
Abstract
Background
Tranexamic acid is commonly used for bleeding control. This study investigated the effect of a single dose of tranexamic acid on blood loss and packed cell transfusion rates in geriatric hip fracture fixation surgery.
Methods
This retrospective cohort study involved a total of 218 patients who were admitted to a single trauma centre in Hong Kong between January 2023 and July 2024. The treatment group was given 1 g of intravenous tranexamic acid upon induction of anaesthesia. Intra-operative blood loss, packed cell transfusion rate, post-operative haemoglobin change and length of stay were compared. The incidence of post-operative thromboembolic complications (cerebrovascular accident, myocardial infarction, deep vein thrombosis and pulmonary embolism) was also compared.
Results
There was no significant difference in terms of intra-operative blood loss, packed cell transfusion rate, post-operative haemoglobin drop, thromboembolic events and length of stay.
Conclusion
One gram intravenous tranexamic acid did not influence blood loss or transfusion requirement, nor increase thromboembolic events.
Introduction
Geriatric hip fractures present a major burden to society. There is an increasing trend in the number of patients admitted to public hospitals in Hong Kong for hip fracture surgery. With a recorded 3678 cases in the year 2000, it is projected to reach more than 14,500 cases in the year 2040. 1
Significant blood loss is associated with higher morbidity and mortality, causing an estimated 20% to 32% of 30-day post-operative deaths after non-cardiac surgery. 2 Allogeneic blood transfusion is often used to treat anaemia, yet carries risks including transfusion reactions and transmission of blood-borne pathogens. We aim to establish a drug protocol that can reduce intra-operative blood loss and hence transfusion requirement among geriatric hip fracture patients.
Tranexamic acid is a synthetic derivative of the amino acid lysine. It competitively inhibits the conversion of plasminogen to plasmin, causing an anti-fibrinolytic effect. Although some studies have suggested that the use of tranexamic acid may promote a hypercoagulable state, systematic review has shown no significant difference in deep vein thrombosis (DVT), acute coronary syndrome, and cerebrovascular events among those who received tranexamic acid and those who did not. 3
Local studies by Yee et al. 4 and Chen et al. 5 have shown that topical tranexamic acid used in hip fracture surgery does not reduce blood loss and transfusion needs, nor increase thromboembolic complications. However, there is limited data regarding the use of intravenous tranexamic acid in hip fracture surgery among the Hong Kong elderly population. This study aims to evaluate the effect of single dose intravenous tranexamic acid on intra-operative blood loss and perioperative transfusion rates among geriatric hip fracture patients receiving fixation surgery. To assess the safety of this drug regime, the effect on post-operative thromboembolic complications (including cerebrovascular accident (CVA), myocardial infarction (MI), pulmonary embolism (PE) and DVT) was also monitored.
Materials and methods
Design and setting
This is a retrospective cohort study including 218 patients aged ≥65 years old admitted to a single trauma centre in Hong Kong between January 2023 and July 2024, who underwent fixation surgery for hip fracture.
This study was approved by and conducted according to regulations set by the Hospital Authority Clinical Research Ethics Review (HA CRER) committee. Informed consent was waived for this retrospective cohort study. Patients under study have already undergone appropriate treatment for their hip fracture per clinician's decision and the department protocol.
Inclusion and exclusion criteria
Prior to December 2023, tranexamic acid was not routinely used in geriatric hip fracture surgery in our department. The department protocol was updated in December 2023, so that eligible patients who underwent fixation surgery for geriatric hip fracture would be given 1 g of intravenous tranexamic acid upon induction of anaesthesia. Hence patients who were admitted from January to November 2023 would act as the control group (not given tranexamic acid), while those who were admitted from December 2023 to July 2024 would act as the treatment group (given tranexamic acid upon induction of anaesthesia).
Exclusion criteria were:
− Those currently on anti-coagulant (e.g. warfarin and novel oral anticoagulant) or anti-platelet (other than aspirin) therapy; − History of DVT or PE; − Estimated glomerular filtration rate (eGFR) <15 mL/min/1.73 m2 or patient on renal replacement therapy; − History of endovascular stenting (e.g. cardiac stenting for ischaemic heart disease, limb stenting for peripheral vascular disease); − Known malignancy; − History of seizure
6
; − Subarachnoid haemorrhage; − Allergy to tranexamic acid; and − Revision surgery for hip fracture (Figure 1).
