
Abstract
A paradigm shift has occurred in the role and organization of laboratory diagnostics over the past decades, wherein consolidation or networking of small laboratories into larger factories and point-of-care testing have simultaneously evolved and now seem to favorably coexist. There is now evidence, however, that the growing implementation of continuous-flow automation, especially in closed systems, has not eased the identification of hemolyzed specimens since the integration of preanalytical and analytical workstations would hide them from visual scrutiny, with an inherent risk that unreliable test results may be released to the stakeholders. Along with other technical breakthroughs, the new generation of laboratory instrumentation is increasingly equipped with systems that can systematically and automatically be tested for a broad series of interferences, the so-called serum indices, which also include the hemolysis index. The routine implementation of these technical tools in clinical laboratories equipped with continuous-flow automation carries several advantages and some drawbacks that are discussed in this article.
Errors in Laboratory Diagnostics
A paradigm shift has occurred in the role and organization of laboratory diagnostics over the past decades, which has been mainly driven by biological discoveries, incessant implementation of novel diagnostic tests within diagnostic reasoning, remarkable technological advances, and economic pressures.1,2 All these forces have paved the way to a revolution in the laboratory environment, wherein consolidation or networking of small laboratories into larger factories and decentralization of some tests (i.e., point-of-care testing) at bedside, physician offices, pharmacies, supermarkets, and other health care facilities have simultaneously evolved and now seem to acceptably coexist.3,4 Contextually with these radical changes, the quality throughout the total testing process has improved in parallel, with a substantial reduction in vulnerability and error rates. Nevertheless, laboratory diagnostics is still not the safe enterprise it is supposed to be, and errors may occur at an estimated frequency of ~0.3% of all tests performed. 5 Although most of them are not associated with adverse health care outcomes, in ~20% of cases, they might generate further inappropriate investigations or increase health care expenditure, whereas in up to 6% of cases, they might also jeopardize patient safety. 6
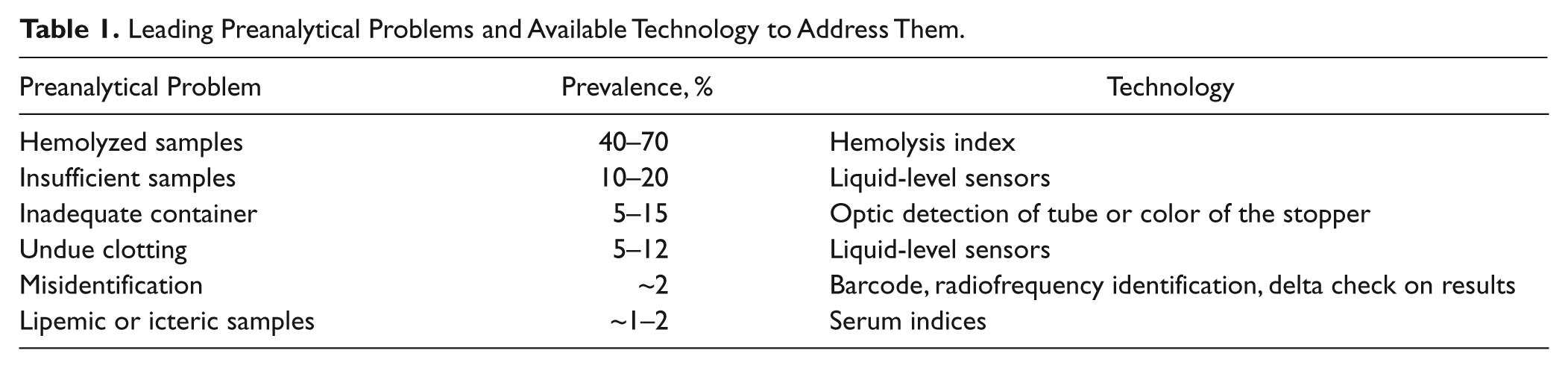
Several lines of evidence attest that the vast majority of mistakes occur in the extra-analytical activities of testing, that is, those comprised within the so-called preanalytical and postanalytical phases.7,8 The manually intensive activities of the preanalytical phase are indeed the most vulnerable steps, being associated with roughly two-thirds of all errors that can be identified throughout the total testing process. As reliably mirrored by distribution patterns, the vast majority of preanalytical errors occurs as a consequence of mistaken or mishandled procedures while collecting and handling blood specimens, which finally results in the generation of samples of poor/unsuitable quality for diagnostic testing. 