
Abstract
Background:
Becker muscular dystrophy (BMD) is caused primarily by in-frame mutations in the DMD gene. Phenotype varies from asymptomatic to severe; manifestations may include muscle weakness, scoliosis, cardiac involvement, loss of ambulation, respiratory impairment, cognitive dysfunction, and premature death. This study aimed to characterize the frequency and age at occurrence of these milestones.
Methods:
A systematic literature review (SLR) was refreshed in 2022 using MEDLINE and EMBASE to identify articles describing the natural history of BMD. The proportion of patients experiencing clinical milestones was reported by ‘life-stage’ age groups (0–17; 18–40; 41+ years) using patient-level data from the general BMD population; age at each milestone's occurrence as mean (standard deviation [SD]).
Results:
From 4948 abstracts screened, 121 publications were included. Among 36 general BMD population studies, by age 41+ years (lifetime-risk proxy), 93.6% experienced muscle weakness; 69.4% cardiac involvement; 55.6% scoliosis; 47.4% loss of ambulation; and 33.3% ventilation. Decreased cognitive function or cognitive dysfunction were reported in 41% across all ages. Among those experiencing milestones (79 studies), mean (SD) age at symptom onset was 12.5 (9.7); muscle weakness, 19.9 (11.7); scoliosis, 24.9 (3.1); cardiac involvement, 31.9 (13.4); loss of ambulation, 33.3 (13.5); ventilation, 35.7 (12.2); and death at 55.6 (19.4) years. Data availability ranged from three to 1079 patients/outcome.
Conclusions:
This SLR highlights the variability in disease presentation in BMD. Stratifying BMD populations into phenotype groups based on the full spectrum of clinical manifestations may better capture disease progression and enhance comparability across studies.
Included clinical trials:
ClinicalTrials.gov NCT01070511 (https://clinicaltrials.gov/study/NCT01070511), ClinicalTrials.gov NCT02147639 (https://clinicaltrials.gov/study/NCT02147639?term=Becker%20Muscular%20Dystrophy&intr=Sodium%20Nitrate&rank=3), ClinicalTrials.gov NCT01350154 and EudraCT number: 2010–024659-10 (https://clinicaltrials.gov/study/NCT01350154?term=NCT01350154&rank=1; https://www.clinicaltrialsregister.eu/ctr-search/trial/2010-024659-10/results).
Keywords
Background
Mutations in the DMD gene are responsible for Becker muscular dystrophy (BMD) along with other interrelated allelic dystrophinopathies including Duchenne muscular dystrophy (DMD) and X-linked dilated cardiomyopathy (XLDCM). 1 The dystrophin protein, encoded by the DMD gene on the X chromosome, has functions in smooth and skeletal muscle and cognitive function. 2 The large size of the DMD gene (79 exons over 2.2 Mb of DNA) renders it prone to mutations (inherited or sporadic [de novo]), namely single or multiple exon deletions or duplications, and point mutations.3,4 Mutations are either in-frame or out-of-frame. 5 Out-of-frame mutations result in a malfunctioning, prematurely truncated protein.1,2 In the majority of cases, in-frame mutations preserve the reading frame, resulting in decreased levels of, or partially functional, truncated dystrophin protein. 2 This principle is referred to as the reading frame rule; however, exceptions have been documented. Specifically, some in-frame mutations can result in a severe DMD phenotype, whereas certain out-of-frame mutations may lead to a milder, BMD-like presentation. 6 Most cases of DMD are caused by out-of-frame mutations, while the majority of BMD cases are caused by in-frame mutations.2,7–9 Becker muscular dystrophy is considered a rare disease with a reported global prevalence estimated at 1.6 per 100,000 people.10,11
The clinical course of BMD is highly heterogenous, making disease trajectory difficult to predict due to variations in the age at disease onset and clinical presentation. 7 Clinical manifestations commonly include muscle weakness and cardiac dysfunction; however, loss of ambulation, loss of upper limb function, pulmonary decline, and premature death may also occur.12–14 Cognitive disability may also be present yet is considered non-progressive. 15 More severe symptoms typically manifest in male patients, while female carriers may exhibit relatively mild skeletal muscle weakness and dilated cardiomyopathy. 6
Among allelic dystrophinopathies, DMD, the most severe of the diseases, typically presents with weakness beginning in early childhood; without treatment, affected individuals are usually wheelchair bound by age 12 and often die from cardiac or respiratory complications in their early twenties. 16 Another of the dystrophinopathies, XLDCM, primarily affects the heart, causing severe cardiac involvement with minimal skeletal muscle symptoms and often leading to heart failure in adolescence. 17 In contrast, BMD generally has a later onset and slower progression than DMD, though severity can range from asymptomatic to severe and cardiac involvement or cardiomyopathy may occur at any age or not at all.7,13,18–21
Diagnostic criteria for classification of dystrophinopathies are based on clinical assessment, laboratory tests (e.g., creatine kinase levels), genetic testing, and cardiac assessment.20,21 Treatment of BMD varies on a case-by-case basis, and may include physiotherapy, and for more severe cases corticosteroids (e.g., prednisone, deflazacort), assisted (noninvasive) or invasive ventilation, cardiac medications (e.g., angiotensin-converting enzyme [ACE] inhibitors, beta blockers), and cardiac transplant.22,23 While physicians are likely to develop a treatment and care strategy based on phenotype (e.g., a patient with a mild out-of-frame DMD mutation [i.e., mild DMD] may not receive corticosteroids while a patient with a severe, in-frame DMD mutation [i.e., severe BMD] may), mutation-specific therapies require an accurate genetic diagnosis.22,24–26
Estimates of the timing of key clinical events characterizing the natural history of BMD are variable. This is the first comprehensive synthesis of literature describing the natural history of BMD and was performed to provide a clearer understanding of how BMD progresses over time, particularly regarding key clinical events such as the onset of symptoms, disease progression, and variability in patient outcomes.
Methods
Search strategy and study selection
A systematic search of the literature was initially conducted on August 12th, 2019, and refreshed on April 13th, 2022, using MEDLINE/MEDLINE In-Process and EMBASE to identify articles describing the natural history of BMD. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines for designing, performing, and reporting the systematic literature review (SLR), and the Guidance for the production and publication of Cochrane systematic review, were followed.27,28 The search strategy (Supplementary Table S1) was guided by the PECOS (Population, Exposures, Comparators, Outcomes, Study design) criteria (Table 1). English language publications reporting natural history milestones in patients with BMD from the year 2000 onwards were included. No limitation was placed on study design.
PECOS criteria to outline the scope of the SLR.
