
Abstract
Background:
Clinical Outcome Assessments (COAs) are essential for monitoring progression and treatment response in neuromuscular diseases. However, substantial variability exists in training, confidence, and implementation of COAs among clinical evaluators working with individuals with Spinal Muscular Atrophy (SMA). This study aimed to identify and address these gaps within the Canadian clinical context through a phased educational initiative guided by the Rare Knowledge Mining Methodological Framework (RKMMF).
Methods:
A qualitative, phased design was used. A needs assessment with 71 physiotherapists and occupational therapists via focus groups identified inconsistent access to SMA-specific training and challenges in applying standardized assessments. Based on these findings, expert faculty co-developed and delivered bilingual workshops incorporating real-world evaluation videos, simulation-based learning, and multidisciplinary case discussions. Pre- and post-workshop surveys, based on an adapted Kirkpatrick Model, measured changes in familiarity, preparedness, and clinical confidence. Data were analyzed using thematic content analysis and descriptive statistics.
Results:
Seventy-nine evaluators from Canada participated. Pre-workshop data revealed major gaps in familiarity with SMA-specific COAs. Post-workshop surveys indicated a 75% average increase in self-reported preparedness, with the greatest gains in the Adapted Test of Neuromuscular Disorders 3.0. Four key themes emerged: limited training and support networks; the critical role of multidisciplinary collaboration; constraints of current COAs due to ceiling and floor effects; and the value of integrating patient-reported outcomes in clinical practice.
Conclusion:
Peer-led, evidence-informed workshops significantly improved clinical preparedness in SMA assessment. These findings support the need for ongoing training strategies and demonstrate the RKMMF as a scalable approach for capacity-building in rare disease care.
Keywords
Introduction
Over the past decade, the clinical landscape of spinal muscular atrophy (SMA) has undergone a profound transformation. Once considered one of the most common genetic causes of infant mortality, SMA has three disease-modifying therapies (DMTs): Spinraza (nusinersen), Zolgensma (onasemnogene abeparvovec), and Evrysdi (risdiplam). These treatments have significantly altered the natural history of the disease and reshaped patient outcomes, standards of care, and long-term expectations. 1 The concurrent implementation of newborn screening programs has further revolutionized disease management by enabling early diagnosis and timely intervention. 2 As SMA management evolves with the advent of adjuvant therapies such as muscle-targeted treatments like apitegromab 3 there remains a critical need to optimize best practices for clinical care and to standardize the selection and administration of clinical outcome assessments (COAs)4,5 that comprehensively describe how a patient feels, functions, or survives, while also capturing treatment-related changes in real-world settings.
SMA is a recessive neuromuscular disease (NMD) characterized by progressive muscle weakness and atrophy due to lower motor neuron loss. Approximately 90% of SMA is caused by a deletion or mutation on chromosome 5 of the Survival Motor Neuron (SMN) 1 gene (5q13.2), 6 which has a crucial role in producing SMN protein. 7 The SMN protein is essential for lower motor neuron health and function. In addition to the SMN1 gene, the SMN2 gene produces a small amount of stable SMN protein. Therefore, a higher number of SMN2 gene copies generally corresponds to more SMN protein present and less disease severity. 8 SMA clinically manifests with muscular, bulbar and respiratory weakness. As a result, persons with SMA (pwSMA) experience functional impairments, including gross and fine motor impairments, fatigue, reduced social participation, pain, gastrointestinal issues, sleep disturbances, emotional dysregulation, respiratory impairment, and bulbar dysfunction affecting speech and swallowing.7–9
Historically, SMA has been classified based on age of symptom onset and maximum motor milestone achievement in untreated patients. 10 However, this classification does not adequately capture the evolving phenotypic spectrum resulting from therapeutic advances and shifts in standard of care. 11 In 2007, a consensus statement on SMA standard of care was published to improve patient management and establish a framework for future clinical trials. 12 These guidelines were subsequently updated in 2018, producing a two-part set of recommendations in response to the expansion of clinical trials and the availability of novel treatments. 13
Clinical evaluators are healthcare professionals who administer and interpret COAs, including neurologists, physiotherapists (PTs), occupational therapists (OTs), respiratory therapists, and speech-language pathologists. In the context of SMA, those involved in clinical trials typically received training on disease-specific COAs. However, clinical trials are relatively uncommon, and access to this training is generally restricted to members of clinical research teams. Expertise in SMA assessment is therefore often tied to trial participation rather than an established standard of care. In community and primary settings, therapists often have limited time and may not require or be expected to conduct detailed research-grade outcome assessments. These assessments are typically performed by PTs and OTs within SMA specialist centers. Whereas, community PTs/OTs provide complementary longitudinal care, enabling transitions between functional assessments and everyday rehabilitation goals. Krosschell and colleagues 14 emphasized that without broader dissemination of training and resources, clinical evaluators working outside of specialized or academic settings seldom receive formal instruction in SMA-specific COAs.