9 In terms of relative prevalence, spurious hemolysis is by far the largely prevailing cause of nonconformance (from 40%–70%), ahead of samples with insufficient volume (from 10%–20%), those collected in inappropriate containers (from 5%–15%) or showing undue clotting (from 5%–12%), and those containing labeling or identification problems (from ~2%) ( Table 1 ).10,11 Irrespective of the large burden, hemolyzed specimens are also associated with relevant clinical, organizational, collective, and economical issues. The presence of cell-free hemoglobin in the sample attributable to spurious breakdown of red blood cells while drawing blood or handling the tube causes a kaleidoscope of biological, chemical, and spectrophotometric interferences that globally jeopardize the reliability of test results, especially hemostasis testing, potassium, aminotransferases, lactate dehydrogenase, and cardiospecific troponins.12–14 When the concentration of cell-free hemoglobin in the sample exceeds manufacturer-, instrument-, and analyte-specific thresholds, test results should be suppressed, and a second—it is hoped suitable—sample should be recollected. This obviously results in increased costs due to the need for drawing a second blood tube, delay in reporting results to the referring clinicians, and frequent complaints from nurses and other health care personnel. 15 On the other hand, when left unidentified or unmanaged, hemolyzed samples are indeed a latent hazard that can seriously affect patient safety, so a standardized procedure for identification and management is needed, indeed. 16
Leading Preanalytical Problems and Available Technology to Address Them.
Hemolyzed Samples and Laboratory Automation
As we move forward toward novel models of laboratory automation and integration, new challenges emerge. The complexity and the radical changes that have occurred in laboratory organization have often culminated in the integration and/or consolidation of analytical and preanalytical instrumentation. In particular, “closed systems” are generally referred to as packages of preanalytical automation lines, analyzers, and postanalytical instruments that are more expensive than open systems, can hardly be modified after installation, and are characterized by poor flexibility. The unquestionable benefits of this type of automation can be mostly found in complete replacement of manual, potentially dangerous, error-prone steps with automated activities that require negligible contribution from laboratory staff, increased throughput, and reduced turnaround time (TAT). There is clear evidence, however, that the adoption of these solutions has not eased the identification of some preanalytical problems. 17 The implementation of continuous-flow automation, where sample processing and analysis develop in a continuous and logical sequence of activities (i.e., check-in, centrifugation, decapping, aliquoting, analysis and storage), has in fact partially—if not totally—hidden the samples from visual scrutiny of medical technologists and laboratory technicians, with the inherent risk that unsuitable samples are left unidentified and thereby loaded and processed. Considering that phlebotomists and nurses have a varying perception on whether a sample is suitable for testing at the time of blood withdrawal (e.g., Stauss et al 18 recently reported that it is more likely that a sample is unsuitable when the phlebotomist thinks it is suitable and vice versa), innovative technical tools should be put forward and integrated within laboratory automation to replace visual scrutiny before blood specimens are analyzed. A variety of technological advances have recently improved the automatic detection of the most common sources of nonconformity. One of the former solutions has been the introduction of liquid-level sensors in the instruments’ needle to limit aspiration errors in samples with low to insufficient volume or detect the presence of microclots or bubbles. Another important tool is the implementation of barcode or even RFID (radiofrequency identification) technology, which now allows a bidirectional communication between instrumentation and laboratory information system (LIS), to prevent identification and transcriptional errors ( Table 1 ).
