
Abstract
Background
Exercise-based rehabilitation is an integral aspect of chronic condition management. However, the traditional in-person delivery of rehabilitation to condition-specific groups limits service accessibility. This study examined the feasibility of a disease-agnostic physiotherapy-led telerehabilitation programme for people with various chronic conditions.
Methods
A mixed-methods single-arm feasibility trial was conducted examining the feasibility of the Telerehabilitation and Exercise for Chronic Conditions (TECC) programme for people with chronic conditions, a disease-agnostic physiotherapy-led telerehabilitation programme. The 6-week programme comprised weekly physiotherapy-led synchronous group exercise sessions, weekly synchronous education sessions, and a social component, all delivered via videoconferencing. Asynchronous recordings were also made available. Primary outcomes included recruitment, retention, adherence, satisfaction, adverse events, and participant experiences via focus groups.
Results
Sixteen participants were enrolled during the 4-week recruitment period, with 14 commencing the intervention. Eleven participants (68.8%) were retained at follow-up. The mean number of participants who attended the synchronous exercise, education, and social sessions were 7 (50.0%), 5.2 (37.1%), and 1.3 (9.3%), respectively. No serious adverse events were reported. High satisfaction levels (93.8%) with the overall TECC programme were expressed by those who completed the programme. The TECC programme was an acceptable and beneficial experience for participants.
Conclusions
The TECC programme can be a feasible, pragmatic rehabilitation delivery method. However, attendance was poor, and the social component was of limited interest. Intervention amendments and refinements are necessary to improve participant attendance and adherence before progressing to more expansive delivery and evaluation.
Trial Registration
ClinicalTrials.gov (NCT06388499).
Introduction
Chronic conditions impose a significant burden on individuals, society, and healthcare systems worldwide.1–3 These conditions typically require long-term management leading to increased health service utilisation, healthcare costs, death and disability rates, and reduced quality of life and function levels.4,5 Chronic conditions will continue to pose a persistent challenge to our healthcare services in the future given their increasing prevalence and our ageing population.6–8
Engagement with exercise-based self-management rehabilitation programmes empowers patients to independently manage their health and wellbeing, reducing health service utilisation and expenses.9–12 Previous research has shown that these programmes are effective for a range of chronic populations, increasing participants’ physical function and quality of life.13–15 While evidence supports the efficacy of these programmes, they are traditionally delivered in clinical settings and can be costly, time-consuming, and inaccessible for many individuals.16–19 This often results in poor uptake and engagement levels.20,21
The delivery of rehabilitation remotely using telecommunication technologies such as videoconferencing, emails, telephone calls and recorded videos, also known as telerehabilitation, offers a promising alternative healthcare service delivery method. This convenient, cost-effective service delivery method could potentially increase accessibility to, and engagement with, rehabilitation.22–25 In addition to this, telerehabilitation is non-inferior to traditional in-person rehabilitation for improving clinical outcomes in various chronic populations, and participants report high levels of satisfaction and positive experiences following engagement with these programmes.22,26–28
Previous research exploring telerehabilitation has focused on condition-specific programmes such as pulmonary telerehabilitation delivered specifically to people with chronic respiratory diseases. However, the structure and content of rehabilitation programs for various chronic populations are strikingly similar, typically consisting of progressive resistance and cardiovascular exercise training as well as educational material focused on health management, despite the variances in underlying diseases.12,29 Disease-agnostic programmes, delivered to groups of people with different chronic conditions, could be a more pragmatic service delivery method allowing for economies of scale and increased clinician flexibility by optimising resource utilisation, improving efficiency, and providing more flexible care to a diverse population.30–33 Disease-agnostic programme delivery could reduce the challenges of staff shortfalls leading to gaps in service delivery by encouraging clinicians to be flexible and expand their knowledge to a broader range of populations, thus reducing the reliance on specialised expertise for specific conditions. 34 Recent evidence supports the development of disease-agnostic programmes catering for a wide range of chronic conditions.30,31,35 However, this previous research has focused on traditional in-person delivery of these programmes. Therefore, we aim to examine the feasibility of a disease-agnostic physiotherapy-led exercise-based telerehabilitation programme for people with a range of chronic conditions, known as the Telerehabilitation and Exercise for Chronic Conditions (TECC) programme. The primary aim of this study is to examine the feasibility of the intervention by examining recruitment and retention, adherence, adverse events, and satisfaction with the intervention. A secondary aim is to examine the effect of the intervention on physical function and quality of life.
