
Abstract
Background:
Myotonic Dystrophy type 1 (DM1) is a multisystemic neuromuscular disorder. Gastrointestinal (GI) symptoms significantly impact quality of life, but remain under-assessed. Currently, no DM1 specific GI questionnaire is available. The Gastrointestinal Symptoms Rating Scale (GSRS) is widely used but lacks validation with modern clinimetric methods.
Objectives:
To evaluate the GSRS using Rasch analysis in DM1 patients and develop a disease-specific, interval-level GI symptom measure.
Methods:
Rasch analysis evaluated item fit, threshold ordering, differential item functioning (DIF), local dependency, and unidimensionality. Model fit was evaluated using chi-square statistics, item and person fit residuals, and the Person Separation Index (PSI).
Results:
Four hundred and three DM1 patients (206 women, mean age 48.3 years) completed the GSRS questionnaire. The GSRS initial data did not meet Rasch model expectations. Three items (hard stools, heartburn, diarrhea) were removed and the item nausea was split by age category. The item constipation had misfit exceeding the Bonferroni threshold, but was retained due to its clinical relevance. The final model did not fulfill Rasch requirements (item fit residuals: −0.23, SD 1.29; person fit residuals: mean −0.27, SD 1.15; item-trait Chi-square: p-value < 0.001; degrees of freedom: 60). Acceptable person separation index (0.76) was obtained.
Conclusion:
This study highlights the challenges of measuring GI symptoms in DM1. Although this research is an important first step, more research is needed for developing a questionnaire that reflects the patient experience whilst simultaneously considering measurement accuracy.
Introduction
Myotonic Dystrophy type 1 (DM1) is a genetically inherited neuromuscular disorder that is caused by a CTG trinucleotide repeat expansion in the Dystrophia Myotonica Protein Kinase (DMPK) gene on chromosome 19. 1 Whereas healthy individuals have 5 to 35 CTG repeats, repeats in DM1 affected individuals range from 50 to 5000. 2 The length of the repeat expansion is moderately correlated with disease severity, as a larger repeat expansion is associated with a more severe phenotype and earlier onset of symptoms. 2
DM1 is generally characterized by muscle weakness and myotonia (inability to relax muscles), although several organ systems can be affected. Cardiac and pulmonary complication are typically prioritized in clinical follow-up due to possible life-threatening complications.3,4 However, gastrointestinal (GI) symptoms, along with urinary and bowel control issues, have the greatest impact on the lives of patients with DM1. 5 Described complaints may vary substantially within and between patients and include dyspepsia, diarrhea, abdominal pain or discomfort, constipation and fecal incontinence.6–12 Currently, the occurrence of GI symptoms in the DM1-population is mainly attributed to affected striated and smooth muscle cells. Striated and smooth muscle cells are found in the whole gastrointestinal tract, which explains the clinical symptoms pallet ranging throughout the whole tract. 7 13–15 GI symptoms are generally attributed to the direct cause of the illness, but can also indirectly flair up due to involvement of the neuroendocrine system.16–18
Although GI-complaints play a large role in the burden of disease for DM1-patients, the course of GI impairment and interaction with muscular symptoms has not yet been fully understood. Studies that have considered the interaction between esophageal and gastric dysfunction, and the degree of skeletal muscle involvement have found little if any correlation.7,8,19,20 However, a relationship between the severity of esophageal and gastric dysfunction, and the duration of skeletal muscle disease have been reported.19,21 Alongside its debilitating impact on patients with DM1, GI impairments may be the first presenting complaints of the disease. 22 In general, GI symptoms develop gradually, leading to adaptation of the patients with little awareness.7,19,23 Consequently, the negative impact of GI symptoms on quality of life, combined with the incomplete understanding of their development in DM1, underscores the need for a psychometrically sound outcome measure.
Currently, there is no golden standard for assessing GI symptoms in DM1 patients. The Gastrointestinal Symptom Rating Scale (GSRS) is a questionnaire that has been developed for assessing gastro-intestinal symptoms in irritable bowel syndrome (IBS) and peptic ulcer disease (PUD). 24 The clinimetric properties of the GSRS have been described well among subjects with dyspepsia, finding acceptable reliability and good internal consistency, but low test-retest reliability in most languages. 25 External validity has been assessed by correlating the GSRS to the 36-Item Short Form Survey (SF-36), Hospital Anxiety and Depression Scale (HADS) and Quality of Life in Reflux and Dyspepsia questionnaire (QOLRAD). 25 The GSRS has been used in several clinical trials, mostly on IBS and PUD, but also in neurologic disorders.26–32 The GSRS assesses outcome measures at ordinal level, based on clinical test theory. 33 This mathematical model, however has several shortcomings. First, ordinal outcome measures do not support parametric testing, therefore sum scores cannot be derived.33,34 Second, it is not possible to compare different questionnaires assessing the same trait. 33 Last, the weight and relevance of the items cannot be assumed to be the same.35,36 Due to these limitations, an alternative model is needed to monitor patients’ outcomes in clinical trials. To overcome these shortcomings, the Rasch measurement model is the most widely used scientific approach.34,37,38 In Rasch-analysis it is attempted to reconstruct ordinal scales into interval level measures.33,37 Because of the need for a validated outcome measure for assessing GI symptoms in the DM1-population, the aim of this study is to evaluate whether the GSRS fits Rasch-model expectation in patients with DM1 and to develop the first disease-specific interval-level outcome measure for assessing GI symptoms in this population.
