
Abstract
Background:
Adeno-associated virus (AAV)-mediated gene therapy with delandistrogene moxeparvovec-rokl (Elevidys®) is an approved treatment for patients with Duchenne muscular dystrophy (DMD). While generally well tolerated, hepatotoxicity has been observed following its administration, leading to liver failure and death in two reported cases to date.
Methods:
This is a case series describing four male patients with DMD, who received delandistrogene moxeparvovec-rokl at a single academic medical center and developed acute liver inflammation. All patients received corticosteroids, with doses increased as abnormalities developed, followed by the addtion of oral sirolimus (goal trough: 3–7 ng/ml), which was used primarily for T-cell immunomodulation. Monitoring included close clinical follow up, serial laboratory testing, and cardiac and functional assessments per institutional protocol.
Results:
The patients were between 5 and 16 years of age with a weight between 20.8 and 56.7 kg, (median: 32.5 kg). Three boys were ambulatory. The four patients were receiving chronic corticosteroids for the treatment of DMD prior to delandistrogene moxeparvovec-rokl administration. All cases developed hepatic enzyme elevations five to seven weeks post-gene therapy. Treatment with high-dose corticosteroids led to transient improvement or worsening of laboratory abnormalities, and initiation of adjunctive sirolimus therapy resulted in normalization of gamma-glutamyl transferase and improvement of transaminases within two to four weeks. The duration of sirolimus treatment ranged from four to twelve weeks, during which corticosteroids were successfully weaned. None of the patients experienced hepatic synthetic dysfunction or serious infections.
Conclusions:
These cases illustrate a subacute pattern of liver inflammation following AAV-gene therapy and support the potential role of mTOR inhibitors in managing AAV-related hepatotoxicity.
Introduction
Duchenne muscular dystrophy (DMD) is a progressive X-linked neuromuscular disorder caused by loss-of-function mutations in the DMD gene, leading to absence of dystrophin, which in turn results in muscle degeneration, loss of ambulation, cardiomyopathy, and respiratory failure. 1 Adeno-associated virus (AAV)-based gene therapy has emerged as a meaningful approach to address the underlying genetic defect of patients with DMD and many other conditions. 2 Despite the therapeutic potential of AAV-based gene therapy, several adverse events related to immune responses have been reported to date including thrombotic microangiopathy, acquired hemophagocytic lymphohistiocytosis and hepatotoxicity that ranges from mild elevation of transaminases to fulminant liver failure and death.2–7
Delandistrogene moxeparvovec-rokl (Elevidys®, SRP-9001) received accelerated approval by the U.S. Food and Drug Administration (FDA) in 2023 as the first commercially available micro-dystrophin gene therapy for the treatment of patients with DMD aged 4 and 5 years, with exceptions based on specific mutations and anti-AAVrh74 antibody status. 8 In 2024, the FDA expanded its approval granting full approval for ambulatory individuals aged 4 and older, and accelerated approval for non-ambulatory individuals, with the non-ambulatory indication contingent on confirmatory trials. 9 As of May of 2025, the approval has been restricted to patients aged 4 and older who remain ambulatory. The revised prescriber information was established after the death of two patients due to liver failure. Ongoing studies will continue to assess safety and effectiveness in non-ambulatory individuals. 10 Delandistrogene moxeparvovec-rokl is comprised of an AAVrh74 capsid and microdystrophin controlled by the MHCK7 promoter. 11 The product has demonstrated encouraging results in preclinical and clinical studies.11,12 Despite observed benefits, delandistrogene moxeparvovec-rokl has been associated with a range of complications, including hepatic adverse events.2,4,13 Clinical trials and post-marketing surveillance have reported elevations in alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transferase (GGT), synthetic function abnormalities, and cases of acute fulminant liver failure unresponsive to additional corticosteroids.4,14
Previous clinical and pre-clinical studies reported findings that appear to be primarily driven by a T-cell mediated response, such as what was described in cases with liver injury associated with onasemnogene-abeparvovec-xioi for patients with spinal muscular atrophy.15,16 Histopathology in these cases was characterized by inflammatory infiltrates composed of CD3+ and CD8+ T cells, and even fibrosis.16,17 Evidence of early acute hepatocellular injury within the first three to ten days after vector administration was seen in cynomolgus and rhesus monkeys. 18 Hordeaux et al. suggest that direct acute tissue damage by the capsid results in secondary complement activation, accompanied by microvascular injury and platelet sequestration in the liver sinusoids. 18 Sirolimus, also known as rapamycin, is a well-recognized oral immunosuppressant that acts as a T cell modulator through the inhibition of the mammalian target of rapamycin complex 1 (mTORC1), with additional B cell immunomodulatory effects.19–23 Further, sirolimus is increasingly being used in the AAV gene therapy field with promising results and an acceptable safety profile.3,23–25
Here, we present a case series of four male patients with DMD who developed acute liver abnormalities following delandistrogene moxeparvovec-rokl infusion. Initially, all patients received additional higher doses of corticosteroids; however, due to only transient improvement or worsening liver enzyme abnormalities, sirolimus was introduced, resulting in rapid laboratory improvements in all cases. In this context, we have extrapolated the definition of steroid-refractory hepatitis from the literature regarding autoimmune hepatitis, which defines it as an episode that does not respond to the use of corticosteroids as first-line therapy.26–28
We characterize these findings within the emerging landscape of AAV gene therapy-associated hepatotoxicity and propose sirolimus as a viable adjunctive treatment in steroid-refractory cases or as an agent that can prevent or reduce the severity of liver toxicity in patients receiving this or similar products, especially with the prospect of increased expression. 23 , 29
Methods
This case series includes four male patients with genetically confirmed DMD who received intravenous delandistrogene moxeparvovec-rokl (1.33 × 1014 vg/kg) at the University of Florida Center for Advanced Therapeutics between August 2024 and April 2025.