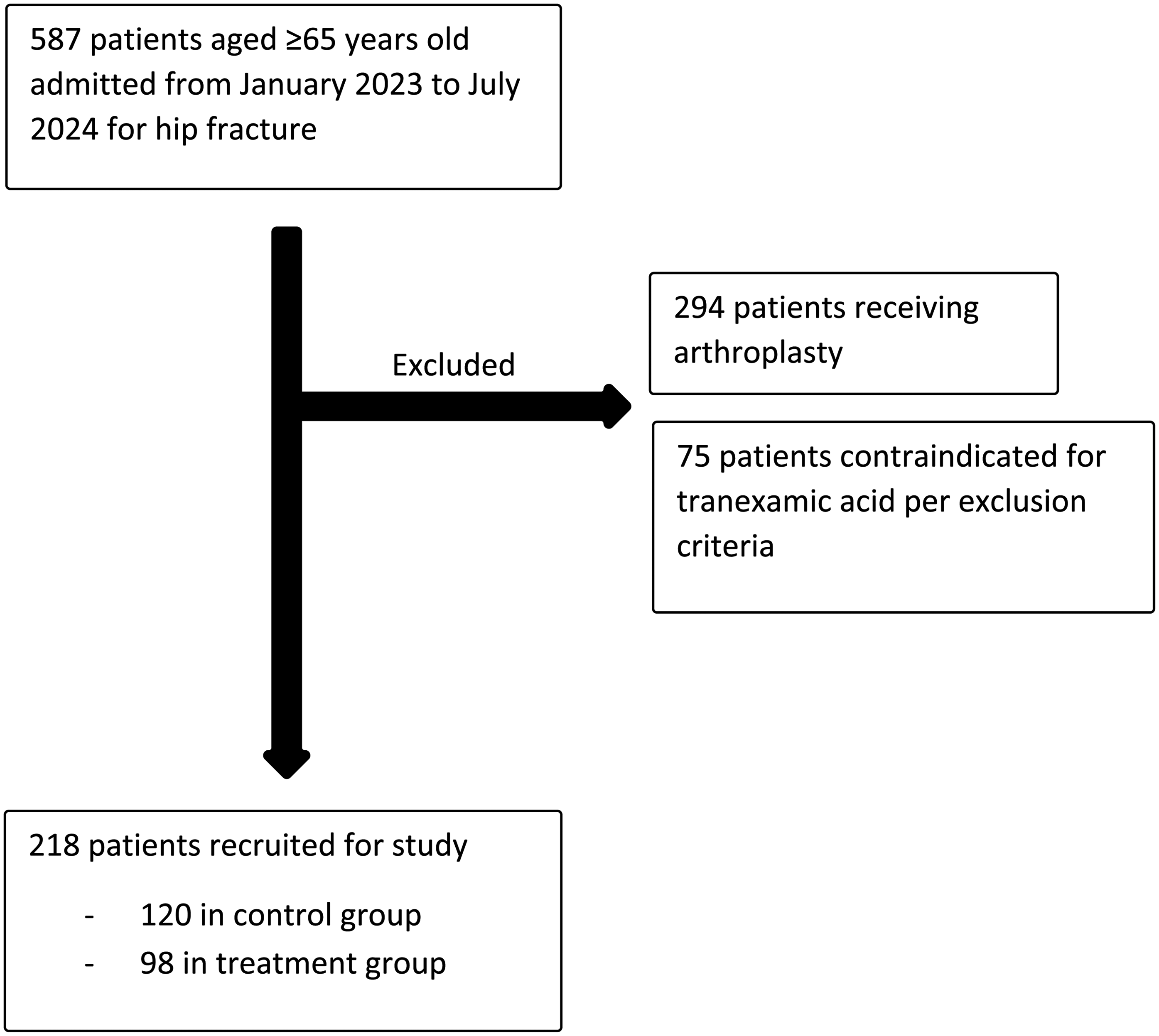
Flowchart of patient enrolment.
Interventions
Patients who sustained an intertrochanteric hip fracture were treated with a cephalo-medullary device (Synthes proximal femoral nail anti-rotation or Synthes TFN-ADVANCED™ Proximal Femoral Nailing System). Those who sustained a non-displaced neck of femur fracture (Garden type I or II) were treated with the Synthes femoral neck system.
All patients provided informed consent. For mentally incompetent patients, consent was signed by two medical officers after liaising with the patient's relative.
Upon admission, patients were given a sequential compression device (SCD) for the lower limbs (unless contraindicated) for mechanical thromboprophylaxis. Contraindications for SCD use included those with active infection of the lower limbs, peripheral vascular disease, pathological fracture of the lower limbs and suspected/confirmed DVT of the lower limbs.