Methods
Study design
This retrospective study is part of the MYODRAFT registration study, an ongoing longitudinal, observational research collaboration between Radboud university medical center (Radboudumc), and Maastricht University Medical Center + (MUMC). As the designated DM1 expertise centers in the Netherlands, Radboudumc and MUMC + evaluate the majority of patients with DM1. The registry was developed based on recommendations from the 222nd European Neuromuscular Centre (ENMC) workshop in Naarden, The Netherlands, and aims to investigate the natural history of DM1, as well as develop appropriate outcome measures. For the purposes of the current study, GSRS data was retrospectively extracted from the registry. The Medical Ethics Committee of both institutions approved the study (METC 16-4-001, approved on March 18th 2016). Patients with a genetically confirmed DM1 diagnosis were invited to participate after providing written informed consent. The study includes all registered patients from February 15, 2017 to August 23, 2023. All participants underwent standardized assessments by neuromuscular specialist with a specific focus on DM1. Eligible patients were asked to complete multiple questionnaires.
Data collection and questionnaires
Demographic data, medical data, and disease classification were recorded. Patients were classified using the four-category system namely: congenital, childhood, adult and late-onset. The GSRS is a 15-item questionnaire designed to capture the severity and subjective impact of gastrointestinal symptoms experienced during the past two weeks. It covers five symptom domains namely reflux, abdominal pain, indigestion, diarrhea and constipation. 39 The 15 items correspond to the following 15 symptoms respectively: epigastric pain, heartburn, acid reflux, hunger pain, nausea, borborygmus, satiety, eructation, flatulence, constipation, diarrhea, loose stools, hard stools, urgent defecation, incomplete evacuation. A seven-point graded Likert-scale is used, where 1 represents absence of symptoms and 7 represents very troublesome symptoms, thereby capturing both frequency and perceived distress associated with each complaint. 25 A higher score indicates more gastro-intestinal complaints. The questionnaire was administered in clinic by a trained researcher. Patients received standardized instructions prior to completing the GSRS questionnaire. In case of uncertain answer, the patient was instructed to choose an answer that would reflect the clinical state to the best of their personal judgement. In instances where a patient required clarification, a caregiver or family member could assist in interpreting the question. Patients had the option to complete the questionnaire online if in person administration was not feasible.
Statistics
Rasch Unidimensional Measurement Model (RUMM2030) and R Studios version 4.3.2 were used for analysis. We examined Rasch model expectations based on the X2 statistic. The Rasch model evaluates whether an outcome measure fulfills the Rasch model requirements. Rasch analysis was conducted in multiple steps to iteratively refine the measurement model. The model was re-estimated after every modification to the items (e.g., removing misfitting items, splitting for DIF, rescoring categories). The evaluation of the measurement model was based on several criteria: (1) item fit was evaluated using an item-trait interaction using a Bonferroni adjusted chi-square value, or fit residuals exceeding ± 2.5; (2) differential item functioning (DIF) was examined using an analysis of variance (ANOVA) on the residuals of each class interval of person factors, Bonferroni adjustment was used for the significance threshold; (3) threshold ordering was evaluated to ensure that response categories functioned as intended across the latent trait continuum; (4) local dependence was assessed by inspecting residuals correlations, with item pairs exceeding residual correlation of 0.2 were flagged for further review; and (5) dimensionality was assessed through an independent samples t-test with binominal confidence intervals, comparing the location of two item groups with the highest and lowest loadings on the first principal component of the residuals. 40 These steps informed the evaluation of the measurement properties of the scale. Meeting Rasch model requirements allows outcome measures to be converted into an interval-scale instrument. The following subgroups for DIF analysis were introduced: sex (male vs. female), age category based on approximately equal distribution of patients across groups (under 40 years old, 40–60 years old, 60 years or older), diagnosis type (congenital, childhood, adult, late-onset). To ensure stable model estimation, the age category and diagnosis type were further refined to ensure that each subgroup contained at least 50 participants. After the scale meets Rasch model expectations, conversion from an ordinal based scale to interval level data can be conducted. Reliability of the RT-GSRS-DM1 was determined by the Person Separation Index (PSI). A value of 0.7 or higher is considered good but is preferably above 0.9 for discriminatory ability.