Another layer of complexity arises from how COAs are selected. Performance outcome measures (PerfOs), particularly those focused on motor function, are often chosen by industry sponsors during clinical trial design.15–17 These trial-specific measures may have limited alignment with broader clinical standards or COAs routinely used in everyday practice.18–20 Despite this, the same SMA-specific PerfOs are frequently adopted by regulatory agencies and health technology assessment bodies to evaluate treatment efficacy and determine reimbursement eligibility in real-world settings.21–23 As a result, measures initially selected for regulatory approval purposes become embedded within public reimbursement criteria, even though they were never widely implemented in clinical care.24–26
This misalignment creates significant challenges. Significant variation in healthcare infrastructure across Canadian provinces contributes to uneven access to qualified personnel, specialized services, and the broader supports required for comprehensive SMA care. 27 Access to DMTs, assistive devices, medical equipment, and genetic testing differs substantially by jurisdiction, reinforcing inequities in care that are shaped more by geographic location than clinical need. This phenomenon, often described as “postal code healthcare,” highlights the absence of a coordinated national strategy to ensure equitable access to therapies and services. 28
Provincial variability in reimbursement criteria has also shaped the availability of trained clinical evaluators. In Quebec, broader public coverage for adults with SMA has facilitated earlier and more consistent access to treatment, which in turn has supported investment in clinical training and capacity. Quebec's health technology assessment agency, INESSS, has adopted a “promise of value” approach to enable early access to therapies that show clinical potential but may lack mature cost-effectiveness data. In contrast, more restrictive reimbursement policies in other provinces, particularly those limiting access for adult populations, have contributed to underinvestment in evaluator training and infrastructure development.29,30
Addressing these disparities requires a harmonized, sustainable, and patient-centered approach to care delivery for individuals living with rare and complex conditions. Recent qualitative research has underscored the need for greater consistency in access and care coordination across jurisdictions. 30 A Canadian consensus-driven toolkit has recently been developed to guide SMA disease monitoring and improve the quality of real-world evidence.31,32 However, persistent gaps remain in clinical capacity, treatment access, and the infrastructure required to generate robust real-world evidence (RWE). These challenges are compounded by the lack of a universally accepted patient registry and limited support for standardized data collection across clinical settings. A national training pathway for SMA clinical evaluators is urgently needed to address these systemic gaps and improve care equity, data quality, and long-term health outcomes.
To address these challenges, we developed a multi-pronged approach that involved: 1) Identifying the learning needs of clinical evaluators including physiotherapists, occupational therapists, and nurses working with individuals with SMA in the context of COAs. Although multidisciplinary SMA care includes many professions, this study focuses on PTs, OTs, and nurses because these disciplines are primarily responsible for conducting motor outcome assessments in Canada, and the identified training gaps were discipline specific. 2) Delivering a structured training workshop as part of an education initiative, and 3) evaluating the outcomes of SMA-focused training workshops designed to enhance evaluator knowledge and skills.
By addressing these objectives, this study contributes to the broader effort to standardize clinical training, improve the consistency of COAs, and strengthen evidence-based decision-making in SMA care, while also underscoring the need for coordinated data infrastructure to support RWE generation.
Methods
The objective of this study was to identify and address gaps in knowledge among clinical evaluators, specifically PTs, OTs, and neuromuscular nurses, across Canada regarding COAs for SMA. The study was designed using a phased qualitative approach guided by the Rare Knowledge Mining Methodological Framework (RKMMF) (Figure 1) 33 and an exploratory sequential mixed-methods design was used. The first phase consisted of a qualitative needs assessment to identify gaps, training needs, and preferred learning approaches among clinical evaluators. The second phase involved quantitative pre- and post-workshop surveys, informed by the Kirkpatrick model, to assess changes in participants’ familiarity and confidence with SMA-specific assessments.
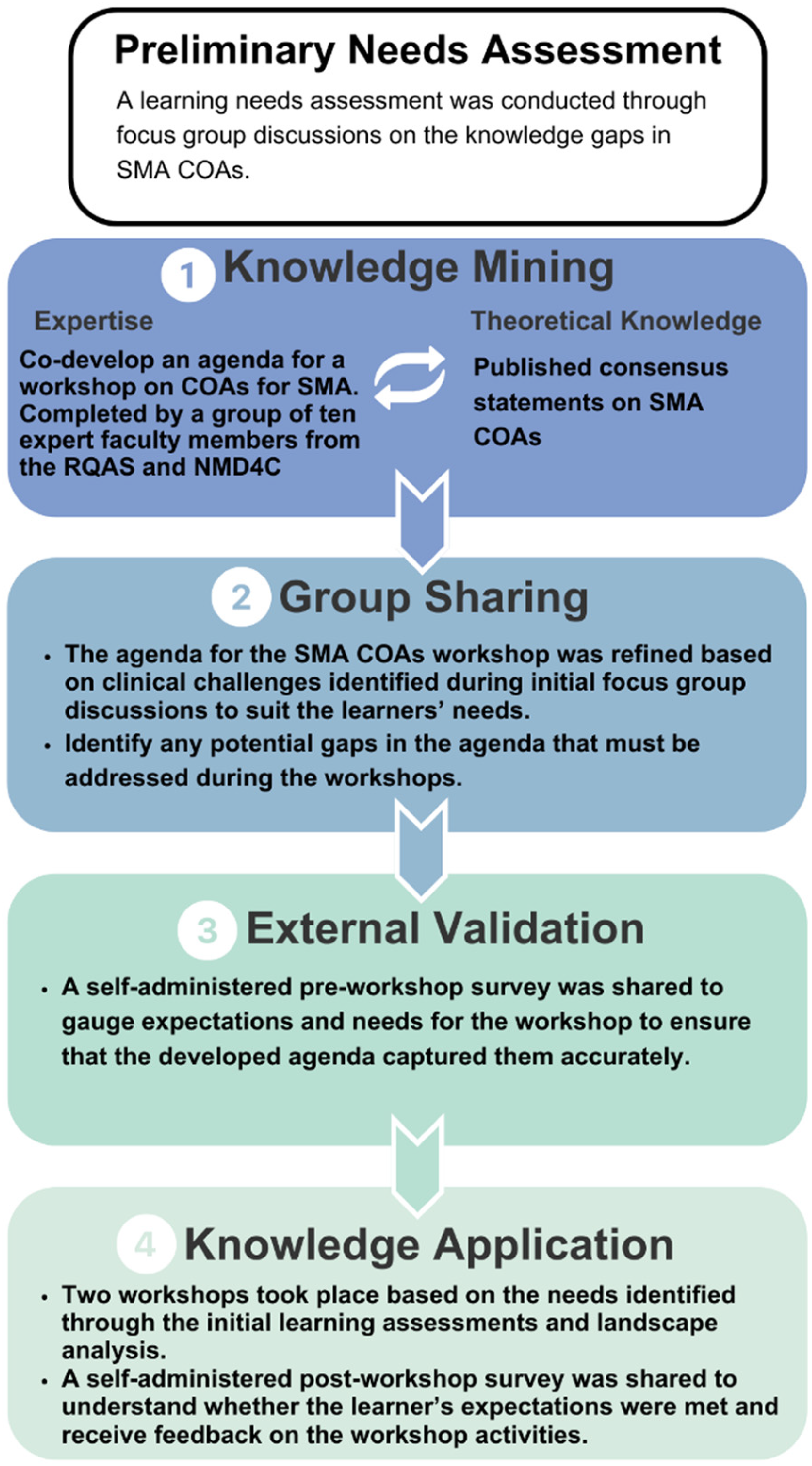
Development of workshops on SMA in accordance to the RMKKF guidelines.