Materials and methods
Design
A mixed-methods single-arm feasibility trial was conducted to examine the feasibility of the TECC programme for people with chronic conditions. This study was conducted and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement extension for pilot and feasibility trials. 36 Ethical approval was granted by the Health Service Executive (HSE) Southeastern Area Research Ethics Committee in Ireland. The trial protocol was previously registered on ClinicalTrials.gov (NCT06388499) and Open Science Framework. 37 The protocol was reported in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist. 38
Development of the TECC programme
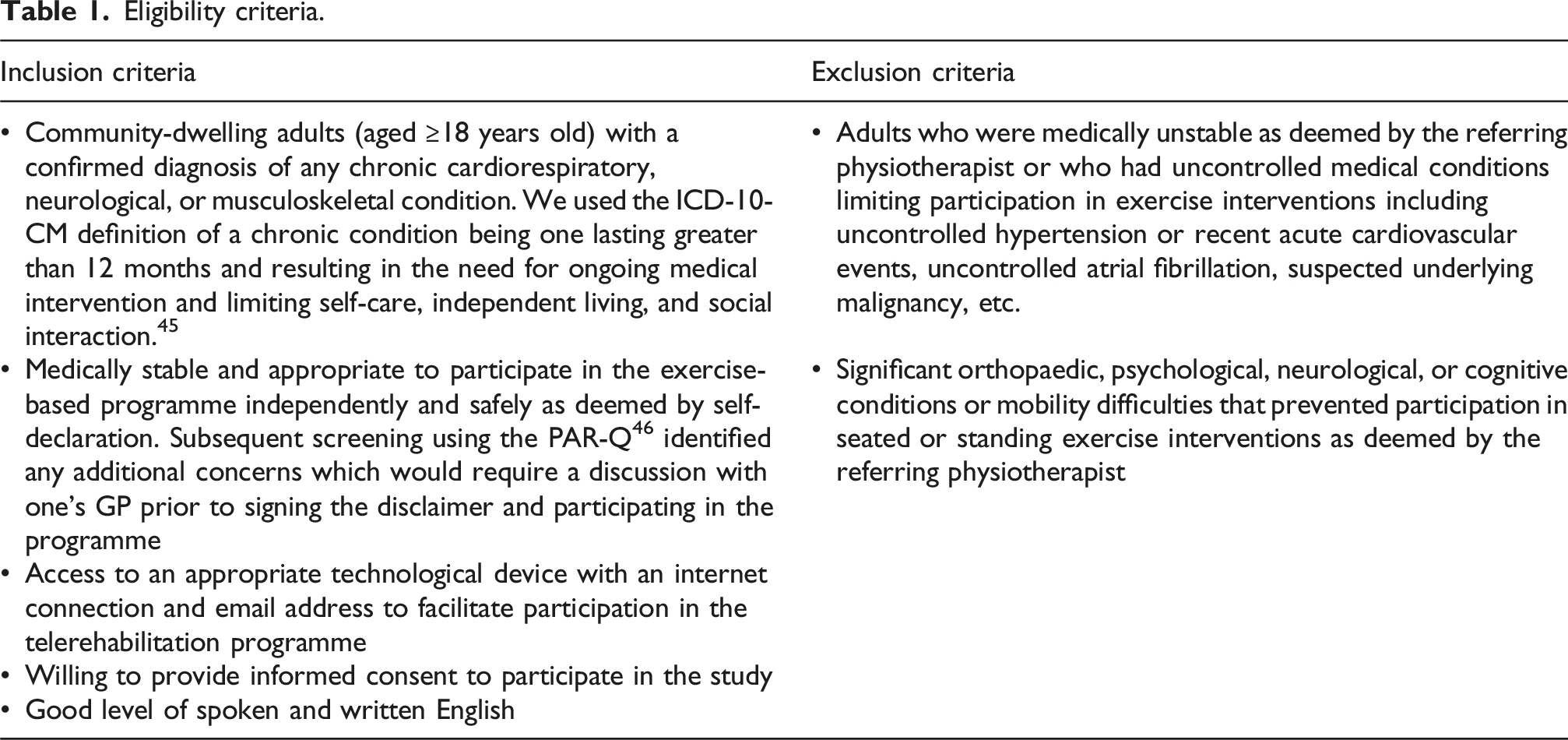
Eligibility criteria.
Participants and setting
Adults with various chronic conditions, including chronic cardiorespiratory, neurological and musculoskeletal conditions, were informed of the study by treating physiotherapists from community sites in Ireland and the networks of the research team from April to May 2024. An outline of the study was provided and those who expressed interest in participating were screened for eligibility based on the pre-defined criteria (Table 1) by the research team.
Study schedule diagram.
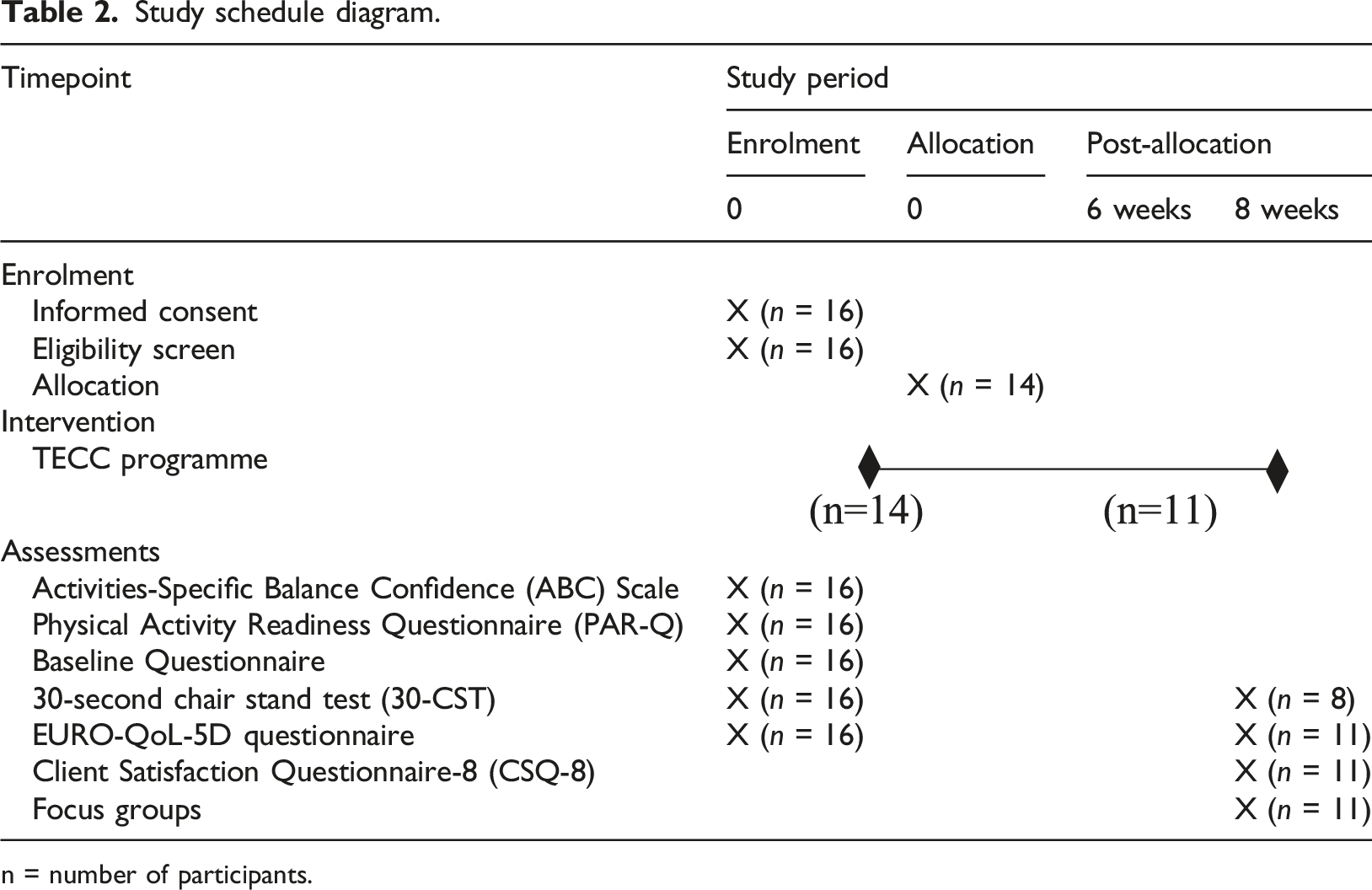
n = number of participants.