Results
Records of 428 DM1 patients were available. Twenty-five subjects were excluded because of missing data, thus leaving 403 records. Demographic and clinical data of the cohort is reported in Table 1.
Overview of demographic- and clinical characteristics of the study cohort.
Step 1: GSRS-01
The pre-phase 15 item GSRS did not meet Rasch model expectations. An overview of the item fit residual statistic, the person fit residual, the item-trait interaction, person separation index and unidimensionality of the initial and final questionnaire can be found in Table 2. Examination of the person-item map indicated that the mean person ability was −1.11 logits, relative to the mean item difficult of 0 logits (Figure 1). Independent t–tests between the two groups of items (5 positively loaded vs. 5 negatively loaded) demonstrated acceptable unidimensionality of the scale. Threshold ordering was examined to evaluate whether the response categories functioned in the intended ordinal manner across the latent trait. Figure 2 indicates how frequently response categories are used. All items showed evidence of disordered thresholds, indicating that respondents are not able to distinguish between adjacent response categories (Figure 3). As a result, all items were rescored from a 7-level Likert scale to a 3-level Likert scale (Figure 4).
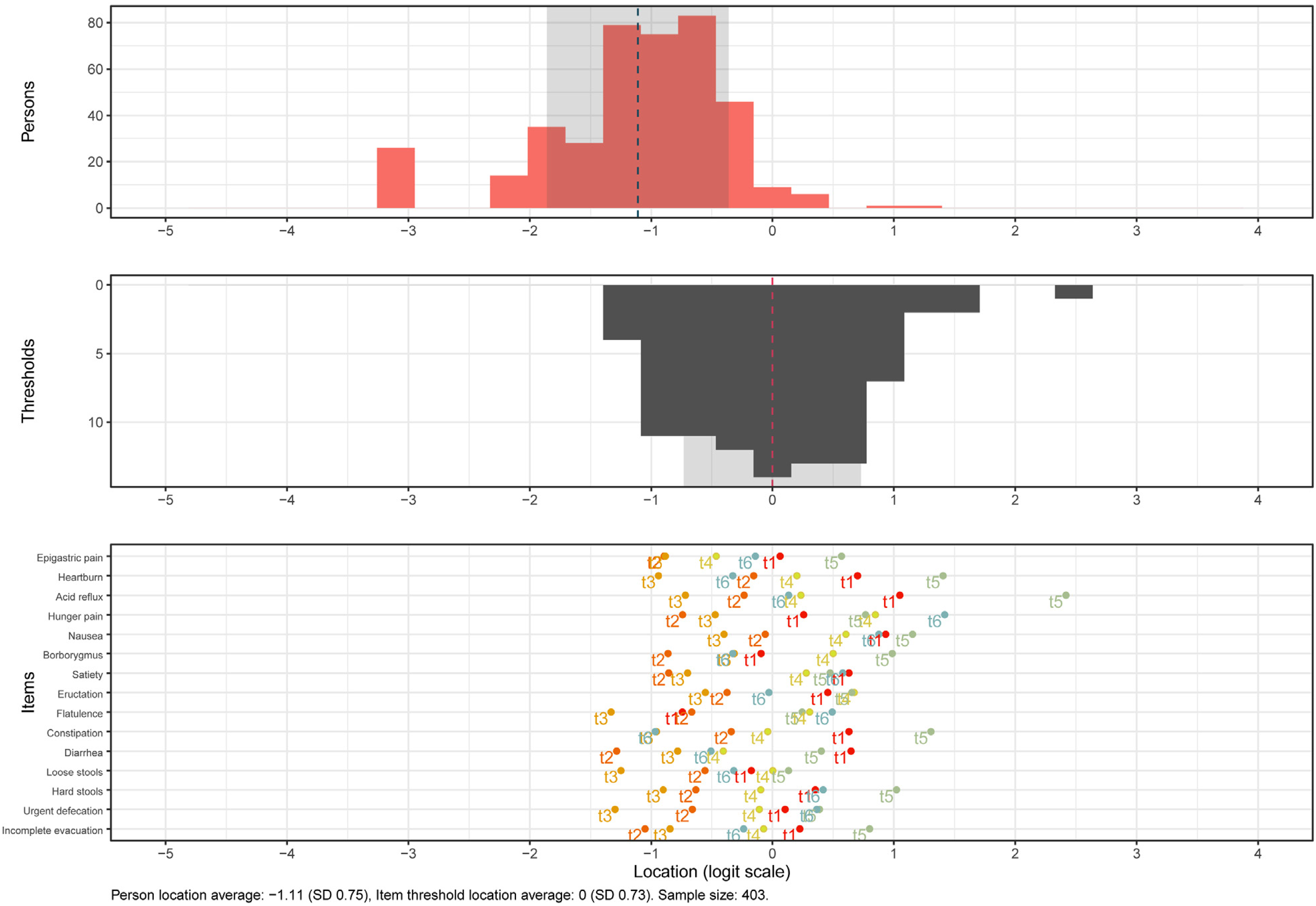
Person-item map of the original scale.