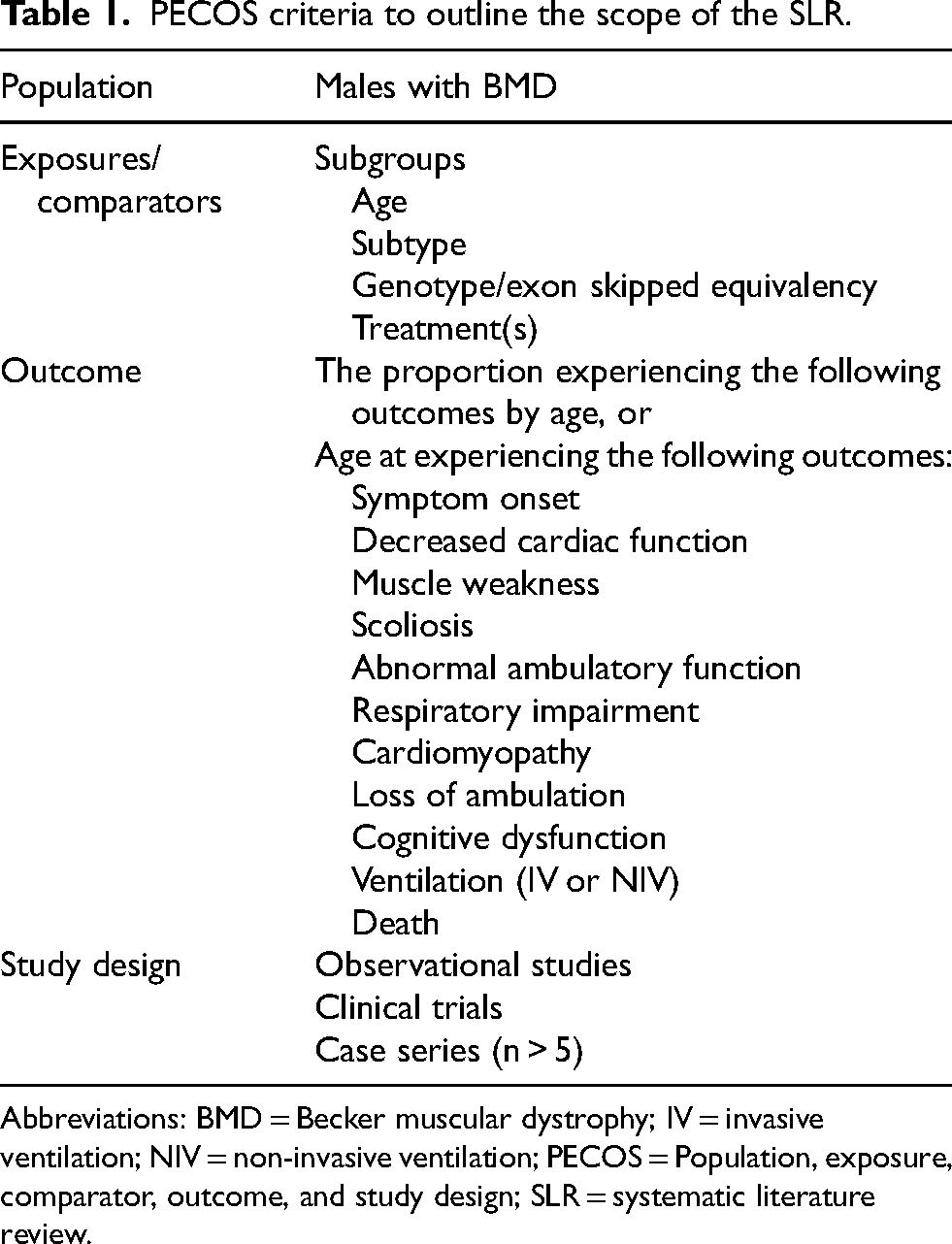
Abbreviations: BMD = Becker muscular dystrophy; IV = invasive ventilation; NIV = non-invasive ventilation; PECOS = Population, exposure, comparator, outcome, and study design; SLR = systematic literature review.
Studies including general BMD populations (i.e., not restricted by clinical or genetic characteristics, such as those enrolled consecutively from neuromuscular clinics) as well as specialized subpopulations of BMD (e.g., restricted by specific clinical features or genetic mutations) were included. Data from clinical trial populations were included in the review, however, these samples were considered specialized subpopulations and only baseline (pretreatment) data were included in analyses.
Natural history milestones of interest included any type of information related to symptom onset, muscle weakness, loss of ambulation, cardiac involvement, pulmonary dysfunction, need for ventilation (noninvasive ventilation [NIH], invasive ventilation [IV], or unspecified), cognitive dysfunction, scoliosis, and death. For natural history milestones, events such as advanced cardiac involvement (i.e., cardiomyopathy) or cognitive dysfunction were considered to have occurred based on the criteria or cutoffs reported by the original authors or investigators; however, these definitions varied across the included publications. Mapping of the specific definitions used in the original studies to the milestone terminology used in this review (symptom onset, muscle weakness/function, cognitive disfunction, cardiac involvement, ambulation status, respiratory involvement, scoliosis, and mortality) can be found in Supplementary Table S2.
Studies were initially included per PECOS criteria if they involved BMD populations and reported age at event or proportion experiencing relevant outcomes by age, regardless of study design. However, only a subset could be used in the final analysis. For example, studies focusing on specialized BMD subpopulations (such as those requiring cardiac involvement for study inclusion) were excluded from the
Two reviewers independently screened abstracts and full-text articles for inclusion; discrepancies were resolved through discussion to achieve consensus.
Data extraction
Data were extracted and quality checked by two researchers. Study characteristics extracted included primary author, year, study design, country/countries, single or multicenter, study focus, data source, study duration and period, objective(s), inclusion and exclusion criteria, study conclusions, and real-world representativeness and/or criteria for non-representativeness. Both grouped data and individual patient data (IPD) for patient characteristics and natural history milestones were extracted from studies depending on how the data were presented by investigators. For continuous variables (e.g., baseline age), the mean (or IPD), median, standard deviation (SD), interquartile range (IQR), and range were extracted when available. For categorical variables (e.g., ambulant, not ambulant), the number of patients, age of patient(s), and proportion in each group were extracted. If only IPD were reported, summary statistics (mean [SD]) were calculated. All post-extraction calculations were noted. Publications that grouped patients into phenotypic categories of any type were noted.
Patient characteristics extracted included baseline demographics, and any details provided regarding gene mutation/genotype, inheritance pattern (familial versus sporadic), and treatment history (corticosteroid, cardiac, or other). Natural history milestones data were extracted in two ways; the proportion of patients experiencing natural history milestones by age group and the age at experiencing natural history milestones for the subgroup who experienced the milestone. For each patient, or group of patients, the definition used by the source publication study investigators for each natural history milestone was recorded. These natural history definitions were standardized into key clinical outcomes through discussion between both extractors to achieve consensus. Extracted data were stored in Excel; visualizations were developed using R.
Due to the limited number of people with BMD, patient overlap between research papers is common. Studies with potentially overlapping patients or patient groups were identified using several indicators (e.g., geographic region, country, registry/data source, sample size, and author names). Where population overlap was identified, data describing each outcome of interest were included from one publication only, depending on which had the most recent (i.e., latest) timepoint for analyses relating to the proportion experiencing outcomes, or the greater sample size for analyses relating to age at experiencing outcomes.
Analysis & synthesis
Natural history milestones are progressive clinical manifestations of BMD that patients may experience (e.g., loss of ambulation). Definitions of these milestones as reported in each publication were recorded (Supplementary Table 2) and were considered either transitional (e.g.,
To estimate the proportion of those with BMD who experience each natural history milestone of interest by life-stage age group, data were included only from studies reporting on general BMD populations. In studies with results reported by strata; such stratified analyses were included provided they collectively described the full sample. For these analyses, data were extracted from tables/statements such as “The patient was ambulating independently at age 22” (IPD), or “Among a group of 56 patients with BMD with mean (SD) age of 33.2 (4.7), 22 had lost ambulation” (grouped), only overall data were extracted (i.e., studies not reporting overall data were excluded).
Age categories were selected to represent
Grouped data, as presented in the literature, were organized by ascending central age (i.e., mean, median, mid-point between minimum and maximum) then presented graphically.
The mean (SD) age at experiencing outcomes were estimated as a weighted average from IPD and grouped data from patients. Means for combined groups were calculated as the weighted average of the individual group means, with weights proportional to group sample sizes. The standard deviations for combined groups were calculated using the unbiased estimator that combines within-sample variances and adjusts for differences in sample means. Specifically, the combined sample variance is obtained by decomposing total sum of squares across groups, accounting for both intra-group variability and inter-group mean differences. For these outcomes, data were included from both general BMD population and BMD subpopulation studies. Age at experiencing outcomes data were extracted from information such as “The patient lost ambulation at age 15”, or “The mean (SD) age at loss of ambulation for the group of nine patients with BMD who lost ambulation was 30.2 (9.3) years”. Results were visually compared with similar data for DMD to illustrate the marked difference in age at occurrence and variability for BMD.
Sensitivity analyses and study quality assessment
The overarching approach taken in estimation, was that estimating the proportion of overall patients with BMD experiencing an event required a representative sample, while estimating the average age at which an event occurred (for the subset in whom the event was experienced) allowed for relaxing this assumption of a representative sample to all patients for whom details of age at event were available (including the consideration of BMD subpopulation samples where available). For example, if a study only included patients who had lost ambulation, their age at loss of ambulation could be included in the mean age at loss of ambulation analysis. However, these patients would not be included in the proportion experiencing loss of ambulation analysis due to being from a specialized subpopulation of BMD, thus non-representative, population.
Classifying data as such required a number of assumptions and the following were explored in a number of sensitivity analyses: (1) only including representative studies in the “age-at” analysis in addition to the similar restriction made for the “proportion with” analysis; (2) studies with mutation-specific inclusion/exclusion criteria were classified as
The strength of the available evidence was assessed using the STrengthening the Reporting of Observational studies in Epidemiology (STROBE) Statement for observational studies, 29 the CARE (CAse REport) guidelines for case reports, 30 and the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2). 31
Results
Systematic literature review
A total of 4948 potentially relevant records were identified (3915 from the initial search conducted in 2019; 1033 during the 2022 update; Figure 1). Four thousand ninety-three publications were excluded during abstract review, and 734 during full text review, resulting in 121 eligible to summarize the natural history of BMD (Figure 1).