Baseline assessments included genetic testing, functional evaluations, echocardiography, and laboratory screening of hepatic enzymes (aspartate aminotransferase [AST], alanine aminotransferase [ALT], gamma-glutamyl transferase [GGT], hepatic function (prothrombin time, International normalized ratio [INR], fibrinogen, albumin, bilirubin), creatine kinase (CK), inflammatory markers, and anti-AAVrh74 antibodies. Ambulatory status was defined as the ability to walk at least 10 meters without assistance.
Patients received their routine corticosteroid regimen (prednisone or deflazacort) and additional prednisone or prednisolone according to the delandistrogene moxeparvovec-rokl prescribing information in the package insert. Infusions were administered per institutional protocol and tolerated without complications. Post-infusion follow-up included serial laboratory tests, including complete blood count, AST, ALT, GGT, liver synthetic function, renal and cardiac function, inflammatory markers, along with frequent clinical assessments per the University of Florida gene therapy protocol and consensus guidelines. 30 In the event of liver test abnormalities, transaminases and synthetic function was checked weekly or every two weeks until resolution of laboratory abnormalities. Sirolimus was started after either worsening, lack of improvement or rebound of laboratory values after a course of higher doses of corticosteroids, aiming to maintain a trough level goal between 3 and 7 ng/mL and dosage was adjusted accordingly based on the nearest available tablet formulation.22,24,31 Data were extracted from the electronic health record. This study was approved by the University of Florida Institutional Review Board (IRB201600103 and IRB201900677).
Results
Baseline patient characteristics
This cohort includes four non-Hispanic white male patients between the ages of 5 and 16 years at the time of dosing. Patients’ weights ranged between 20.8 kg and 56.7 kg, with a median of 32.5 kg. Three of the four patients were ambulatory at the time of infusion. All patients were on corticosteroids at baseline and one of them (patient 1) was receiving weekly eteplirsen infusions prior to gene therapy. Patient 2 received givinostat prior to gene therapy administration, which was discontinued eight weeks prior to the infusion. None of the patients had any preceding history of liver disease. Details of each patient, along with baseline function and medications are provided in Table 1.
Patient characteristics and initial immunosuppression regimen.
# all non-Hispanic.
+At dosing.
BMI: Body mass index; vg: vector genomes.
**Due to an error during the conversion from deflazacort to prednisone, the patient inadvertently received a lower total corticosteroid dose. The total recommended dose should have been 60 mg of prednisone.
Clinical course and management
Patient 1
Patient 1 is a five year-old, 20.8 Kg, ambulatory male with DMD due to a deletion in exons 45–50. He was taking daily prednisone and had previously received weekly eteplirsen infusions, which were discontinued one month prior to delandistrogene moxeparvovec-rokl administration. His daily dose of prednisone increased to a total dose of 36 mg per day. The infusion was well tolerated. Beginning on day 38 after dosing, the patient developed progressive increase in ALT and AST, not attributable to muscle injury (as CK remained stable), as well as a 10-fold increase in GGT from baseline. On day 45 (week 6) after dosing, he received additional prednisolone at a dose of 1 mg/kg for nine days (2.75 mg/kg, equivalent to 57 mg of prednisone) without significant improvement, (day 45–53), in addition to intravenous methylprednisolone 2 mg/kg on days 49, 51, and 10 mg/kg on day 52). He was hospitalized on day 54 after gene therapy for further work up and initiation of sirolimus. At the time, the patient was asymptomatic, and did not report a recent history of acute infection. Liver ultrasound was unremarkable, including normal portal venous flow.
Infectious work up for etiologies including Hepatitis A, B, C, Cytomegalovirus (CMV), Epstein Barr Virus (EBV), common bacterial, viral and parasitic causes of gastroenteritis was negative.
After initiation of sirolimus at a loading dose of 3 mg/m2 (2.4 mg) on day 56 post infusion (week 8), followed by a daily dose of 1 mg/m2 (0.8 mg), he achieved stabilization of ALT, AST within 3 days and consistent improvement of GGT in the same period. Patient remained on 2 mg/kg/d of methylprednisolone during hospitalization due to behavioral challenges with administration of oral medications. He was discharged on day 59 after gene therapy on 0.8 mg of sirolimus (1 mg/m2) and 2 mg/kg of prednisolone (total dose: 42 mg). One week after initiation of sirolimus, all laboratory values had improved. Sirolimus trough remained between 4 and 5 ng/mL once on a stable dose. Corticosteroids were tapered over six weeks to his baseline dose, and sirolimus was discontinued twelve weeks after initiation, on day 155 after gene therapy infusion. Synthetic function was normal throughout. Laboratory testing remained stable afterwards.
He exhibited increased irritability and hyperactivity during higher doses of corticosteroid treatment, which improved after the wean. He did not experience any side effects from the addition of sirolimus.