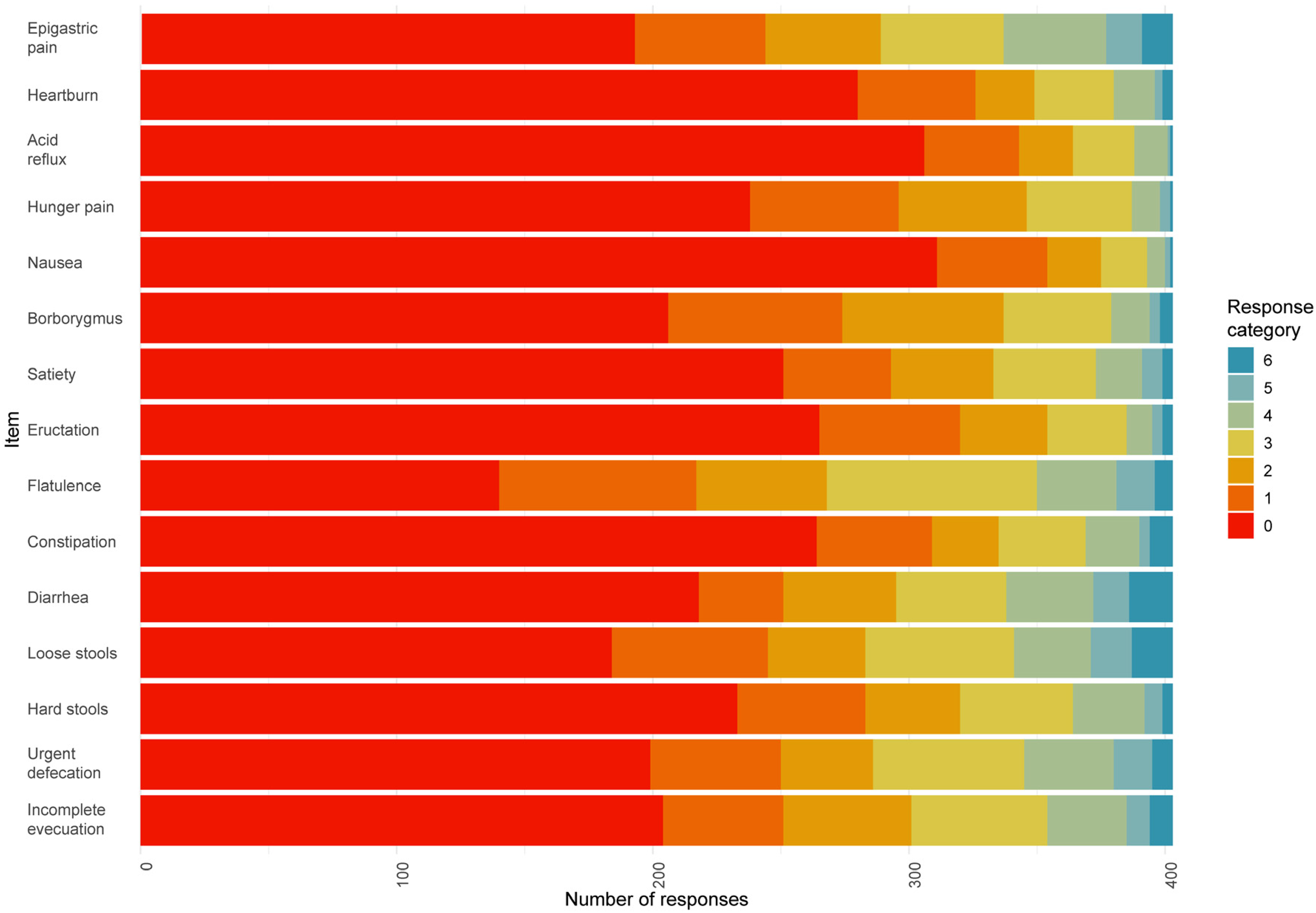
Response distribution per item of the original scale.
