
Abstract
Background
In-person therapy (IPT) after orthopedic surgery can be costly, time-consuming, and difficult to access, particularly for patients affected by social determinants of health. Free web-based therapy (WBT) programs may offer a more accessible alternative. This study evaluated patient interest, barriers, and preferences for WBT following shoulder or wrist surgery.
Methods
A cross-sectional survey was administered to 50 postoperative patients at a level 1 trauma center during 2- or 6-week follow-up visits, assessing willingness to use WBT, barriers to IPT and WBT, and desired program features.
Results
Participants were 18–70 years old; 60% underwent wrist and 40% shoulder surgery. Fifty-eight percent had not attended IPT, most commonly due to time, cost, and distance. Interest in WBT was high (78%), particularly for free and customized programs. Reported WBT barriers included limited personal interaction, computer access, and customization.
Conclusions
Patients demonstrated a strong interest in WBT, especially when free and personalized. Virtual platforms may help address common barriers to postoperative therapy, though concerns regarding personalization, interaction, and technology access remain important considerations.
Keywords
Introduction
Advancements in orthopedic surgical techniques have led to improved outcomes and accelerated recovery for patients undergoing shoulder and wrist procedures. However, the success of these surgeries depends not only on the surgeon expertise but also on effective postoperative rehabilitation, with postoperative therapy playing a crucial role in optimizing recovery and long-term functional outcomes. 1
Postoperative therapy protocols for shoulder and wrist surgeries often vary based on surgeon preference, but evidence supports that engaging in a well-structured, evidence-based program early in the recovery period provides numerous benefits. Therapy helps minimize postoperative pain, swelling, and joint stiffness, facilitating quicker recovery and a timely return to activities of daily living. 2
Beyond the immediate postoperative period, timely postoperative therapy plays a pivotal role in ensuring sustained improvements in long-term functional outcomes. 3 By addressing muscle imbalances, enhancing joint stability, and improving neuromuscular control, an effective rehabilitation program restores strength, range of motion, and proprioception. Additionally, comprehensive therapy programs empower patients to regain independence, resume occupational and recreational activities, and avoid secondary impairments due to prolonged immobility or disuse. 4
However, in-person therapy (IPT) can be expensive, time-consuming, and logistically challenging, especially for patients from low-income backgrounds or those facing barriers to attending in-person sessions. A free web-based therapy (WBT) program could offer a valuable alternative, reducing both the financial burden and logistical barriers for patients needing postoperative care.
WBT is an online, asynchronous platform offering a library of rehabilitation exercises that can be tailored to a patient's specific surgery and health data (e.g., age, weight, ability level). Previous studies have investigated WBT's role in postoperative rehabilitation. For example, Zachwieja et al. compared rehabilitation costs in patients using different combinations of WBT and IPT following total knee arthroplasty in 701 patients. Their study found that increased use of WBT reduced overall rehabilitation costs while maintaining similar functional outcomes. 5 Recent high-level evidence further supports the feasibility of digital rehabilitation following rotator cuff repair. A systematic review and meta-analysis evaluating virtual reality (VR)-based rehabilitation compared with conventional IPT included six studies comprising approximately 332 patients. The analysis demonstrated no significant differences between digital and conventional rehabilitation in postoperative pain reduction or patient-reported functional outcomes. Notably, VR-based programs were associated with significantly greater improvements in shoulder abduction range of motion, while gains in flexion and external rotation were comparable between groups. The authors also reported that home-based digital programs may enhance adherence, although patient satisfaction appeared to depend in part on the degree of clinician interaction incorporated into the rehabilitation model. These findings suggest that digital rehabilitation platforms may provide outcomes comparable to traditional IPT while offering potential advantages in accessibility and engagement.6,7 Given its lower cost and greater accessibility, WBT could be especially beneficial for patients of lower socioeconomic status, who often face difficulties accessing IPT due to financial constraints or logistical challenges, such as transportation issues in lower-income urban areas.8–11 In fact, studies have shown that patients from lower socioeconomic backgrounds are less likely to access necessary postoperative therapy. Sarkisoova found that children with government-funded insurance had lower rates of access to postsurgical rehabilitation following orthopedic surgery. 8 WBT's minimal cost could bridge this gap for patients who may otherwise struggle to access necessary care.12–15
This study aims to evaluate the potential utility of WBT in a safety-net hospital setting for patients recovering from shoulder or wrist surgery. Specifically, we aim to survey postoperative patients to assess their interest in participating in a WBT program, identify challenges they anticipate in using such a program, and explore potential barriers to IPT or WBT participation. The findings may help inform the design of an optimized WBT program for this patient population.
Material and methods
Following institutional review board approval, a prospective, deidentified survey consisting of 10 questions (Appendix 1a) was administered to 50 patients at a single level 1 trauma center/safety-net hospital at the 2 or 6 week in-person postoperative visit after a shoulder or wrist surgery. The survey aimed to gauge patient opinions regarding IPT versus a theoretical free virtual therapy platform. Additionally, the survey examined patient preferences regarding a generalized virtual therapy program versus a more personalized and intensive virtual therapy program.