Pre-operatively, blood was taken for baseline haemoglobin and haematocrit. Demographic data (age and sex), comorbidities (including hypertension, diabetes mellitus, CVA, MI, history of PE and history of DVT) were recorded.
Upon induction of anaesthesia, patients were given a single dose of either cefazolin or vancomycin (for those allergic to cefazolin or known to be methicillin-resistant Staphylococcus aureus carriers). Those in the treatment group were also given 1 g of intravenous tranexamic acid. Intra-operatively, intertrochanteric fractures were reduced and fixed with a cephalo-medullary device, while non-displaced neck of femur fractures were fixed in situ with the Synthes femoral neck system. The volume of intra-operative blood loss (mL), intravenous fluids given (mL) and any packed cell transfusion (mL) were recorded in the anaesthetic record. Meticulous haemostasis was performed and the wound was closed in layers to achieve a watertight seal.
Post-operatively, two more doses of intravenous antibiotic (cefazolin or vancomycin) were given.
Outcome and data collection
Data was collected by the principal investigator using the Hospital Authority's Clinical Management System.
Blood tests were performed on post-operative day 1 to measure post-operative haemoglobin and compared with the pre-operative level. If post-operative haemoglobin dropped below 7.0 g/dL, or lied between 7.0 and 10.0 g/dL in a patient with anaemic symptoms, packed cell transfusion was given on a unit-by-unit basis. Haemoglobin level was rechecked post-transfusion, and further transfusion was given if the above transfusion trigger was met.
Blood loss was estimated by two methods. Firstly, the amount of intra-operative blood loss was extracted from the anaesthetic record. Secondly, total blood loss was calculated by the Gross and Nadler formulae.7,8
Total blood loss (mL) = PBV × (Hctpre−Hctpost)/Hctave
PBV = predicted blood volume Hctpre = the initial preoperative haematocrit level Hctpost = the lowest postoperative haematocrit level during hospitalization or the lowest postoperative haematocrit prior to blood transfusion Hctave = the average of the Hctpre and Hctpost
PBV (mL) = k1 × height3 (m) + k2 × weight (kg) + k3
k1 = 0.3669, k2 = 0.03219, and k3 = 0.6041 for men k1 = 0.3561, k2 = 0.03308, and k3 = 0.1833 for women If an allogeneic transfusion was performed, the volume transfused was added when calculating total blood loss.
Post-operative thromboembolic complications including CVA, MI, PE, and DVT were tracked during their inpatient stay in our acute hospital, and their subsequent stay in the rehabilitation ward of another district hospital. Length of stay in our acute hospital were recorded.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics version 28.0.0.0. Normality of continuous variables was assessed by Shapiro–Wilk test. Parametric data was analysed by the independent samples T test, while non-parametric data was analysed by the Mann–Whitney U test. Categorical variables were analysed using Chi-squared and Fisher's exact tests. Statistical significance was set at p < 0.05.
Baseline demographics including age and comorbidities were compared. Primary outcomes included the incidence of patients requiring intra-operative red cell transfusion, volume of intra-operative blood loss and degree of post-operative haemoglobin drop. Secondary outcomes included the incidence of thromboembolic complications and length of stay in our acute hospital.
Results
120 patients were included in the control group, while 98 patients were included in the treatment group. Among the control group, 93 cases were fixed with a 170 mm length ‘short’ cephalo-medullary device, 8 cases with a ‘long’ cephalo-medullary device spanning the whole femur length and 19 cases with the femoral neck system. As for the treatment group, 75 cases were fixed with a ‘short’ cephalo-medullary device, 4 cases with a ‘long’ cephalo-medullary device and 19 cases with the femoral neck system.
