
Abstract
Congenital disorders are a significant contributor to neonatal intensive care unit (NICU) admissions and neonatal mortality, adding to substantial healthcare costs and emotional burden for families. The introduction of rapid next-generation sequencing (NGS), also known as massively parallel sequencing (MPS), in the NICU has advanced neonatal care by enabling rapid and precise diagnoses. This review explores various NGS technologies utilized in the NICU, their clinical utility, and their role in newborn screening (NBS). It also highlights several challenges hindering its widespread adoption. Addressing these barriers will require a combined effort from all the different stakeholders to ensure fair and responsible integration of NGS into neonatal care.
Introduction
Genetic disorders are estimated to contribute to approximately 13–30% of NICU admissions. 1 They are also a significant cause of neonatal morbidity and mortality, responsible for up to one-third of neonatal deaths.1,2 Beyond their medical complexity, these conditions also result in prolonged hospital stays and high financial burdens. 3 On average, the cost of NICU care for a newborn with a genetic diagnosis exceeds that of other neonates by approximately $250,000. 4 The broader economic impact is more challenging to measure, but historical estimates suggest billions of dollars are spent annually on genetic conditions during childhood. 5 In addition to monetary strain, families experience significant emotional distress, which cannot be quantified in financial terms.
Among these, neuromuscular diseases (NMDs) represent a key subset of these disorders, which often present with nonspecific hypotonia. Hypotonia is a common finding among infants admitted to the NICU and may be the sole presenting symptom of an underlying neuromuscular disease. These infants frequently undergo a long diagnostic odyssey and require prolonged hospitalization; hence, early consideration of genetic testing is recommended. 6 In a multicenter retrospective study of 147 infants with unexplained hypotonia, 54% had hypotonia as the primary clinical finding, while 46% had hypotonia as part of a multisystemic presentation, such as seizures or other congenital anomalies. Of those who underwent rapid exome or genome sequencing, 60% received a molecular diagnosis. 7 This highlights the diagnostic value of genomic sequencing for neonates with neuromuscular presentations.
Diagnosing genetic conditions in newborns is particularly challenging due to their diverse clinical presentations. The presentation can range from hypotonia, seizures, a single anomaly, to multiple malformations or more subtle features that are difficult to recognize, especially in preterm infants. 1 Traditionally, the diagnostic process was slow and followed a stepwise approach, often delaying definitive diagnoses and targeted interventions. However, advances in genomic sequencing have transformed this landscape. NGS has expedited the diagnostic process, providing faster and more accurate results. Rapid whole exome or genome sequencing (rWES/rWGS) has proven especially valuable in critical care settings, enabling timely interventions that can reduce morbidity and mortality.8–11 Additionally, they can play a crucial role in guiding end-of-life decisions, offering families essential information for future reproductive planning and providing reassurance during a difficult time.
These advancements continue to enhance diagnostic accuracy, improve treatment strategies, and support data-driven clinical decision-making, ultimately improving outcomes for neonates with genetic conditions. An overview of sequencing approaches and their clinical indications in the NICU is summarized in Figure 1.