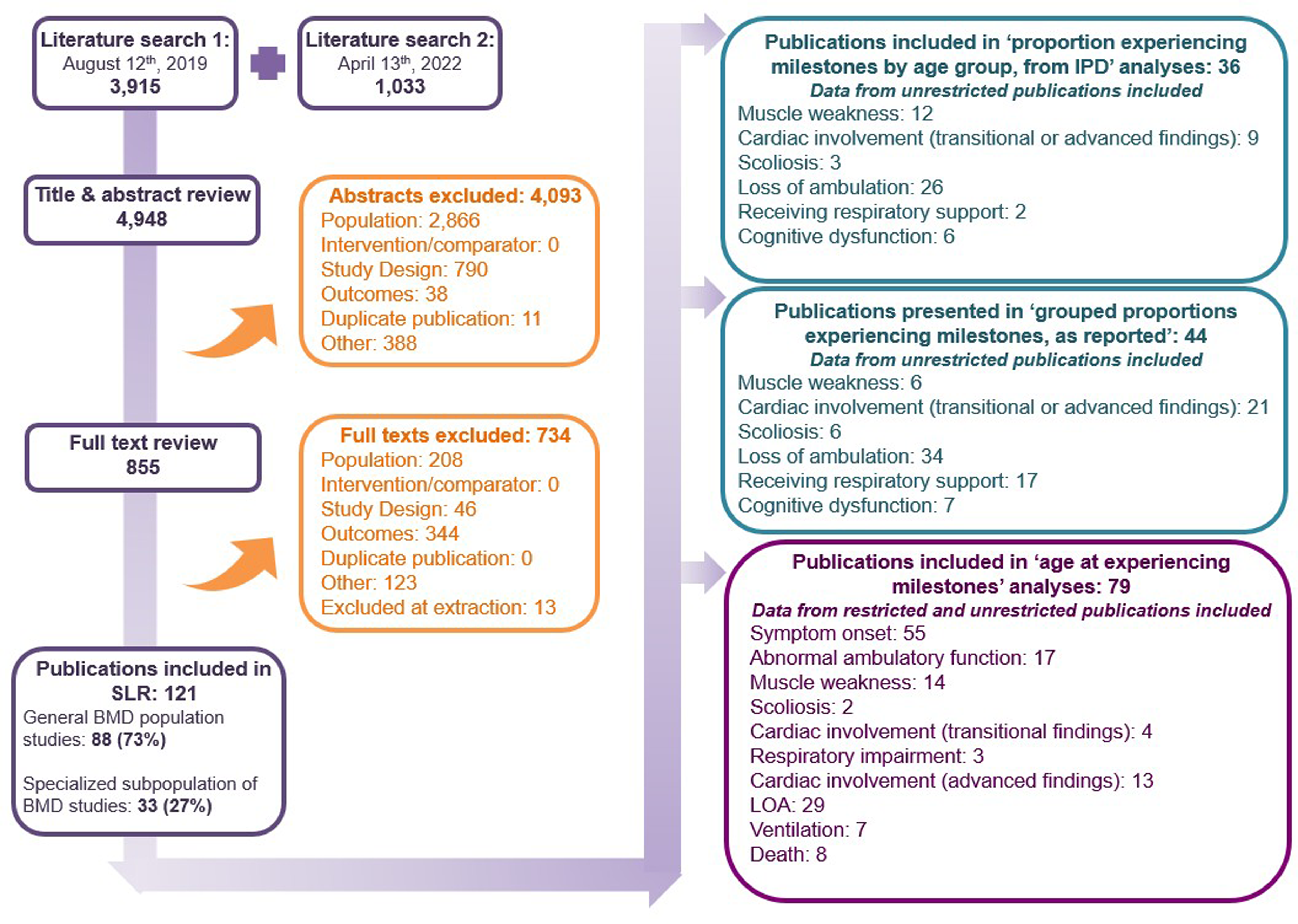
PRISMA study flow diagram.
Of the 121 publications included in the review, 88 (73%) were reported on a general BMD population,5,15,32–117 or representative of the real-world BMD population, and 33 (27%) were reporting on a specialized subpopulation of BMD (Figure 1; Supplementary Table S3).8,9,118–148 Most publications comprised patients with BMD from Europe (n = 57; 47%),8,9,15,32,34,37,39,40,45–47,49,52–54,56,61,62,64,65,74,76–78,81,84,89,92,96,99,101–104,107–109,112,114,117,118,122,123,126,127,129,130,138–141,143–148 Asia (n = 31; 26%),35,41,43,67,68,71–73,79,83,85–88,90,91,93–95,97,105,110,111,113,116,121,133–136,142 and North America (n = 15; 12%).5,33,38,42,44,59,63,70,80,100,120,124,131,132,137 Studies also examined BMD samples from South America (n = 6; 5%),48,55,57,98,119,128 the Middle East (n = 5; 4%),36,66,69,75,82 and Africa (n = 4; 3%).50,51,58,60 Two studies (2%) were comprised of individuals with BMD from multiple geographic regions.115,125 Most publications were observational in nature (n = 116; 96%) comprising cross-sectional, prospective, and retrospective cohort studies, and case series5,8,9,15,32–131,134–136,138,140–147; and five were interventional clinical trials (4%).132,133,137,139,148 Three abstracts were included. Sample sizes (exclusive to BMD) ranged from n = 173,81,93,122,139 to n = 251. 9 Study and patient characteristics are available in the supplementary materials (Supplementary Table S3).
A total of 2988 patients with BMD were included, ranging in age from ‘at birth’ to 88 years.59,135 Information on corticosteroid use (current or prior) was available for 29% of included individuals.5,32,33,36,41,43,44,56,59,60,65,70,72,76,77,98,99,107,110,113,118,132,137,142 Among this 29%, 2% reported corticosteroid use,59,77,118,137,142 78% were grouped data reported as ‘mixed’ with respect to corticosteroid use (i.e., within a group, some individuals had current or prior corticosteroid use while others did not, but individual-level data were unavailable),5,33,36,41,43,44,56,70,72,76,99,110,132 and 20% reported no current or prior corticosteroid use.32,41,44,56,60,65–67,70,77,85,98,99,107,110,113,132 Information on corticosteroid use was not available for the remaining 71% of included individuals.8,9,15,34,35,37–40,42,45–55,57–59,61,63,64,68,71,73–75,78–84,86,89,90,92–97,100–103,105,111,112,114,115,117,119–128,130,133–135,137–141,144–148
Proportion experiencing natural history milestones by life stage age group from individual patient data
Data describing the proportion of individual patients with BMD experiencing outcomes by ‘life-stage’ age groups were identified from 36 publications, all of which were characterized as reporting on a general BMD population.15,34,37,39,40,47,49–53,55–57,59,67,71,75,77,78,81,84,90,91,93,96,98,102–105,112,114–117 These data varied by outcome (Table 2; Figure 2), with the most frequently-observed milestone being muscle weakness, followed by cardiac involvement (transitional or advanced findings), scoliosis (at least mild), loss of ambulation, and finally, receiving respiratory support or ventilation.

Proportion of patients with BMD experiencing outcomes by ‘life-stage’ age groups from IPD (general BMD population studies). Abbreviations: BMD = Becker muscular dystrophy; IPD = individual patient data. Notes: * Respiratory support and ventilator use; †Cognitive disability is presumed to remain stable throughout the course of BMD; therefore, data where patient age was not provided were included, and progression over ‘life-stage’ age groups was not considered.
Proportion of BMD patients experiencing milestones by ‘life-stage’ age groups from IPD from general BMD population studies.