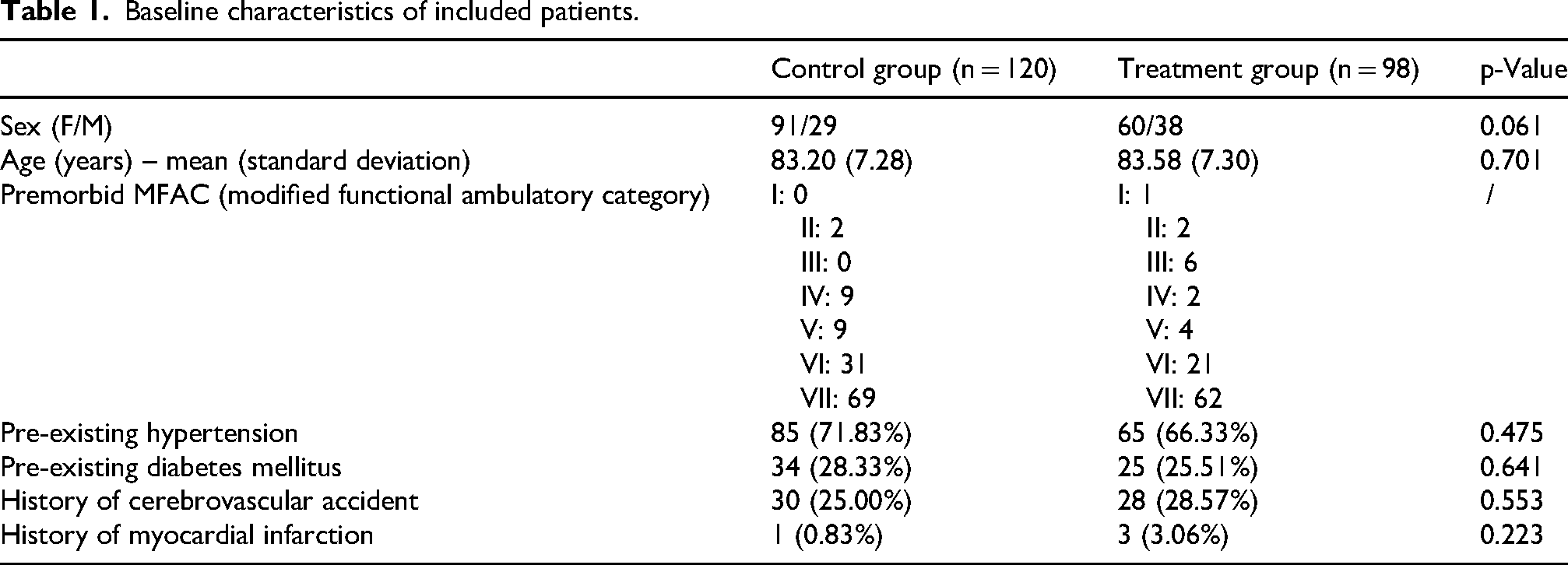
Baseline characteristics were comparable among the two groups. There was no significant difference between the control and treatment groups in terms of sex, age, and comorbidities (including hypertension, diabetes mellitus, history of CVA or MI) (Tables 1 and 2).
Baseline characteristics of included patients.
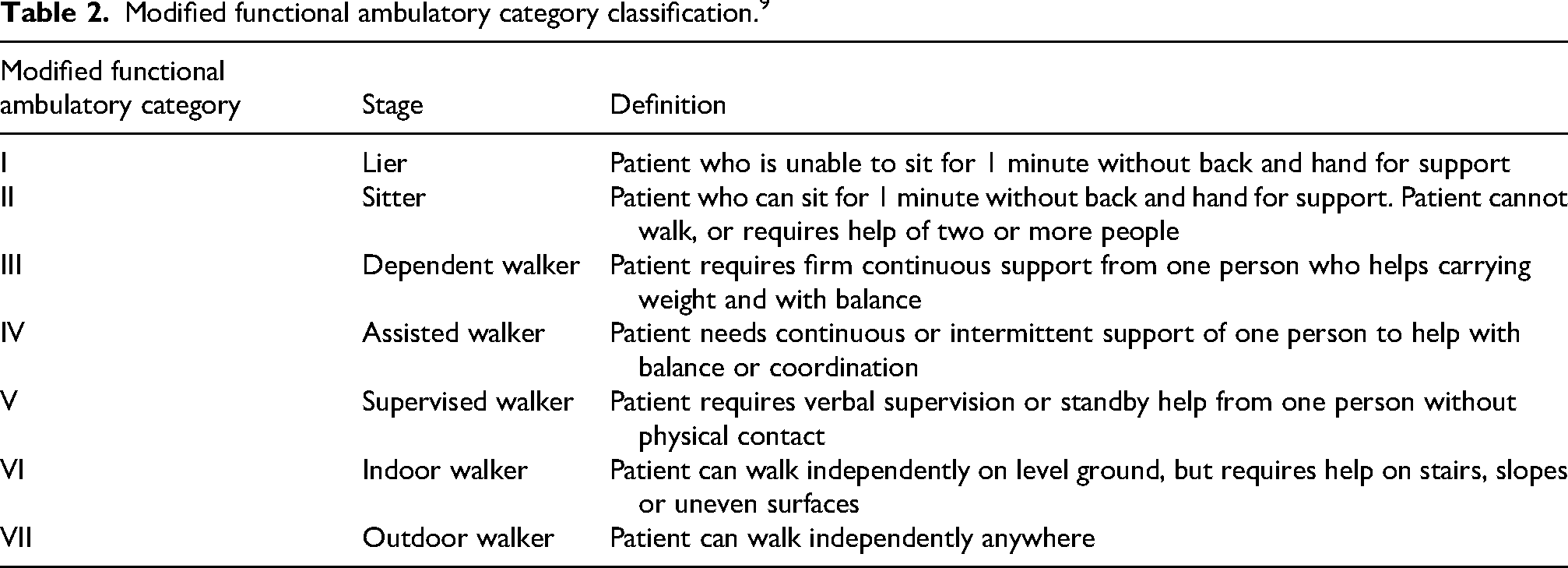
Modified functional ambulatory category classification. 9
There was no significant difference in terms of operative time and volume of intra-operative intravenous fluids given. Blood loss, red cell transfusion requirement (both intra-operatively and post-operatively) and post-operative haemoglobin change (as calculated by post-operative D1 haemoglobin minus pre-operative haemoglobin) were also comparable. There was no significant difference in length of stay.