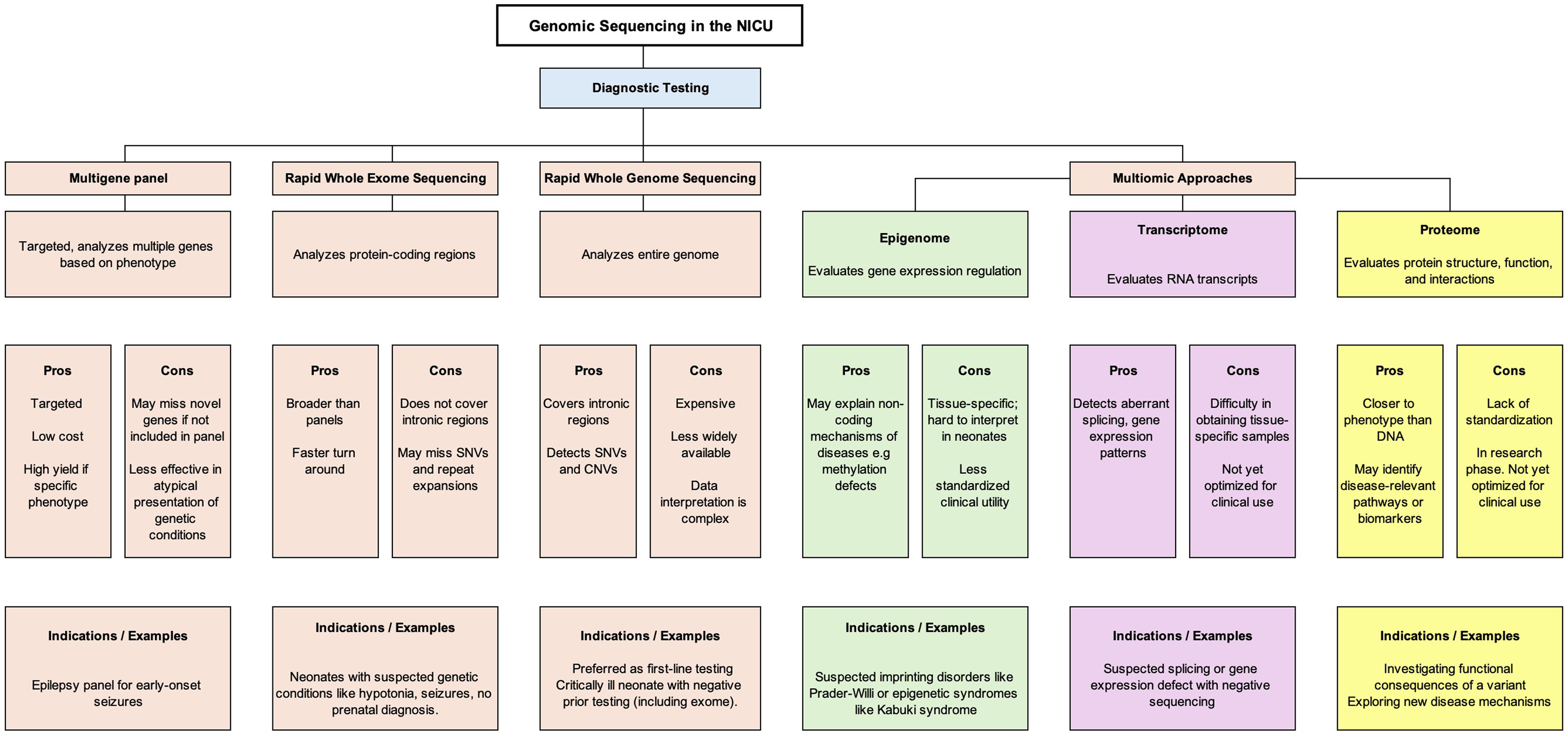
This figure summarizes diagnostic genomic and multi-omic approaches in the NICU, comparing their targets, advantages, limitations, and clinical indications to guide test selection based on the clinical context.
Next-Generation sequencing (NGS): platforms and technologies
NGS encompasses several technologies that enable the parallel, massive, and simultaneous sequencing of large genomic regions while being fast, accurate, and relatively affordable. While rWES/rWGS have transformed neonatal diagnostics, their performance depends on the sequencing platforms used.
Short Read Sequencing (SRS): Generates reads ranging from 50 to 300 base pairs. Methods such as sequencing by synthesis (SBS) and sequencing by binding (SBB) replicate DNA fragments to determine the nucleotide sequence within a sample. 12 This approach is ideal for many routine genetic applications due to its scalability and cost-effectiveness.