Preliminary Needs Assessment: According to Gagnon and colleagues, 33 conducting a needs assessment is an essential step prior to implementing RKMMF-informed workshops, as it ensures that educational interventions are aligned with the real-world challenges and priorities of the target audience. 33 Consistent with this recommendation, we completed a preliminary needs assessment to characterize the current knowledge, confidence, perceived gaps, and preferred learning modalities of clinical evaluators regarding the use of COAs in SMA care. This assessment was conducted through virtual focus group discussions with PTs, OTs, and nurses actively working with individuals living with SMA.
Discussion prompts examined how evaluators currently acquire knowledge about NMDs, including through formal education, continuing professional development, mentorship, industry-led training, and self-directed learning, as well as how SMA- and COA-specific training is typically obtained in routine practice. The assessment also explored discrepancies between academic preparation and clinical expectations in managing rare neuromuscular conditions, barriers to applying SMA-specific COAs such as limited hands-on opportunities and restricted access to specialized mentorship, and variability in the availability of standardized tools across care settings. Participants were further asked to describe their preferred formats for future training, including interactive workshops, online modules, case-based instruction, mentorship, and certification pathways.
Insights from this needs assessment directly informed the design of the workshop content and delivery model, ensuring that the educational intervention was relevant, feasible, and responsive to the diverse experience levels of clinical evaluators in SMA care.
Knowledge Mining: Based on insights gathered during the needs assessment, key content leads were identified from two Canadian networks: the Réseau québécois de l'amyotrophie spinale (RQAS) (https://www.rqas.ca/), a regional network focused on SMA in Quebec, and the Neuromuscular Disease Network for Canada (NMD4C) (https://neuromuscularnetwork.ca/), a pan-Canadian clinical, research, and academic network comprising scientists, neurologists, physiatrists, allied health professionals, trainees and patient partners. These content leads were selected based on their expertise of SMA COAs, having previously received training on clinical assessments used in therapeutic trials. In addition, they had extensive experience training others through preceptorships and had been actively involved in the implementation and evaluation of SMA motor function assessments in both clinical and research settings. These leads were invited to form an expert faculty consisting of 10 clinical evaluators, who engaged in structured discussions on their experiences with SMA COAs, reviewed available relevant literature,31,32 and collaborated to co-develop a workshop agenda.
Group Sharing: Open discussions were conducted to validate and refine findings with input from four medical experts, including clinician-scientists, physiatrists, and neurologists. The workshop agenda was iteratively revised to address clinical challenges identified in focus group discussions and expert faculty consultations, ensuring that the content remained relevant and responsive to the needs of clinical evaluators. The knowledge mining and group sharing phases were conducted in a continuous, iterative manner, with ongoing discussions and refinements to ensure the workshop curriculum effectively aligned with the evolving learning needs of participants and real-world clinical practice.
Workshop participants were recruited through targeted email communication from the NMD4C and Muscular Dystrophy Canada (MDC, https://muscle.ca/), a national patient organization. As part of the recruitment strategy, clinicians who participated in the learning needs assessment were specifically invited to attend, allowing them to further engage with the workshop content and benefit from the training tailored to the gaps identified in the assessment phase. This also facilitated continuity in addressing the challenges and educational priorities they had previously expressed. A registration form was distributed to express interest in attending the SMA COAs workshops, delivered in English and French. To ensure relevance to the workshop objectives, the inclusion criteria required participants to be registered members of RQAS or NMD4C, confirming their involvement in NMD clinical practice. All attendees met this criterion, ensuring that the training reached clinical evaluators actively engaged in the assessment and management of individuals with SMA.
External Validation: A self-administered pre-workshop survey was designed to assess participant familiarity with SMA COAs, perceived challenges, expectations, and learning needs. This survey contained eight Likert-style and open-ended questions adapted from the Kirkpatrick model, a framework for evaluating the effectiveness of training interventions. 34 The feedback obtained from this survey enabled the faculty and medical experts to refine the workshop content and format.
Knowledge Translation: In order to evaluate the workshops, an identical post-workshop survey was administered. All workshop sessions were audio recorded to support comprehensive note-taking and to facilitate further analysis of the outcomes. A qualitative content analysis approach35,36 was employed to analyze the focus group discussion transcripts, extracting key concepts that informed the development of the workshop content and structure. Pre- and post-workshop survey data were analyzed to assess changes in participant knowledge, uptake of training content, and perceived impact on clinical practice. Open-ended responses from the surveys, along with workshop summaries and transcripts, were subjected to thematic content analysis, with key themes systematically categorized to identify overarching insights and areas for future development. Quantitative data were analyzed using descriptive statistics and frequency distributions to provide a detailed overview of participant demographics and survey responses.
Results
Of the 113 individuals invited to participate in the preliminary needs assessment, 71 PTs, OTs and nurses from MDC's membership database participated. These participants represented both urban and rural settings across multiple provinces, providing a diverse national perspective on clinical practice needs. Participants worked in public and private practice settings, served diverse age groups, and provided care for individuals with NMDs, reflecting the broad scope of clinical evaluators engaged in neuromuscular care.