None of the patients in either control or treatment groups had post-operative CVA, DVT or PE. Three patients in the control group and one patient in the treatment group developed MI post-operatively. This was not statistically significant (p = 0.418).
Subgroup analysis was performed for those who received a ‘short’ cephalo-medullary device and femoral neck system. Due to the relatively small sample size of patients who received a ‘long’ cephalo-medullary device, this group was not analysed separately. Again, we found no significant difference in blood loss and transfusion requirements (Tables 3–5).
All subjects.
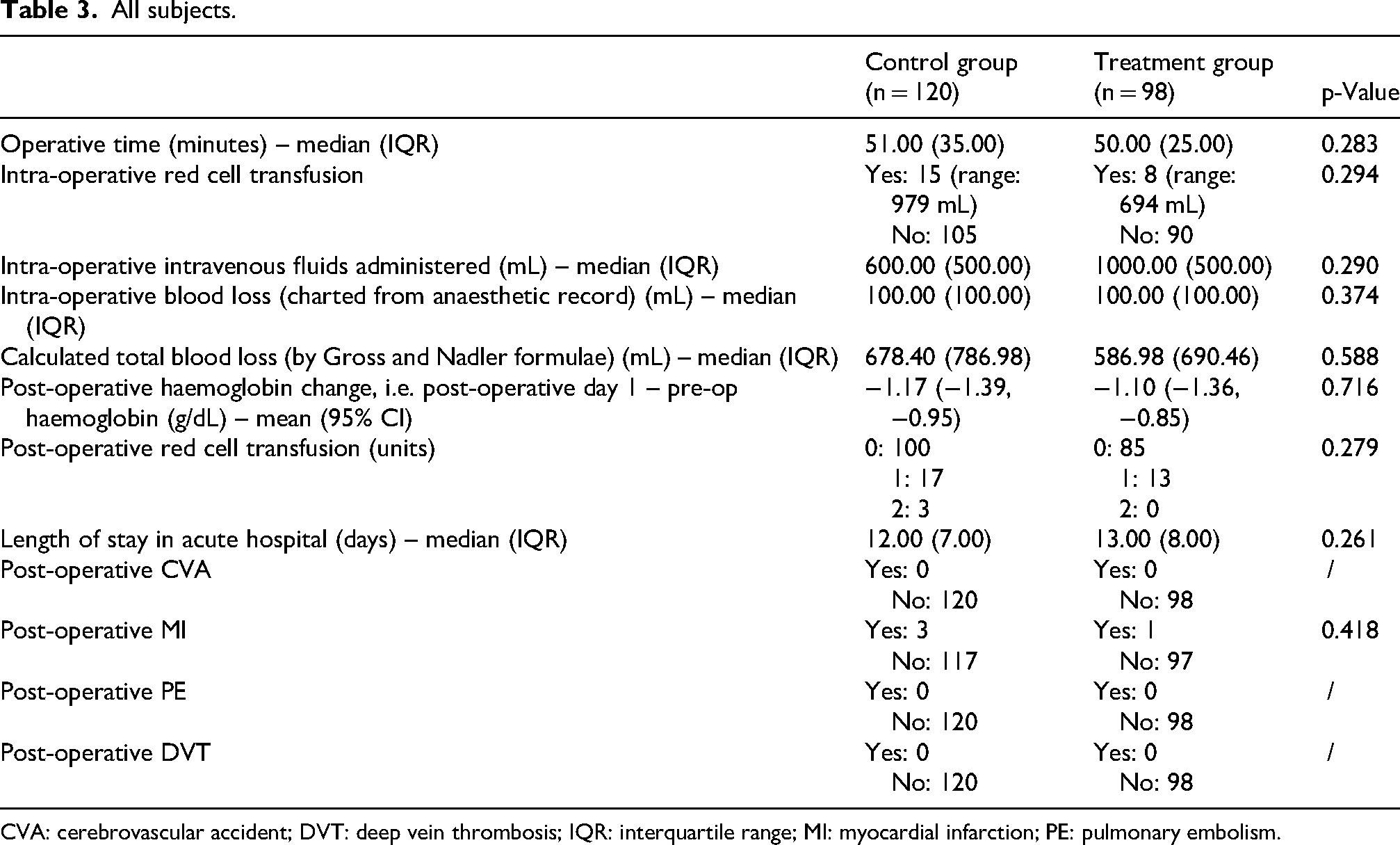
CVA: cerebrovascular accident; DVT: deep vein thrombosis; IQR: interquartile range; MI: myocardial infarction; PE: pulmonary embolism.