Regardless of these breakthroughs, reliable detection and management of unsuitable specimens remain the major tasks in laboratory diagnostics, and their identification, especially of those plagued by spurious hemolysis, remains rather challenging in “closed” automation systems ( Figure 1 ). The recognition of hemolyzed samples has been traditionally accomplished by visual inspection and by direct comparison with standardized color-coded scales to determine the degree of hemolysis and thereby roughly estimate the content of cell-free hemoglobin. Although largely perfectible due to the high arbitrariness of judgment,19,20 this technique has nevertheless represented the “gold standard” for decades. Together with the technical innovations previously discussed, the new generation of analytical and preanalytical workstations is increasingly equipped with systems that can systematically and automatically test for a broad series of interferences, the so-called serum indices, which also include the hemolysis index (HI). 21
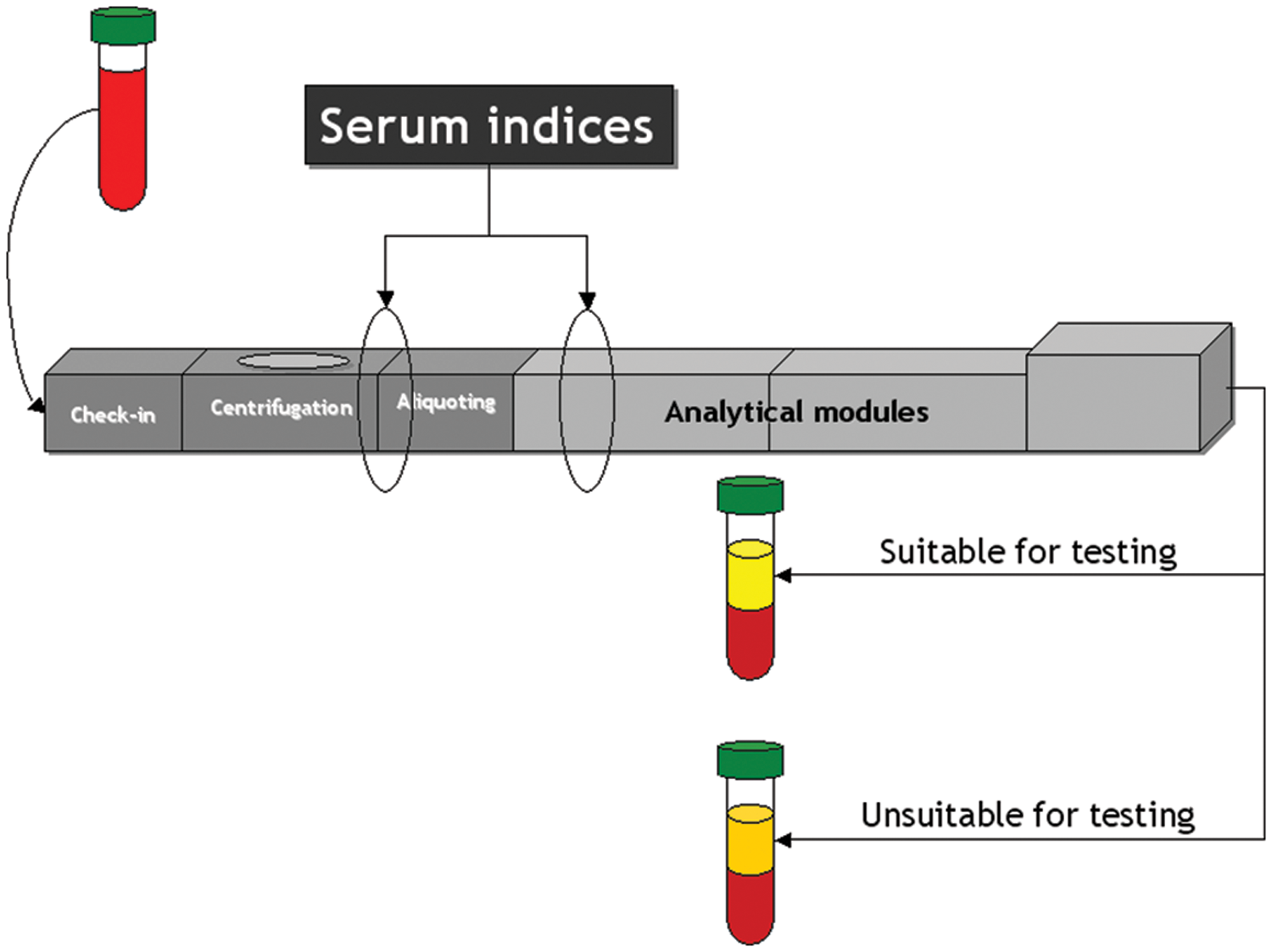
Identification of hemolyzed specimens in “closed” continuous-flow automation.