A total of 79 regulated allied health professionals participated in the two SMA COA workshops, including 28 OTs, 50 PTs, and 1 registered nurse. The following provinces were represented: Alberta (n = 4), British Columbia (n = 4), Manitoba (n = 2) New Brunswick (n = 7), Nova Scotia (n = 2), Ontario (n = 6), Quebec (n = 49) and Saskatchewan (n = 5). The geographic distribution of participants reflected regional differences in SMA treatment access and training opportunities.
Among the 79 workshop attendees, 49 participants were practicing in Quebec. While this may reflect the alignment between treatment availability and a relatively high concentration of trained clinical evaluators in the province, it is also likely influenced by contextual factors such as the organization of neuromuscular services within rehabilitation centers, as well as recruitment dynamics including local champions, word-of-mouth promotion, and professional networks that may have facilitated broader participation. Quebec's broader reimbursement policies for DMTs, including access for adults, have driven a greater demand for SMA assessments, fostering higher familiarity and experience with SMA-specific COAs. Pre-workshop survey results indicated that Quebec-based clinical evaluators were generally well-versed in COAs applicable to both pediatric and adult patients and expressed a strong interest in ongoing professional development to further enhance their expertise.
In contrast, the remaining 30 participants represented other provinces across Canada, where access to DMTs, particularly for adults, is more restrictive. Many of these clinical evaluators worked in pediatric settings. Despite working with pediatric populations, this cohort reported significantly lower familiarity with SMA-specific COAs in the pre-workshop survey. Participants noted having had no prior formal training in standardized motor COAs and described very limited familiarity overall. Aside from one assessment routinely used in clinical practice, they indicated little to no familiarity with the outcome measures typically used in SMA-specific COA administration.
The expert faculty developed a comprehensive workshop agenda covering key topics relevant to SMA assessment and clinical management. Although COAs span multiple functional domains in SMA, the workshop focused primarily on standardized motor function assessments that are commonly used in clinical research. The agenda included:
Introduction to SMA and its evolving phenotype Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP-INTEND) Bayley Scales of Infant and Toddler Development, Third Edition (BSID-III) Adapted Test of Neuromuscular Disorders 3.0 (ATEND 3.0) Hammersmith functional motor scale-extended (HFMSE) 6-minute walk test (6MWT) Revised upper limb module (RULM) Patient-reported outcome measures (PROMs) Establishing an adult SMA specialized clinic
Several of the COAs included in the workshop, such as CHOP-INTEND, HFMSE, RULM, and the 6MWT, have been widely used in SMA clinical trials. In contrast, ATEND 3.0 is a newer assessment developed in response to evolving adult SMA phenotypes and has not been part of traditional clinical trial protocols. The pre- and post-workshop survey data revealed an average 75% increase in self-reported preparedness and familiarity across all COAs covered in the training (Figure 2). The greatest improvement was observed with the ATEND 3.0, where familiarity ratings increased the most following the workshop, while the smallest gains were seen in BSID-III. Collectively, these findings highlight the significant impact of structured training and targeted education in strengthening clinical capacity for SMA assessment, reinforcing the need for ongoing professional development to standardize and enhance evaluator expertise.
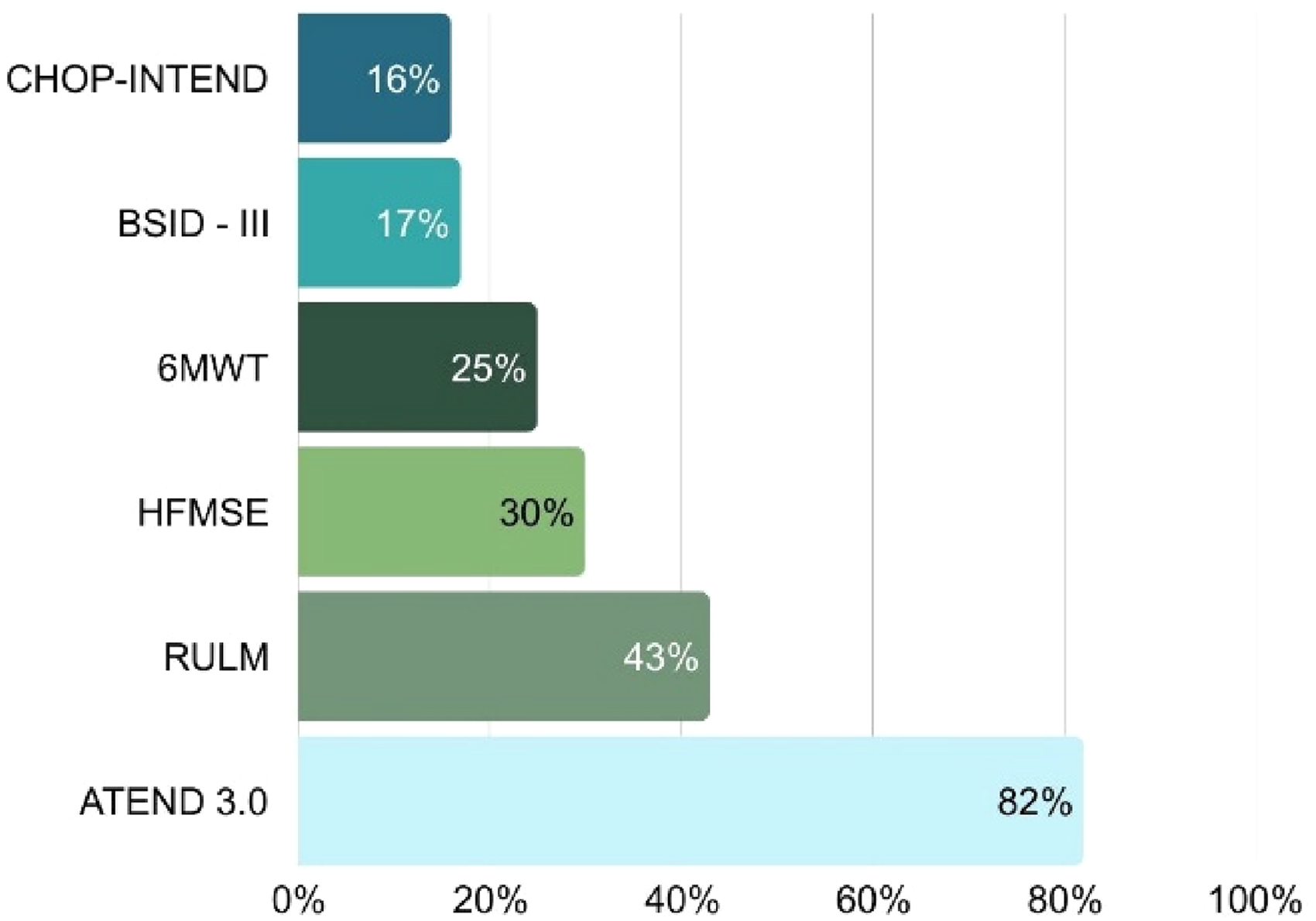
Perceived increase in participants’ familiarity and comfort with targeted COAs after attending workshops.
