
Abstract
The evolving landscape of generalised myasthenia gravis (gMG) treatment with new targeted immunotherapy options presents challenges for neurologists and potentially leads to therapeutic inertia (TI), the failure to initiate or intensify treatment when therapeutic goals are not met. This study aimed to assess neurologists’ therapeutic decision-making process in gMG and its influencing factors. A cross-sectional, web-based study was conducted, involving 149 neurologists (mean age [standard deviation]: 39.0 [9.4] years; 54.4% male; median MG experience [interquartile range]: 7 [3–15] years). Participants responded to 8 simulated case scenarios, 7 of which assessed TI. Overall, 79.9% of neurologists (n = 119/149) exhibited TI in at least 2 of the 7 scenarios. Multivariate analysis revealed that lower organisational support (odd ratio [OR] = 0.308, 95%CI:0.109–0.870, p = 0.0262) and greater reluctance to adopt new treatments (OR = 0.015, 95%CI:0.001–0.739, p = 0.0347) were significant predictors of TI. Understanding these factors is crucial for optimising gMG treatment decisions, underscoring the importance of updated guidelines and continued professional education.
Keywords
Introduction
The therapeutic landscape of generalised myasthenia gravis (gMG) has evolved drastically in recent years. Six targeted treatments showed positive results in phase III clinical trials demonstrating their efficacy and safety in adult gMG patients with antibodies against the nicotinic acetylcholine receptor (AChR-IgG).1–6 Some of these treatments focus on diminishing the levels of autoantibodies, either by preventing their recycling through the neonatal Fc receptor (FcRn) (efgartigimod, rozanolixizumab, nipocalimab)1–3 or by depleting CD19+ B cells, which include antibody-producing plasmablasts (inebilizumab), 5 whereas other treatments focus on preventing the damage caused by autoantibodies by blocking the complement cascade at the C5 stage (eculizumab, ravulizumab, zilucoplan).4,6,7 Most of these treatments have become available for use in clinical practice at a similar time and have growing positive long-term evidence from clinical trials,8–10 as well as emerging real-world neurologists’ experiences.11–14 In Spain, only efgartigimod, rozanolixizumab, ravulizumab, and zilucoplan are approved and reimbursed for use in clinical practice for gMG.
Despite the recent approval of the first treatments specifically developed for gMG, neurologists may encounter challenges during therapeutic decision-making.15,16 This complexity arises from the diverse drug profiles, few scientific guidelines and consensus regarding their application and limited personal experience with these novel therapies.16–19 Moreover, clinicians must weigh the adoption of these new treatments against the option of using one or more broad-spectrum immunosuppressants. The latter are drugs they are more familiar with, and which are widely used in their clinical practice. All these factors can lead to therapeutic inertia (TI), defined as the lack of treatment initiation or escalation when therapeutic goals are not met. 20 TI is a complex issue with contributing factors at the healthcare system, healthcare professional, and patient levels.21,22 Regarding physicians, it has been particularly associated with certain professional factors, such as fewer years of experience, a lower number of patients treated, non-specialisation in the disease, or working in a non-tertiary care centre.20,23,24 Additionally, personal factors such as aversion to ambiguity, being a risk-taker, or having non-innovative profile may contribute.
Within this evolving therapeutic landscape, characterised by the emergence of numerous novel treatment options and inherent resistance to departing from established practices, we aimed to elucidate neurologists’ decision-making processes in gMG. This involved assessing the prevalence of TI, treatment choices, and their associated factors.
Methods
Study design and participants
PROMPT-MG was an online, non-interventional, cross-sectional study in collaboration with the Spanish Society of Neurology (SEN) designed to assess therapeutic decisions in AChR-IgG seropositive gMG. From April to July 2024, neurologists assisting adult patients with myasthenia gravis (MG) were invited to participate by email and proactively answered an online survey. Further details can be found in the previously published protocol. 25 The study was conducted in accordance with the International Conference on Harmonisation Guidelines for Good Clinical Practice and the ethical principles of the Declaration of Helsinki and was approved by the investigational review board of Hospital Clínico San Carlos (Madrid, Spain). All participants provided written informed consent.
Outcome measures
Eight simulated case scenarios were developed to assess neurologists’ therapeutic decision-making in AChR-IgG seropositive gMG patients. Seven of these scenarios were specifically designed to evaluate TI, featuring diverse patient presentations: two cases of Myasthenia Gravis Foundation of America (MGFA) classification IIa with limb symptom worsening (one treated with azathioprine and the other treated with azathioprine plus corticosteroids), two cases of MGFA IIb with bulbar symptom worsening (one treated with azathioprine and the other treated with azathioprine plus corticosteroids), two cases of rapidly progressing disease (one naïve and one treated with azathioprine plus corticosteroids), and one treated-patient with persistent ocular symptom worsening. A single control case was also included to mitigate random responses from participants (Supplementary material). The simulated case scenarios were carefully designed to see if different factors –like the location of weakness (limbs versus bulbar muscles), the type of therapy (monotherapy versus combination), or a rapid symptom progression– would result in different treatment plans. The cases were straightforward and avoided ambiguous symptoms like occasional eyelid drooping. Furthermore, possible subjectivity of patient-reported symptoms was reduced by stating the weakness was confirmed by the Quantitative Myasthenia Gravis scale in all case scenarios, thus reducing possible variability between patients and physicians.