The 10-item questionnaire was developed de novo by the study team to assess patient perspectives regarding in-person and web-based postoperative therapy. Survey items were designed based on a review of existing literature on tele-rehabilitation, access to care, and social determinants of health, 9 as well as input from orthopedic surgeons involved in postoperative rehabilitation management. The instrument included structured multiple-choice questions and optional open-ended responses to capture qualitative feedback. Given the exploratory nature of this study, formal psychometric validation was not performed.
Participants were sampled consecutively during eligible postoperative visits and represented a range of educational and technological backgrounds typical of a safety-net hospital population. Formal measures of educational attainment or digital literacy were not collected. To standardize understanding of WBT, a scripted explanation describing the theoretical virtual platform—including its asynchronous format, exercise library, and customization features—was delivered verbally in a consistent manner to each participant prior to survey completion. Patients were given the opportunity to ask clarifying questions to ensure comprehension before responding.
Inclusion criteria included adult patients (>18 years) at the 2- or 6-week postoperative visit following shoulder (rotator cuff repair, labral repair, proximal humerus fracture fixation, shoulder arthroplasty) or wrist surgery (arthroscopy, fusion, distal radius fracture fixation). Participants were required to speak, understand, read, and write in English.
Exclusion criteria included patients aged <18 years, those without the required English language proficiency, individuals unwilling to participate, and patients who had not undergone shoulder or wrist surgery 2 or 6 weeks prior to the visit.
Descriptive statistics were used to summarize the demographic characteristics of the participants and their preferences for IPT and WBT. Chi-square independence tests were employed to assess the association between demographic variables and therapy modality preference. Qualitative responses were analyzed thematically to identify common themes and insights related to patient experiences and suggestions for improvement.
Results
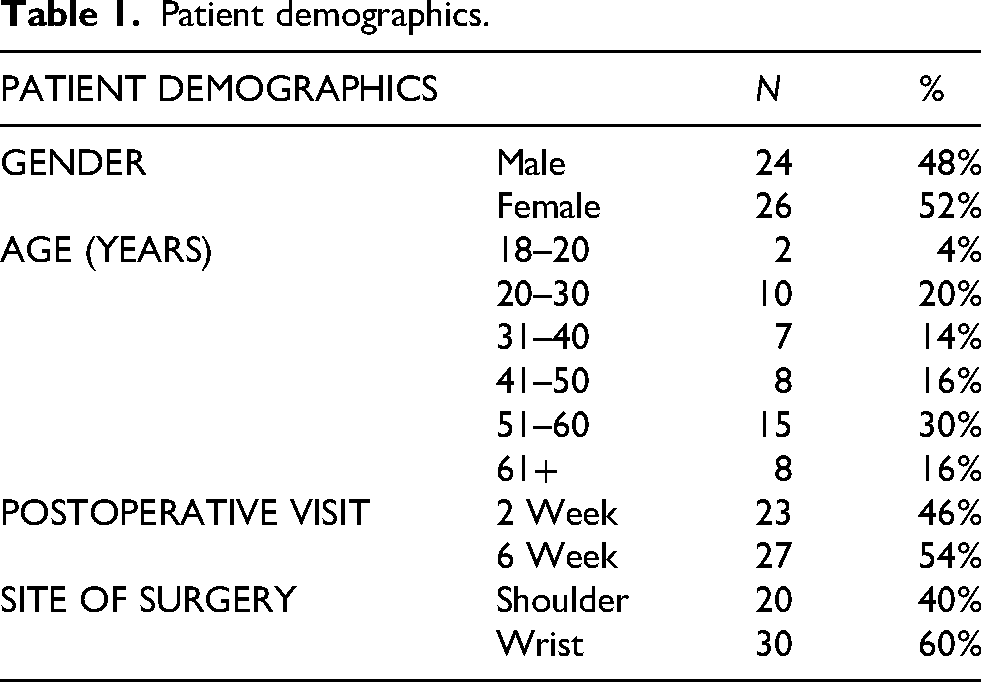
A total of 50 patients were included in the study: 20 had undergone a shoulder procedure and 30 had undergone a wrist procedure. The response rate was 100%. The average age of respondents was 44.6 years. In total, 24 patients were identified as male while 26 patients were identified as female. In total, 23 of the patients were interviewed 2 weeks after their operation, and 27 patients were interviewed 6 weeks after their operation (Table 1).
Patient demographics.
In total, 42% of patients had attended IPT postoperatively. The biggest challenges that they anticipated or experienced in attending IPT were time (52%), cost (34%), and distance/transportation issues (34%). 14% of patients indicated that they did not anticipate any challenge in completing IPT (Table 2).
Survey responses.