Some differences exist in the way the HI is assessed and reported, but most instruments can provide a qualitative or quantitative measure of cell-free hemoglobin in the sample, which can be further compared with specific thresholds that would help determine if the sample is suitable or not for testing. Although the assessment of this type of interference by using multiple wavelengths may be preferable, 22 this approach is unavailable on most automated analyzers, so measurement of the HI is usually based on monitoring of serum or plasma absorbance at a bichromatic wavelength, most commonly between 570 and 600 nm (the serum indices for lipemia and icterus are instead typically monitored at bichromatic wavelengths between 660–700 and 480–505 nm, respectively). 23 By solving a set of predefined equations, the HI is finally calculated and expressed as either a quantitative value (e.g., cell-free hemoglobin in arbitrary units or g/L) or a qualitative index (e.g., from “0” to “+”). The medical technologist can also customize the cutoffs for generating specific alerts. A recent evaluation of the HI on seven different automated clinical chemistry instruments has documented excellent performances in terms of imprecision (i.e., intra-assay coefficient of variation between 0.1% and 2.7%) and interlaboratory agreement. 24 Specific external quality assessment (EQA) schemes based on shipment of frozen materials can also be settled to harmonize and monitor interlaboratory performance. 25
Advantages and Limitations of the Hemolysis Index
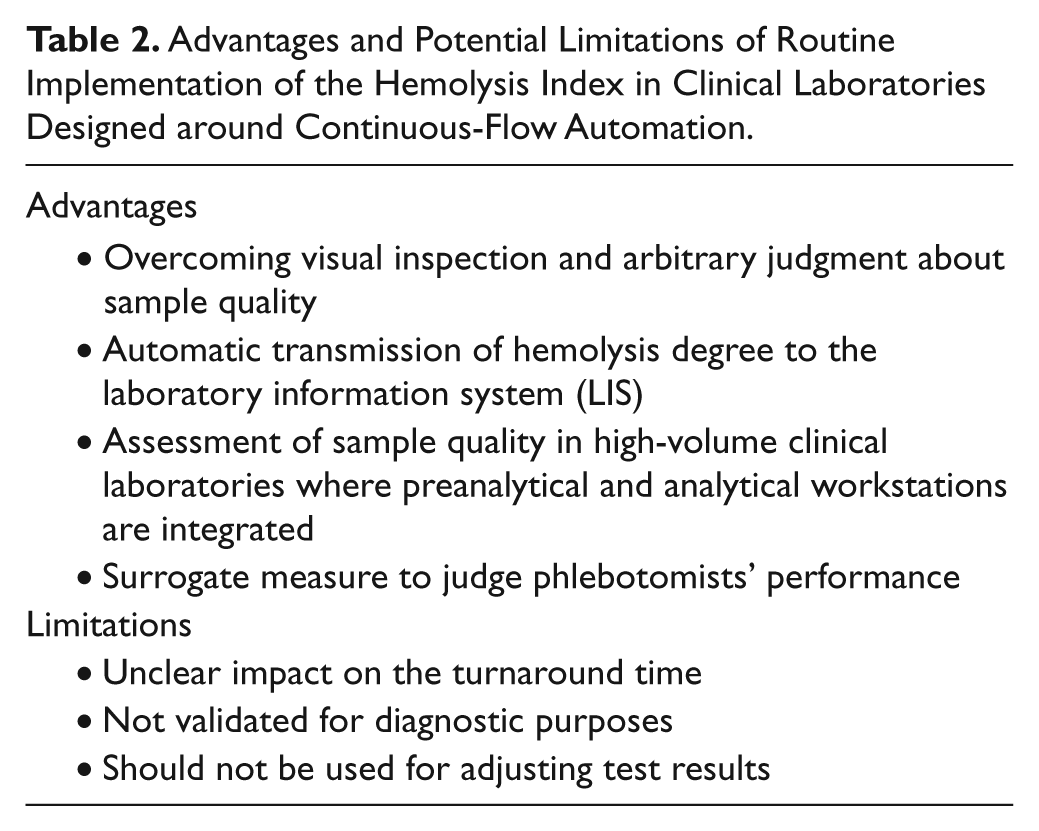
There are some obvious advantages in the widespread adoption of the HI in routine laboratory practice ( Table 2 ). These include (a) overcoming visual inspection and arbitrary judgment about sample quality; (b) transmission of the HI to the LIS, where the data are safely archived for both forensic reasons (i.e., complaints from the wards) and practical reasons (i.e., potential inclusion in the laboratory report); and (c) assessment of sample quality in high- volume clinical laboratories that use continuous-flow automation with integration of preanalytical and analytical workstations, where automatic/systematic monitoring of serum indices represents the only suitable approach to detect unsuitable specimens in “real time,” before they are released from conveyor belts. Another important advantage of the HI is that it can be used as a surrogate to judge transport time, transport temperature and centrifugation efficiency, and assess phlebotomists’ performance, wherein individual phlebotomists or phlebotomy centers encountering a high burden of spuriously hemolyzed specimens can be objectively identified and further subjected to technical (e.g., replacement of the material used for drawing blood) or educational (e.g., specific training) interventions. 