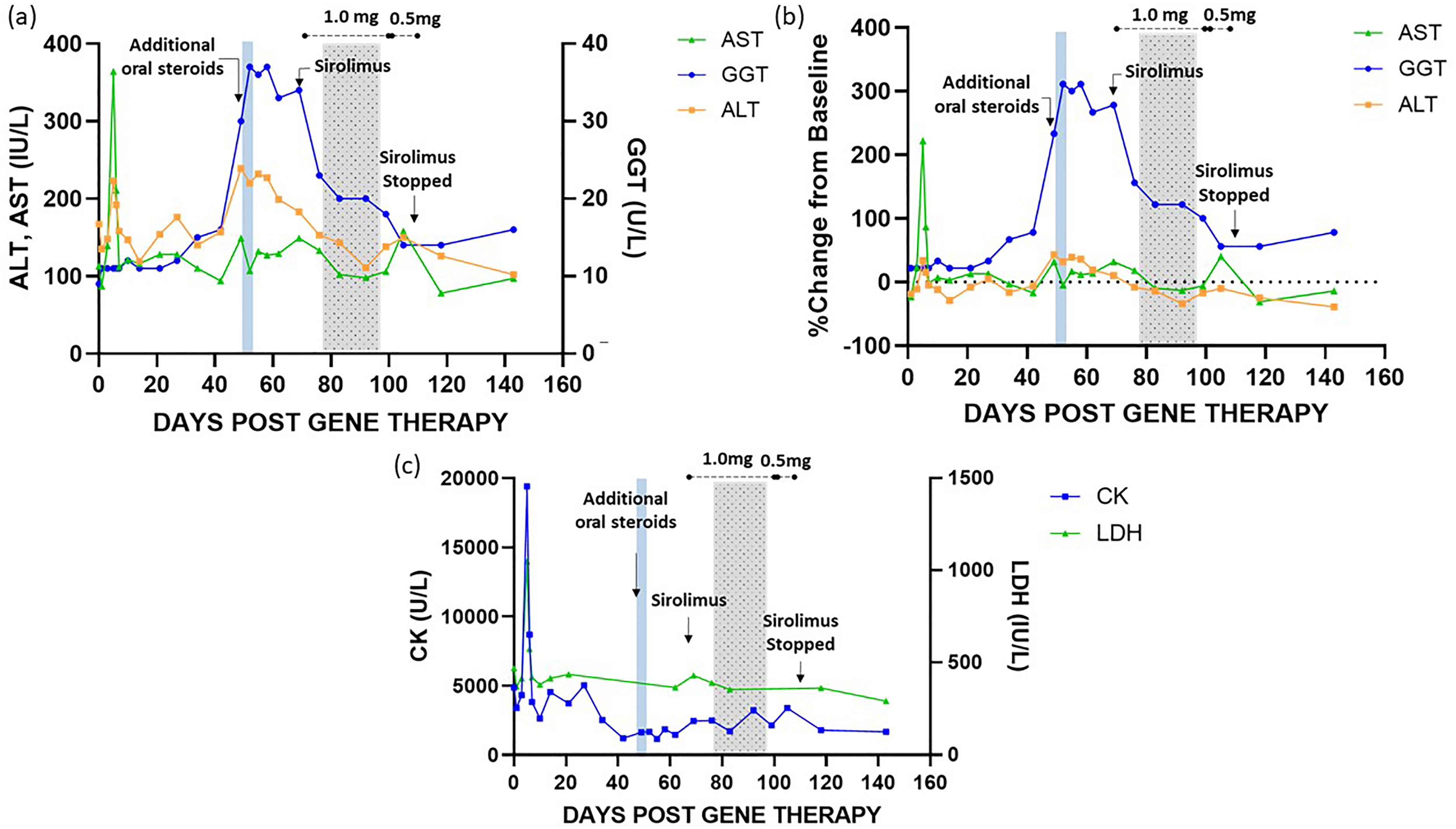
Laboratory changes and interventions are shown in Figure 1.
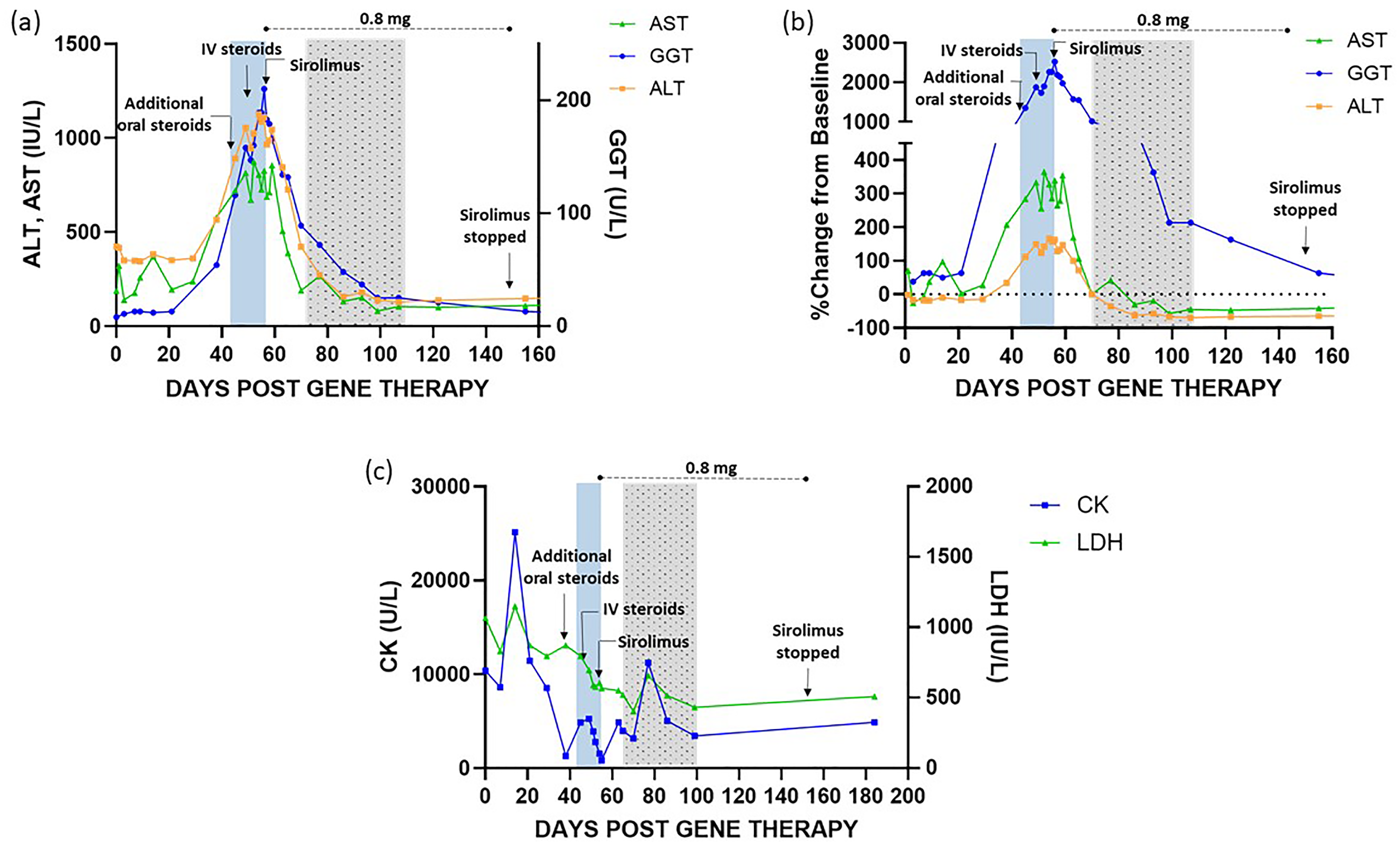
Laboratory changes and interventions for patient 1. The patient is a 5-year-old with deletion of Exons 45–50 in the Dystrophin gene. Progressive increase of ALT, AST, GGT prompted addition of prednisolone (1 mg/kg) for 9 days (day 45–53), in addition to intravenous methylprednisolone 2mg/kg on days 49, 51, and 10 mg/kg on day 52, and continued during hospitalization (Day 54–59) at a total daily dose of 2 mg/kg/d. Sirolimus was initiated on day 56 post-infusion (week 8) at a dose of 3 mg/m2 (2.4 mg), followed by 0.8 mg daily (1 mg/m2). ALT, AST and GGT improved within a week. Additional corticosteroids were tapered between days 73 and 107 post-infusion. Sirolimus trough remained between 4 and 5 ng/mL once on a stable dose. Sirolimus was stopped after a total of 12 weeks. Trough remained between 4 and 5 ng/mL. 1a. Changes over time of ALT, AST, GGT. 1b. Change from baseline (%) of ALT, AST, GGT. 1c. Changes of CK and LDH during interventions. ALT: alanine aminotransferase; AST: aspartate aminotransferase; CK: Creatine Kinase; LDH: Lactate dehydrogenase; GGT: gamma-glutamyl transferase. Daily sirolimus dose above dotted line. Blue area shows period of increased steroids, gray (dotted) area shows steroid taper.
Patient 2
Patient 2 is a thirteen year-old, ambulatory male with DMD due to a duplication of exon 17, who was receiving daily deflazacort at a dose of 0.8 mg/kg/d and givinostat. Givinostat was discontinued eight weeks before delandistrogene moxeparvovec-rokl administration. His total corticosteroid dose was increased to 40 mg of prednisone equivalent prior to gene therapy administration. The infusion was uneventful. On day 37 (week 5), the patient demonstrated a two-fold increase in ALT, AST and GGT from baseline, although GGT values remained below the upper limit of normal (ULN) (8 U/L to 16 U/L, ULN: 32U/L). He received additional oral prednisone at a dose of 1 mg/kg for six days with temporary stabilization of laboratory markers; however, a rebound was noted on day 56 (week 8), with ALT and GGT increasing to three times baseline and AST increasing two-fold from baseline. Viral studies were negative for acute infections. He did not undergo abdominal imaging. Liver biomarkers worsened slightly after initiation of an already delayed steroid taper, prompting initiation of sirolimus on day 67 at a loading dose 