Intervention
The TECC programme comprised of a 6-week disease-agnostic exercise-based telerehabilitation programme for people with chronic conditions delivered by a chartered physiotherapist. The programme has been described using the TIDieR (Template for Intervention Description and Replication) checklist to ensure good reporting and intervention description 49 (Supplemental File 5). The programme consisted of weekly synchronous exercise sessions followed by a social component, and synchronous educational webinars to promote self-management of health and well-being. Recordings of the exercise and education sessions were made available to participants each week via email. Participants were advised to perform additional exercise sessions at their own convenience to supplement the synchronous exercise sessions and facilitate adherence to physical activity guideline recommendations. Participants were advised to record any engagement with the recorded exercise and education sessions via electronic self-report logbook (Supplemental File 6).
Exercise component
Synchronous group exercise sessions led by a physiotherapist, were delivered weekly via videoconferencing using Microsoft Teams software. The exercise sessions included a 10-minute warm-up, 30- to 40-minute main exercise session which included resistance, aerobic, balance and flexibility training, and a 5-minute cool down. We initially planned to deliver the exercise sessions to two exercise group levels based on baseline functional mobility levels. It was planned that one group would perform seated-based exercises while the other group would perform standing-based exercises. Allocation to either exercise group was based on the ABC scale score with participants scoring below the threshold of 67% allocated to the seat-based exercise group. 50 However, based on the ABC scale scores, all participants enrolled in this trial were allocated to the standing-based exercise group. Therefore, the planned seated-based exercise class was not required. Exercises were instructed and demonstrated by a physiotherapist with instructions for suitable regressions and progressions for each exercise also provided. Participants were informed of the use of the BORG RPE Scale 48 before the programme to guide appropriate exercise intensity during exercise performance. Participants were encouraged to exercise at an intensity of 11–14 on the BORG RPE scale during the exercise sessions.
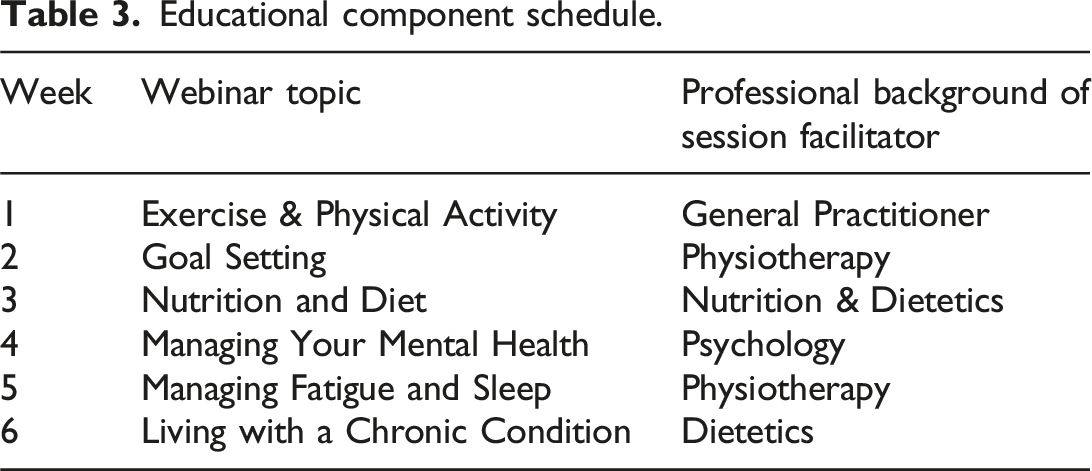
Educational component
Educational component schedule.
Social component
At the end of each weekly synchronous group exercise session, participants had the opportunity to engage in a 10- to 15-minute synchronous online social interaction with other participants in the group via videoconferencing. The social component could be guided by the research team with theme-driven discussions based on the educational topics explored in the webinars, or unregulated and left to participants to discuss subjects of their choice.
Data collection
Primary outcomes
Measurement method for each outcome of interest.