TI was defined as the lack of treatment initiation or escalation when the patient presented a Myasthenia Gravis Activities of Daily Living scale (MG-ADL) score of at least 1 after enough time receiving the treatment and/or when there were severe adverse events associated with the treatment. 25 Corticosteroids, azathioprine, and mycophenolate mofetil were grouped as lower-efficacy treatments; accordingly, treatment escalation was considered as switching to one of the newly approved treatments. 11 This was based on solid results in clinical trials and growing experience from new targeted treatments, deemed as more efficacious or having a greater probability of achieving the proposed goal with a better benefit-risk profile than off-label treatments.2–4,6 This approach ensures a demanding therapeutic goal for gMG of an MG-ADL score of 0, with a possible minor weakness of some muscles on examination,26–28 ensuring as well a rapid treatment escalation and avoiding switching between similar non-specific immunosuppressants. As eculizumab and nipocalimab were not available for clinical practice in Spain at the time this study was conducted, only efgartigimod, ravulizumab, rozanolixizumab, and zilucoplan were included among the possible answers. Furthermore, acetylcholinesterase inhibitors were excluded from the answers and indicated at the beginning of the exercise. This was made to avoid aggregating complexity by including a lower efficacy category and possible combinations, since the majority of patients described in case scenarios were already treated with at least one immunosuppressant treatment.
Participating neurologists provided demographic and professional information to identify potential associations between these characteristics and therapeutic decisions. To further explore factors influencing decision-making, neurologists completed various questionnaires. These included scales assessing resistance to change,29,30 healthcare-related regret (Regret Intensity Scale, RIS-10), 31 burnout (a single-item measure from the Physician Work Life Study), 32 attitudes towards clinical risks, empathy (Jefferson Scale of Physician Empathy, JSPE), 33 work engagement (Utrecht Work Engagement Scale, UWES), 34 and personality traits (Big Five Inventory, BFI-10). 35 A summary of these assessments and their corresponding scores can be found in the Supplementary Material (Table S1), with further details available in the previously published protocol. 25
Statistical analysis
Descriptive statistics were calculated. For continuous variables, measures of central tendency (mean and median) and variability/dispersion (standard deviation [SD] and interquartile ranges [IQR]) were used. Categorical variables were reported as absolute and relative frequencies (percentages).
The presence of TI was determined by at least one incorrect response according to the established definition in any of the clinical case scenarios, and this criterion was used to compute TI prevalence. The TI score was defined as the number of simulated case scenarios per participant with an incorrect response (e.g., a score of 0 means no TI is present in any of the simulated case scenarios). Therapeutic error (TE) in turn was defined as no action taken by the participating neurologist, which meant choosing the option of maintaining the current treatment in the clinical case scenario. For this analysis, case 3 was eliminated as there was no such option in the responses. The TE score was defined as the number of simulated case scenarios with no action taken by the participant. The relationship between neurologists’ characteristics (demographic, professional and behavioural) and the presence of TI/TE was analysed using the Chi-square test for categorical variables and the Mann-Whitney U test for continuous variables. Statistical significance was considered for p < 0.05.
To assess predictors of TI, univariate analysis was used to assess the relationship between neurologists’ characteristics and the dichotomous outcome of TI presence, considering each predictor individually. Variables with p < 0.1 were then entered into a multivariate logistic regression model. Odds ratios (ORs) and their corresponding 95% confidence intervals (95% CI) were calculated.
Results
A total of 2,050 neurologists received the email invitation to participate in the study. Of those, 185 neurologists agreed to participate in the study, with 149 (80.5%) ultimately being included in the analysis. Of those agreeing to participate but not included, 19 registered but did not enter any data, 8 withdrew their consent, and 9 did not complete the cases. None of the participants answered the control case incorrectly; therefore, no participants were excluded from the final sample based on this criterion. The mean age (SD) was 39.0 (9.4) years, and 81 (54.4%) were male. The median years of experience managing MG patients (IQR) was 7 (3–15), with a median of 10 (5–20) patients monthly. Most participants, 141 (94.6%), worked at academic hospitals, and 48 (32.2%) were neuromuscular specialists. Additional characteristics are detailed in Table 1.
Demographic, professional, and behavioural characteristics of participants.