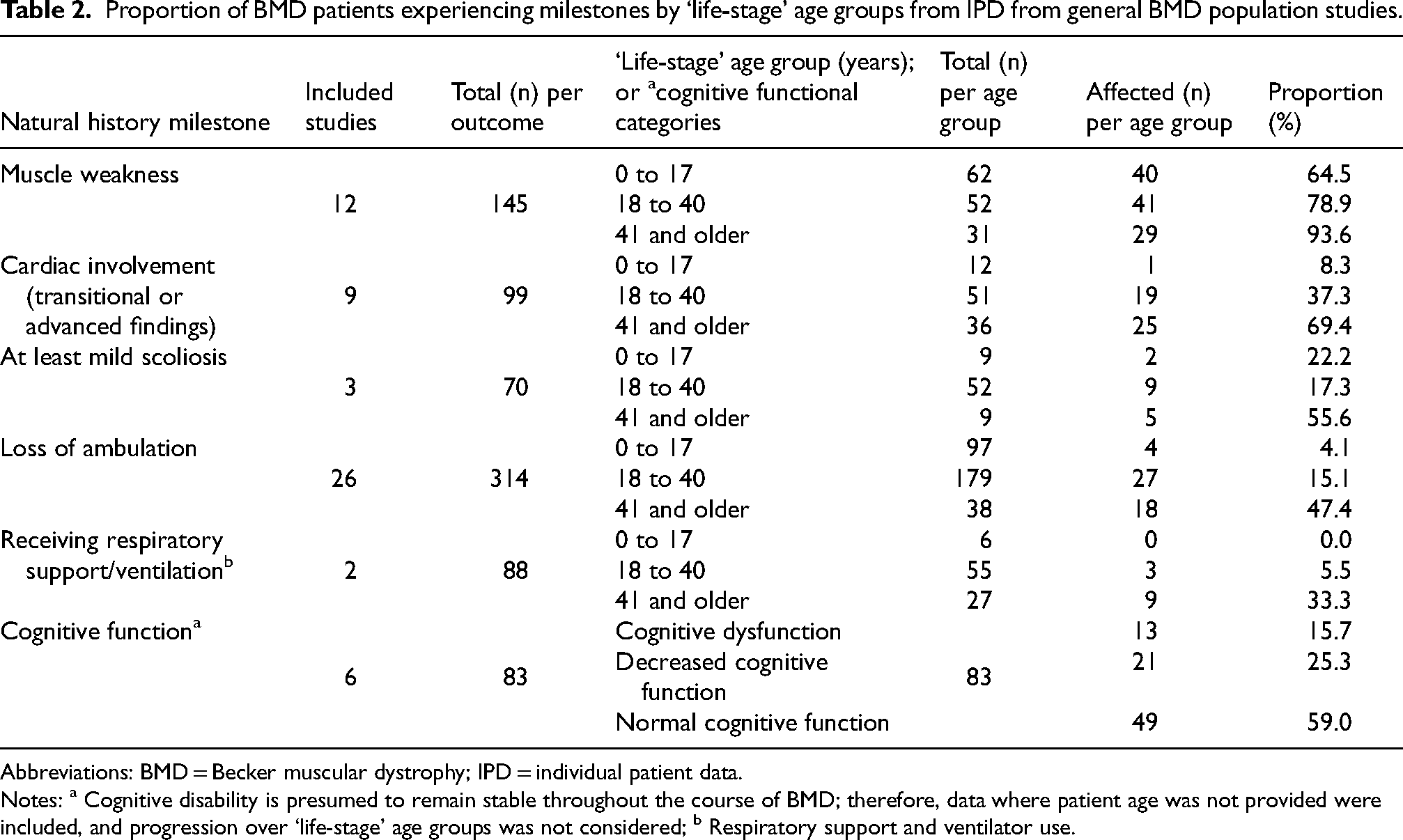
Abbreviations: BMD = Becker muscular dystrophy; IPD = individual patient data.
Notes: a Cognitive disability is presumed to remain stable throughout the course of BMD; therefore, data where patient age was not provided were included, and progression over ‘life-stage’ age groups was not considered; b Respiratory support and ventilator use.
Individual patient data describing the occurrence of muscle weakness were aggregated from 12 studies.47,49,51,59,77,78,90,98,102,104,112,115 Muscle weakness was observed in 64.5% of patients from birth to 17 years of age (n = 62), 78.9% of those aged 18 to 40 years (n = 52), and 93.6% of those aged 41 years and older (n = 31). The second most observed milestone was cardiac involvement (transitional or advanced; nine publications),49,52,53,77,78,98,114,116,117 with 69.4% of those aged 41 years and older (n = 36) experiencing some form of cardiac involvement. Three publications reported on scoliosis, with the majority of data within the 18 to 40 year age group (n = 52), of which 17.3% had at least mild scoliosis.81,116,117 The most frequently reported IPD milestone, ambulatory status, was described in 26 publications,37,39,40,47,50,51,53,56,57,67,71,75,84,90,91,93,96,98,102–105,112,115–117 with loss of ambulation reported in 4.1% of patients from birth to 17 years of age (n = 97), 15.1% of those aged 18 to 40 years (n = 179), and 47.4% of those aged 41 years and older (n = 38). The proportion of those receiving respiratory support or ventilation (two publications),49,116 among those aged 0 to 17 years was 0% (n = 6), 18 to 40 years, 5.5% (n = 55), and 41+ years, 33.3% (n = 27).
Cognitive function was grouped by functional status, rather than age. Among the 83 patients with BMD for whom data were available from six publications,15,34,55,56,96,115 13 (15.7%) had cognitive dysfunction, 21 (25.3%) had decreased cognitive function, and 49 (59.0%) had normal cognitive function.
Proportion experiencing natural history milestones by life stage age group – grouped data as reported
Aggregate data on the proportion of people with BMD experiencing natural history milestones by age were reported in 44 publications with general BMD study populations and are summarized in Figure 3(a) (muscle weakness, cardiac involvement (transitional or advanced findings), at least mild scoliosis, loss of ambulation, and receiving respiratory support/ventilation) and Figure 3(b) (cognitive function).5,32,34,36,37,41,43–46,54–58,61,62,64–66,68–72,76,79,80,85,86,88,89–92,94,95,97,99–101,106–113,127
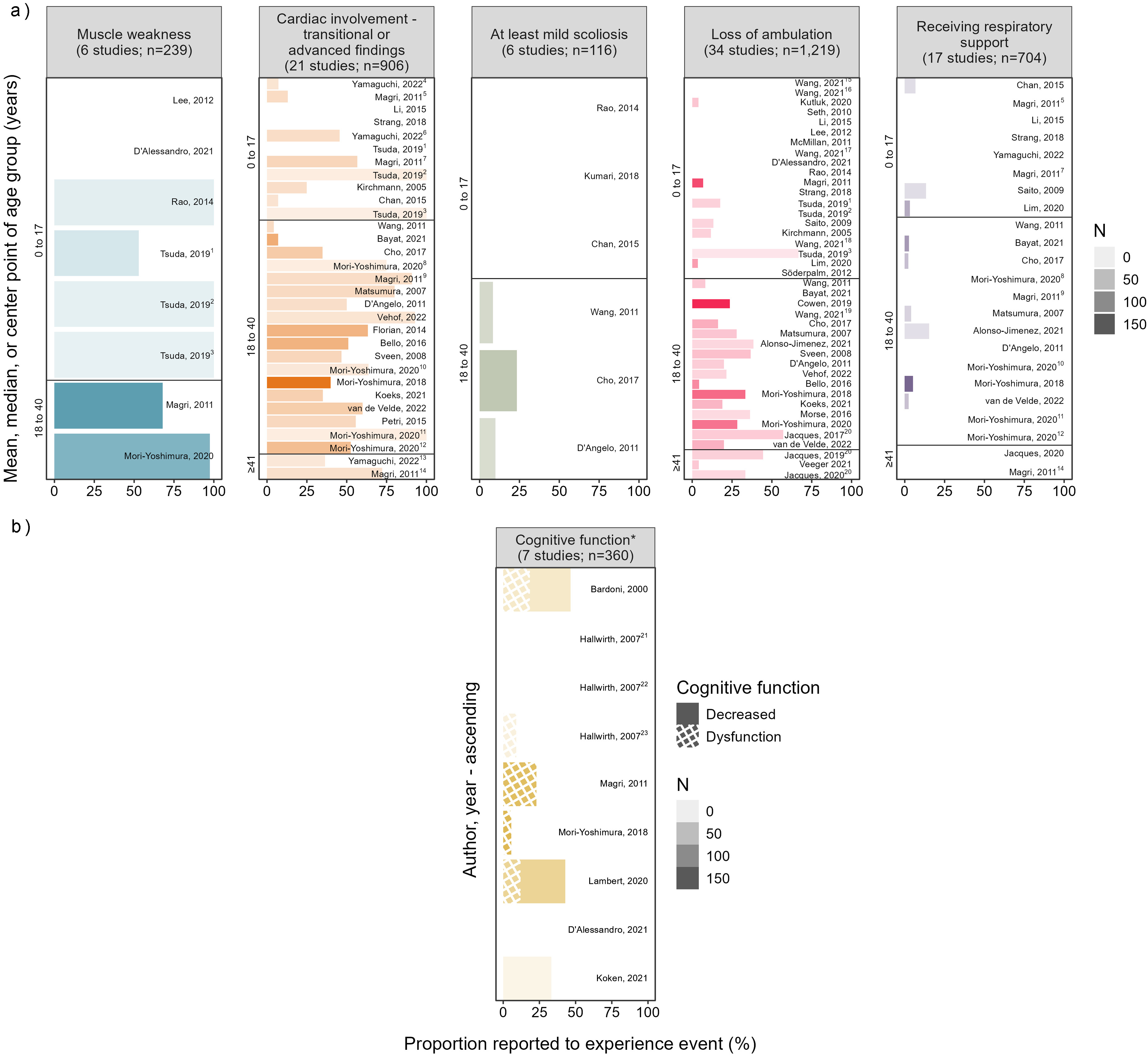
Patients with BMD experiencing (a) outcomes and (b) cognitive dysfunction from the literature, (general BMD population studies). Note 3a: horizontal bars, labeled with the primary author and year of publication, are ordered by ascending central tendency of age (mean, median, center of range), the length of the ‘branch’ depicts the proportion experiencing the event of interest, and the thickness visually represents the sample size (see legend). Subgroups 3a: 1Latent left ventricular dysfunction; 2Chronic persistent left ventricular dysfunction; 3Acute progressive left ventricular dysfunction; 4Age 1 to ≤10; 5Age 1 to 10; 6Age 10 to ≤18; 7Age 11 to 20; 8Duplication; 9Age 