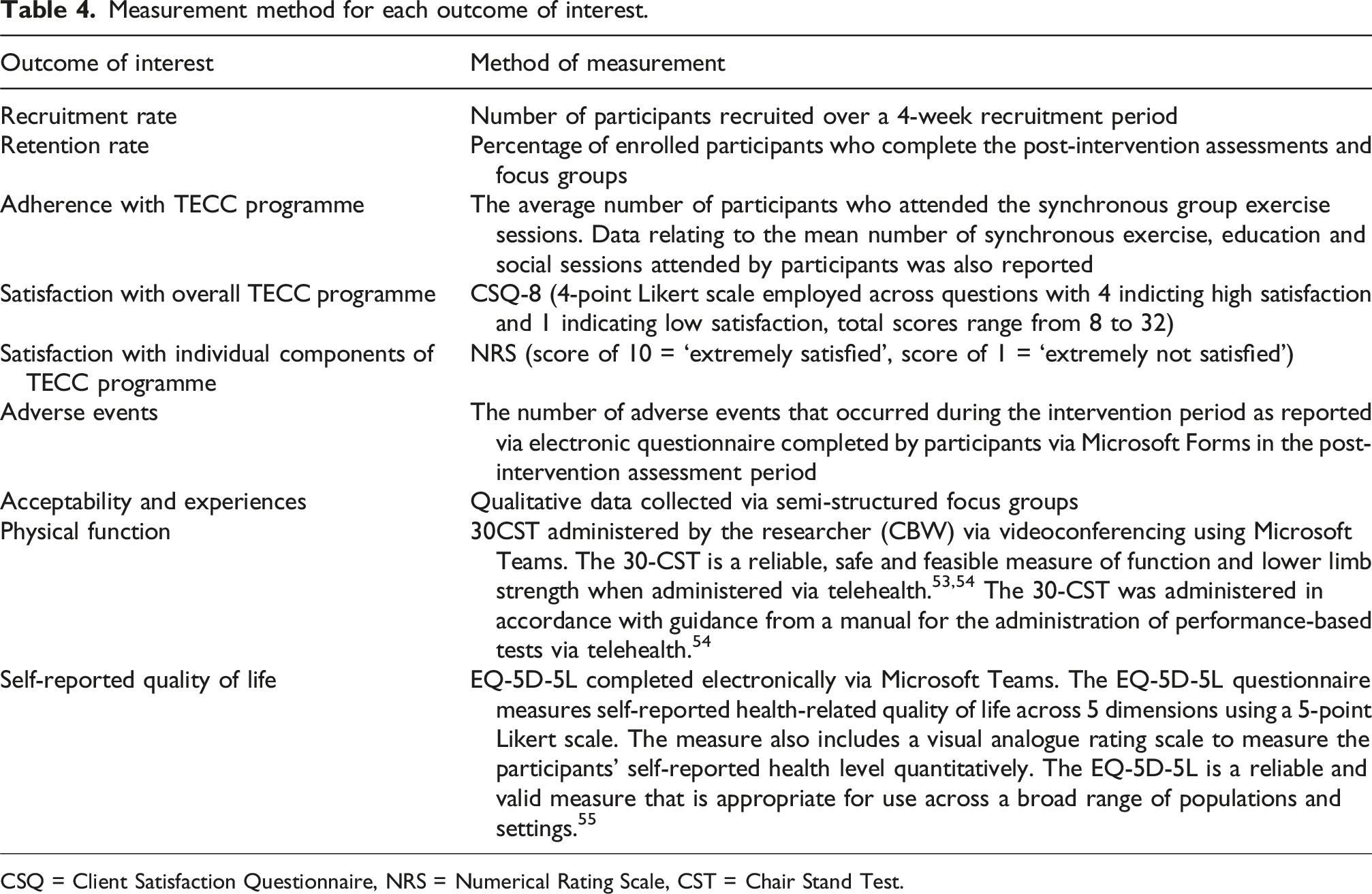
CSQ = Client Satisfaction Questionnaire, NRS = Numerical Rating Scale, CST = Chair Stand Test.
Qualitative data relating to participant experiences was collected using semi-structured focus groups which were conducted via videoconferencing using Microsoft Teams during the post-intervention period. Two focus groups were conducted by the primary author (CBW) with five and six participants in each group (female n = 7, male n = 4). Both groups lasted approximately 40 minutes. The questions were informed by an interview guide which was based on the research and clinical experience of the authors (Supplemental File 7). The interview guide included open-ended questions to explore the participants’ experiences participating in the TECC programme. Focus groups were recorded and automatically transcribed using Microsoft Teams software.
Secondary outcomes
The secondary outcomes of interest related to the clinical impact of the programme, including changes in self-reported quality of life and objective physical function, following the TECC programme (Table 4).
Statistical analysis
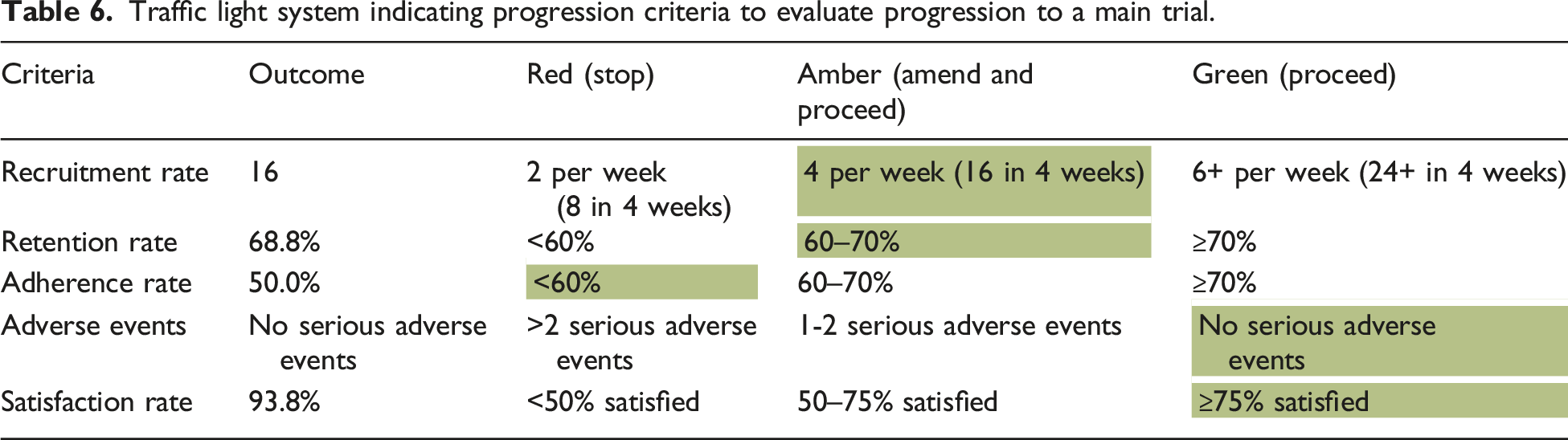
Descriptive statistics were used to describe the characteristics of the participants at baseline using proportions, percentages, ranges, means and standard deviations. Visual plots and the Shapiro-Wilk test of normality were used to assess numerical data for skewness. Primary feasibility and adherence outcomes were reported using proportions and were also evaluated using a traffic light system as reported in the feasibility trial protocol. 37 The traffic light system includes red (stop until solutions found), amber (amend and proceed) and green (proceed) thresholds which indicate progression criteria to evaluate progression to a main trial. 53 A preliminary analysis of clinical outcomes involved evaluating mean differences (with associated 95% confidence intervals) between pre-and post-intervention scores. Paired t-tests were conducted to calculate the significance of the results. Data analysis was conducted using SPSS software (v29.0.2.0) and supported by Microsoft Word and Excel for organisation and storage.