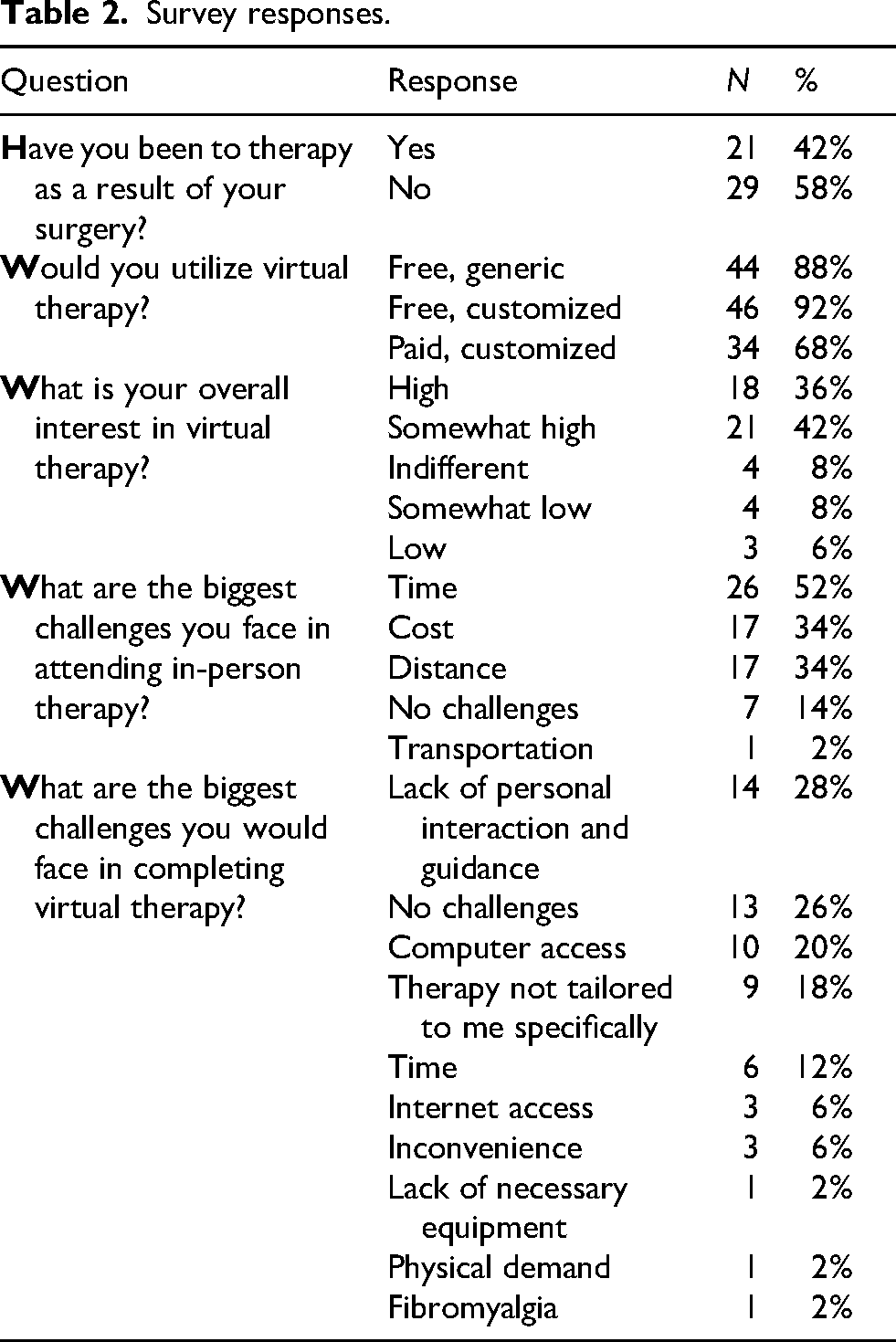
Patients showed strong interest in WBT. In total, 36% of patients had high interest, and 42% of patients had somewhat high interest. In comparison, very few patients exhibited low (6%) and somewhat low (8%) interest. The vast majority of patients stated that they would utilize virtual therapy if offered. In total, 88% said that they would use a free, generic WBT. In total, 92% said they would use a free, individualized WBT. In total, 68% said that they would use a paid, individualized WBT program. The biggest challenges that patients anticipated in completing virtual therapy were lack of personal interaction and guidance (28%), lack of computer access (20%), lack of individualization (18%), time (12%), and lack of internet access (6%). In total, 26% of patients indicated that they did not anticipate any challenge in WBT (Table 2).