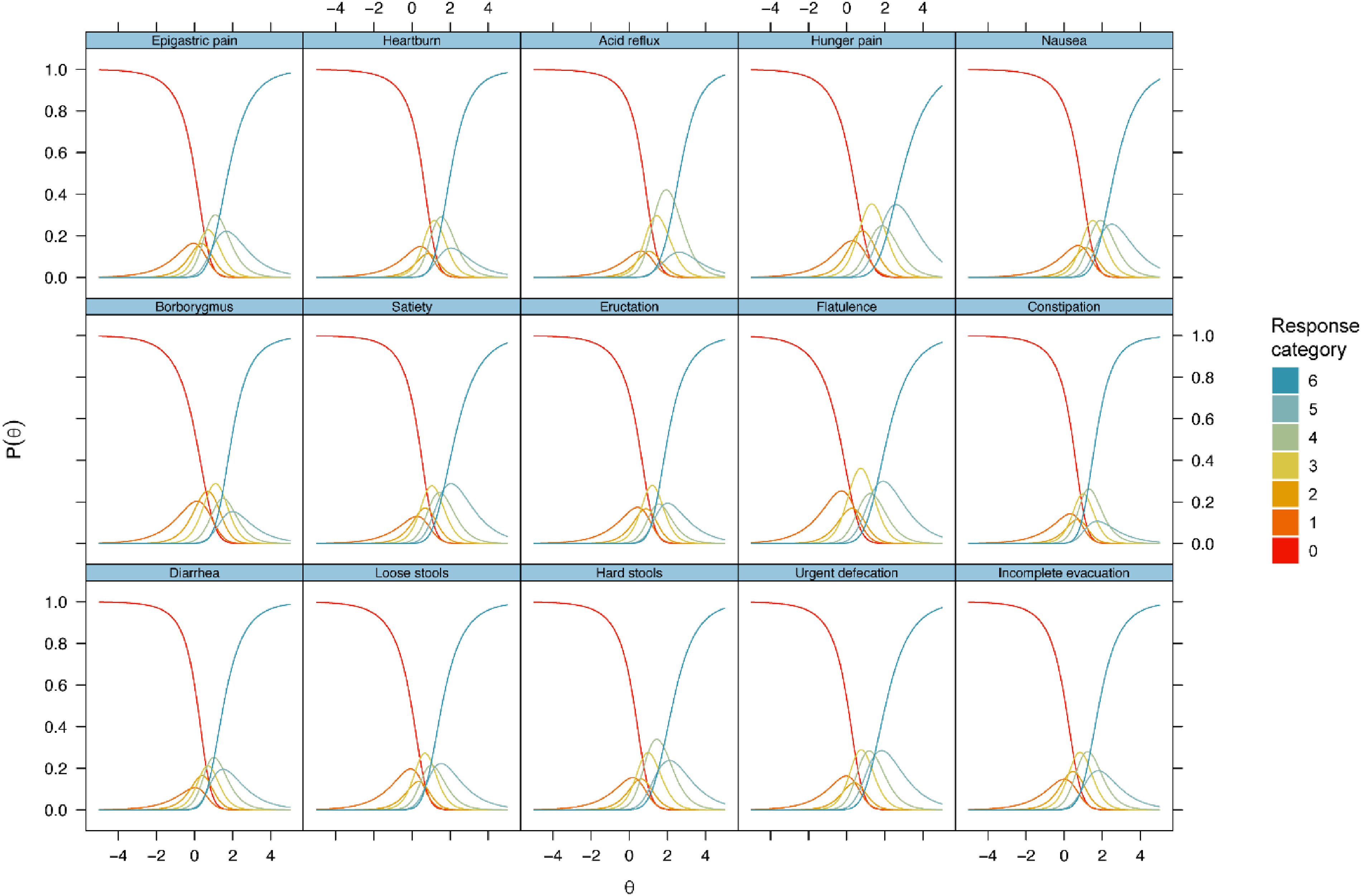
Item probability function before rescoring.