Qualitative data analysis was conducted using open inductive coding through line-by-line reading of the transcripts of the focus groups using the principles of grounded theory. Focus group data was video recorded and transcribed using Microsoft Teams software. The first author (CBW) checked the transcripts and edited minor errors relating to sound quality and accent variation, by comparing the transcripts to the video recordings. Transcripts were sent to participants to ensure accuracy and participants were invited to send any comments or edits to the research team within 1 week of receiving the transcripts. The transcripts were initially reviewed by CBW to familiarise with the data. Transcripts were then coded by CBW to identify themes. Microsoft Word and Excel software was used to facilitate data analysis, organisation and storage.
Results
Primary outcomes
Recruitment and retention
Participant characteristics.
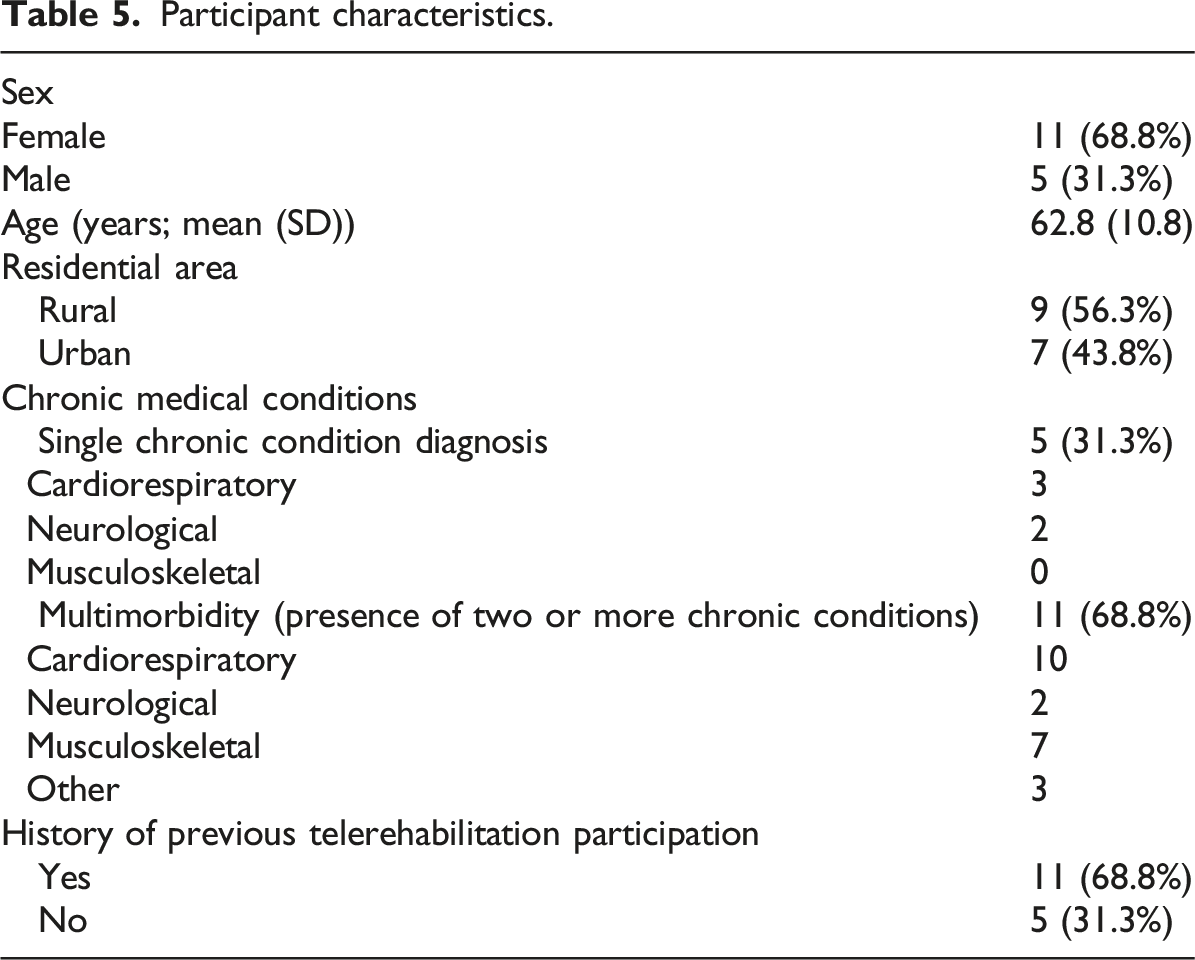
Two individuals withdrew from the study before commencing the programme due to medical reasons (including an exacerbation of a neurological condition). Three individuals withdrew from the study during the intervention phase for personal and medical reasons (including family bereavement and exacerbation of respiratory and musculoskeletal conditions). Three participants were unable to complete the post-intervention 30CST outcome measure due to medical reasons (including two acute musculoskeletal injuries that occurred independent of the intervention and one hospital admission due to an acute respiratory infection). A total of 11 participants (n = 7 female, n = 4 male), of the 16 who enrolled, (68.8%) completed the 6-week intervention, post-intervention CSQ-8 and EQ-5D-5L measures and focus groups.
Adherence
All participants who commenced the programme attended the orientation session before commencing the intervention. Attendance rates are detailed in Supplemental File 8. The mean attendance rates at each of the synchronous exercise, education, and social sessions were 7 (50%), 5.2 (37.1%), and 1.3 (9.3%) participants, respectively. The recordings made available to watch asynchronously were viewed by several of the 14 participants who commenced the intervention (exercise recordings n = 10 (71.4%); education recordings n = 7 (50%)). The mean (SD) number of asynchronous exercise sessions completed by participants each week was 2.2 (1.8). The mean (SD) rate of perceived exertion reported by participants for exercise sessions completed throughout the intervention was 13.7 (1.6) equating to a ‘somewhat hard’ level of perceived exertion.