Four key themes emerged from the analysis of preliminary needs assessment, the development and delivery of the RKMFF-informed workshops and the pre- and post-survey results.
Lack of training opportunities and a support network for clinical evaluators in SMA
The first theme relates to baseline training gaps and the absence of structured support for allied health professionals involved in SMA assessment across provinces and institutions. Training specific to SMA was found to be limited, with most available educational resources primarily targeted at researchers and physicians. Participants reported that webinars and training sessions often put on by their academic or clinic institution focused largely on disease progression and investigational drug updates geared towards physicians rather than on practical, hands-on training to improve clinical assessments and patient management for allied health professionals. This highlights the unmet need for targeted, evidence-based training programs tailored to clinical evaluators, particularly those with limited experience in assessing individuals with SMA. Participants emphasized the lack of mentorship and peer-to-peer support opportunities as a major barrier to developing expertise in SMA motor function assessment. Many expressed the need for a formalized support network where they could engage in discussions about challenges in COA administration and interpretation, particularly for those measures with which they had less experience.
A key component of the workshops was the use of video recordings of real-world patient evaluations and in-person simulation demonstrations, showcasing individuals with SMA across the clinical spectrum from non-sitters to those who are ambulatory. This format enabled participants to observe standardized assessments in practice, analyze performance on specific COA items, and discuss scoring discrepancies. These interactive discussions allowed participants to compare COA scores, refine their assessment techniques, and work toward a consensus on best practices. Consensus referred to general agreement among at least 90 percent of participants, reached through facilitated group discussion on the most appropriate scoring for each assessment scenario. This process underscored the value of hands-on, collaborative learning in supporting consistent and accurate assessment practices and mirrors current clinical trial training practices, including video-based scoring on different patient phenotypes and facilitated score harmonization.
Multidisciplinary capacity as a determinant of consistent COA practice
This theme highlights how system-level factors, particularly multidisciplinary capacity and staffing structures, influence the ability to conduct and integrate COAs into routine care.
There are substantial disparities in access to multidisciplinary care across NMD centers in Canada, particularly in the composition and capacity of clinical teams responsible for administering COAs. Participants reported these differences stem not only from local program design, but also from broader systemic limitations in access to publicly funded PT and OT services. Participants also emphasized that very few PT services are covered for adults with SMA under provincial health programs, creating significant gaps in community-based rehabilitation options. Systemic funding constraints and inconsistencies in neuromuscular-specific care models further compound these challenges for both clinical evaluators and patients.
While certain motor function assessments are required for reimbursement by both public and private payers, the availability of trained personnel to administer these assessments varies significantly across sites. Many participants reported being the sole clinical evaluator at their location, responsible for conducting all assessments without the support of a broader multidisciplinary team. This limited staffing capacity often prevents clinical evaluators from participating in broader aspects of rehabilitation and holistic patient management. As a result, many PTs and OTs primarily serving as clinical evaluators rather than as active members of a comprehensive care team. A key concern raised was that the need to complete specific assessments for the purpose of reimbursement often shifts clinical focus away from holistic, patient-centered rehabilitation. Clinical evaluators noted that the emphasis on scoring and data collection can detract from broader therapeutic goals and functional improvements that align with the patient's priorities. This dynamic creates tension between meeting administrative requirements and providing high-quality, individualized care.
These observations were further supported during workshop discussions, where participants learned about the adult SMA clinic in New Brunswick. This clinic uses a model in which a physiatrist leads a multidisciplinary team located within a tertiary-level rehabilitation center that includes PTs, OTs, respiratory therapists, and clinical research specialists. This structure allows for both comprehensive assessments and ongoing therapeutic intervention and is regarded as a model of best practice. However, participants agreed that this approach is not common and does not reflect the reality at most centers across Canada, where clinical evaluators often work in isolation.
Despite these challenges, many participants expressed optimism during focus group discussions that even modest increases in staffing, such as the addition of a nurse or allied health professional, could significantly enhance care delivery. Clinical evaluators noted that incremental improvements in team capacity would facilitate better coordination of assessments, reduce the workload on individual providers, and support more comprehensive, rehabilitation-focused care for individuals with SMA. This theme emerged consistently across all four focus groups, with over two-thirds of participants articulating this need. In addition, there was widespread agreement that required assessments should be embedded within a holistic treatment plan that considers patient function, quality of life, and personal goals. This perspective was strongly endorsed by participants and was consistently reflected across transcripts, suggesting a shared view on the importance of integrating assessments into meaningful clinical decision-making. Taken together, these observations highlight how strengthening evaluator knowledge and team capacity can support more consistent rehabilitation practices, particularly in community settings.