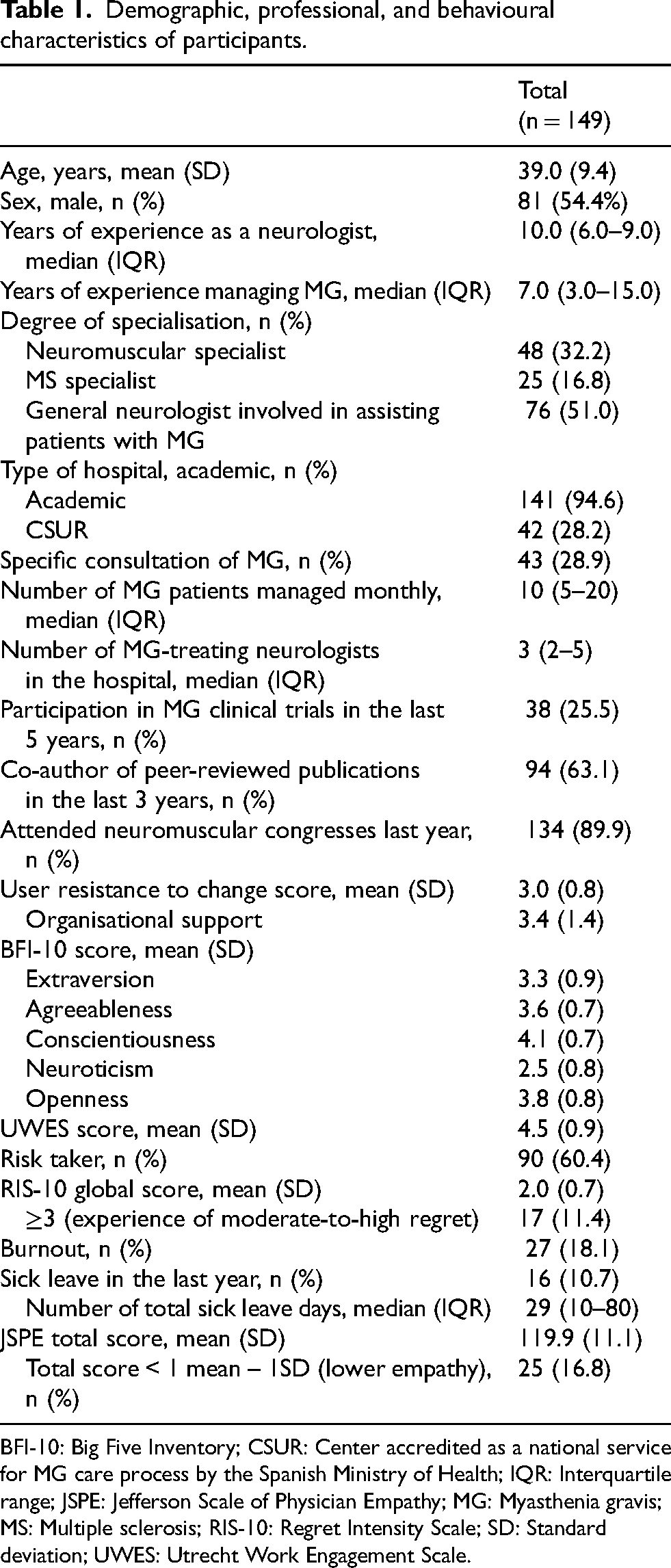
BFI-10: Big Five Inventory; CSUR: Center accredited as a national service for MG care process by the Spanish Ministry of Health; IQR: Interquartile range; JSPE: Jefferson Scale of Physician Empathy; MG: Myasthenia gravis; MS: Multiple sclerosis; RIS-10: Regret Intensity Scale; SD: Standard deviation; UWES: Utrecht Work Engagement Scale.
Therapeutic inertia in gMG