Patient opinions by demographic groups
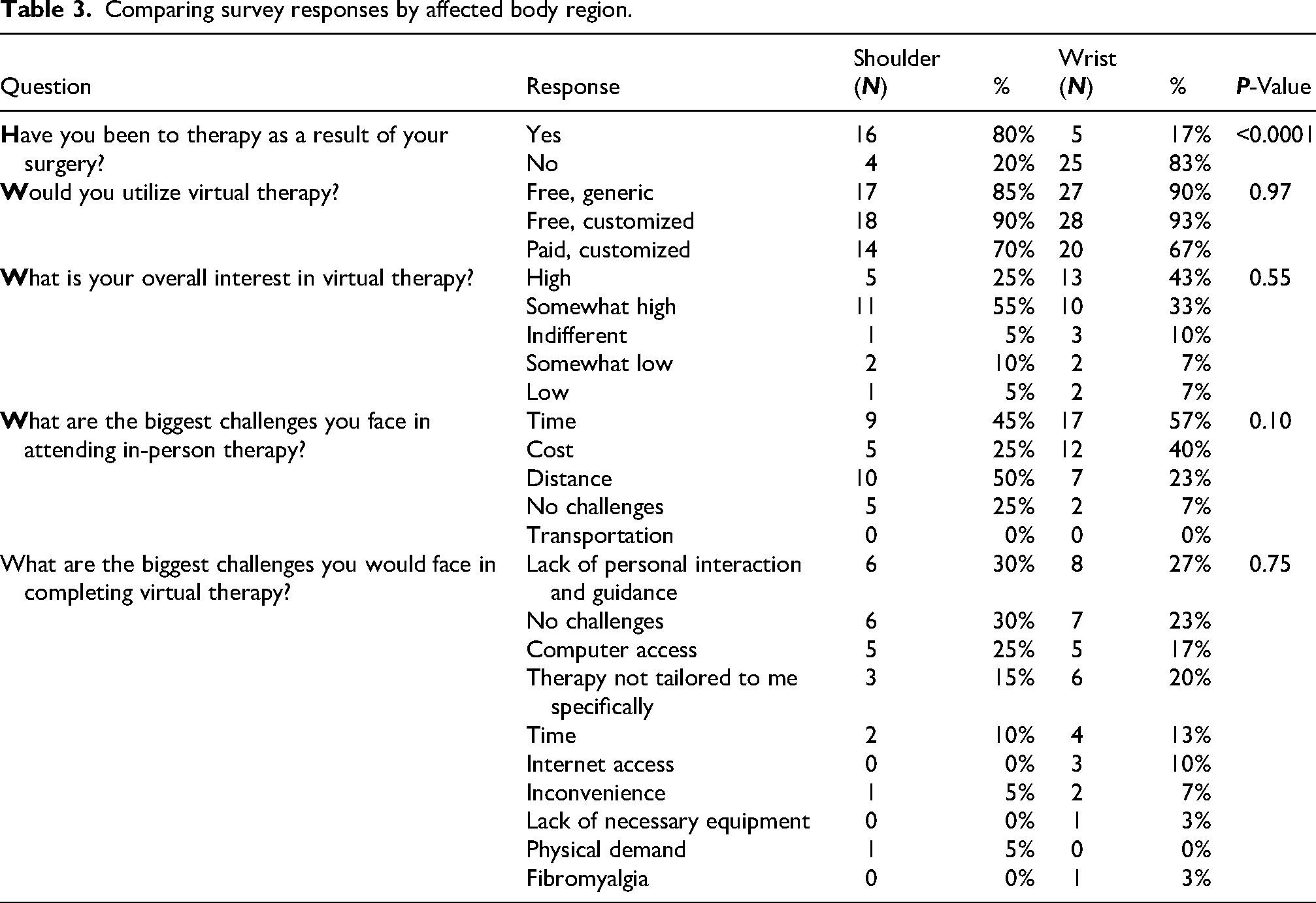
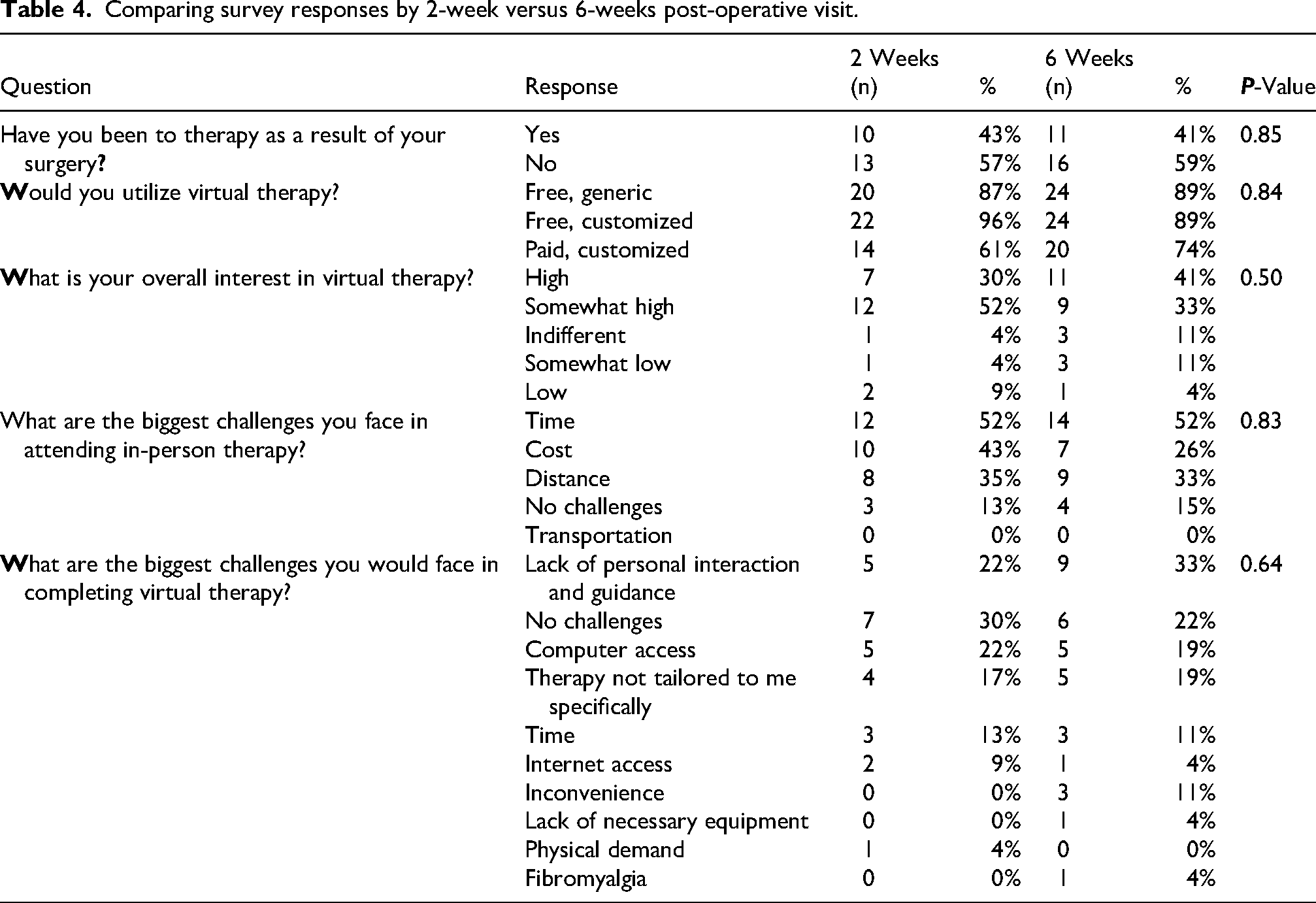
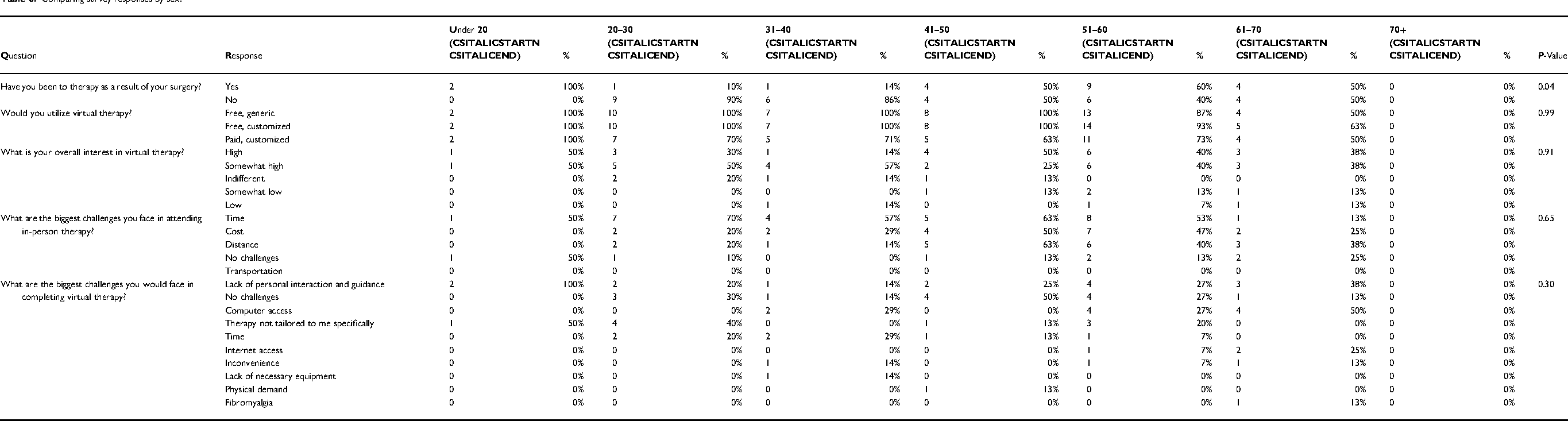
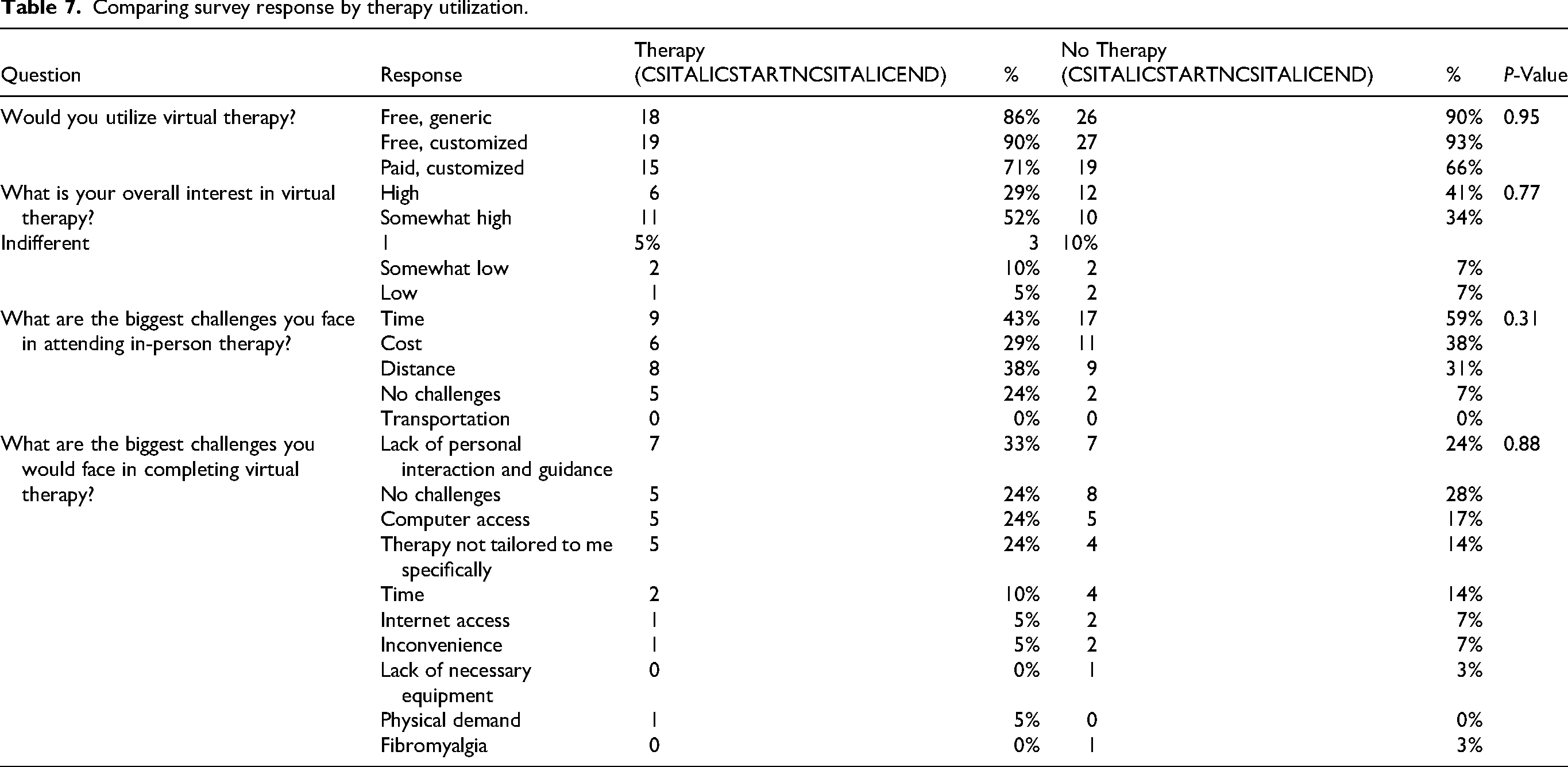
Chi-squared analysis of the survey responses revealed no significant differences across most demographic and clinical variables: patients who underwent shoulder surgery versus wrist surgery (Table 3), those seen at 2 weeks postoperatively versus 6 weeks (Table 4), male versus female patients (Table 5), different age groups (Table 6), and those who had previously received IPT for their surgery versus those who had not (Table 7).
Comparing survey responses by affected body region.
Comparing survey responses by 2-week versus 6-weeks post-operative visit.
Comparing survey responses by sex.
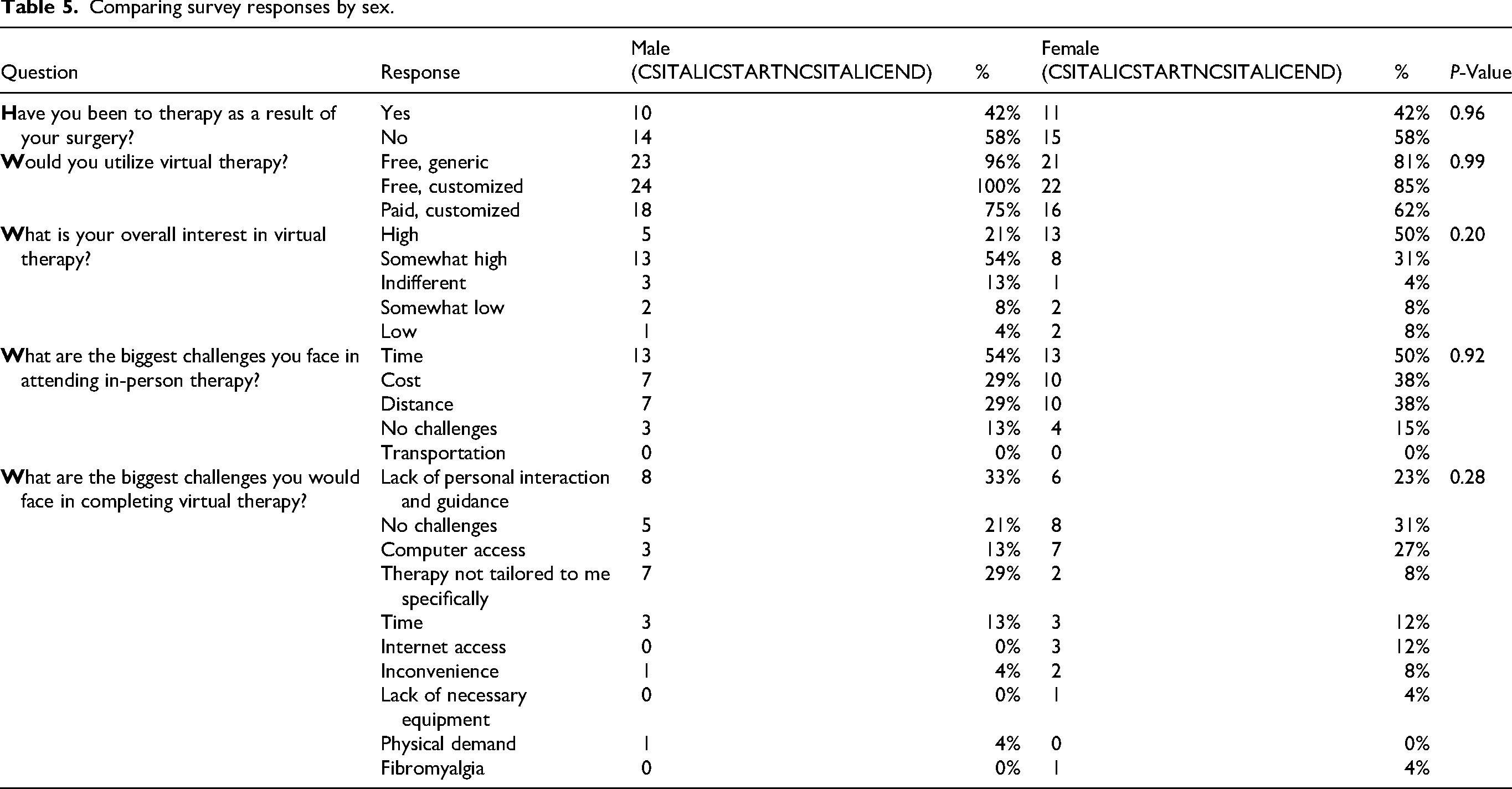
Comparing survey responses by sex.
Comparing survey response by therapy utilization.
Across all groupings evaluated, only 2 significant differences were identified. Patients who had shoulder surgery were significantly more likely to have attended therapy compared to those who underwent wrist surgery (p < 0.0001). Additionally, younger patients reported attending therapy at higher rates than older patients (p = 0.04). In these cohorts, no differences in opinion or preference regarding WBT was identified.
Discussion