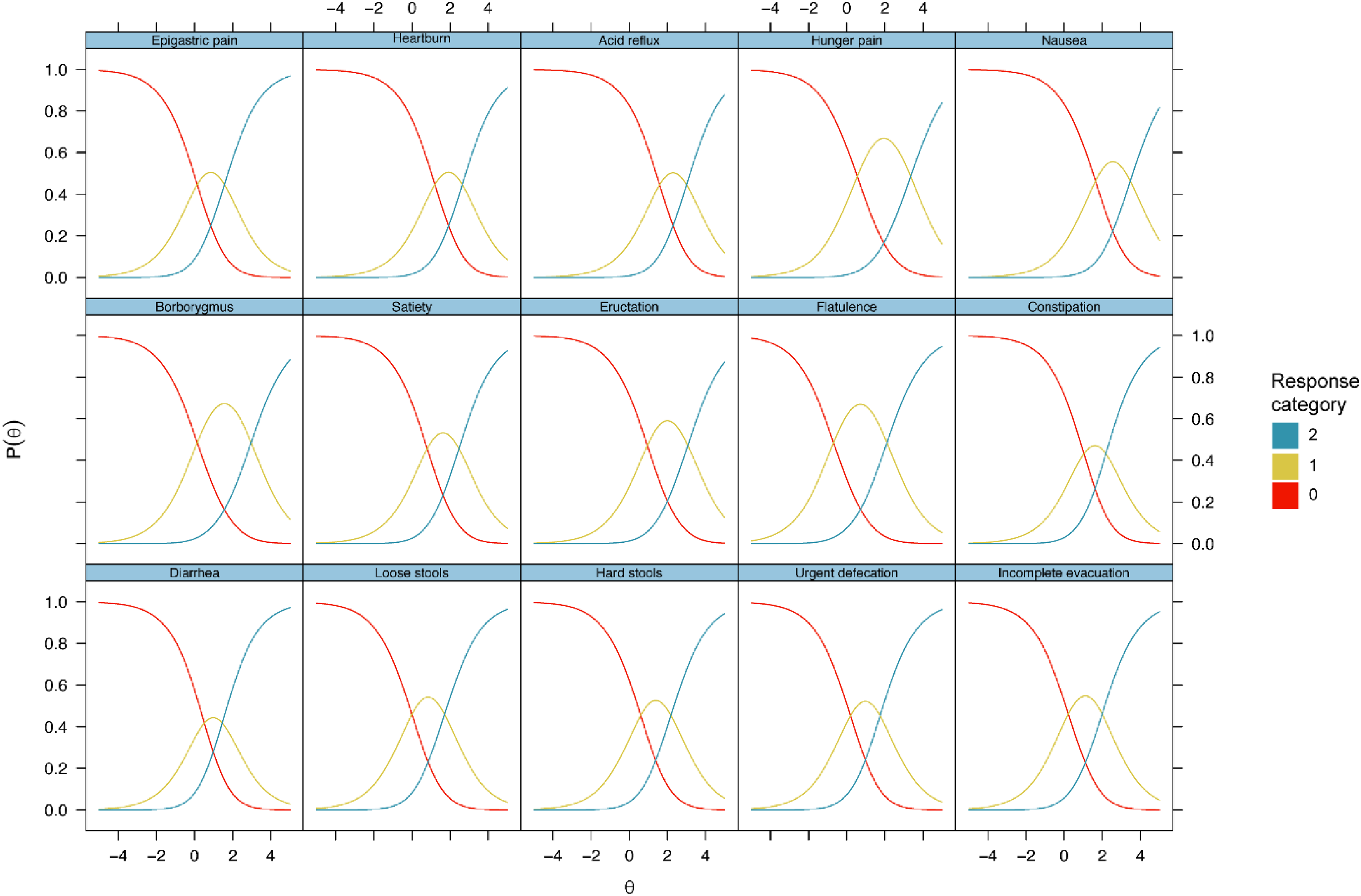
Item probability function after rescoring.
Summary Rasch analyses statistics for RT-GSRS-DM1 construction.
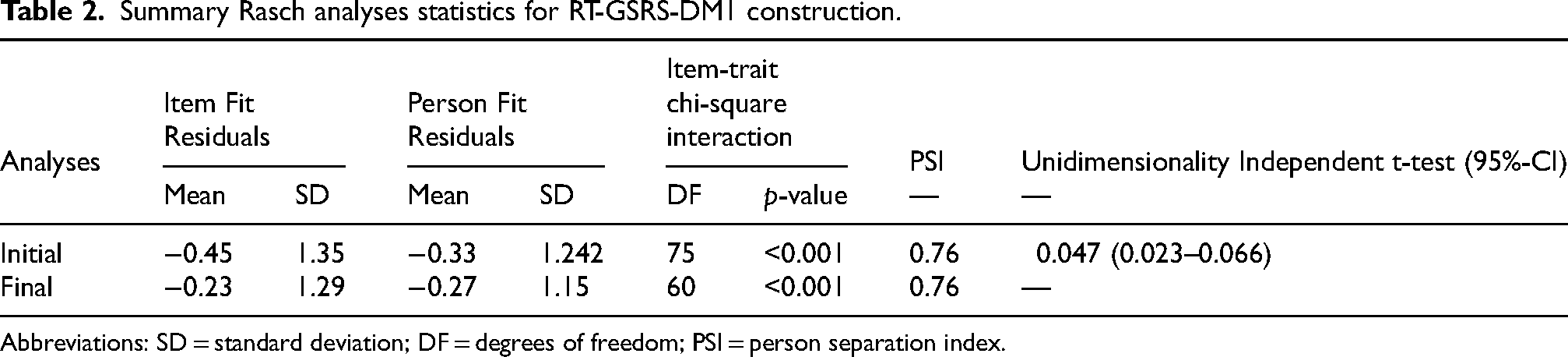
Abbreviations: SD = standard deviation; DF = degrees of freedom; PSI = person separation index.
