resulted in an underestimation of disease activity. In IBM patients without biopsy confirmation, no genetic testing was performed to exclude Myofibrillar Myopathy and Facioscapulohumeral Muscular Dystrophy. Additionally, the retrospective design precluded longitudinal imaging, which is particularly relevant in slowly progressive entities such as IBM. Moreover, our group based semi-quantitative scoring approach facilitates feasibility and reproducibility but may obscure subtle, muscle-specific differences. The use of a unified semi-quantitative score combining STIR and T1-weighted abnormalities limits differentiation between active inflammation and chronic structural change; however, as fatty infiltration was predominantly mild and largely colocalized with STIR signal alterations in this early-stage cohort, this approach was considered sufficient for capturing overall disease burden and enabling robust pattern recognition. The absence of dedicated imaging of the upper extremities using specific upper-extremity coils may have resulted in an underestimation of involvement in this region, particularly for IBM and ASYS patients. Moreover, averaging left and right sided scores limited the ability to assess asymmetry as a separate metric, which could have been especially relevant in IBM. Finally, MRI evaluation was performed by a single radiologist, and intra-observer variability was not assessed.
Future directions and conclusions
Future research should focus on larger, multicentre cohorts to validate these findings and explore MRI-based phenotyping in early disease stages. In addition, MRI analysis should aim to differentiate between distinct stages of muscle involvement, such as oedema, fatty infiltration, and atrophy, to provide more nuanced insights into disease progression and subtype-specific pathology. Integrating MRI with clinical, serological, and histopathological data using machine learning approaches could further improve diagnostic precision and enable personalized treatment strategies. 14 Ultimately, the development of standardized, phenotype-specific MRI protocols will be critical to ensure consistent, comparable assessments across studies and clinical settings, advancing care for patients with IIM. 33
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261425506 - Supplemental material for Semi-quantitative analyses of muscle magnetic resonance imaging for pattern recognition in early idiopathic inflammatory myopathies
Supplemental material, sj-docx-1-jnd-10.1177_22143602261425506 for Semi-quantitative analyses of muscle magnetic resonance imaging for pattern recognition in early idiopathic inflammatory myopathies by Yana Leven, Suam Kim, Antoine Sanner, Fatma Merzou, Sergio Groppa, Christopher Nelke, Ahmed Othman, Andreas Deistung, Benjamin Troppa, Alexander Mensch, Sven G Meuth, Tobias Ruck and Marc Pawlitzki in Journal of Neuromuscular Diseases
Footnotes
Abbreviations
Acknowledgements
None.
ORCID iDs
Ethical considerations and consent to participate
The study received ethical approval by the local ethics committee (2016-2455_2) and was registered under the trial number: 2021-1417. All patients provided informed written consent.
Consent for publication
Not applicable
Authors’ contributions
All authors conceived the study and developed the study design. MP, TR and CN were mainly responsible for data acquisition and patient recruitment. AO, SK and AS pre-processed and analysed MRI data and provided technical support throughout the project. AM, AD and BT provided additional MRI data and assisted with data analysis. YL analysed and interpreted the clinical data as well as semi-quantitative MRI data and drafted the manuscript. MP, TR and CN supervised and revised the manuscript. All authors read and approved of the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are included in the supplementary materials. Additional data are available from the corresponding author upon reasonable request, subject to ethical and legal restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.