Long Read Sequencing (LRS): Used by platforms like PacBio and Oxford Nanopore, sequences a much longer stretch of DNA ranging from thousands to millions of base pairs in a single pass.13,14 It is also beneficial for identifying complex structural variations. Beyond standard genomic applications, it also offers epigenomic profiling. LRS can directly read native DNA without amplification or bisulfite conversion, making it possible to detect methylation marks in real-time. It also enables analysis of chromatin structure and methylation footprints with single-molecule precision, revealing epigenetic diversity that bulk short-read methods may miss. These capabilities make long-read technologies a powerful tool not only for genomics but also for comprehensive epigenetic research. 15
Depending on the clinical presentation and urgency, NGS technologies can support a range of clinical applications, such as targeted gene panel testing and rapid whole genome or exome sequencing, as discussed in the subsequent section.
Targeted gene panel testing
Targeted multigene panels examine multiple genes simultaneously and are helpful when a patient presents with a specific clinical feature, such as seizures or hypotonia. Depending on panel design, targeted sequencing can also detect copy number variants (CNVs) and interrogate challenging genomic regions such as triplicated segments. 16 This is particularly relevant for significant genes like TTN and NEB, frequently implicated in congenital myopathies. 17 While they are relatively cost-effective and can detect single-nucleotide variants (SNVs) and small insertions or deletions (indels) in up to a few hundred known disease-associated genes, they have notable limitations. These panels may miss newly discovered genes or genes not traditionally linked to the presenting phenotype, especially in cases with atypical clinical features., A recent GEMINI (The Genomic Medicine in Ill Infants and Newborns) study found that genome sequencing had a higher diagnostic yield (49%) compared to targeted panels (27%). 18
Rapid and ultra rapid whole exome or genome sequencing (rWES/rWGS)
rWES and rWGS are now first-line genetic tests for critically ill infants.6–20 While WES focuses on approximately 2% of the genome, primarily coding regions, WGS sequences the entire genome, including non-coding regions. WGS provides a more comprehensive analysis, detecting single-nucleotide variants (SNVs), copy-number variants (CNVs), small insertions or deletions, and chromosomal or mitochondrial abnormalities. 21
rWES and rWGS typically provide diagnostic results within 5–7 days, while ultra-rapid genome sequencing (URGS) refers to methods that can reliably deliver results in less than 3 days of receiving the sample. 8 In the NICU, diagnostic yield ranges from 19–75%, depending on patient population and clinical indication.10,22–29 Yield is highest in trios where both parents are sequenced. Turnaround times have significantly improved over the past decade, from 50 h for the fastest reported rWGS result in 2012 to as little as 5 h at Stanford University22,30
Globally, the adoption of rapid sequencing has accelerated, with impressive diagnostic yields reported across multiple countries. In China, the diagnostic yield reported was 69.6%. 31 In contrast, Poland has reported 72.2%, 32 and Australia has demonstrated an overall yield of 51%, with the highest yield 56% seen in NICU patients. 33 France, Belgium, and the Netherlands have reported yields of 49%, 57.5%, and 50%, respectively.34–36 These findings highlight the growing impact and clinical utility of genomic sequencing in the NICUs across the globe. Building on this, emerging multi-omic technologies such as epigenomics, transcriptomics, and proteomics are further expanding diagnostic precision.
Multi-omic approaches
Epigenetic sequencing
Epigenetic sequencing assesses chemical changes to DNA, such as methylation, histone modifications, and chromatin remodeling, that influence how genes are expressed. The whole-genome bisulfite sequencing (WGBS) maps DNA methylation at single-base resolution across the genome. 37 Another method, Chromatin Immunoprecipitation Sequencing (ChIP-seq), identifies DNA regions associated with specific histone modifications or DNA-binding proteins by sequencing fragments isolated through targeted antibodies. 38
Tools like the EpiSign classifier use DNA methylation patterns to help diagnose neurodevelopmental disorders by comparing patient profiles to an extensive reference database. EpiSign currently screens for over 90 genetic conditions, including imprinting and repeat expansion disorders, and can detect alterations in epigenetic regulation and other cellular processes.39,40 In a study of 207 patients, primarily pediatric patients, EpiSign provided a diagnostic result in 27.6% of cases, with a higher yield in those with prior inconclusive findings. 41 Ongoing large-scale efforts like EpiSign-CAN aim to evaluate the clinical utility of methylation testing as a first-line diagnostic tool in rare diseases. 42 These methods are increasingly used to complement genome sequencing, particularly in neurodevelopmental and imprinting disorders.