Step 2: GSRS-02; rescored response options
Item fit analysis indicated that most items fell within the acceptable range for infit measures. However, item 13 (hard stools) demonstrated misfit with a probability below the Bonferroni adjustment. Residual correlation analysis indicated that the following items exceeded the threshold for local independence: item 13 (hard stools) and item 10 (constipation); item 11 (diarrhea) and item 12 (loose stools); and item 2 (heartburn) and item 3 (acid regurgitation). Before deleting items, DIF analysis was conducted to further determine potential misfit. DIF was found for age groups for items 5 and 13. As a result, item 13 was deleted because it showed misfit, local dependence and DIF.
Step 3: GSRS-03; rescored response options, deleted item 13
DIF was found for age groups for item 5. As a result, this item was split between participants under 40 years old and those over 40.
Step 4: GSRS-04; deleted item 13, rescored response options, split items 5 for age category
Item 11 (diarrhea) and item 12 (loose stools) showed significant local dependency. Item 11 (diarrhea) was subsequently deleted.
Step 5 GSRS-04; deleted item 13, rescored response options, split items 5 for age category, deleted item 11
Item 2 (heartburn) and item 3 (acid regurgitation) showed significant local dependency. Item 2 (heartburn) was subsequently deleted.
Step 6: GSRS-04; deleted item 13, rescored response options, split items 5 for age category, deleted item 10, deleted item 2
Item 10 (constipation) showed misfit statistics exceeding the Bonferroni threshold, but was retained due to the clinical relevance of the symptoms. Rasch model expectations were not met in the final 12-item model. The item “flatulence” had the lowest item location, and the item “nausea” had the highest item location. The item difficulty ranged from −0.82 to 1.16 (range 1.98). Patient location ranged from −4.01 to 3.20 (range 7.21) logits.
Discussion
This study provides evidence for the clinimetric validity of the Rasch-Transformed Gastrointestinal Symptom Rating Scale in patients with Myotonic Dystrophy type 1 (RT-GSRS-DM1). Through systematic Rasch analysis, the scale was refined to ensure unidimensionality, consistent threshold ordering, and the absence of item bias related to sex, diagnosis type or age group, supporting its validity as an interval-level measure of GI symptoms. These findings offer insights into how GI symptoms are measured and underscore the inherent complexities in using self-reported symptom scales. Despite refinement, Rasch model expectations were not fully met in the final 12-item RT-GSRS-DM1.
Dimensionality testing within the Rasch model revealed that the 15-item GSRS adhered to unidimensionality assumptions, indicating that all items measured a single latent construct as defined by the scale. This demonstrates that the items collectively capture the underlying construct of GI manifestations, rather than measuring multiple unrelated dimensions simultaneously. This finding supports the internal coherence of the GSRS as a measurement tool. However, it should be noted that while acceptable unidimensionality was reached, not all retained items were locally independent. This indicates that while the assumption of unidimensionality is met, some level of local dependence is inevitable when measuring complex interrelated symptoms.
The original questionnaire exhibits disordered thresholds across all items, suggesting that respondents were unable to distinguish between adjacent response categories on the original 7-point Likert scale. Respondents struggle to distinguish between closely related symptoms, which may suggest that self-reports of GI symptoms are often imprecise and influenced by individual interpretation. As a result, all items were rescored to a 3-point Likert scale. These findings suggest that accurately classifying symptoms is challenging, as patients may struggle to recognize subtle variations in symptom severity.
Another notable finding was the presence of DIF across age categories for item 5 (nausea) and item 13 (hard stools). DIF analysis demonstrated that patients aged 40 years and older responded differently to these items than younger patients, which could indicate that GI symptoms are reported differently depending on the age of the participants. GI symptoms are one of the first symptoms in DM1, and often precede musculoskeletal manifestations. 7 Patients likely experience some degree of habituation and therefore older patients that have experienced gastrointestinal symptoms for a prolonged period might underreport some symptoms. 19 In addition, the observed age-related DIF may reflect heterogeneity in disease phenotype (late- vs early-onset DM1), differences in gut motility with advancing age, or the influence of age-associated factors such as BMI. 41 In response to the observed DIF, we split item 5 (nausea) between age categories. By addressing these issues, this study attempts to ensure that the scale is more consistent across different age groups.