TI was present in 79.9% of participants (n = 119) in at least 2 out of 7 scenarios. Results per simulated case scenario can be found in Table 2. Ten participants (6.7%) had no TI in any of the case scenarios, whereas 22 (14.8%) showed TI in all cases (Figure 1). The mean TI (SD) score was 3.7 (2.1). Individual choices per case are detailed in the Supplementary Material.
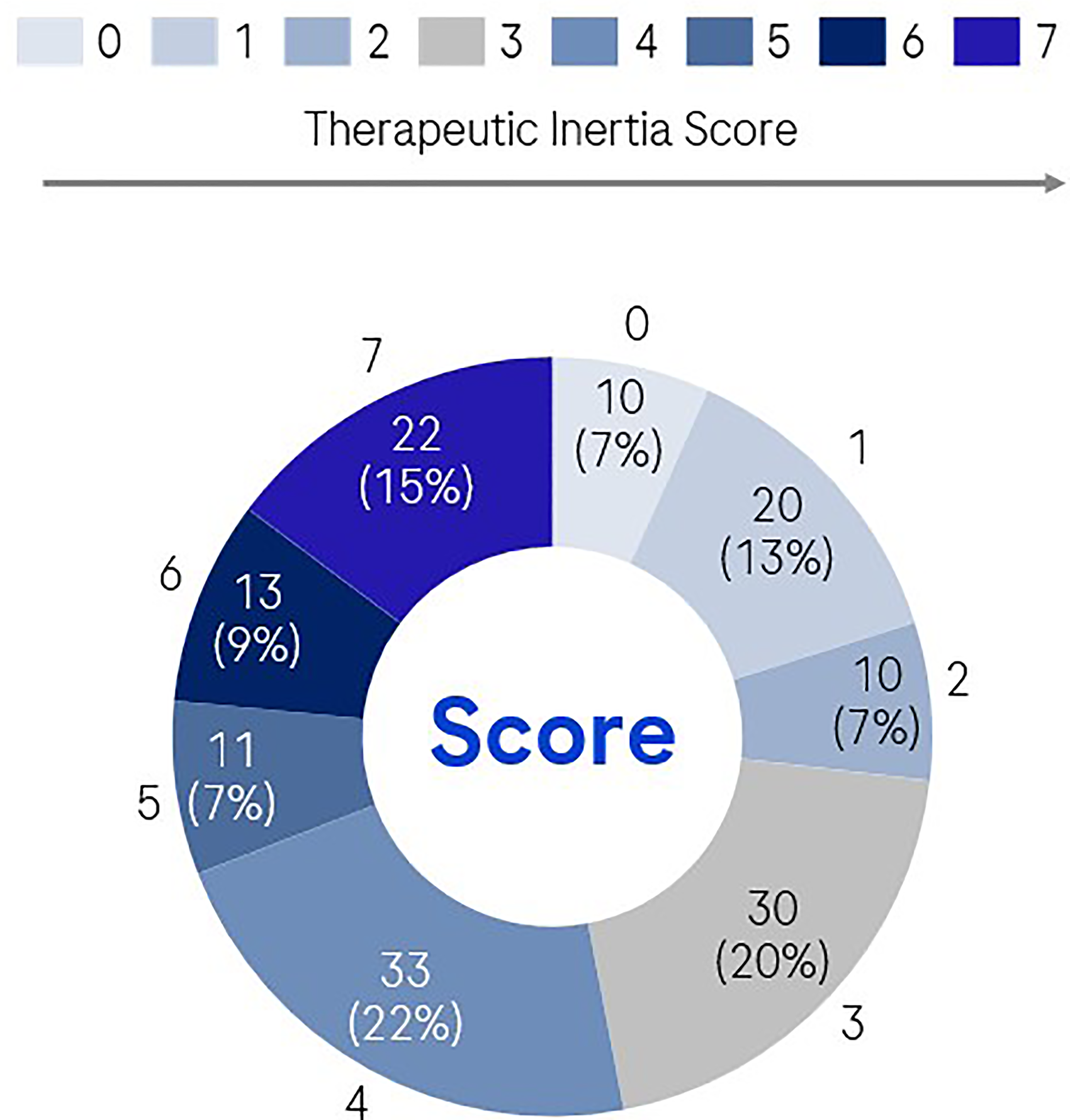
Therapeutic inertia score.
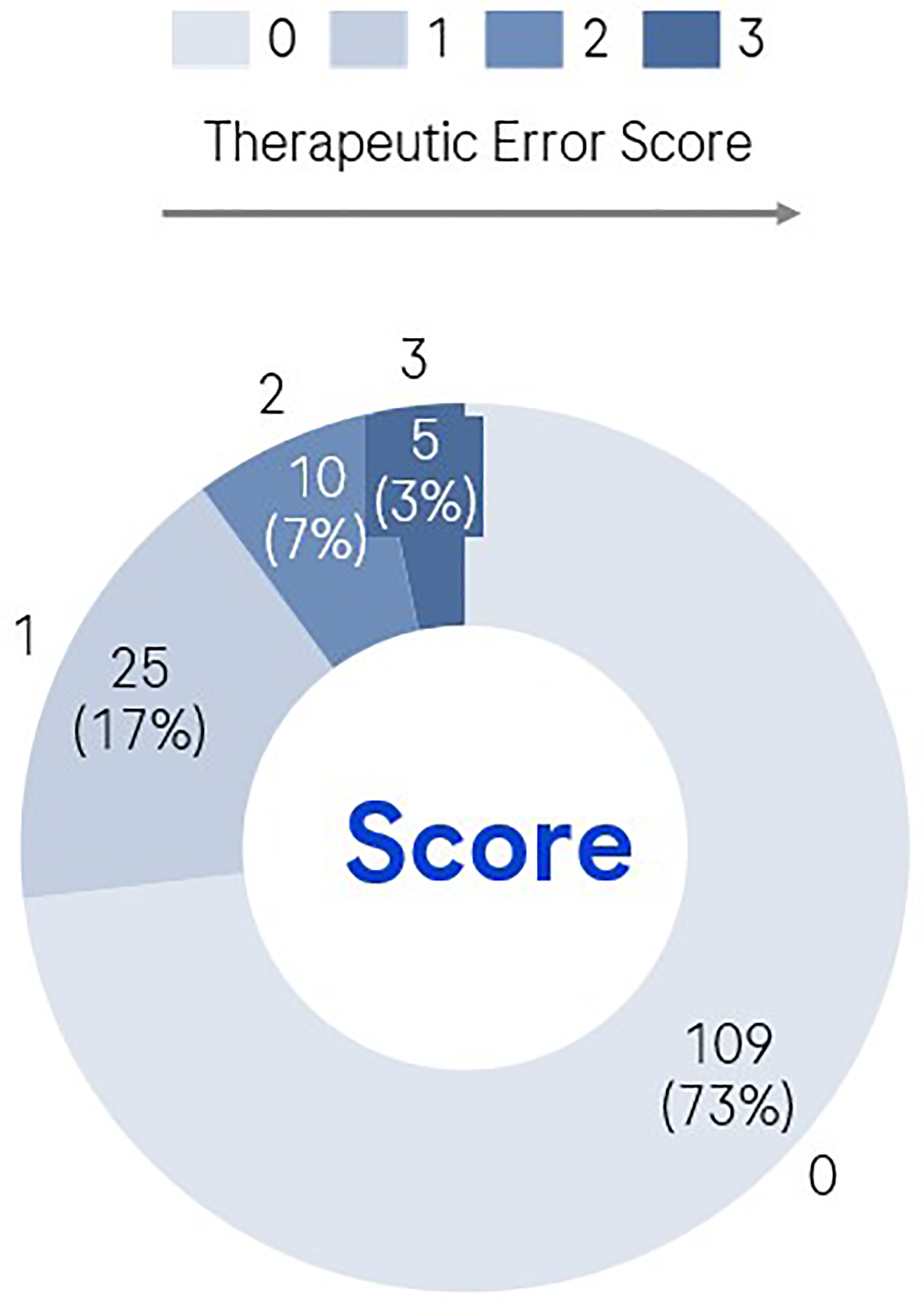
Therapeutic error score.