RNA sequencing
RNA sequencing (RNA-seq) adds value to DNA-based genetic testing by revealing how genes are expressed and regulated, especially in response to disease or environmental factors. 43 In a prospective study of 34 neonates in the NICUs with suspected genetic conditions, rWES provided a diagnosis in 41% of cases within an average of 8.6 days. When RNA-seq was added for cases where rWES was inconclusive, the overall diagnostic rate increased to 47%. 44 A Canadian study evaluated patients with pediatric-onset complex neurological conditions likely caused by a genetic disorder. In this group of 22 patients from 20 families, combining RNA-seq with rWGS led to a confirmed diagnosis in an additional 25% of cases. 45 This highlights how transcriptomic data can resolve otherwise inconclusive DNA-based testing.
Proteomics
While genomics reveals an individual's underlying genetic makeup, proteomics offers a dynamic view of how proteins change in response to disease or genetic conditions. With advances in proteomics technology, there is growing potential to discover new disease-specific biomarkers. A recent study by Hock et al. described an untargeted mass-spectrometry-based proteomics pipeline for ultra-rapid diagnosis of rare disorders. 46 Most studies are based on small sample sizes, emphasizing the need for further research in this area. 47 Nevertheless, proteomic and metabolic profiling may soon extend precision diagnostics beyond the genome.
Clinical applications and impact
Identifying the right NICU candidates for genomic sequencing is crucial for balancing over-testing and under-diagnosis. Studies like SeqFirst-Neo have demonstrated that using broad, simplified exclusion criteria, rather than strict inclusion rules, can promote equitable access to testing. 48
The American College of Medical Genetics (ACMG) defines clinical utility as a test's ability to influence medical management, provide prognostic information, offer psychological benefits to families, or reduce healthcare costs.
49