Subgroup analysis of patients receiving ‘short’ cephalo-medullary device.
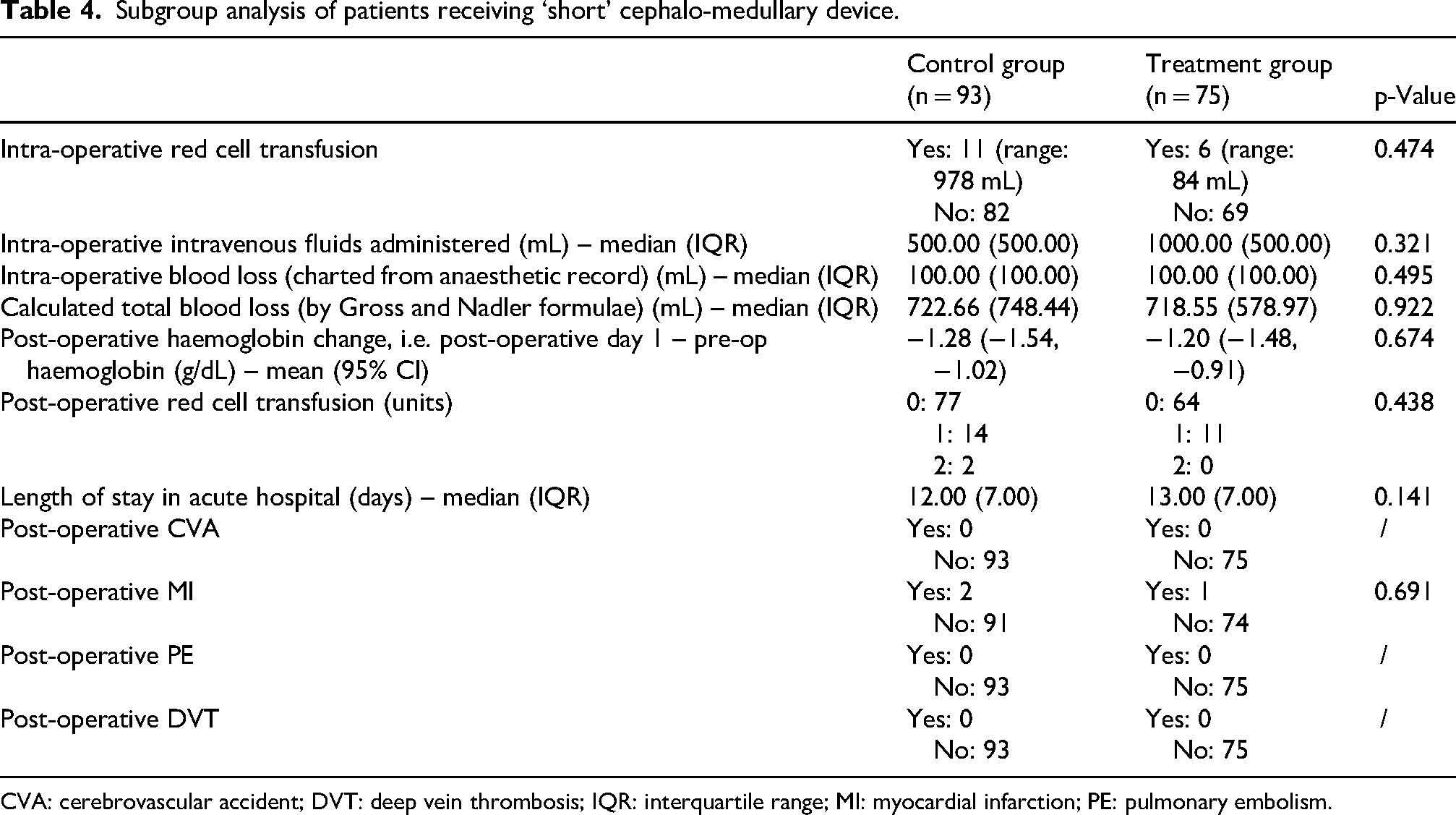
CVA: cerebrovascular accident; DVT: deep vein thrombosis; IQR: interquartile range; MI: myocardial infarction; PE: pulmonary embolism.