Therapeutic inertia and therapeutic error in simulated case scenarios (N = 149).
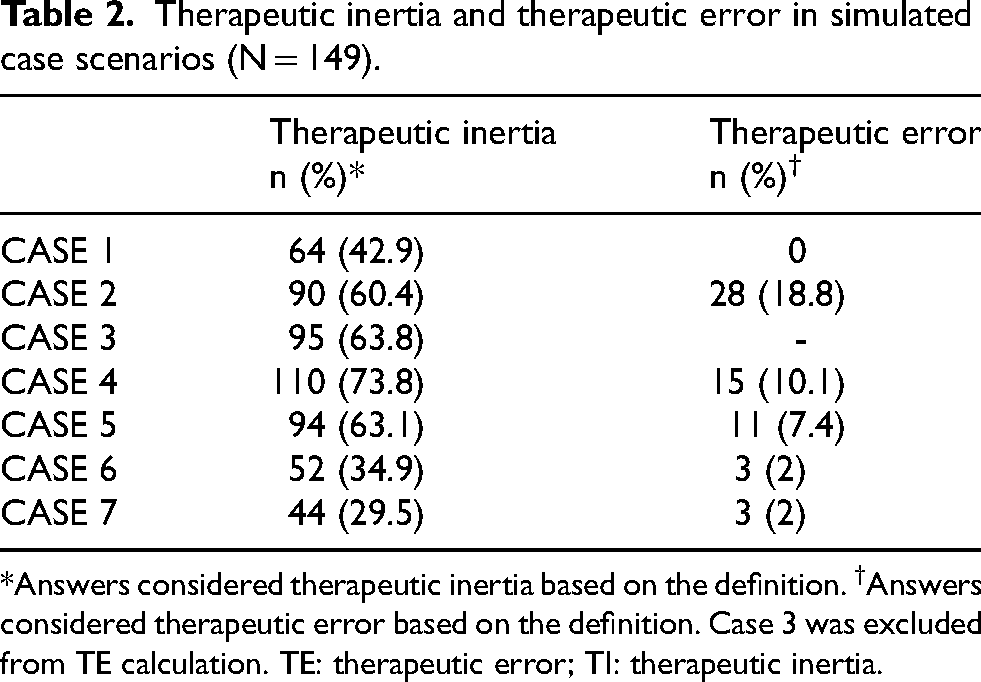
*Answers considered therapeutic inertia based on the definition. †Answers considered therapeutic error based on the definition. Case 3 was excluded from TE calculation. TE: therapeutic error; TI: therapeutic inertia.
When considering all cases collectively, the presence of TI was associated with a lower perceived ease of use for new targeted treatments (p = 0.0162), reduced organisational support for their introduction (p = 0.0156), and greater overall user resistance to change behaviour (p = 0.0161). When evaluating the cases individually, factors related to the presence of TI included: being a neuromuscular specialist or general neurologist (cases 1, 2 and 5); exhibiting factors related to greater resistance to change concerning the adoption of new treatments for gMG (cases 1–4, and 7); greater risk aversion (cases 2 and 7); lower empathy (cases 1 and 7); a greater openness personality trait (cases 5 and 7); lower burnout (case 5); a fewer number of MG-treating neurologists in the hospital (case 5); and a lower dedication to work (case 7). No factors were related to TI presence in case 6. A summary of these correlations can be found in Table 3.
Factors related to therapeutic inertia (N = 149).