3 mg/m2 (2.67 mg) and a daily dose of 1 mg/m2 (0.9 mg, rounded to 2.5 mg and 1 mg doses respectively, using tablets). The dose of sirolimus was reduced to 0.5 mg tablets daily due to high trough levels (8.6 ng/ml) three days after starting the medication, as the goal was 3–7 ng/ml. However, the trough continued to be slightly higher than desired (7.4 ng/ml 8 days after initiation) but the dose of 0.5 mg tablets was continued as liquid formulation was not available. Sirolimus trough continued to be slightly above the goal and between 7.4 and 10.5 ng/ml). ALT and AST returned to baseline within two weeks, and GGT declined within three weeks of sirolimus initiation, allowing completion of his steroid taper by day 77. Sirolimus was discontinued on day 97 (week 13). Synthetic function was monitored before and after hepatic inflammation and it remained normal.
The patient developed a very mild acneiform facial rash during the final week of sirolimus treatment, which resolved after discontinuation of the medication. Figure 2 includes laboratory changes and interventions for patient 2.
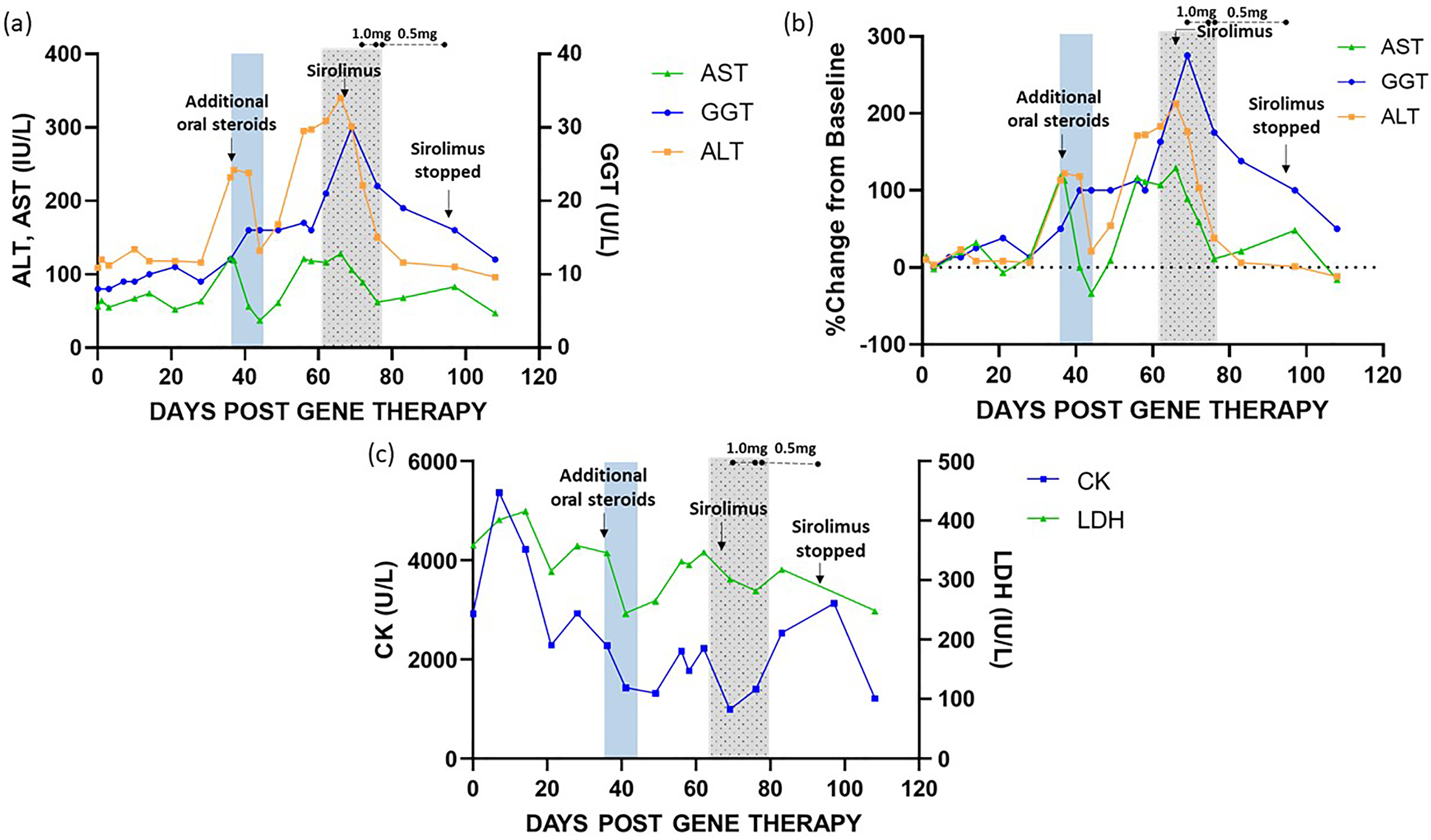
Laboratory changes and interventions for patient 2. The patient is a 13-year-old with duplication of exon 17 in the Dystrophin gene. A two-fold increase in ALT, AST and GGT from baseline around day 37 (week 5) prompted addition of prednisone (1 mg/kg) for six days with improvement of laboratory results. On day 56 (week 8), ALT, AST and GGT progressively worsened after attempting to wean corticosteroids. Sirolimus was initiated on day 66 (loading dose: 3 mg/m2; daily dose: 1 mg/m2, 2.5 mg and 1 mg, respectively) and decreased to 0.5 mg tablets due to elevated trough levels. Sirolimus trough level was 7.4 ng/ml 8 days after initiation, prompting a dose reduction to 0.5 mg daily. Sirolimus trough remained between 7.4 ng/ml and 10.5 ng/ml, measured weekly. ALT, AST and GGT returned to baseline within three weeks. Corticosteroids were tapered by day 77. Sirolimus was discontinued on day 97 (week 13). 2a. Changes over time of ALT, AST, GGT. 2b. Change from baseline (%) of ALT, AST, GGT. 2c. Changes of CK and LDH during interventions. Decline of ALT and AST occurs prior to decline of GGT. ALT: alanine aminotransferase; AST: aspartate aminotransferase; CK: Creatine Kinase; LDH: Lactate dehydrogenase; GGT: gamma-glutamyl transferase. Daily sirolimus dose above dotted line. Blue area shows period of increased steroids, gray (dotted) area shows steroid taper.