Current COAs do not reflect the current needs and priorities of patients
This theme focused on the limitations of currently used COAs when applied in real-world clinical settings. The analysis revealed significant concerns among clinical evaluators regarding the applicability of COAs in real-world practice. Clinical evaluators emphasized that clinical trials typically assess treatment efficacy in highly selected and relatively homogeneous patient populations. While this approach is necessary to achieve statistical power, it limits the applicability of trial-based findings to real-world clinical settings, where individuals with SMA often present with greater variability in age, disease phenotype, and functional status. 25 This mismatch reduces the generalizability and clinical utility of trial-validated outcome measures. These observations underscore a growing recognition that the outcome measures used in research may not be suitable for routine clinical practice. 17 There was discussion in support for simplified, low-burden, and cost-effective tools that are feasible for use in clinical settings. Such tools should be validated against established research-grade assessments but designed for practical implementation to facilitate ongoing monitoring and informed clinical decision-making in diverse patient populations.
Equally concerning was the perceived lack of responsiveness, or longitudinal validity, of many currently used COAs. 32 Responsiveness refers to an instrument's ability to detect meaningful or clinically significant change over time.37,38 The minimal clinically important difference (MCID) represents the smallest change in a COA that is perceived as meaningful by patients, caregivers, or clinicians and that reflects a real improvement in daily functioning. Participants noted that current SMA COAs often lack established MCID values, particularly in treated populations with evolving phenotypes, which limits their ability to detect subtle but important changes. As discussed in the focus groups, many pwSMA describe improvements such as requiring less time to eat, groom, transfer, or complete self-care tasks. However, these clinically meaningful gains are not consistently captured by existing capacity-based COAs.
Ceiling effects: The need to re-evaluate COA selection in the context of newborn screening, early intervention, and evolving SMA phenotypes was also discussed. With earlier treatment initiation and increased use of gene-replacement therapy, more infants are reaching motor milestones that exceed what tools like CHOP-INTEND were designed to assess. 16 Clinical evaluators noted that ceiling effects may now be observed in these cases, necessitating a shift toward alternative assessments such as the Alberta Infant Motor Scale (AIMS) and Peabody Developmental Motor Scale-2 (PDMS-2) to provide a more comprehensive evaluation of early motor function (Figure 3). AIMS and PDMS-2 have robust psychometric support in general pediatric motor assessment; however, validation in treated SMA populations remains limited. Their use was recommended by workshop faculty because they capture higher-level motor skills increasingly observed in treated infants and toddlers, making them valuable complementary tools when CHOP-INTEND no longer reflects functional ability.39,40
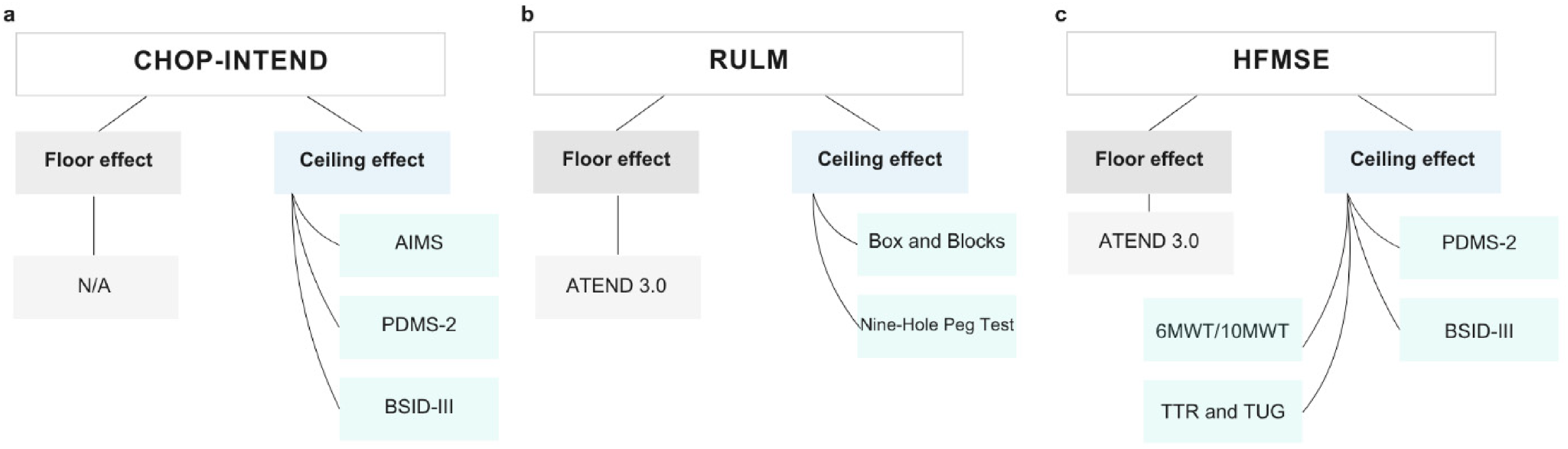
Schematic representation of suggested COAs that could be performed along with the standardized ones if suspecting a floor or ceiling effect
Similarly, as more children with SMA gain the ability to sit independently, transitioning from the CHOP-INTEND to the HFMSE was identified as a more appropriate approach to measuring their functional capabilities (Figure 3). Another major concern was the inability to administer certain CHOP-INTEND items to toddlers and adolescents, leading to the recommendation that ATEND 3.0 be used for sitters and HFMSE for non-sitters (Figure 3).
Floor effects: Evaluators noted that the RULM presents limitations, particularly in strong sitters and ambulant individuals, where it does not sufficiently measure fine motor skills or upper limb dexterity. To improve assessment accuracy, the Box and Blocks Test and Nine-Hole Peg Test were suggested as alternative tools for these populations (Figure 3). In non-sitter adults and older adolescents, participants noted that RULM frequently leads to floor effects, making ATEND 3.0 a more suitable option to assess motor function changes in this group. Evaluators described cases where patients with SMA struggled to demonstrate progress due to the inherent limitations of existing COAs. In some instances, motor function assessments required for reimbursement were misaligned with the patient's true functional abilities, making it difficult to justify continued treatment despite observable real-world benefits. Evaluators also emphasized that the stress associated with these assessments particularly for individuals who understood that their continued access to treatment depended on COA scores could introduce variability in performance.