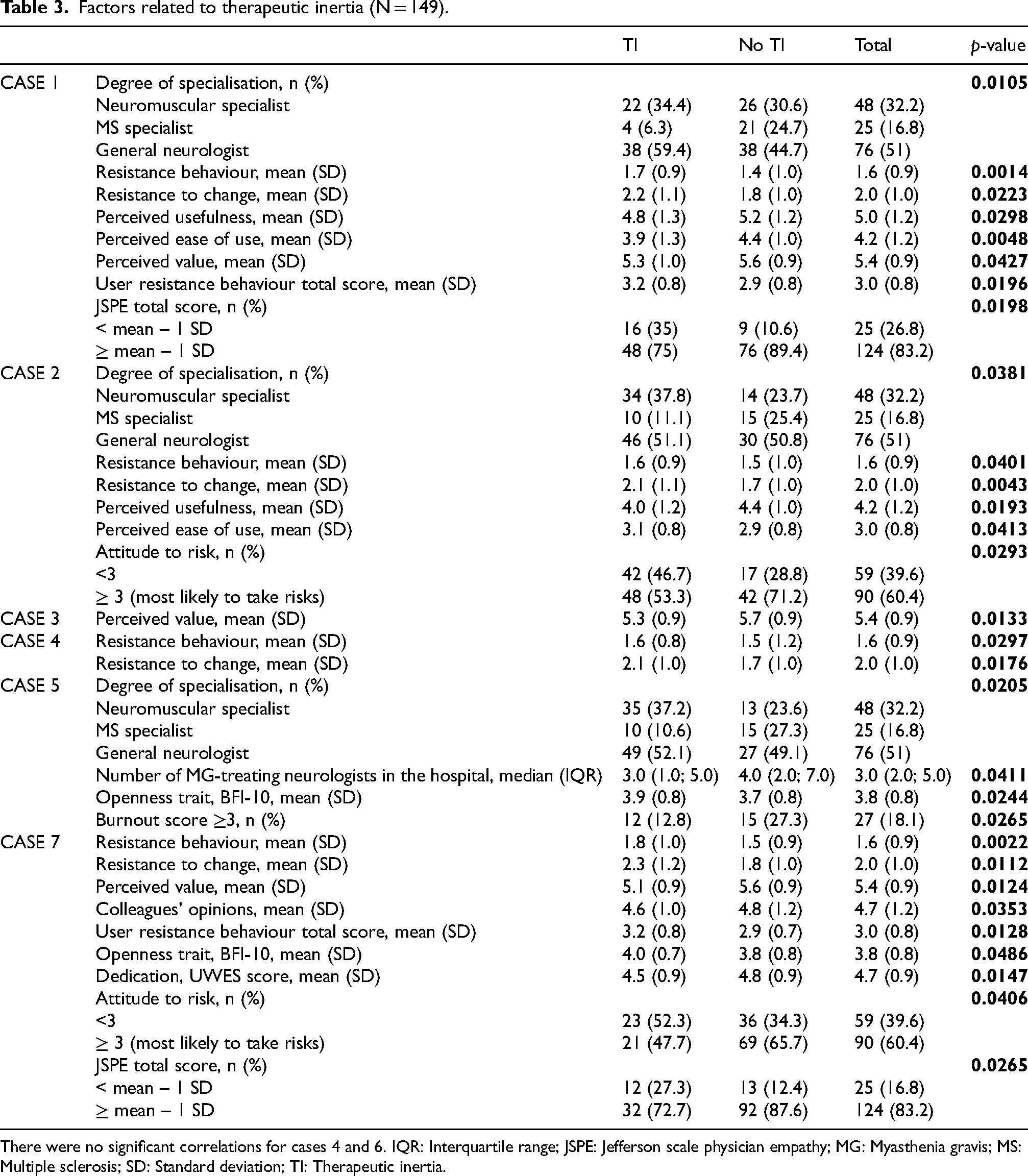
There were no significant correlations for cases 4 and 6. IQR: Interquartile range; JSPE: Jefferson scale physician empathy; MG: Myasthenia gravis; MS: Multiple sclerosis; SD: Standard deviation; TI: Therapeutic inertia.
In the multivariate analysis, a lower organisational support for change (OR = 0.308, 95% CI: 0.109–0.870, p = 0.0262) and greater user resistance to change (OR = 0.015, 95% CI: 0.001–0.739, p = 0.0347) were predictors of TI.
Therapeutic error in gMG
A total of 26.8% (n = 40) of neurologists exhibited TE, with instances divided into presenting TE in at least one case scenario (16.8%), two cases (6.7%) or three cases (3.4%) (Figure 2). Factors associated with the presence of TE included: managing MG together with other neurologists in the hospital (p = 0.0370), not attending neuromuscular congresses in the previous year (p = 0.0146), greater resistance to change regarding the adoption of new treatments (p = 0.0187), lower vigour and absorption towards work (p = 0.0194 and p = 0.0411, respectively), a higher number of sick leave days (p = 0.0387), and the presence of burnout (p = 0.0226).
Discussion
Traditional therapeutic management of gMG usually relies on corticosteroids and non-specific immunosuppressants.36–38 These therapies are often associated with a delayed onset of action and variable efficacy. Nearly half of patients may fail to achieve satisfactory control with these conventional treatments, indicating a substantial unmet need for more effective and tolerable therapeutic options. 15 Long-term use of these treatments can lead to adverse effects such as arterial hypertension, diabetes mellitus, osteoporosis, infections, increased risk of malignancies, hepatotoxicity, nephrotoxicity, and pancreatitis, among others, thereby requiring regular monitoring.38–41
In recent years, new targeted treatments have emerged.15,16 These therapies have a specific mechanism of action, which reduces the impact on the immune system and directly addresses the disease's pathogenesis, leading to a greater benefit-risk ratio. This may be of great importance in a disease where the highest prevalence is in individuals over 60 years of age.41,42 Despite these advances and guidelines recommending escalation, overturning the status quo of using well-established traditional non-targeted treatments can be challenging.15,16,18,38
Our study found that, in simulated case scenarios describing gMG patients receiving non-specific traditional treatments and experiencing persistent symptoms or rapid disease progression, 80% of the participating neurologists exhibited TI by not escalating treatment to one of the new targeted therapies. These outcomes were associated with a resistance to adopting innovations and a lower organisational support for change. Furthermore, one out of four participating neurologists demonstrated TE by taking no action and maintaining the current treatment.