Analysis of fit revealed that most items fell within Rasch model expectation, with an acceptable fit statistic across most items. However, some items did not exhibit good model fit. Item 13 (hard stools) was deleted because it showed DIF, misfit and local dependence with item 10 (constipation). Item 3 (heartburn) was deleted due to its conceptual overlap with item 2 (acid regurgitation). In general reflux symptom epidemiology, heartburn is more frequently reported than acid regurgitation.
42
Expert consensus recognizes both heartburn and regurgitation as the cardinal manifestations of reflux disease
A key limitation of this study is that the removal of conceptually important symptoms may compromise comprehensiveness of the scale. As a result, striking an optimal balance between statistical accuracy and clinical completeness remains a challenge. The original questionnaire was developed for patients with IBS and PUD. 24 As a result, the symptoms of these populations may not overlap with the symptoms of the DM1 population. For example, dysphagia should be considered when addressing the entirety of GI issues related to DM1. Future refinement should involve direct patient input to ensure that the retained items reflect the lived experience of individuals with DM1. This limitation also extends to the evaluation of test-retest reliability, which was not examined in the current study due to its retrospective design. The GSRS has documented low test-retest reliability. Future studies should combine Rasch-based refinements with traditional evaluations of reliability and validity, including patient input, to ensure the retained items accurately capture the full spectrum of gastrointestinal symptoms. Additionally, the GSRS and other questionnaires depend on patient self-report, which is inherently subjective. As previously noted, patients struggle to distinguish between closely related symptoms, and their responses may be influenced by personal interpretation, recall bias, or habituation to chronic symptoms. Furthermore, this study was conducted on a sample of patients from the Netherlands, which may not be representative of the global DM1 population. Cultural, linguistic or healthcare system differences can impact the generalizability of these findings. Additionally, we expect that there may be some inverse dependence present. The questionnaire does not only have overlapping symptoms, but also symptoms that are likely not to co-occur. For example, it would be unlikely that both constipation and diarrhea are present simultaneously. Additionally, motility symptoms vary from day to day, and this could lead to inconsistent symptom reporting. This temporal variability, alongside inverse dependence of certain symptoms, call for caution when assessing the total score of the questionnaire. Future research should consider the full spectrum of GI symptoms, including dysphagia, while accounting for their dynamic and sometimes opposing nature. Last, there is a need to investigate how DM1 patients perceive and report their GI symptoms. The cognitive profile of the DM1 population, alongside habituation to symptoms, may lead to underreporting or mischaracterization of symptoms.
Conclusion
In conclusion, this study highlights the challenges of measuring GI symptoms in DM1. Clinicians and researchers should be aware of the potential limitations with self-reporting GI symptoms. Although the RT-GSRS-DM1 offers an improved method for assessing GI symptoms in DM1 patients, continued efforts are necessary to ensure accurate and comprehensive capture of this disease domain. Incorporating patient input through in-depth interviews will be essential to ensure that gastrointestinal symptom assessment reflects patient-reported experiences and contributes to the development of a disease-specific questionnaire that balances comprehensive coverage with measurement accuracy.
Footnotes
Ethics
The local Medical Ethics Committee of Maastricht concluded that this research falls outside the scope of the Medical Research Involving Human Subjects Act (WMO). Written informed consent was obtained from all patients. The study was conducted in accordance with the Declaration of Helsinki.
Author contributions
L.F. and B.v.V. had full access to all the study data and takes responsibility for the integrity of the data and the accuracy of the data analysis. L.F. and B. v. V. were responsible for conceptualization, methodology, formal analysis, investigation, and writing – original draft., S.v.K., I.M and C.F. were responsible for supervision, and funding acquisition, T.H., and J.C. helped with investigation. All authors contributed to a critical review and editing of the manuscript. All authors approved the final version of the manuscript to be published and agreed to be accountable for all aspects of work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Prinses Beatrix Spierfonds, (grant number W.OR150-25, W.TR19-01, W.TR23-02).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LA. la Fontaine, B.P.A.P. van Veen, T. Hamadeh, J.M. Conchillo and S.M.J. van Kuijk report no competing interests. I.S.J. Merkies received grants from Grifols and Lamepro. Consultancy services for Talecris, CSL, Behring, Novartis, Octafarma, UCB and Argenx. I.S.J. Merkies did not personally benefit financially from these activities. C.G. Faber received grants from the Prinses Beatrix Spierfonds. Consultancy services for Biogen, Vertex, Olipass, and Sangamo. All reimbursements were received by MUMC+. C.G. Faber did not personally benefit financially from these activities.