Of the 14 participants who commenced the programme, the mean number of synchronous exercise sessions attended per participant was three sessions out of a total of six synchronous exercise sessions (50%). Two participants (14.3%) did not attend any synchronous exercise session and subsequently withdrew from the programme. Three participants (21.4%) attended 1-3 synchronous exercise sessions, while the remaining eight participants (57.1%) attended four or more synchronous exercise sessions. The mean number of synchronous education sessions attended per participant was 2.2 sessions out of a total of six synchronous exercise sessions (36.7%). Five of the 14 participants (35.7%) did not attend any synchronous education sessions, with two of these subsequently withdrawing from the programme. Six participants (42.9%) attended 1-3 synchronous education sessions, and three participants (21.4%) attended four or more synchronous education sessions. The mean number of synchronous sessions attended per participant, including both exercise and education sessions, was 5.2 sessions out of a total of 12 synchronous sessions (43.3%). The mean number of optional social component sessions attended per participant was 0.6 sessions out of a total of six (10.0%). Seven of the 14 participants (50.0%) did not attend any of the social component, while the remaining participants (n = 7) (50.0%) attended 1-3 social sessions out of a total of six sessions.
Satisfaction
The CSQ-8 was completed by 11 participants following programme completion. The responses to the CSQ-8 are shown in Supplemental File 9. Total scores ranged from 24 to 32. The total mean score was 30 (SD = 2.4), equating to a rate of 93.8% satisfaction with the overall TECC programme (See Supplemental File 9).
Supplementary File 9 outlines the participant satisfaction levels with each of the programme components. Participants reported high satisfaction levels with the orientation sessions, exercise, and education components, each scoring more than 8/10 on the NRS. However, a low level of satisfaction (3.6/10 NRS) with the social component was reported.
Adverse events
There were no serious adverse events reported by participants in the post-intervention questionnaire. One participant reported some minor knee joint discomfort while performing the exercises included in the programme. As stated previously, three participants withdrew from the study during the intervention phase due to personal and medical reasons that were independent of the TECC programme. Three participants who completed the programme were unable to complete the post-intervention 30CST measure due to medical reasons which were also independent of the programme.
Criteria to evaluate progression to a main trial
Traffic light system indicating progression criteria to evaluate progression to a main trial.
Qualitative focus group feedback
The main themes identified from the qualitative focus group data include: 1. Shared aims; 2. Telerehabilitation perceptions; 3. Programme evaluation; and 4. Recommendations for change.
Shared aims
Participants were asked about their experience of participating in a disease-agnostic programme which included a group of participants with various chronic health conditions. Since most had participated in condition-specific rehabilitation programmes such as pulmonary rehabilitation previously, this disease-agnostic programme for a mixed-condition group was a novel experience. All participants, however, expressed no initial concerns about participating in a programme with a mixed-condition group, and noted that they did not encounter any related issues while participating in the programme. Both the exercise and education components of the programme, according to the participants, applied to them and met their needs. PT-08: ‘I will say initially it (mixed-condition group) was sort of novel because anything I've done similar to this before has all been geared towards COPD that I have. But I didn't have any problem with it, it made no odds (difference) once the exercises that you (facilitator) had put together were suitable for each of the different conditions that people had’. PT-13: ‘To me personally, it didn't matter really. I didn't know what was wrong with people, what conditions they had, it didn't really matter’.
Participants expressed that, although variations in their underlying medical conditions existed, all participants were striving towards the same goal of enhancing their overall health and well-being. Participants expressed appreciation for the variety of content covered in the educational component, noting that many of the topics covered would ‘apply to everyone across the board’ (PT-10). PT-03: ‘Yeah, I just found we were all on the same aim trying to keep ourselves well. So, it was nice. And I don't think it really mattered what (condition) you had; we were all on the same goal’. PT-10: ‘so many, many things overlap and we're all getting older, there are so many things that apply to you as you age that apply to everyone across the board. I thought they (education sessions) were brilliant’.
Telerehabilitation perceptions
Most participants expressed that they would be satisfied to participate in a similar programme again in the future, indicating that they had a positive experience with the remote online telerehabilitation programme. Some expressed their initial concerns about using technology, and a few participants encountered challenges with technology throughout the programme. All participants did, however, affirm that this would not stop them from taking part in telerehabilitation in the future. It was recognised that participation was facilitated by the support provided by the service provider and family members. After participating in the programme, the participants stated they felt more comfortable using technology. PT-11: ‘my concern was the technology and being able to access it online and I wouldn't be au fait with a lot of the technology, and I did say to (facilitator) that there was once or twice I wasn't able to get on and but within seconds I emailed (facilitator) and she had it sorted for me. So, for me that was really helpful and now I'd like to think that I'm a bit more au fait with the technology’. PT-01: ‘We can pass on the word now to say that the online works and don’t be afraid of it, embrace it’.
The majority of the group emphasised how practical and convenient the telerehabilitation programme was, especially with regard to the accessibility of the asynchronous recorded content. The programme's flexibility and the ability to access the content at any time and location were appreciated by participants. There was also discussion on the advantages of the synchronous content. Participants stated that they were motivated to engage with the programme due to the structured nature of the synchronous sessions. PT-08: ‘… having the online from the comfort of your home, if it's raining you don’t have to worry about getting out somewhere or sitting in traffic for half an hour’. PT-01: ‘The big thing for me is the recordings…when you’re doing the exercises, if you’re a bit under pressure, you can pause it, you can go back to it whenever you feel like it…you can do your few little jobs, then you come back and you can continue exercising, which is much more beneficial, I think, than being in a class where you have to get everything done within the hour. So, the recordings are great, that's what I found really good’.
Programme evaluation
Participants listed several benefits of participating in the program, and generally expressed satisfaction with the experience. Self-reported physical benefits included improved breathing, and increased strength and energy levels. Some participants reported the exercise component was challenging but manageable, while participants valued the options to modify exercises with regression and progression options to suit their individual needs. It was also observed that the BORG rate of perceived effort scale was helpful in guiding the intensity of the exercise component to cater for individual needs. PT-02: ‘I find if I'm sitting in the chair, and when I stand up, I find it easier to stand up. I'd be grunting before, but I do less grunting now and stand-up kind of better and easier’. PT-03: ‘I really enjoyed it, I felt stronger and felt more energetic while I was doing it’.