Patient 3
Patient 3 is a 56 Kg 16-year-old non-ambulatory male with an intronic mutation in exon 7, who received daily deflazacort since 11 years of age. He was started on additional prednisone the day before the infusion following prescribing information at a total daily dose of 60 mg of prednisone equivalent. The patient reported headache and fever on day 2 (T max 38.5°C), as well as intermittent nausea and emesis during the first week after infusion. He was also found to have leukopenia (white blood cell count [WBC] nadir: 3700/μL on day 5 post infusion from 8000/μL at baseline), and thrombocytopenia (platelet count nadir: 131,000/μL on day 6 from 282,000/μL at baseline). All these parameters improved by day 10. The patient also demonstrated marked elevation of ferritin (peak 884 ng/mL on day 5, up from 220 ng/mL on day 3; ULN: 102 ng/mL; no baseline), along with an elevated CK compared to baseline (4,303U/L from 2,825U/L) and AST (108 IU/L from 74 IU/L) with stable ALT. All symptoms resolved by day 8.
The patient then presented with rapid elevation of ALT, AST and GGT, reaching approximately two times baseline in the case of ALT and AST, and four times baseline for GGT on day 43 post-infusion (week 6). Compared with the week prior, GGT values had doubled (baseline GGT: 10 U/L; day 43: 44 U/L; ULN: 61 U/L). He received additional prednisone at a dose of 40–60 mg per day for seven days (total dose 90–110 mg of prednisone). During this period, GGT continued to increase, peaking at 51 U/L (five times baseline), even though ALT and AST stabilized. Simultaneously, a work-up for infectious causes of hepatitis including EBV, CMV, Parvovirus B19, Adenovirus serology and PCR was performed and resulted negative for active infections. He did not undergo abdominal imaging.
Sirolimus was initiated on day 55 (week 8) at a loading dose of 4.5 mg (3 mg/m2) followed by a daily dose of 1.5 mg (1 mg/m2) with rapid improvement in all laboratory values. Additional corticosteroids were progressively tapered off by day 85 (week 12). Sirolimus was discontinued on day 100 post-dosing (week 14) following a reduction of the dose during the prior week. Trough levels were maintained between 4–7 ng/mL. Synthetic function was monitored every one to two weeks and remained normal.
The patient developed a very mild facial acneiform rash, around week 12, while on sirolimus, which resolved within a few days. Laboratory values and management are depicted in Figure 3.