High value in implementing PROMs in clinical practice
The final theme emphasized the importance of PROMs, particularly in capturing meaningful functional and quality-of-life changes that clinician-rated COAs may overlook. A lack of awareness and limited use of PROMs among clinical evaluators working with pwSMA emerged as a key gap in training & practice. While there is a growing recognition for PROMs, their integration into routine clinical assessments remains limited, despite their potential to capture meaningful functional and quality-of-life changes that are not reflected in standard COAs. To address this gap, expert faculty provided suggestions and shared a list of relevant PROMs for this population alongside testimonials from pwSMA describing their experiences with existing assessments.
One of the most frequently reported treatment-related changes discussed was a reduction in fatigue levels, a factor not adequately captured by traditional COAs. 41 While the 6MWT can assess fatiguability, its application is limited to ambulatory individuals, leaving sitters and non-sitters without a standardized tool to document fatigue-related limitations. Clinical evaluators noted that fatigue in pwSMA is often only identified if the patient proactively reports it, making it difficult to assess its impact in a systematic way. Evaluators working with pediatric pwSMA further noted that younger children may not have the verbal skills or self-awareness to articulate fatigue, leading to under-recognition of its effects on daily activities and therapy participation.
Discussions highlighted the critical importance of the value of PROMs that capture real-world functional improvements, particularly those reflecting time efficiency in daily activities. Ultimately, there remains an unmet need to develop and implement PROMs that are important to patients and families coupled with timed functional assessments sensitive to changes in functional efficiency and treatment impact from the patient perspective.
Discussion
The availability of DMTs has fundamentally altered the clinical trajectory of SMA, redefining disease phenotype, functional abilities, and patient care needs. The role of clinical evaluators has recently expanded significantly, necessitating updated training in COA selection, administration, and interpretation. This study describes the development and implementation of two SMA-focused COA workshops, designed to address gaps in clinical evaluator training and best care practices. Through a structured, multi-step process guided by the RKMMF, including a learning needs assessments of clinical evaluators working with pwSMA, the formation of an expert faculty, and the evaluation of training content through pre- and post-workshop surveys, two workshops were developed, delivered and key gaps on the situation in Canada were uncovered.
While some of the insights were directly related to Canada, the advent of newborn screening 42 and early access to DMTs, 43 including gene replacement therapy, has contributed to concerns about the applicability and reliability of existing COAs across the world. Ceiling and floor effects that were discussed in the workshops, reflecting clinical challenges in accurately tracking treatment outcomes in an evolving patient population, have been documented in other studies. 44 For example, for the CHOP-INTEND, a key COA used in clinical trials for infants with SMA, has limitations when applied in real-world settings. An international study evaluating its validity in infants under three months of age demonstrated that while eight of the sixteen test items exhibited developmentally mature responses in the first week of life, the COA only became reliably interpretable at three months, questioning its use following early identification and treatment of infants. 44 This illustrates how COAs developed in controlled trial environments for a non-treated population may not seamlessly translate into clinical practice, particularly in the context of early diagnosis and intervention.
Ceiling and floor effects in adult SMA populations that were highlighted in the workshops have been similarly documented in the literature.31,32,45–50 A study in treated adults with SMA demonstrated a ceiling effect when administering the RULM to highly functional ambulatory individuals, whereas non-ambulatory individuals exhibited floor effects when assessed with the HFMSE or RULMs. 51 These findings emphasize the need to reassess the appropriateness of standard COAs for various SMA phenotypes, particularly in a real-world setting where heterogeneity in disease progression is substantial.
Current COA required for treatment reimbursement rely primarily on performance outcome measurements, which fail to fully capture the multisystemic nature of SMA. Our findings reinforced the need for developing PROMs appropriate for routine clinical practice to supplement motor evaluations and provide a more comprehensive picture of treatment effects. PROMs have been widely recognized as potentially valuable tools to assess quality of life, symptom burden, functional status, pain, and social and mental well-being.50,52,53 They have been particularly instrumental in evaluating treatment outcomes in diseases where curative options are not available, such as cancer, and have been formally recognized by regulatory agencies, including the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA), as valid measures of treatment efficacy. 54 However, in Canada, the adoption of PROMs into routine healthcare remains inconsistent, despite efforts to advance their collection and application. 55 The present workshops emphasized that PROMs remain underutilized in SMA care, largely due to a lack of clinician familiarity with available tools and limited infrastructure to support their systematic implementation. Furthermore, while SMA-specific PROMs exist, they remain limited in scope and do not typically address critical domains such as bulbar function and fatigue, both of which are highly relevant to SMA-related disability.32,46 Further investigation is required to progress towards the development of a PROM that can capture the subtle but meaningful treatment effects that are described by patients, particularly in infants and young children who may not be able to clearly articulate their experiences. 56 Additionally, the implementation of PROMs could contribute to RWE generation, further strengthening the evidence base for SMA therapies.32,46 Possible use of the Patient Global Impression of Change (PGIC) as a valuable PROM for capturing patient-perceived improvement, and additional tools focused on fatigue and functional efficiency would help address current measurement gaps. The inclusion of PGIC may also support the derivation of MCIDs, which remains a critical need in neuromuscular populations to assess responsiveness to intervention.