A significant disease burden has been reported by gMG patients, including poor quality of life and decreased productivity due to the consequences of muscle weakness and side effects of medications.38,41,43 In fact, one-third to one-half of patients are dissatisfied with the management of their symptoms.44,45 Additionally, for each point increase on the MG-ADL score, the rate of exacerbation is elevated by 13%, 46 and up to 40% of patients have refractory disease.38,47 This might be more frequent in the first years after the diagnosis but still occurs in the long term. 48 Several studies reported high percentages of treatment escalation to a second line in incident patients, all around 80%,40,41,47,49 with a mean time between 1–9 months,41,47,50 a median of two treatment escalations per patient, 40 and percentages of 32.5% and 20% reaching a third line after a year and a fourth line, respectively. 47 Pyridostigmine is the most frequent treatment used, followed by corticosteroids, and immunosuppressants,40,47,50,51 but even the combination of these three medications as concomitant therapies is not enough to manage the disease in one out of four patients, highlighting the important need for innovative, effective, and well-tolerated therapies.16,47 Furthermore, in a recent survey exploring physicians’ decisions on the use of novel therapeutic agents, the most frequent treatments used as first-line option were azathioprine and mycophenolate mofetil, leaving the new treatments for refractory cases or as bridging therapies. 16 These results are in consonance with our findings of TI in gMG and uncover the high reliance on conventional treatment and corticosteroids, with an elevated steroid burden (nearly two-thirds of patients receiving high corticosteroid doses) leading to inadequate disease control in a large proportion of patients and suggesting the need for early use of more effective treatments.
On analysing patients’ perspectives, negative conversations are dominated by treatment issues, usually in corticosteroid-treated patients and in those with intravenous immunoglobulins, and symptom severity.45,52,53 Regarding conversations discussing treatment barriers, two-thirds focus on side effects and lack of efficacy, pointing to a need for treatment options that improve quality of life. 52 This is in consonance with a prospective observational study demonstrating that patients’ disease burden and symptoms are not well managed by conventional treatments, with symptom stability being a major treatment goal. 53 This suboptimal disease control and patient transition across various low-efficacy, non-specific treatments can in fact increase TI, as patients get frustrated when they have wasted several months trying to control their disease or when they have to make trade-offs between treatment efficacy and feeling better versus a treatment burden that diminishes their quality of life. 45
TI is a common occurrence when introducing innovative treatments into routine clinical practice, and it has been observed in neuro-immunological conditions such as multiple sclerosis and neuromyelitis optica spectrum disorder.20,23 In gMG, several factors are thought to contribute to TI, including a lack of consensus, concerns about potential additional side effects, and the time required to observe treatment benefits.16,25,38 A significant predictor of TI identified in our study was resistance to adopting new therapies. When clinical scenarios were examined individually, neuromuscular specialists and general neurologists showed higher rates of TI in some cases compared to demyelinating specialists. This difference may be attributed to the established shift in the therapeutic approach for multiple sclerosis and neuromyelitis optica spectrum disorder, where highly effective therapies are readily used when symptoms are not controlled, leading to easier overturning of the status quo. In contrast, neurologists specialising in neuromuscular diseases are encountering these innovations for the first time.23,54–56 The higher rates of TI among general neurologists who do not exclusively focus on MG align with previous research.24,57 This highlights the need for ongoing medical education and suggests that referring patients to specialised tertiary centres, which typically offer more continuous training and manage a larger volume of patients, could be beneficial. Increasing awareness about the growing practice of using these new targeted treatments earlier in the course of the disease to achieve rapid symptom control, optimal disease management, and limit permanent neuromuscular junction damage may also help reduce TI.16,38,40,46,58,59 It is important to note that the term TI should not be understood as pejorative or a negative judgement of physicians, but as a challenge or area for growth and development.21,22
Taking all this together, the shared decision-making process becomes even more relevant for preventing TI among patients and neurologists. Patients must communicate if they have symptoms that interfere with their normal lifestyle by keeping in mind the conscious or unconscious adaptations to diminish the impact of those symptoms. 60 Expert consensus recommends using the Patient Acceptable Symptom State (PASS) alongside the MG-ADL to determine patient satisfaction with symptom status and treatment. 61 This will help to reach a common approach between patients and their healthcare professionals to what is satisfactory control and quality of life. 43
Our study identified lower organisational support for the introduction of new targeted therapies as a significant predictor of TI. This finding underscores the critical role that institutional frameworks and resources play in facilitating the adoption of novel treatments in clinical practice.61–63 The reluctance to embrace new therapeutic approaches, even with their demonstrated efficacy and improved risk-benefit profiles, can be exacerbated by a lack of clear internal guidelines, insufficient training opportunities, or limited access to the necessary infrastructure for administering these therapies. While individual neurologists’ resistance to change is a factor, organisational support can mitigate this by fostering an environment conducive to innovation, providing comprehensive education on new treatments, and streamlining the processes for their integration into routine care. 62 Addressing this organisational aspect may be crucial for overcoming TI and ensuring that patients with gMG benefit from the latest advance in treatment.