21 to 35; 10No deletion/duplication; 11Micromutation; 12Deletion; 13Age >18; 14Age ≥35; 15Age 0 to 4; 16Age 5 to 9; 17Age 10 to 14; 18Age 15 to 19; 19Age 20 to 25; 20Included overlapping populations to show change over time for the purpose of this analysis. Note 3b: horizontal bars, labeled with the primary author and year of publication, are ordered by ascending central tendency of age (mean, median, center of range), the length of the ‘branch’ depicts the proportion experiencing the event of interest, and the thickness visually represents the sample size (see legend). Subgroups 3b:21White patients; 22Indian patients; 23Black patients.
Age at experiencing natural history milestones
Seventy-nine publications reported data used to estimate the mean (SD) age that natural history milestones were experienced (Table 3).8,9,15,33,35,37,38,42,43,45–51,53,56,57,59,60,63,64,66,71,73–76,82,83,85–88,90–94,96,98,101,103–111,115,116,118–126,128–148
Mean age at experiencing outcomes among those who have experienced them.
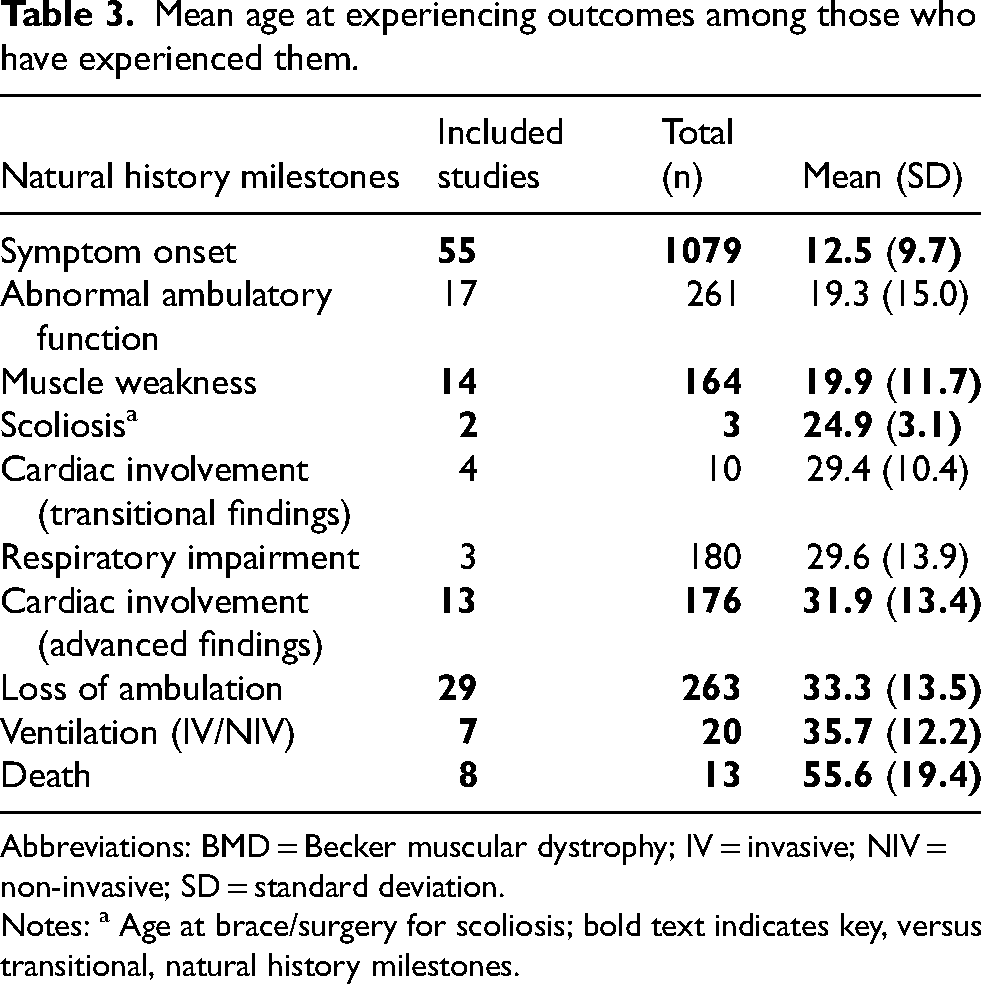
Abbreviations: BMD = Becker muscular dystrophy; IV = invasive; NIV = non-invasive; SD = standard deviation.
Notes: a Age at brace/surgery for scoliosis; bold text indicates key, versus transitional, natural history milestones.
Of the key natural history milestones (i.e., non-transitional), the mean (SD) age at symptom onset was 12.5 (9.7) years (55 publications; n = 1079). 55 Next were age at experiencing muscle weakness, 19.9 (11.7) years (14 publications; n = 164),38,45,49,51,59,74,76,83,96,98,125,130,140,143 scoliosis, 24.9 (3.1) years (two publications; n = 3),43,136 cardiac involvement (advanced findings), 31.9 (13.4) years (13 publications; n = 176),9,33,49,63,64,76,92,116,118,120,130,136,146 loss of ambulation, 33.3 (13.5) years (29 publications; n = 263),9,33,37,43,47,57,59,64,76,85,88,91,101,104,115,116,119,121,124,125–131,135,136,138,144,146,147 and ventilation (noninvasive ventilation [NIV], IV, or simply ventilation or mechanical ventilation [NIV or IV not specified]), 35.7 (12.2) years (seven publications; n = 20).43,49,116,122,136,139,146 The mean age at death from any cause was estimated from eight publications at 55.6 (19.4) years (n = 13).8,49,50,53,92,123,135,146 Among the 13 patients for whom age at death was reported, nine deaths were cardiovascular-related (seven cardiac related, two stroke), three were from unknown or unreported causes, and one was from gall bladder cancer.
Age at transitional outcomes included abnormal ambulatory function (indicative of transitioning to loss of ambulation), decreased cardiac function (transitional findings), and respiratory impairment (transitional to requiring ventilation), are also reported in Table 3. Abnormal ambulatory function occurred earliest at a mean (SD) age of 19.3 (15.0) years (17 publications; n = 261),8,49,51,74,76,86,96,104,124,125,130,132,135,136,142,143,147 followed by decreased cardiac function (transitional findings) 29.4 (10.4) years (four publications; n = 10),42,49,133,146 and respiratory impairment 29.6 (13.9) years (three publications; n = 180).76,88,136
Original definitions as provided by each publication, before categorization into the above groups, are available in the supplementary materials (Supplementary Table S2).