26 The routine use of the HI, however, has some drawbacks. First, we know of no study that has established how the systematic measurement of HI on all samples would affect TAT. This may be relevant in terms of throughput and efficiency since the HI is performed as an add-on test in some automated instrumentations. Moreover, although the HI is often provided by manufacturers also for immunoassays, it is typically part of the chemistry (colorimetric) analyzer, which would hence lead to inefficiencies when the degree of hemolysis in samples received only for immunoassay has to be checked with a necessary transit of the specimens through the chemistry module(s). It is then noteworthy that this measure has not been validated for diagnostic purposes (e.g., for diagnosing and monitoring hemolytic anemia or for assessing blood substitutes), and it can only be used for obtaining information on sample quality. Although specific software might be available for automatic correction of test results carried out on hemolyzed specimens according to the degree of hemolysis, and some laboratories have actually incorporated the HI into their reporting algorithms, the HI must not be used for adjusting test results. We have recently proven that the mechanical injury of erythrocytes and other blood cells that may arise during collection, handling, transportation, or storage of blood specimens does not occur homogeneously (i.e., it is largely dependent on the individual erythrocyte fragility), 27 nor is the intracellular content of several molecules (especially ions, enzymes, hemoglobin, and other proteins) identical and hence sufficiently predictable among different subjects, which would make the use of corrective formulas based on the HI of the sample unreliable and even misleading. 28 Finally, manufacturers often provide hemolysis limits for their assays and assume that the laboratory will take notice of the HI of that assay. It is therefore the laboratories’ duty to comply with that stated use.
Advantages and Potential Limitations of Routine Implementation of the Hemolysis Index in Clinical Laboratories Designed around Continuous-Flow Automation.
Most clinical laboratories, especially those with the largest volume of samples, clearly profit from total laboratory automation and integrated preanalytical-analytical systems because of the minor handling of specimens, prevention of mislabeling, 29 and possibility of relieving medical technologists and medical laboratory technicians of repetitive activities such as transporting specimens and loading analyzers. 30 Besides detailed analysis of workflow to make laboratory automation as efficient as possible, the process also requires a straightforward knowledge of the potential sources of poor-quality specimens as well as the best solutions to identify and manage this foremost preanalytical problem. Continuous-flow automation indeed represents a remarkable improvement for laboratory organization, which requires systematic monitoring of sample quality. Special consideration hence should be given to routine implementation of serum indices in clinical laboratories equipped with continuous-flow automation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.