Several limitations should be noted regarding our study. Firstly, its cross-sectional design prevents us from evaluating changes in therapeutic decisions over time or causality. Secondly, the limited experience in clinical practice with new targeted treatments, together with an overrepresentation of young participants, might have led to increased percentages of TI, as fewer years of experience has been described as a factor related to TI. 20 In turn, as the study was performed only with Spanish neurologists, the results obtained might not apply to other countries. Thirdly, although specifically stated at the beginning of the clinical cases that it was a hypothetical situation without costs or protocol/guidelines restrictions, inherent drug factors, such as price, or patient factors could be indirectly affecting participant answers. Furthermore, our study lacked the reasons for neurologist's treatment choices and, although including it might have led to cognitive fatigue due to the study duration, it would have added a great value to the study. Despite these limitations, our study helps in the awareness of avoiding the status quo using conventional treatments and accepting high-efficacy therapies that enhance patients’ quality of life.
In conclusion, our study found high rates of TI in gMG among the participating neurologists, mainly driven by resistance to change to the introduction of new targeted treatments. Being aware of these results might help to challenge the therapeutic status quo and highlight the importance of establishing specific medical educational interventions to achieve the best care for gMG patients.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261420993 - Supplemental material for Neurologists’ decision-making in the management of generalised myasthenia gravis: Therapeutic inertia and treatment choices
Supplemental material, sj-docx-1-jnd-10.1177_22143602261420993 for Neurologists’ decision-making in the management of generalised myasthenia gravis: Therapeutic inertia and treatment choices by Gerardo Gutiérrez-Gutiérrez, Rocío Gómez-Ballesteros, Adrián Ares, Ramón Villaverde, Virginia Reyes, Thaís Armangué, Paola Díaz-Abós, Pablo Rebollo, Neus Canal, Luis Querol, Jorge Maurino and Elena Cortés-Vicente in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
The authors are most grateful to the Spanish Society of Neurology (SEN) and to all participating neurologists for making the PROMPT-MG study possible.
ORCID iDs
CRediT authorship contribution statement
G Gutiérrez-Gutiérrez: Conceptualization, Writing - original draft, Writing - review & editing. R Gómez-Ballesteros: Conceptualization, Methodology, Formal Analysis, Writing - original draft, Writing - review & editing. A Ares: Conceptualization, Writing - review & editing. R Villaverde: Conceptualization, Writing - review & editing. V Reyes: Conceptualization, Writing - review & editing. T Armangué: Conceptualization, Writing - review & editing. P Díaz-Abós: Conceptualization, Writing - review & editing. P Rebollo: Conceptualization, Methodology, Formal Analysis, Writing - review & editing. N Canal: Formal Analysis, Writing - review & editing. J Maurino: Conceptualization, Methodology, Writing - original draft, Writing - review & editing. L Querol: Conceptualization, Writing - review & editing. E Cortés-Vicente: Conceptualization, Methodology, Writing - original draft, Writing - review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Roche Medical Department, Spain (SL45180). The funding source had no role in the design of the study, data analysis and interpretation, review and approval of the manuscript, or in the decision to submit for publication.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G Gutiérrez-Gutiérrez reports receiving consulting fees from CSL Behring, Biogen, Alter, Takeda, Akcea, Lupin Neuroscience, Roche, Alexion, and Argenx; congress support from Alter, Esteve, Sanofi-Genzyme, Pfizer, and UCB Pharma; scientific collaborations with Lilly, Alexion, Genzyme, Takeda, Biogen, Pfizer, and Alter; royalties from books published with Exeltis, Alter, Esteve, Andrómaco, and Bristol-Myers; and grants and awards from Lilly, UCB Pharma, and CSL Behring. A Ares reports receiving speaking honoraria, consultation fees, or travel support for congress and scientific meetings attendance from Almirall, Bayer, Biogen, BMS, Janssen, Merck, Novartis, Roche, Sanofi, and Teva. L Querol reports receiving speaker honoraria from Merck, Sanofi, Roche, Biogen, Grifols, and CSL Behring; providing expert testimony for Grifols, Johnson & Johnson, Annexon Pharmaceuticals, Sanofi, Novartis, Takeda, and CSL-Behring; and receiving research funds from Roche, UCB, and Grifols. E Cortés-Vicente reports consulting or advisory relationships with UCB Pharma SA, Janssen Pharmaceuticals Inc, Alexion Pharmaceuticals Inc, Argenx, and Lundbeck. P Rebollo and N Canal are employees of IQVIA Spain, the contract research organization that conducted this study for Roche. R Gómez-Ballesteros, P Díaz-Abós, and J Maurino are employees of Roche Farma Spain. R Villaverde, V Reyes, and T Armangué declare no conflicts of interest for this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.