Comparison to DMD
The age at occurrence of natural history milestones were graphically compared to published DMD values (Figure 4) to contextualize results76,149–153; transitional, early-stage milestones were not included due to lack of comparison values available.
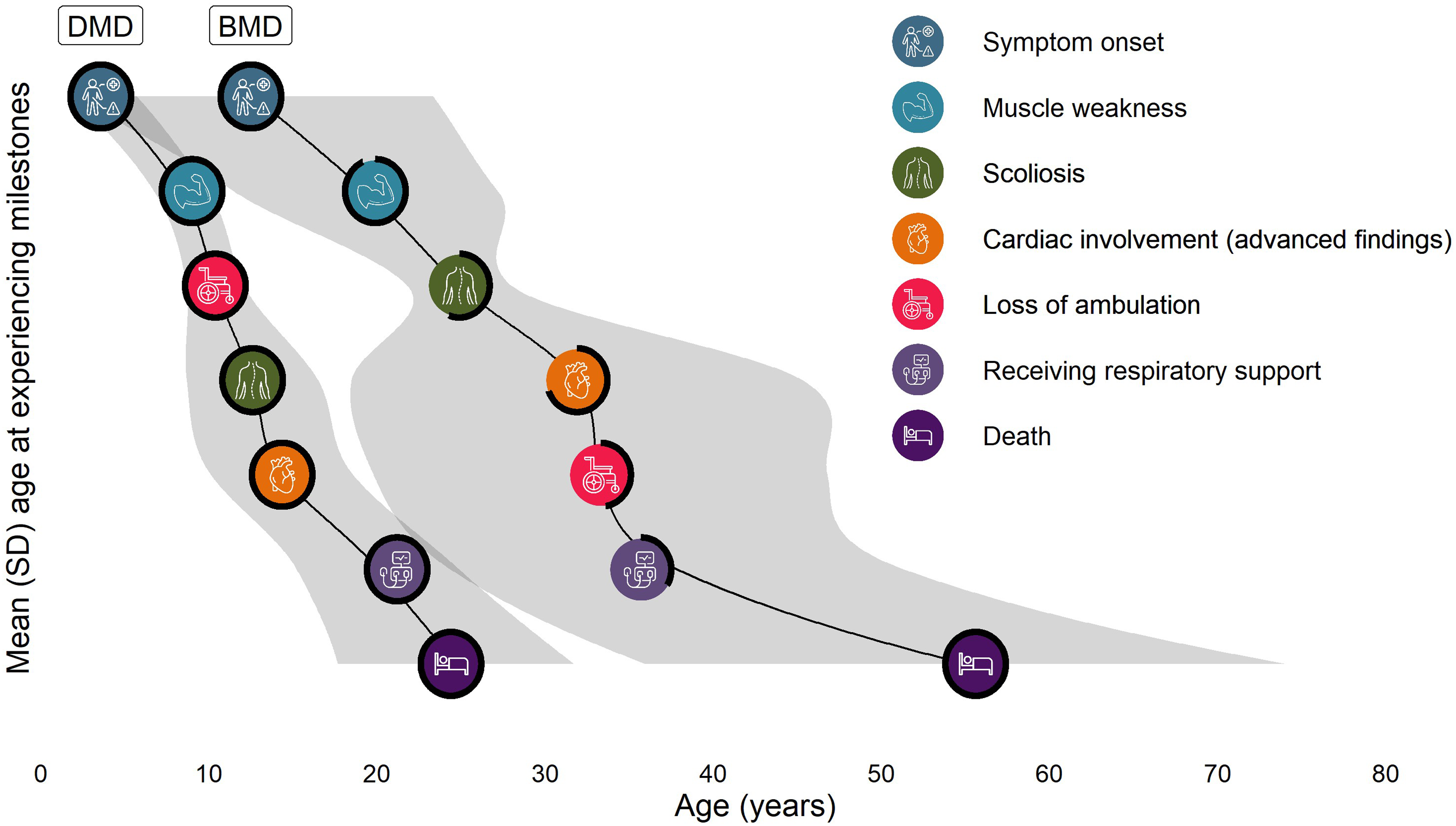
Mean (SD) age at natural history milestones among patients with BMD*; DMD values for comparison. *Among patients who experienced the event from IPD and grouped data. Abbreviations: BMD = Becker muscular dystrophy; DMD = Duchenne muscular dystrophy; IPD = individual patient data; SD = standard deviation. Notes: *Ventilation included both invasive and noninvasive types; DMD estimates sourced from the following: Magri et al., 2011 76 ; Singh et al., 2018 149 ; Posner et al., 2016 150 ; Barber et al., 2013 151 ; Bach et al., 2015 152 ; Wahlgren et al., 2022. 153 .
Sensitivity analyses
Results from four sensitivity analyses conducted for the age at event estimates are reported in Table 4. In the first sensitivity analyses, data from general BMD population studies only were included; results are similar across milestones with the greatest differences (noting those with mean absolute change ≥3 years) in mean (SD; n) age at death, from 55.6 (19.4; 13) to 48.4 (18.6; 7) years (four fewer studies),8,123,135,146 scoliosis, from 24.9 (3.1; 3) to 21.8 (n = 1) years (one fewer study included), 136 decreased cardiac function (transitional findings) from 29.4 (10.4; 10) to 32.5 (14.6; 4) years (two less studies),133,146 and loss of ambulation from 33.3 (13.5; 263) to 30.2 (11.0; 174) years (14 fewer studies),9,119,121,124,125,129–131,135,136,138,144,146,147 In the second sensitivity analysis, studies restricted based on genetic criteria only were categorized as general BMD population studies rather than specialized subpopulations of BMD. The most notable difference was that age at ventilation increased from 35.7 (12.2; 20) to 39.0 years (11.0; 14) years (three fewer studies).122,136,139 For the third sensitivity analysis, information on age at cardiac event (e.g., cardiac device implanted) was added; however, estimates of age at transitional and advanced cardiac involvement were not strongly impacted. Finally, for the fourth sensitivity analysis, including data on the age that cardiac medication was initiated as a proxy for transitional cardiac involvement decreased the estimate from 29.4 (10.4; 10) to 23.1 (8.9; 32; three additional studies).43,63,64
Sensitivity analyses.
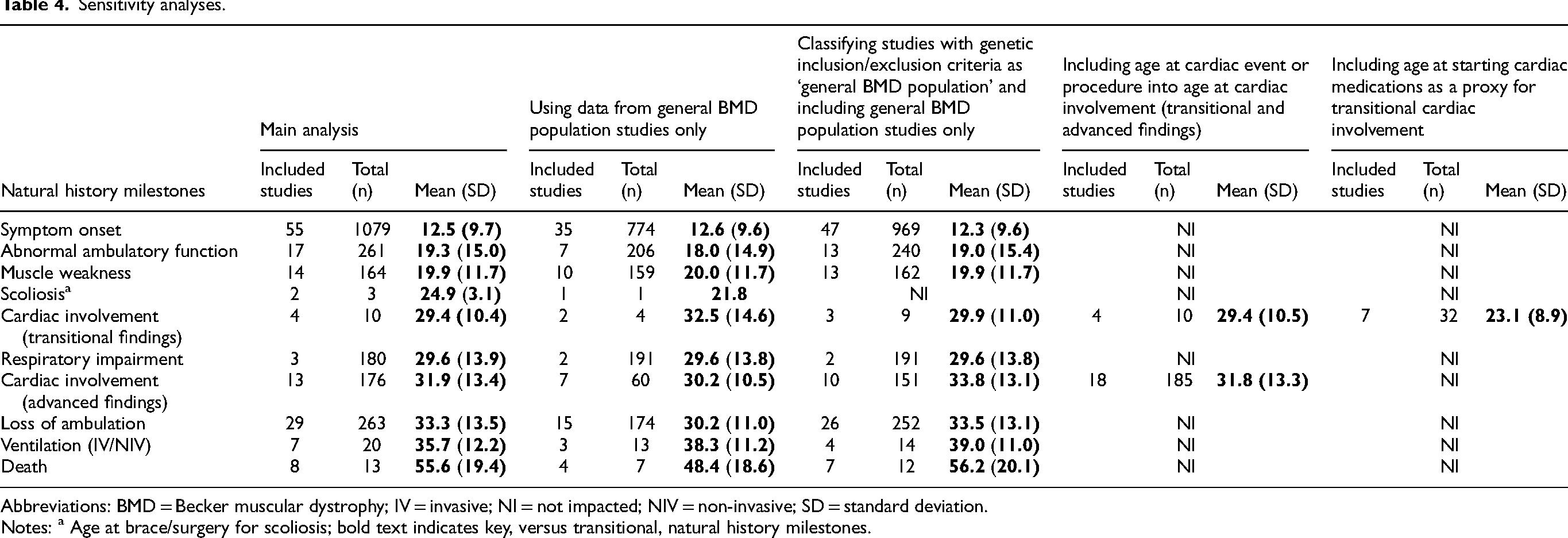
Abbreviations: BMD = Becker muscular dystrophy; IV = invasive; NI = not impacted; NIV = non-invasive; SD = standard deviation.