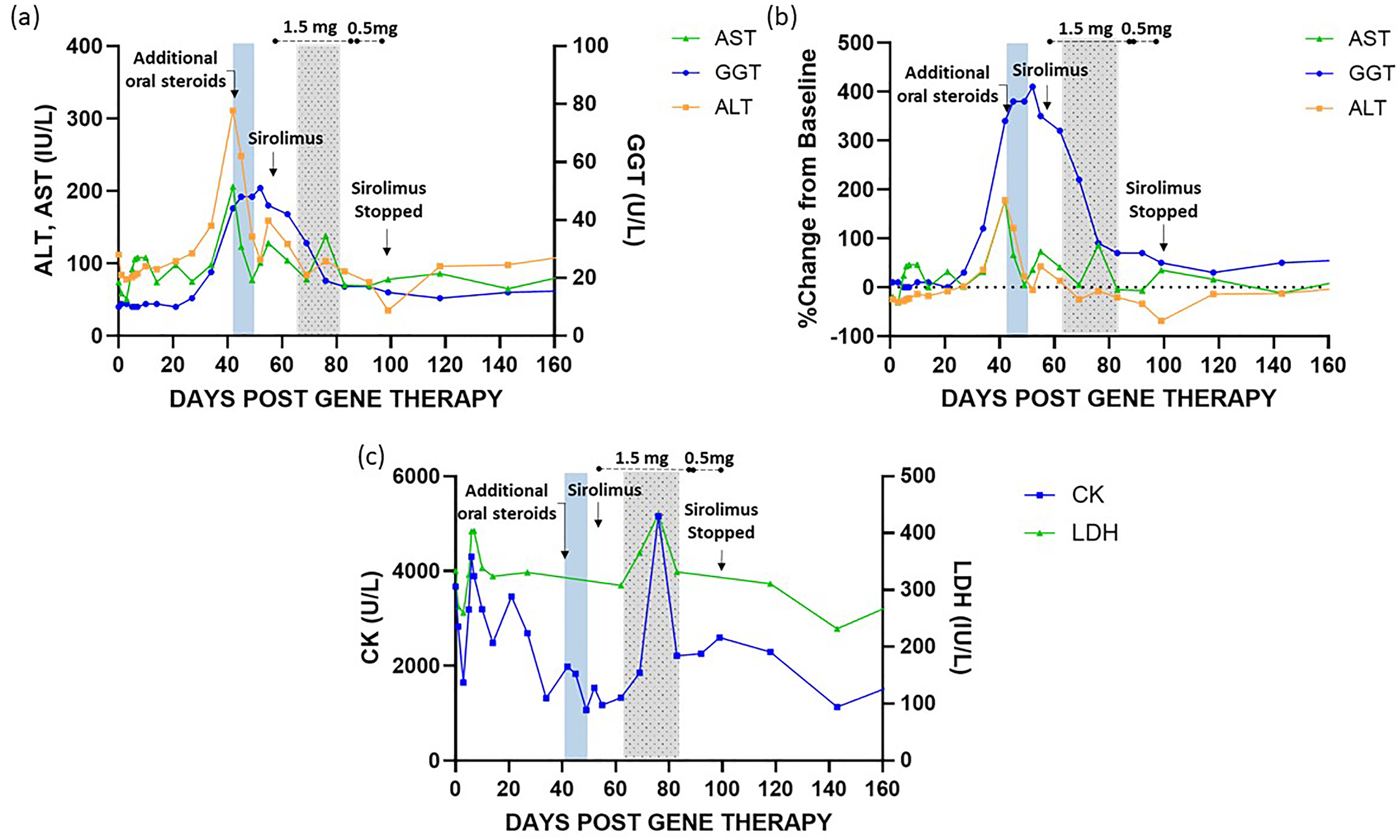
Laboratory changes and interventions for patient 3. The patient is a 16-year-old with an intronic deletion in exon 7 of the Dystrophin gene. ALT and AST increased over two times baseline and GGT increased four times compared to baseline on day 43 post-infusion (week 6). He received additional prednisone (40–60 mg/d for seven days) and GGT continued to increase, with stable ALT and AST. Sirolimus was initiated on day 55 (week 8). Corticosteroids were progressively tapered off by day 85 (week 12). Sirolimus was discontinued on day 100 post-dosing (week 14). Trough levels were maintained between 4–7 ng/mL. This patient demonstrated leukopenia and thrombocytopenia (not showed) and elevated CK during the first week post-dosing. 3a. Changes over time of ALT, AST, GGT. 3b. Change from baseline (%) of ALT, AST, GGT. 3c. Changes of CK and LDH demonstrating an acute elevation of CK and LDH during the first week after dosing. ALT: alanine aminotransferase; AST: aspartate aminotransferase; CK: Creatine Kinase; LDH: Lactate dehydrogenase; GGT: gamma-glutamyl transferase. Daily sirolimus dose above dotted line. Blue area shows period of increased steroids, gray area shows steroid taper.
Patient 4
Patient 4 is an eleven-year-old, 43 Kg ambulatory male with an intronic deletion in exon 7 (sibling of patient 3), who had been on chronic deflazacort since age 7. He received a total daily corticosteroid dose of 48 mg (prednisone equivalent), instead of 60 mg due to a mistake during the conversion from deflazacort to prednisone. Similar to patient 3, he developed nausea, intermittent emesis, and fatigue (without worsening weakness) beginning on day 3 post-dosing, as well as elevated CK from baseline (peak: 19,000U/L on day 4; baseline: 4789 U/L) hyperferritinemia (peak: 1496 ng/mL on day 4; 88 ng/mL on day 2) and leukopenia (WBC nadir: 4100/μL on day 4, lymphocyte count: 940/μL on day 4, LLN: 1400/μL, baseline WBC count: 8200/μL). Symptoms and laboratory values improved within three days. The patient received ondansetron as needed.