Participants reported that the education component provided them with a deep understanding of the value of lifestyle modifications and self-management strategies. Participants also cited some practical ‘hints and tips’ which they gained from the educational sessions which they have since incorporated into their lives to self-manage their health and wellbeing. PT-11: ‘The one thing I think the Doctor who talked the first week and it just seems to be sticking in my head is he talked about exercise snacking. And that’s been, if I’m standing doing the dishes or cooking, going up on my heels and back down, they (exercises) don’t have to be in the chunks that the little ones can also help. So, for me, that was a great suggestion’. PT-08: Well, that's one of the things I found about all the (education) talks there was something practical in all of them.
Recommendations for change
Poor engagement with the social component of the programme was noted. This was attributed to factors including time limitations, social anxiety, and fear related to the discussion of their medical conditions. Participants offered suggestions to improve this component of the programme in the future including a group introduction session prior to commencing the programme or exercise session, and increased support from the programme facilitator to encourage social interaction among the participants. Some participants noted that they prefer to socialise in-person, and they would rather use the telerehabilitation programme for the exercise and education components rather than for social purposes. PT-08: ‘I have to say, I probably felt a little bit anxious about the talks (social component) that I didn't actually join in any of them, but it coincidentally I just had stuff on at the same time. So, it was simple for me to say, look great, thanks, good luck, see you again’. PT-03: ‘Yeah, to me if I'm picking the time for exercise… I'm always making extra lists for myself and jobs that I need to do, but I didn't really have time for the chats, I did well to do the exercise’.
To promote individual, unsupervised exercise performance between the group synchronous sessions, some participants also suggested the availability of a visual print-out of the exercise sessions. There were no further recommendations for enhancements to the education or exercise components of the TECC programme.
Secondary outcomes
Secondary outcomes pre- and post-intervention.

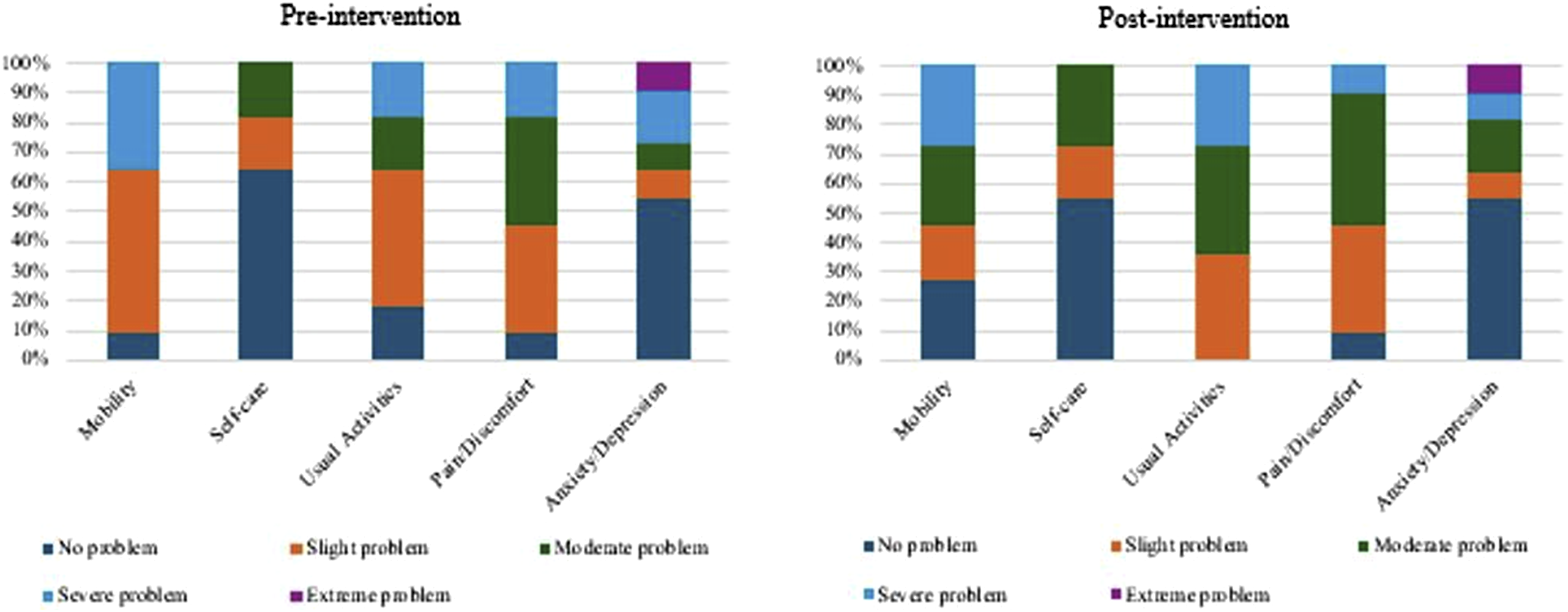
EURO-QoL-5D-5L outcomes pre- and post-intervention.
Discussion
This study examined the feasibility of the TECC programme, a disease-agnostic physiotherapy-led exercise-based telerehabilitation programme for people with chronic conditions. This study also included a preliminary evaluation of the clinical effectiveness of the programme.
Our findings indicate that the TECC programme is feasible and acceptable among participants; however, our results also suggest that some amendments to the programme are necessary before progressing to a main trial. The recruitment rate did not meet the pre-set thresholds and desired sample size outlined in the trial protocol. 37 However, this trial adopted a pragmatic proof of concept approach. Therefore, participants were recruited promptly within a narrow recruitment period and pathway over 4 weeks by physiotherapists in a limited number of clinical settings. The recruitment pathway should be broadened for future trials and an extended recruitment period could enhance recruitment rates. The retention of participants who commenced the intervention phase and progressed to complete the post-intervention assessments was satisfactory, thus showing promise for a future, more expansive intervention and trial.
The adherence rate, as measured by synchronous exercise session attendance, did not meet the a priori traffic light system thresholds that we set in the study protocol. 37 It is important to note that this adherence rate was based on the mean attendance at the synchronous group exercise sessions only. Perhaps attendance with the synchronous group exercise sessions was poor due to the availability and convenience of the asynchronous recorded sessions. Most participants reported some engagement with the asynchronous recorded content including both the recorded exercise and education sessions. This reinforces the value of including both synchronous and asynchronous content which has been previously cited by people with chronic conditions. 39 However, due to inconsistent engagement with the self-reported logbook and incomplete recording, it is difficult to accurately report adherence to the asynchronous recorded content. Some participants engaged in other exercise rehabilitation classes during the intervention period which may also have contributed to the poor attendance rate at the synchronous group exercise sessions. Therefore, the adherence rate reported for comparison with the traffic light system threshold should be interpreted with caution. Future research should evaluate adherence to the asynchronous programme content to include a more accurate representation of participant adherence to the overall programme. Consideration should also be given to intervention amendments that could engage participants more effectively and improve participant attendance. A largely positive, enjoyable, and beneficial experience was reported by those who participated in the telerehabilitation programme. The programme was also safe, with no serious adverse events reported, convenient and flexible.