The workshops emphasized the need for continuous evaluation of COAs that reflect the evolving impact of treatment and ensure best care practices adapt to the changing disease landscape.11,48,50 The selection of SMA COAs has traditionally been derived from clinical trial evidence collected in highly controlled environments with homogenous patient cohorts. However, real-world SMA populations are far more heterogeneous, making it imperative to refine assessment strategies that account for variability in phenotypes and disease progression. Participants emphasized the need for broader dissemination of training beyond clinical trial sites, suggesting that virtual modules, asynchronous video-based scoring, and standardized onboarding resources could extend access to clinicians working outside research centers. They also noted that a blended training model, combining hands-on practice with flexible virtual components, would help balance clinical workload demands while still supporting skill development. For instance, incorporating brief calibration sessions into existing team meetings and aligning training activities with routine assessment cycles to ensure that training is integrated into clinical workflow without disrupting patient care.
Meta-analyses evaluating real-world outcomes of nusinersen have consolidated evidence that treatment leads to motor function stabilization or improvement as measured by the HFMSE, RULM, and 6MWT in adolescents and adults, 57 as well as in pwSMA under 12 years old. 58 In contrast, natural history studies have demonstrated that untreated patients typically experience a progressive decline in motor function.59,60 National SMA registries, such as the Canadian Neurological Diseases Registry implemented in Canada, that provides a repository for collecting this important data. 29 While RWE has the potential to fill critical gaps in clinical knowledge particularly regarding long-term treatment effects, healthcare utilization, and disease burden, it remains hindered by a lack of harmonized and standardized data collection practices.
Limitations
This study has some limitations. The involvement of nurses in SMA assessment reflects Canadian practice and may not generalize to jurisdictions where nursing roles differ. Participation in the needs assessment and workshop was voluntary, introducing potential self-selection bias toward clinicians with a specific interest in COA training. Because the workshop focused exclusively on motor function assessments, the findings may not reflect training needs in other clinical domains. Pre- and post-workshop outcomes were based on self-reported familiarity and confidence, which may not align with objective performance or long-term skill retention. Finally, the study examined short-term knowledge gains and did not assess whether training translated into sustained practice change or improved patient outcomes. Future studies should include long-term follow-up across diverse care settings.
Future directions: sustainable training and knowledge dissemination
This study directly informed the creation of a sustainable, on-demand virtual training platform titled Training Resource for Assessments in Neuromuscular Disorders (Train(e)d), available at https://learn.muscle.ca/. This platform delivers accessible, up-to-date educational modules focused on SMA assessments. It is designed to promote national consistency in clinical practice by offering flexible learning opportunities that include expert-led instruction on OM selection, administration, and interpretation. The platform also features real-world case examples and interactive components that support deeper engagement and practical application.
In addition to its instructional content, Train(e)d includes a dedicated online community forum. This forum provides clinical evaluators with a space to connect with peer experts, ask questions, and exchange clinical experiences. The goal of this collaborative environment is to facilitate continuous learning and ensure that the training remains current with evolving evidence and clinical needs. By overcoming geographic and institutional barriers, the platform aims to strengthen national clinical capacity, improve coordination of care, and enhance patient outcomes through more consistent and informed use of COAs across SMA and other neuromuscular disorders. Long-term effectiveness of the Train(e)d platform will be explored through user engagement metrics and potential follow-up assessments to understand whether the knowledge acquired is maintained and integrated into clinical practice.
An important strength of the workshop process was its peer-led structure, which enabled clinical evaluators to learn directly from experienced colleagues actively involved in SMA clinical trials and specialized care. This format supported clarification of key uncertainties and encouraged practical knowledge translation. The workshops also contributed to the formation of a national Neuromuscular Community of Practice (CoP). This initiative is intended to serve as an ongoing platform for professional collaboration, shared learning, and the dissemination of best practices among clinical evaluators.
Sustained collaboration among clinician networks, patient advocacy organizations, and health system stakeholders will be essential for closing the knowledge gap in SMA care. Optimizing clinical practice and RWE generation depends on these partnerships. As additional DMTs become available for conditions such as Myasthenia Gravis, Pompe disease, Myotonic Dystrophy, and Friedreich ataxia, the SMA experience provides a valuable framework for clinician training and health policy development. A grounded theory approach could further clarify how training and support influence long-term evaluator competence, with insights that may extend to other rare diseases. Prioritizing clinician education at the policy level will be critical to achieving equitable access to high-quality care and ensuring meaningful outcomes for individuals affected by SMA and other rare neuromuscular conditions.
Conclusion
With critical gaps in training, standardized assessment methodologies, and RWE generation, sustained investment in clinician education, standardized COA training, and the integration of PROMs into routine practice. If an outcome measure is mandated by payers as a condition for treatment reimbursement, there must be a corresponding commitment to ensuring that clinical evaluators have access to standardized training, qualified evaluators are available across care settings, and the measure itself reliably reflects meaningful functional changes that justify continued access to therapy. Without these safeguards, COA requirements risk becoming administrative hurdles rather than tools that enhance patient care and evidence-based decision-making.
Footnotes
Acknowledgements
The authors thank the content leads and faculty who co-designed and co-developed the workshop curriculum, including Melissa Dermody, Angela Chiu, Cheryl Scholtes, Allison Banks, Dorothy Drost, Sarah Turgeon-Désilets, Mélanie Claveau, Monique Emond, Catherine Desautels, and Isabelle Demers. We are grateful to Marie-Hélène Bolduc for her coordination and support throughout this initiative. Special thanks are extended to our patient partners, Amy Loignon and Catherine Boivin, whose lived experience and insights enriched the content and ensured its alignment with person-centered care.
Ethical considerations
Not applicable.
Consent for publication
Not applicable.
Funding
This study was supported by the Neuromuscular Disease Network for Canada (NMD4C) through grants from the Canadian Institutes of Health Research and Muscular Dystrophy Canada (Network Grant: OR2-189333; Network Catalyst Grant: NG2-170044). Equal funding for the workshops was provided by Biogen, Hoffmann-La Roche, and Novartis Pharmaceuticals through restricted educational grants. These grants supported only the workshop activities and not the research study. The sponsors had no role in the study design, data collection, analysis, interpretation, or manuscript preparation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.