In critically ill infants, genomic sequencing has yielded diagnoses in 12–75% of cases and led to management changes in 13–60%
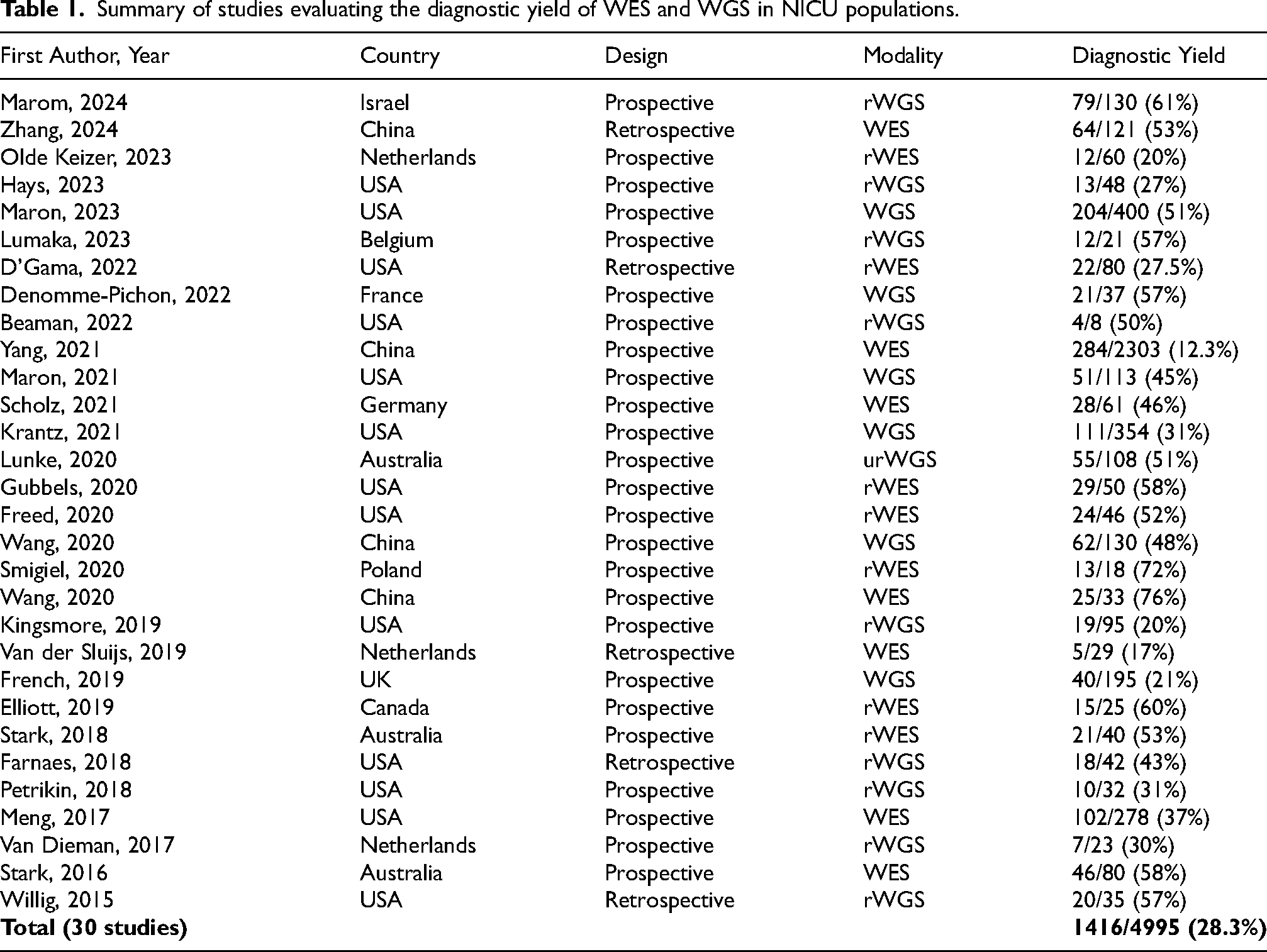
A summary of key studies is provided in Table 1. Across 30 studies, genomic sequencing identified a molecular diagnosis in 1416 of 4995 neonates (28.3%)
Summary of studies evaluating the diagnostic yield of WES and WGS in NICU populations.
Over the past decade, the declining cost of genomic sequencing has expanded its clinical use, yet financial and insurance barriers persist. Despite these limitations, multiple studies show that early implementation of rWGS can shorten hospital stay and reduce healthcare costs. For instance, Farnaes et al. reported cost savings of $800,000—$2,000,000 in critically ill infants diagnosed via rWGS, primarily due to management changes. 3 Similar cost-effectiveness has been confirmed in other NICU studies.3,51
Although the clinical and economic benefits of genomic sequencing are increasingly evident, implementation in NICUs remains challenging
Challenges and barriers of incorporating genome sequencing in the NICU
Widespread implementation faces hurdles, including difficulty interpreting results, limited access in low-resource settings, and high costs. Initiatives like Project VIGOR (Virtual Genome Center) have been developed to expand genomic care in safety-net NICUs through remote consultation and training. 52
Ethical and legal considerations also need to be addressed, particularly regarding parental consent and the management of incidental findings, which may cause unnecessary stress for the results. Financial considerations also play a role, as many insurers remain hesitant to cover the cost of genomic sequencing for critically ill infants due to questions about its clinical utility and cost-effectiveness. A collaborative effort among stakeholders, including healthcare providers, policymakers, and ethicists, is necessary to ensure the responsible and equitable integration of genomic sequencing in neonatal care.