Furthermore, a preliminary evaluation of the clinical effectiveness of the TECC programme demonstrated evidence of improvements in objective physical function following participation. However, evidence of improvements in self-reported quality of life was not observed. Although further evaluation would be needed to establish the clinical efficacy of the programme, results from the initial evaluation are promising.
Participant satisfaction with the TECC programme was remarkably high. The orientation video call, exercise, and education components were reported by participants to be particularly useful and enjoyable. However, despite previous research promoting the inclusion and importance of opportunities to facilitate social interaction during telerehabilitation programmes, 39 the social component of the TECC programme was reported to be substantially less useful for participants. This was reflected by the poor uptake and engagement with the social component during the programme with 50.0% of participants not attending any social session and the remaining participants attending less than half of the social sessions. The qualitative data suggests that this was attributed to various factors such as time limitations and participant fear and anxiety regarding the nature of the social interaction. This mirrors previous findings of Cahalan et al. 54 who also reported poor attendance at the optional social component of a telehealth intervention because of similar reasons. Previous qualitative findings of Barry Walsh et al. 39 highlighted participants’ desire for the inclusion of a social component within telerehabilitation programmes. However, this research was completed shortly after the COVID-19 pandemic, a time when there was limited opportunity for in-person social interaction due to cocooning and social distancing requirements. Perhaps now that in-person social events and activities have recommenced as usual, people can engage in social activities elsewhere and no longer desire these opportunities to be included in telerehabilitation programmes. Proposed improvements to the social element of the TECC programme such as the inclusion a group introduction session prior to commencement of exercise sessions, or increased support from the programme facilitator to encourage social interaction, should be explored with potential participants in advance of any such amendments.
Overall, the encouraging findings from this study endorse previous literature supporting the convenience, feasibility, acceptability and clinical effectiveness of telerehabilitation interventions for a wide range of chronic populations.22,26,55,56 Additionally, the present study adds a novel finding to the existing research suggesting that these positive results are also obtained with the delivery of a disease-agnostic telerehabilitation programme to a mixed-condition group. Furthermore, our research shows that this method of healthcare service delivery to a heterogeneous group is acceptable among people with chronic conditions. Previous evidence suggests that disease-agnostic programmes for people with various chronic conditions have the potential to maximise resource utilisation allowing for greater economies of scale when compared to traditional rehabilitation service delivery methods focusing on condition-specific populations. 18 Given the increasing prevalence of chronic conditions and particularly the increasing incidence of multimorbidity (the co-occurrence of two or more chronic conditions), 57 our results are promising and may encourage this novel and pragmatic approach to healthcare service delivery which may help to manage the increasing challenges and demands being placed on our healthcare services.
There are some limitations to this research that should be acknowledged. The sample size included in this study was relatively small and did not reach the target sample size set in the trial protocol. 37 However, the sample included participants diagnosed with a wide variety of chronic conditions spanning chronic cardiorespiratory, neurological and musculoskeletal conditions. Based on the ABC scale scores all participants were allocated to the standing-based exercise group, therefore the planned seated-based exercise class was not required. Furthermore, some of the included participants were unable to complete the post-intervention physical function assessments due to medical reasons; therefore. the number who completed the assessments of physical function was smaller. Some participants engaged in other exercise rehabilitation classes during the intervention period. Data relating to engagement with the asynchronous content was collected through self-report by participants. However, participant logbook records were inconsistent and largely incomplete, undermining the accuracy of adherence rates reported. The primary author was involved in programme delivery and data collection. Therefore, this data may have been subject to an increased risk of bias due to the lack of blinding.
The results of this preliminary evaluation are encouraging and suggest that the TECC programme is safe and satisfactory and progression to further evaluation may be warranted. However, amendments and improvements must first be made to improve recruitment, retention and adherence rates before progression to a main trial. Our findings are promising and indicate that this novel method of rehabilitation service delivery for people with chronic conditions could potentially be a pragmatic, viable, and effective approach to healthcare service delivery.
To our knowledge, this is the first original research study exploring the feasibility of a disease-agnostic physiotherapy-led exercise-based telerehabilitation programme for people with chronic conditions. While further evaluation is needed, our initial evaluation suggests that the TECC programme is a safe and acceptable intervention. However, participant attendance and adherence to the programme was poor. Therefore, consideration needs to be given to solutions and intervention amendments that focus on improving the recruitment and retention of participants and their adherence to synchronous content. The social component was of limited interest and was poorly attended by participants. Improvements to this component of the intervention also need to be considered. The results serve as a foundation for the future development of telerehabilitation interventions. Further amendments and progressive refinement of the programme need to be considered before embarking on a full-scale evaluation. 58
Supplemental Material
Supplemental Material - A physiotherapy-led disease-agnostic telerehabilitation programme for people with chronic health conditions: A mixed-methods feasibility trial
Supplemental Material for A physiotherapy-led disease-agnostic telerehabilitation programme for people with chronic health conditions: A mixed-methods feasibility trial by Caoimhe Barry Walsh, Roisin Cahalan, Niamh Julian, Rana S. Hinman, and Kieran O’ Sullivan in Physiotherapy Practice and Research
Footnotes
Acknowledgements
The authors would like to thank those who participated in this study for their contributions, gatekeepers at recruitment sites for their contribution and support with participant recruitment, and the healthcare professionals involved in the delivery of the educational component of the TECC programme.
Ethical approval
Ethical approval was granted by the Health Service Executive (HSE) Southeastern Area Research Ethics Committee. All participants provided informed consent via electronic consent forms.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Health & Medical Research Council Investigator Grant (#2025733), Irish Research Council (GOIPG/2022/1854).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.