The use of WBT programs as a rehabilitative option for patients recovering from orthopedic surgery has gained attention in recent years. The aim of this study is to evaluate patient opinion on any potential limitations of WBT programs after orthopedic surgery to the shoulder or wrist in a safety net hospital setting.
Our results demonstrate a clear interest in increased accessibility to rehabilitation programs for patients in the early postoperative period, and analysis revealed that patient responses were consistent across demographic groups, thus decreasing the likelihood of bias affecting responses.
The survey responses did not show statistically significant differences between the demographic groups analyzed, including patients who underwent shoulder surgery as compared to wrist surgery (Table 3), those seen at 2 weeks postoperatively versus 6 weeks (Table 4), male versus female patients (Table 5), different age groups (Table 6), and those who had previously received IPT for their surgery versus those who had not (Table 7). This consistency across groups suggests that patient opinions about WBT programs are largely universal, regardless of demographic or clinical variables, further supporting the broad patient interest and potential applicability of WBT as a rehabilitative option.
This consistent interest across demographic groups underscores the importance of addressing common barriers to rehabilitation access through innovative solutions such as WBT. In total, 86% of patients cited challenges in attending IPT, with the most common challenges cited being time (52%), cost (34%), and distance (34%). These challenges are consistent with known common social determinants of health that prevent patients from accessing healthcare. 8
A well-constructed WBT program could help alleviate these concerns. We found that 26% of patients anticipated no challenges in completing WBT compared to only 14% who anticipated no challenges in completing IPT. One key advantage of WBT programs is their accessibility and convenience. Postoperative therapy programs often require several sessions per week. With WBT, patients can access their rehabilitation plans from home, eliminating the need to arrange travel and allocate time for transport to in-person visits therapy visits.
Patients can also utilize a video library in WBT to complete their therapy sessions on their own schedule, which is particularly beneficial for those with demanding work schedules that interfere with attending IPT appointments. This flexibility is especially valuable for patients who may face challenges with IPT due to transportation, mobility, or geographical distance. Additionally, WBT programs generally have lower costs than traditional IPT. 5 This can translate to lower costs for patients using WBT, benefiting those who face financial barriers to postoperative rehabilitation, a challenge cited by 34% of patients as a barrier to completing IPT. Taken together, these benefits highlight the potential advantages of offering WBT as an option for postoperative rehabilitation.
In gathering information about patient preferences regarding a potential WBT program, several trends have become evident. Patients show a strong interest in using a WBT program. According to our survey, 78% of patients expressed a desire in WBT, listing “High” (36%) or “Somewhat High” (42%) interest in virtual internet-based therapy (Table 4). Moreover, 92% of patients indicated they would use a free, customized WBT after surgery. Additionally, there is a slight preference for customized WBT over a generic templated version (92% vs 88%, respectively). When asked about “the biggest challenges you believe you would face in completing virtual therapy,” 18% of patients cited concerns that their rehabilitation plan might not be tailored to their specific needs. This preference for customized programs highlights the importance of personalized care in patient adherence to and satisfaction with therapy. It also emphasizes how important integration of personalized rehabilitation into any potential WBT is, such as allowing providers to tailor rehabilitative exercise regimens to meet individual patient needs.