On day 51 (week 7) post-infusion, the patient presented with an increase in ALT, AST, GGT levels (GGT: 30 U/L from 9 U/L at baseline, ALT: 239 U/L from 167 U/L, AST: 149 U/L from 113 U/L) prompting a three-day course of additional prednisone at a dose of 40 mg daily (total dose: 90 mg prednisone), without improvement of GGT levels (GGT: 37 U/L). Sirolimus was initiated on day 71 post dosing (week 11) at a dose of 3 mg per day (slightly lower than the calculated dose of 3.8 mg based on body surface area), followed by a daily dose of 1 mg, and discontinued on day 110 (week 15), after a week on a reduced dose. Sirolimus troughs were 3.6 ng/mL and 4.2 ng/mL on 1 mg tablets. Additional corticosteroids were tapered back to baseline dose on day 97 (week 13).
Additional infectious work up was unremarkable for CMV, EBV, Adenovirus, and Parvovirus B19. Bilirubin and hepatic synthetic function remained normal throughout. The patient did not undergo imaging studies. Figure 4 shows laboratory trajectories and management.
Laboratory changes and interventions for patient 4. The patient is an 11-year-old with an intronic delection in exon 7 of the Dystrophin gene. On day 51 (week 7) post-infusion, he had an increase of ALT, AST and GGT. GGT increased had a three-fold increase from baseline, prompting a three-day course of additional prednisone at a dose of 40 mg daily. Sirolimus was administered from day 71 to day 109 post-dosing (week 10 to week 15) at a dose of 3 mg per day followed by a daily dose of 1 mg, and discontinued on day 110 (week 15), after a week on a reduced dose. Sirolimus troughs were 3.6 ng/ml and 4.2 ng/ml after one week and two weeks on 1 mg tablets, respectively. Additional corticosteroids tapered back to baseline dose on day 97 (week 13). Similar to patient 3, this patient demonstrated leukopenia and thrombocytopenia (not showed) and elevated CK during the first week post-dosing. 4a. Changes over time of ALT, AST, GGT. 4b. Change from baseline (%) of ALT, AST, GGT. 4c. Changes of CK and LDH demonstrating an acute elevation of CK and LDH during the first week after dosing. ALT: alanine aminotransferase; AST: aspartate aminotransferase; CK: Creatine Kinase; LDH: Lactate dehydrogenase; GGT: gamma-glutamyl transferase. Daily sirolimus dose above dotted line. Blue area shows period of increased steroids, gray area shows steroid taper.
Discussion
Hepatotoxicity has been described in animals and humans following administration of AAV products, with poor concordance in findings between species.32,33 In humans, there is evidence of a cell-mediated response to the AAV capsid based on clinical and histopathological reports across different clinical trials and post-marketing reports, including studies in patients with hemophilia, spinal muscular atrophy, X-linked myotubular myopathy (XL-MTM), among other conditions.2,6,15,16 During a gene therapy trial using AAV2 for the treatment of hemophilia B, transient hepatic enzyme elevation and loss of factor IX expression were attributed to a cellular response. 34 Furthermore, several cases of hepatoxicity related to onasemongene abeparvovec-xioi demonstrated periportal CD8+ T cells with a polymorphic inflammatory infiltration (neutrophils, eosinophils and plasma cells), hepatocyte degeneration and ductal reaction, with persistent fibrosis in one case.16,33,34 A particular case is that of patients with XLMTM1, in whom preexisting liver disease seemed to play an important role. Histopathological findings from patients in this cohort demonstrated cholestatic changes with peliosis or giant cell hepatitis and cirrhosis associated with severe intrahepatic cholestasis. 35 The study resulted in the death of four patients and severe non-fatal hepatobiliary dysfunction in five others. 33 .
Additional inflammatory pathways have been associated with liver toxicity in pre-clinical models including an innate immune response to the capsid through the Toll-Like-Receptor 9 (TLR-9) pathway, acellular mediated response to the transgene, and direct effect on hepatocytes, although these have not been clearly described in humans.33,36 Another potential contributor to this and other immunologic responses is the total amount of capsid protein delivered with AAV-gene therapy and is a function of the product characteristics, especially the full:empty ratio of the drug product. A systemic AAV vector infusion leads to a very high instantaneous capsid protein exposure, unlike a natural viral infection. When considering the total capsid exposure, the primary driver of immune complex formation, a 20 kg patient would receive a total dose of 2.66 × 1015 vg or 200 mL of drug product. The protein concentration of delandistrogene moxeparvovec-rokl is 330 μg/mL (+/- 50 μg/mL), which represents the vector capsid protein given the high purity of a commercial AAV product. Therefore, for a 20 kg patient, the total protein exposure is 66 mg, which is a substantial challenge of a non-self antigen. 3
By inhibiting mTORC1, sirolimus effectively blocks T-cell activation and proliferation, particularly by interfering with the signaling pathways activated by interleukin-2 (IL-2) and other growth factors.19,20 Sirolimus has been extensively used in patients undergoing solid organ transplantation, and as a steroid sparing agent in patients with a variety of conditions, with well-established pharmacokinetics and pharmacodynamics in the pediatric population.3,21,24,31,37,38
The decision to utilize sirolimus rather than calcineurin inhibitors, such as tacrolimus was guided by several mechanistic and safety considerations. In addition to its T-cell effects, sirolimus also impairs B-cell activation and antibody production.20,24,39 This dual action is particularly relevant in the context of AAV gene therapy, where capsid-driven immune responses may involve both arms of the adaptive immune system.3,15 Sirolimus has been shown to inhibit B cell proliferation, decrease T cell dependent antibody production and increases B cell apoptosis. 22 Sirolimus can effectively block B cell differentiation into plasma cells even at low dose (trough level of 2 ng/ml), and can totally suppress plasma cell development at a level of 6 ng/ml. 22 In contrast, tacrolimus primarily acts on T-cell–mediated pathways and has limited effect on B-cell modulation. 22 Given the possibility of neutralizing antibody production or complement-mediated injury following AAV delivery, we prioritized sirolimus for its broader immunomodulatory profile. In addition, we have shown in pre-clinical studies that further suppression of B-cell activation by pre-treatment with a combination of rituximab and sirolimus both attenuates liver injury but also significantly augments the effect of the AAV-mediated gene therapy. 23