The role of genomic sequencing in newborn screening (NBS)
Newborn screening, a public health program to screen babies for various potentially treatable disorders using tandem mass spectrometry, is increasingly being supplemented with individual gene sequencing. More recently, genomic sequencing is gaining recognition as a powerful tool for comprehensive newborn screening. 53 The utility of rWES/rWGS versus a panel of genes with potentially effective therapies is an active area of research that continues to be studied. 54 For example, Kingsmore et al. reviewed 457 genetic conditions and found that 85% had effective treatments, making them strong candidates for inclusion in newborn screening panels. To evaluate the potential of genomic screening at a population level, they applied a simulated newborn screening model using rWGS data from 454,707 individuals in the UK Biobank. The model demonstrated a high specificity of 99.7% and a sensitivity of 88.8% in detecting individuals with pathogenic or likely pathogenic variants, supporting the feasibility and accuracy of genomic approaches for early detection of treatable conditions. 55
The BabySeq project was one of the first randomized trials to explore the impact of integrating genomic sequencing into the care of both healthy and sick newborns. 56 In this study, newborns and their families were randomized to receive either standard newborn screening alone or standard screening with genomic sequencing. BabySeq demonstrated that genomic sequencing could identify unanticipated but actionable genetic variants and influence medical management, Building on this, more recent large scale initiatives, such as The Generation Study in the UK, the Genomic Screening Consortium for Australian Newborns (GenSCAN) in Australia, and the pilot Newborn Genetic Screening Program in the UAE, seek to sequence the genomes of healthy newborns-marking a significant shift toward universal genomic screening.54,57–59 However, as these novel technologies are introduced, they must be implemented with care to ensure they do more good than harm, especially in vulnerable or underrepresented populations.
While genomic sequencing offers transformative potential, its integration into standard newborn screening presents several challenges. Many genetic variants remain poorly understood, which can lead to ambiguous or misleading results. There are also significant ethical and legal concerns, including consent, data privacy, and potential discrimination based on genetic findings. Additionally, successful implementation requires trained personnel to conduct testing, interpret results, and provide genetic counseling. Standardization of sequencing methods, data interpretation, and reporting is also crucial to ensure consistency across laboratories. 60
Another challenge is the need for long-term follow-up systems to manage individuals diagnosed with genetic conditions. The psychosocial impact of genomic findings on families, particularly regarding late-onset conditions, is not well understood and requires further study. Moreover, equitable access remains a concern, as socioeconomic and geographic disparities may limit access to genomic sequencing, exacerbating existing healthcare inequities. 61
Evaluating the cost-effectiveness of genomic sequencing is another complex issue. The vast number of genetic conditions that can be identified, along with the corresponding interventions, complicates economic modeling. Genomic sequencing has the potential to revolutionize newborn screening by enhancing detection capabilities and identifying conditions missed by traditional biochemical methods. However, integrating this technology into routine healthcare will require addressing ethical, logistical, and economic challenges.
Conclusion
Genomic sequencing is shifting neonatal medicine, offering unprecedented opportunities for early and accurate diagnosis of congenital disorders. Integration of rWES/rWGS into NICU has significantly improved diagnostic yield, leading to timely and targeted medical interventions. Despite these advancements, several barriers impede the widespread adoption of genomic sequencing in NICUs. Challenges such as interpretation difficulties, ethical and legal considerations, cost constraints, and inequitable access must be addressed through continued research, policy development, and improvements in healthcare infrastructure. There is a need for standardizing sequencing methodologies, increasing genomic literacy among clinicians, and determining sustainable financial models to ensure equitable access to genomic sequencing. The role of genomic sequencing as a neonatal screening tool also needs further study, with many ethical, financial, and implementation issues that need to be addressed.
Footnotes
Acknowledgements
The authors have no additional acknowledgments to declare.
Consent for publication
Not applicable
Author contributions
S.S.A drafted the manuscript and the figure. P.B.A. edited and reviewed the manuscript and figure. Both authors approved the final version of the manuscript for publication.
Funding
This work was supported by NIH R01-HG011798-04 and the Because of Bella Foundation to P.B.A.
Because of Bella Foundation, National Human Genome Research Institute, (grant number NIH R01-HG011798-04 ).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
This review article does not contain any primary data collection, and therefore, no new data were generated or analyzed as part of this study. The article is based solely on a comprehensive literature review of existing publications, which are cited within the text.
Statements and declarations
Not applicable