While individualization of the rehabilitation plan garners patient interest, the cost of care is an even larger determining factor in determining patient usage of WBT programs. When asked if they would utilize a customized virtual therapy program if there was a co-pay or fee, only 68% of patients answered affirmatively compared to 92% of patients who stated they would use the same program if it were free. Despite the clear interest in individualized rehabilitation plans, the considerable influence of cost on patient engagement with WBT programs cannot be overlooked. This disparity in willingness to participate based on cost highlights a critical barrier to access and aligns with known social determinants of health that prevent patients from obtaining care. 8
Beyond financial considerations, patients face several other challenges when using virtual therapy programs, which further complicate their ability to benefit from these services. One of the primary limitations identified was a lack of personal interaction and guidance, with 28% citing this as a concern. The absence of direct supervision and hands-on guidance from a qualified therapist is certainly a valid criticism of widespread implementation of WBT. Without proper oversight, patients may perform exercises incorrectly or inadequately, potentially leading to suboptimal outcomes or even risk of injury. Additionally, IPT offers patients the opportunity to receive wound care and scar management, which would not be available through virtual platforms. In a safety-net hospital context, practical strategies could help mitigate these concerns. Hybrid or semi-supervised models that combine periodic in-person or telehealth check-ins with digital therapy can provide essential guidance while minimizing travel and time burden. WBT programs can also incorporate interactive instructional videos, progress tracking, and remote feedback tools to reinforce proper technique and provide real-time monitoring by clinicians. Onboarding sessions or brief tutorials can help patients learn to navigate the platform, reducing errors and increasing confidence in performing exercises independently. These strategies may enhance patient engagement, adherence, and satisfaction while maintaining safety and effectiveness. Additionally, web-based programs could enable remote monitoring and feedback from healthcare providers, which may enhance patient engagement and motivation while addressing concerns about the lack of personal interaction. Even with these channels for feedback between patients and providers, web-based programs may not be suitable for all patients, such as those with complex or severe conditions that require specialized care. Future research efforts are needed to delineate the factors that determine which patients are good candidates for WBT and which require increased supervision available via IPT.
Another notable challenge patients cited in our survey was a lack of access to a computer (20%) and the internet (6%). Such technological constraints disproportionately affect underserved populations and could impede equitable participation in WBT. 16 To address this, programs could provide loaner devices, subsidized internet access, or preloaded tablets, and leverage national initiatives such as the FCC Lifeline program, which subsidizes smartphones and internet service for low-income individuals. 17 Coupled with simple, intuitive platform design and technical support, these measures may help ensure that all patients, regardless of socioeconomic status or digital literacy, have the opportunity to benefit from virtual rehabilitation.
Our findings align with emerging evidence supporting digital rehabilitation following upper extremity surgery. Recent meta-analytic data demonstrate that VR-based rehabilitation achieves comparable outcomes to conventional IPT in pain reduction and functional improvement, with superior gains in shoulder abduction range of motion and potential improvements in adherence. 7 Other studies support WBT as a practical and effective tool for improving quality of life, reducing fatigue, and increasing activity levels for patients rehabilitating from orthopedic surgery.18,19 Additionally, Mulieri et al. 20 compared the outcomes of patients recovering from total shoulder arthroplasty who utilized IPT and a home-based, physician-guided therapy program. They found that both methods yielded similar benefits, suggesting that home-based therapy may be an adequate rehabilitation option for patients though they identified no statistically significant benefit of WBT. 21
Limitations
This study has several limitations. First, the sample size was modest and drawn from a single safety-net hospital, which may limit generalizability. Second, participants represented heterogeneous educational and technological backgrounds, but formal assessment of digital literacy or education level was not performed, which may influence perceptions of WBT. Third, eligibility criteria required participants to read and understand English and attend a 2- or 6-week follow-up visit. These criteria may have introduced selection bias, as language proficiency, follow-up adherence, and digital literacy are closely tied to social determinants of health. Consequently, the study may underestimate barriers and overestimate patient interest in WBT compared with the broader patient population served by the hospital. Finally, the study assessed hypothetical interest rather than actual WBT utilization or clinical outcomes. Future research should evaluate patient engagement, adherence, and clinical effectiveness of implemented digital rehabilitation programs across diverse populations, including non-English speakers and those with lower digital literacy.
Conclusion
WBT programs have the potential to offer important rehabilitative benefits for patients recovering from orthopedic surgery by improving accessibility, promoting patient engagement, and providing scheduling flexibility. Our data shows strong patient interest in WBT programs, particularly those that are customized and offered for free. However, limitations such as the lack of direct supervision and access to technology must be taken into account. Future research should focus on evaluating the effectiveness and safety of WBT programs and developing standardized guidelines for their optimal use in postoperative orthopedic rehabilitation.
Footnotes
Author contributions
Justin Choy, William F. Pientka II, and Brian Webb conceptualized the study. Justin Choy performed data collection and drafted the initial manuscript. William F. Pientka II conducted statistical analysis. All authors contributed to manuscript review and critical revisions. The authors declare that they have no financial disclosures or conflict of interests to report. This study was reviewed and approved by the North Texas Regional Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.