Notes: a Age at brace/surgery for scoliosis; bold text indicates key, versus transitional, natural history milestones.
Quality assessment
Results of the quality assessments conducted on 118 of 121 included publications (three abstracts were not assessed for reporting quality) are available in the supplementary materials (Supplementary Table S4).
Discussion
This SLR was conducted to address the lack of a synthesis of published data on the frequency and timing of key natural history milestones in BMD. This review presents findings on outcome measures for which sufficient data are currently available, allowing for trends to be meaningfully identified.
In this review, extensive variability was identified in both the timing of key clinical milestones and in the proportion of patients who experienced the events. Due to the nature of the available data, the mean age at event occurrence could only be calculated among individuals who had experienced the event, unlike in traditional time-to-event analyses, which include both those who have and have not experienced the event and typically report a median age at event. As a result, the reported estimates are younger than those that would have been observed in conventional survival analysis. While the onset of symptoms typically occurred during early adolescence, there was substantial variation in the ages at which patients experienced other clinical outcomes including muscle weakness, scoliosis, cardiac involvement, loss of ambulation, ventilation, and death, if these events occurred at all.
When comparing these results to the literature, there is some redundancy because the referenced literature is included in the SLR. Apart from a few large dystrophinopathic cohorts with extended follow up, most data contributing to this SLR were smaller database and clinical studies.
When the results of individual studies were contextualized within the broader findings of the review, they were generally consistent with the synthesized conclusions. However, a few points warrant further discussion (note that the proportion of data from a contributing study included in this analysis for each outcome will be herein termed ‘contribution’). Data from one large cohort (n = 115; Magri et al., 2011) with extended follow-up (mean [SD] follow-up of 10.3 (8.8) years) were included in several analyses presented, with findings similar to the overall synthesis. 76 The mean (SD) age at disease onset as reported by Magri et al. was 12.9 (11.8) years (contributing 11% to this analysis), with only eight of the 115 patients losing ambulation during follow-up. The authors also noted that muscle involvement was unpredictable, with onset ranging from six to 50 years old (mean, 19.2 years) and 68% of patients developing symptoms over follow-up (contributing 70%). The age of cardiac involvement was 28.7 (7.1) years (n = 24; contributing 14%) with 26% developing severe cardiac impairment over follow-up. Loss of ambulation was observed at a mean age of 31.7 (10.7) years (contributing 3%). Finally, the age at respiratory involvement was 28.6 (11.7) years (contributing 25%), and among those older than age 35, 28% showed respiratory involvement and none required ventilation. 76
Clemens et al. 2020 used data from the Cooperative International Neuromuscular Research Group (CINRG) to report the proportion of those losing ambulation among 83 patients with BMD, applying similar reference age categories to those used in this study. 7 Among those aged 0 to 20 years, none of 36 BMD patients had lost ambulation (0%), aged 20 to <40 years, four of 23 (17%) had lost ambulation, and aged ≥40 years, 11 of 24 (46%) were non-ambulant. 7 This study's inclusion criteria restricted by genotype; thus, the data are not included in the proportion experiencing loss of ambulation analyses; however, the findings align well.
Bello et al.'s 2016 publication followed 69 patients with BMD referred to the Neurology Clinic at the University of Padova for one year. 37 The proportion of those with cardiomyopathy between the ages of six and 69 years (mean age, 33.2 years) was reported to be 51%; three were wheelchair bound at baseline (4.6%), and two additional patients lost ambulation over the year, for a total of 7.2%. 37 These data are reported grouped and reported as presented, therefore do not contribute to the analyses.
Aggregate data on the proportion of people with BMD experiencing natural history milestones by age were shown as reported in the literature. The data generally align with what was observed in the IPD analyses, with muscle weakness and cardiac involvement occurring most frequently, and from a younger age. The frequency of receiving respiratory support and the occurrence of scoliosis among those with BMD were similar to the younger ‘life-stage’ age groups in the IPD analyses yet did not reach 50% at age 41+ and over which is not surprising given the available IPD data were so few. Loss of ambulation was estimated to occur in up to 67% of patients, somewhat higher than what was observed with the IPD analysis (47%). Alignment between the two sets of data was dependent on the amount of data available for comparison in either the IPD analyses or grouped data.
Andrews et al., 2022 published a summary of 12 patients with BMD from the Center for Disease Control and Prevention (CDC) Muscular Dystrophy Surveillance, Tracking, and Research Network, known as MD STARnet. 33 The reported mean age of symptom onset 14.5 years (contributing 1%), age at cardiomyopathy, 18.0 years (contributing 3%) and loss of ambulation was 22.0 years (contributing 5%).
A few key papers on the natural history of BMD have been published since executing this review; their findings are largely in line with those of this synthesis. They include three-year follow-up data on the CINRG cohort previously described by Clemens et al. in 2020,7,154 two natural history studies from Japan (Nakamura et al.),155,156 and a retrospective Italian study (Gorgoglione et al.). 157 The Nakamura et al. studies included overlapping BMD cohorts with an in-frame mutations and pathogenic microvariants (n = 274) that were all ambulatory after the age of 16,155,156 while the Italian study included 943 patients diagnosed with BMD based on a combination of clinical, biochemical and genetic criteria. 157 The age at key clinical milestones described by Nakamura et al. in their cohorts (e.g., mean age at experiencing loss of ambulation and ventilation) are similar and align well with the findings of this study. Gorgoglione et al. describe an older (median) age at loss of ambulation, which is as expected as their analysis included those who did, and did not, lose ambulation, rather than estimating the mean age from those who did, as in this analysis. Their conclusions on the clinical heterogeneity in timing of loss of ambulation and cardiac involvement align with the general findings of the present study.
The Nakamura and Gorgoglione papers are interesting for their focus on patients with a genetic diagnosis.155–157 There is evidence that mutation location (e.g., by domain) can impact phenotype and being able to provide stratification by genotype in the present synthesis may have been insightful. However, with the present dataset, available information was a limitation as genetic mutation data were reported for fewer than one-third of the subjects included in this SLR (30%). Among those, genotype data were often presented for groups of subjects in ways that did not facilitate further analyses (e.g., a cohort was described as having 70% deletions, 10% duplications, and 20% small mutations, but milestone data were reported for the cohort as a whole). As more genetic data are published in the future, a synthesis focusing on genotype specific analyses will be valuable.
A visual comparison of the mean age of occurrence of key natural history milestones among those with BMD versus those with DMD highlighted the later age of occurrence and greater heterogeneity of the age of occurrence of key clinical events common to both diseases. This figure, however, does not highlight the different proportions of patients who experience outcomes, as in DMD (unlike BMD), all patients will experience each outcome if survival allows. However, even among people with the same mutation, phenotype can vary due to modifier genes, epigenetic effects, lifestyle, and environmental factors.
The wide variability in disease progression contributes to significant heterogeneity in the reported clinical phenotype of BMD, making it challenging to describe the disease course. Emerging discussions on the diverse phenotypes of BMD suggest that determining a way to stratify patients based on clinical presentation may help reduce this heterogeneity and improve understanding of disease progression. One explanation for such heterogeneity may be differences in progression between pediatric- and adult-onset BMD. In most data included in this synthesis, both pieces of information needed to stratify by this variable (i.e., age at onset or diagnosis and cardiac involvement) were rarely available.
Limitations
There are several limitations to the current study. First, is the heterogeneity of study design. While care was taken to contextualize study design in data synthesis and interpretation to mitigate bias, it is nonetheless the case that data were derived from a diverse collection of designs including clinical trials, observational studies, and case series/reports. A sensitivity analysis was considered based on study quality assessments (Supplementary Table S4); however, the range of study designs was too heterogeneous to allow for meaningful comparison.