Subgroup analysis of patients receiving femoral neck system.
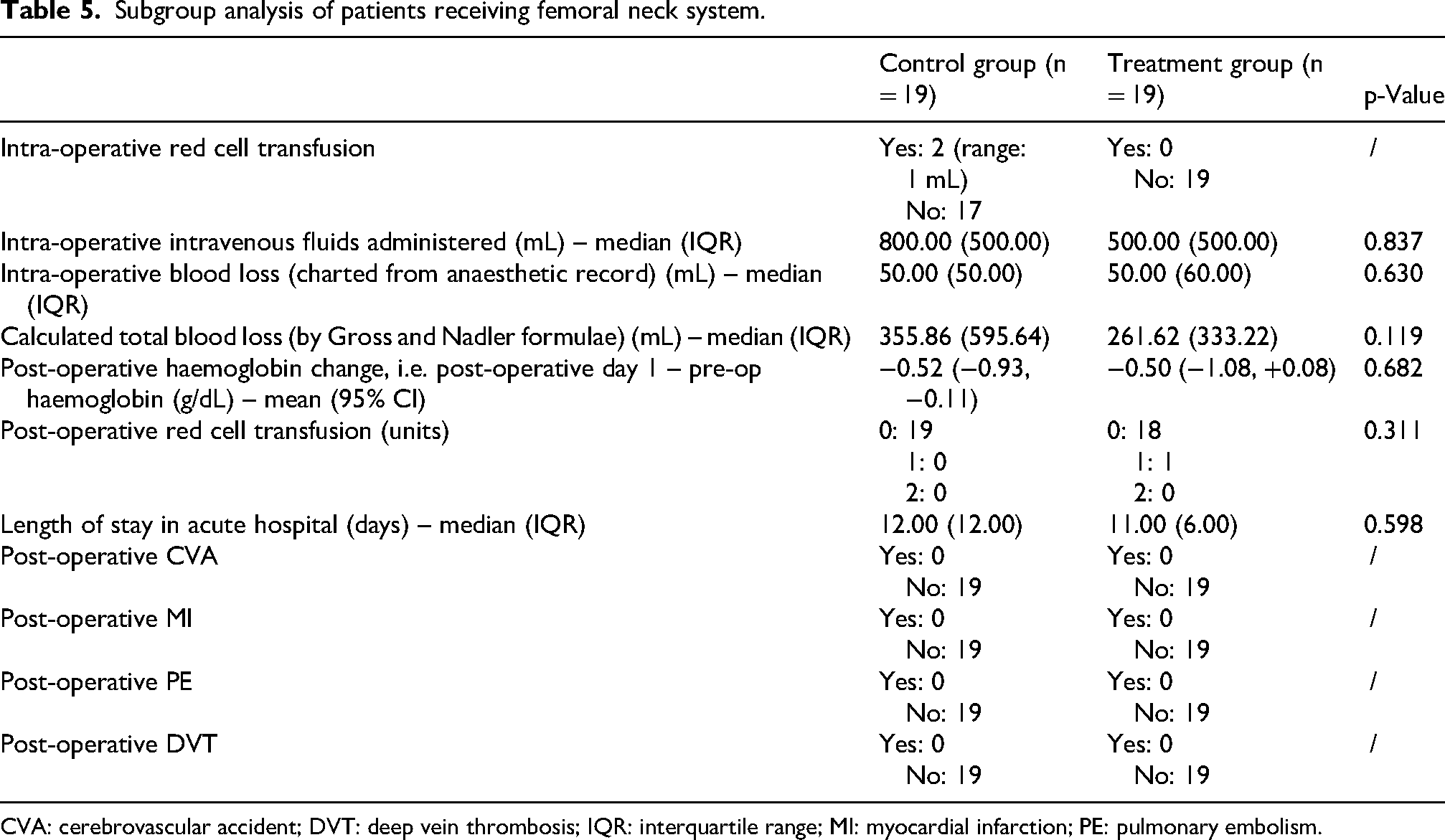
CVA: cerebrovascular accident; DVT: deep vein thrombosis; IQR: interquartile range; MI: myocardial infarction; PE: pulmonary embolism.