Side effects related to the use of sirolimus have been well described. The most common side effect is stomatitis, particularly with long-term use, occurring in about 52% of patients. Acneiform rash has been observed in about 10% of patients, as well as menstrual abnormalities, diarrhea, respiratory infections, and decreased appetite with lower frequency. 40 In addition, interstitial pneumonitis has been described in patients receiving sirolimus, although this appears to be more common at higher therapeutic levels and with long-term administration.41–43 Hyperlipidemia, thrombocytopenia, and leukopenia can also be seen in patients receiving sirolimus, although transient elevations of white blood cell counts are possible with long-term use.40,44 Furthermore, sirolimus was selected for its favorable hepatic safety profile at the dosing regimen employed in this cohort. While sirolimus has historically been associated with hepatotoxicity and increased malignancy risk in solid organ transplant recipients, these adverse effects are generally observed at a higher therapeutic target level.45–47 In the patients described, our therapeutic goal was a trough level of 3–7 ng/mL, based on our previous experience and published literature.3,22,24,31 The doses required to achieve this therapeutic range was well tolerated overall, although trough levels were higher at times primarily due to limited availability of the liquid formulation for dose adjustments. Two patients developed a mild and time-limited acneiform rash, possibly related to sirolimus administration. While our initial dosing of sirolimus was guided by prescribing information and published data 48 and achieved therapeutic levels within the first week of administration, the required dose reduction in the first patient led us to initiate a lower starting dose for patient 4, which resulted in adequate trough levels.
In the four cases described, the use of sirolimus resulted in rapid improvement of hepatic abnormalities and allowed us to safely taper additional steroids, which can often cause significant side effects. It is important to mention that although patient 4 received a slightly lower dose of prednisone before and during the first few weeks of post-dosing monitoring, and higher doses of steroids might have prevented or accelerated the resolution of liver abnormalities , we opted for a more proactive approach based on the clinical response and trajectory observed in our three previous cases, including patient 3, his sibling. This decison was made particularly in light of the recently reported fatalities associated with delandistrogene moxeparvovec-rokl.
This manuscript highlights the importance of proactive and close monitoring of patients receiving gene therapy products, as even subtle changes in laboratory parameters from baseline may require adjustments in follow up frequency or management of any potential side effects, including hepatotoxicity. The use of a single arbitrary laboratory cutoff value for all patients may delay the identification of adverse events and subsequently delay appropriate interventions. In our cohort, increases in laboratory values of 1.5–3 times above baseline prompted the initiation of additional steroids, which in some cases appeared to temporarily halt liver abnormalities. However, close monitoring of trends allowed us to initiate sirolimus within a reasonable timeframe, before significant liver injury occurred.
At our institution, we have treated a total of twenty-nine patients with delandistrogene moxeparvovec-rokl. This number includes twenty-one ambulatory and eight non-ambulatory patients aged 4 to 20 years at the time of dosing, with an observed incidence of hepatotoxicity of 14% (N = 4), and no cases of synthetic dysfunction or liver failure. While accurate reporting of transient or mild cases of hepatotoxicity is now a significant challenge after commercial approval of these medications, this manuscript and recent events highlight the importance of administering this and other advanced therapeutics at centers with the experience and resources to identify and manage this and multiple other complications related to gene therapy. 30
Our study is limited by the small number of patients but demonstrates a feasible approach for the treatment of hepatoxicity in patients receiving AAV products. Furthermore, preclinical data suggests that the use of sirolimus in conjunction with AAV products can lead to a potential increase in protein expression.
Conclusion
This report highlights a consistent pattern of hepatotoxicity emerging several weeks after delandistrogene moxeparvovec-rokl infusion in patients with DMD. While corticosteroids remain the mainstay of immunosuppressive management, our findings suggest that sirolimus may serve as an effective adjunct in these cases. At low therapeutic doses, sirolimus was well tolerated and associated with timely normalization of liver enzymes without systemic toxicity. As AAV-based gene therapies are increasingly adopted in clinical practice, vigilant post-infusion monitoring and a proactive, individualized immunosuppressive strategy, including the use of mTOR inhibitors, are critical to optimizing patient safety and therapeutic success. Larger prospective studies are needed to define the optimal timing, duration, and therapeutic thresholds for sirolimus in this setting, as well as to evaluate the prophylactic use of sirolimus given its potential to enhance gene expression and improve the durability of the therapeutic effect, or its impact in the reduction of the severity of hepatoxicity in aggressive cases when used prior to gene therapy administration.
Footnotes
Acknowledgments
We want to acknowledge and thank our patients and their families for their participation and consent.
ORCID iDs
Ethical considerations
This study was approved by the University of Florida Institutional Review Board under the following study protocols IRB201600103 and IRB201900677.
Consent to participate
Patients’ legal guardians provided written informed consent. Whenever appropriate, patients provided written assent for participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BJB and MC receive funding from National Institute of Neurological Disorders and Stroke (grant number U01-NS116752-01A1) and Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant number R01HD052682).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article. BJB is a member of the Global Pompe Advisory Board supported by Sanofi. BJB has received consulting fees from Amicus Therapeutics, Rocket Pharma, and Tenaya. BJB and CLA are site investigators of clinical trials sponsored by Sarepta Therapeutics. BJB and MC are a co-founders of Ventura Life Sciences, LLC. CDZ has received consulting fees from Scholar Rock and ML Bio MC has received consulting fees from UniQure, Voyager, Entrada, TRiNDS and Neurogene. The University of Florida is entitled to licensing revenue related to AAV technology. BJB is an uncompensated member of the Muscular Dystrophy Association Board of Directors.