For the frequency of occurrence of natural history milestones, right censoring is present, for example, a 42-year-old patient counted as ‘ambulant’ based on age and status at the time of the study could lose ambulation over subsequent years. This would be true for all ‘life-stage’ age groups assessed and may have resulted in an underestimate of the frequency of outcomes occurring in BMD. No studies identified in this review reported lifetime risk.
Observed variation in the frequency and timing of events across studies may be accounted for, at least in part, by the definitions used to categorize a natural history event as having occurred. For example, various cut-points are used to distinguish a person from having, or not having, advanced cardiac involvement (indicative of cardiomyopathy) across the literature (e.g., left ventricular ejection fraction of ≤55% and fractional shortening <25% were used to classify cardiomyopathy in individual publications).9,64 Transitional ambulatory outcomes were considered, as they could represent either a reduction in ambulatory function (i.e., progression toward loss of ambulation) or be the result of developmental delay in motor skills (i.e., difficulty achieving walking milestones), particularly when reported in younger ages. For this reason, these outcomes were classified as ‘abnormal’ rather than ‘decreased’ ambulatory function (e.g., difficulty climbing stairs; waddling gait). Respiratory outcomes may also be impacted by this ambiguity. For example, the use of CPAP was included under the “receiving respiratory support/ventilation” category of patients but may be solely related to the presence of obstructive sleep apnea in some patients, resulting in potential misclassification bias. While certain milestones (e.g., hypertrophic cardiomyopathy) were inferred based on the context in which they were reported, it can never be ascertained with certainty that every clinical manifestation reported is directly a result of their muscular dystrophy. The different definitions for natural history milestones included in this review are available in the supplemental materials (Supplementary Table S2). In addition, data for some age group strata were sparse which should be considered when interpreting estimates. Furthermore, milestones related to symptoms, mobility, and other functional limitations are rarely discrete events with a clearly identifiable onset date. Instead, they often progress gradually, making it difficult to determine exactly when they occur. Additionally, many studies relied on patient or caregiver recall, which may introduce recall bias and affect the accuracy of reported timing. This limitation was present in the studies included in this review and therefore in also inherent to this systematic review. Although the timing of events was captured to the extent possible, the gradual nature of these changes, and potential recall inaccuracies, should be considered when interpreting the results.
Using the definitions provided in the publications, the goal, wherever possible, was to accurately reflect the authors’ interpretations of whether individuals experienced specific clinical milestones. However, these definitions may overlap and introduce misclassification bias. For example, although left ventricular ejection fraction (LVEF) values within recognized cutoff ranges could classify patients as having cardiac involvement, one publication described patients with borderline low LVEF as not having cardiac involvement, because other patients in the same cohort were explicitly reported as having dilated cardiomyopathy. 49 Similarly, patients with the same IQ may have been classified differently across publications. For example, one publication described patients 56 with an IQ >70 as having typical cognitive function, 76 while others described those with an IQ >85 as normal. 34 Additionally, while not included in the cognitive analyses, the prevalence of other clinically significant neurodevelopmental or neuropsychiatric disorders (e.g., depression, anxiety, and autism spectrum disorder) are higher in patients with BMD than in healthy children and may have had an impact on cognitive function in these patients.158,159
All estimates of the age at which events occurred were derived from those who had experienced the events only, due to how the data were reported in the literature. This will have resulted in an earlier estimate of the age at experiencing outcomes than if data were available from a real-world cohort accounting for censoring (i.e., calculated from a denominator of those with and without having experienced the outcome over a lifetime risk assessment). In addition, publications reporting on specialized BMD subpopulations were included in these analyses. However, the various criteria for restriction could result in bias in either direction (i.e., towards a younger or older age of occurrence) and the result of a sensitivity analysis conducted with only general BMD population studies resulted in limited impact.
Additionally, the present study aimed to provide an overview of the occurrence of natural history outcomes among individuals with BMD; however, data on age at onset aligned with each outcome or the proportion achieving each outcome were not available, so analyses stratified by pediatric versus adult onset could not be conducted. Prior literature has identified this distinction as important, with earlier onset of signs and symptoms associated with earlier age at LOA in DMD and BMD populations. 160 Future analyses evaluating the natural history of BMD should consider stratification by age at disease or symptom onset, or ensuring these data are available when presenting individual patient characteristics.
While assumptions were required around classifications of outcomes (given some heterogeneity in definitions across studies) and characterizing studies as reporting on a general BMD population vs. a BMD subpopulation, limited impact was observed when testing these outcomes in sensitivity analysis. Very little impact was observed across most sensitivity analysis, likely due to the large availability of data across outcomes and that if the decision was difficult, the classification in either direction should make little impact. One notable difference was the difference in age at decreased cardiac function (cardiac involvement) was substantially younger when data for age at starting cardiac medications (e.g., ACE inhibitor therapy) was included in the estimate. This may reflect the prophylactic initiation of cardiac medication prior to the onset of symptoms, a practice employed at some centers to improve cardiac outcomes in BMD. 161
This research sought to explore the impact of corticosteroid use and underlying genotype on the frequency and timing of BMD progression outcomes; however, data were too sparce to elucidate the impacts of these potential disease modifiers. The use of corticosteroids was reported in only 36% of included publications (yes, no, or mixed), and where reported, was done so inconsistently with little to no information provided on type of corticosteroids prescribed, dosing amounts or regimens, or duration of treatment. The same was true for any other medication used (e.g., cardiac medications). Regarding underlying mutation, this information was more commonly reported; however, there was a wide variety of genotypes represented and methods of categorization by genotype were inconsistent, therefore it was not possible to stratify results.
Finally, the authors acknowledge that the time elapsed between the search initiation and the publication of the SLR exceeds the recommended window for reviews of this nature. Given the scale of this work, substantial time was required for data extraction, cleaning, and synthesis during which additional relevant studies may have been published. Furthermore, the iterative nature of this SLR, including decisions related to study and outcome classification, differed from that of typical reviews.
Conclusions
This SLR sought to characterize data availability and synthesize findings related to the natural history of BMD. Although the available evidence is limited, key clinical outcomes were consistently reported in studies including patients across a broad age. In most patients, major BMD-related events such as the need for ventilatory support, loss of ambulation, or development of scoliosis were not observed, whereas transitional or advanced cardiac involvement was eventually reported in approximately three quarters of cases. Among patients in whom these events occurred, the age at onset varied considerably.
Further longitudinal data from large, well-characterized cohorts are required to address existing knowledge gaps in the natural history of BMD. Study reporting should include precise definitions of clinical outcomes, documentation of individual patient mutations, and detailed descriptions of prior and current treatments (including corticosteroid and cardiac therapies) and their respective regimens. Stratifying BMD populations into phenotype groups encompassing the full spectrum of clinical manifestations, as well as by pediatric-versus adult-onset disease, may facilitate a more accurate characterization of disease progression and improve comparability across studies.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261420045 - Supplemental material for The natural history of Becker muscular dystrophy: A systematic literature review
Supplemental material, sj-docx-1-jnd-10.1177_22143602261420045 for The natural history of Becker muscular dystrophy: A systematic literature review by Alexis T Mickle, Karissa M Johnston, Kristen L Ricchetti-Masterson, Andrew R Kennedy, Sarah GC Korpach and Katherine L Gooch in Journal of Neuromuscular Diseases
Footnotes
Abbreviations
Acknowledgments
The authors thank Elizabeth Badillo for providing medical writing support and for their assistance in preparing and refining the manuscript.
Ethics approval
As all data used in this review was derived from published sources, ethics approval was not required.
Consent for publication
Not applicable.
Authors’ contributions
Authors ATM, KMJ, KLRM, ARK, SGCK, and KLG contributed to the study conception and design. Data analysis was performed by ATM and ARK. ATM drafted the manuscript. Authors ATM, KMJ, KLRM, ARK, SGCK, and KLG read and approved the final manuscript.
Funding
Sarepta Therapeutics Inc.
Declaration of conflicting interests
ATM, KMJ, ARK, and SGCK are employes of Broadstreet HEOR which received consulting fees from Sarepta Therapeutics Inc. to carry out this project. KLRM and KLG are employes of Sarepta Therapeutics Inc. and may hold stock/options.
Availability of data and materials
All data sets generated in the course of this research are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.