Discussion
Due to its anti-fibrinolytic properties, tranexamic acid has been used extensively as an adjunct in spine surgery, 10 total knee and total hip arthroplasties. 11
The use of intravenous tranexamic acid has been studied in the context of geriatric hip fractures among international populations. In a randomised controlled trial conducted by Nikolaou et al., elderly patients undergoing hemiarthroplasty (for subcapital fracture) or intramedullary nailing (for intertrochanteric fracture) were given either a single dose of 15 mg/kg intravenous tranexamic acid (diluted in 100 mL normal saline) or placebo (100 mL normal saline) before the incision was made. They found that patients who received tranexamic acid had significantly lower total blood loss and were less likely to require blood transfusion. 12 A study by Kahan et al. 13 utilising up to four doses of intravenous tranexamic acid has found a reduction in transfusion requirement without an increase in cerebrovascular event, MI, and venous thromboembolic disease.
In our study, we evaluated the clinical significance of the change in our department protocol for geriatric hip fracture fixation surgery, that is, the addition of 1 g intravenous tranexamic acid upon induction of anaesthesia. To our knowledge, this is the first local study assessing the effect of intravenous tranexamic acid on geriatric patients who received fixation surgery for neck of femur fracture.
In our study, we found that the administration of intravenous tranexamic acid had no significant effect on intra-operative blood loss, red cell transfusion requirement (both intra-operatively and post-operatively), post-operative haemoglobin change and length of stay.
We note the difference in estimated blood loss as charted in the anaesthetic record versus estimated by the Gross/Nadler formulae. There are limitations to both methods. For the first method (i.e. from anaesthetic record), the volume recorded is often from visual estimation, which creates intra- and inter-observer variations. For the formulaic method, it may be affected by the administration of intravenous fluids. As we routinely give patients intravenous fluids post-operatively until their oral intake is satisfactory, the haemodilutional effect may cause an overestimation of the total blood loss. However, no matter the estimation method, there was no significant difference in blood loss among control and treatment groups.
The use of tranexamic acid in geriatric hip fracture fixation surgery is not associated with an increase in post-operative CVA, MI, PE or DVT. This is consistent with the current literature regarding the safety of using intravenous tranexamic acid perioperatively.
There are some limitations to our study, which is a single-centre retrospective study without randomisation. The surgeries were performed by surgeons with various levels of experience, ranking from basic surgical trainees (1–2 years’ experience), higher orthopaedic trainees (3–6 years’ experience) to specialists (> 6 years’ experience). The surgeon's level of expertise may have affected the degree of blood loss.
Different anaesthetists were also involved in our patients’ care. The decision for initiating intra-operative red cell transfusion is partially anaesthetist dependent.
A multicentre randomised control trial testing different regimes for administration of tranexamic acid (e.g. single dose vs multi-dose, higher vs lower dose, different timing of administration) would be useful to further elicit the effect of intravenous tranexamic acid on geriatric hip fracture surgery. We may also analyse the effect of tranexamic acid on arthroplasty operations for geriatric hip fracture.
Supplemental Material
sj-docx-1-otr-10.1177_22104917261451431 - Supplemental material for Safety and efficacy of single dose IV tranexamic acid in geriatric hip fracture fixation surgery
Supplemental material, sj-docx-1-otr-10.1177_22104917261451431 for Safety and efficacy of single dose IV tranexamic acid in geriatric hip fracture fixation surgery by Kwok Rosaline Hiu-mun and Tse Yu Nang Benny in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Acknowledgements
We used the STROBE cohort checklist when writing our report. 14
Ethics consideration
This study was approved by and conducted according to regulations set by the Hospital Authority Clinical Research Ethics Review (HA CRER) committee.
Consent to participate
Informed consent was waived for this retrospective cohort study. Patients under study have already undergone appropriate treatment for their hip fracture per clinician's decision and the department protocol.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.