
Abstract
Background
The use of three-dimensional (3D) navigation percutaneous screw fixation has been reported in non-displaced or minimally displaced pelvi-acetabular fractures. For carefully selected displaced acetabular fractures, 3D navigation technique can be applied, which traditionally required open approach.
Methods
From 2018 to 2024, 29 patients underwent 3D-guided navigation percutaneous screw fixation. Various reduction techniques were used. Functional and radiological outcomes were assessed.
Results
Twenty-four patients were followed up after definitive fixation with average duration of 33 months. All patients showed fracture union with average union time of 7.3 months. The mean Merle d’Aubigne and Harris Hip scores were 14.3 and 86.2 points, respectively. Younger age, lower injury severity score and earlier definitive operation correlated with improved functional outcome. Percutaneous fixation demonstrates advantages in terms of operative duration, blood loss, length of stay.
Conclusion
This surgical technique safely and effectively manages pelvi-acetabular fractures, resulting in pain relief, early mobilization and favourable patient outcomes.
Introduction
Pelvi-acetabular fractures, while uncommon, have historically been associated with substantial morbidity and mortality. Different surgical options are available for fixation of pelvi-acetabular fractures, including traditional open reduction and internal fixation (ORIF), minimally invasive percutaneous screw fixation (MIS), external fixation and a combination of the above techniques.
An upward trend in acetabular fracture incidence is observed globally, predominantly in geriatric patients.1–3 This is attributable to demographic shifts, greater utilization of advanced imaging modalities and enhanced trauma resuscitation and intensive care. Minimally invasive approaches have gained favour in this subgroup due to their ability to minimize operation time and intra-operative blood loss, as significant proportion of geriatric patients may not tolerate the magnitude of open acetabular surgery.
This retrospective review aims to: (1) identify reduction techniques demonstrating feasibility of three-dimensional (3D) navigation MIS, (2) recognize the benefits and pitfalls of navigation and percutaneous techniques and (3) evaluate early and mid-term radiological and functional outcomes.
Materials and methods
Data collection
Between January 2018 and October 2024, 29 patients with displaced pelvi-acetabular fractures underwent 3D-guided navigation MIS at a single trauma tertiary hospital. Pre-operative data including patient demographics, mechanism of injury, Injury Severity Score (ISS), time to definitive surgery were recorded. Fracture characteristics were evaluated. Peri-operative data including operating time, blood loss, need for 3-in-1 activation, length of stay were noted. Post-operatively, mobility status, functional scores (Merle D’Aubigne (MDA) and Harris Hip scores (HHSs)), reduction quality using Matta's criteria and radiological outcomes with fracture union, union time were recorded. Complications including infection, neurovascular injury, fracture non-union and implant breakage were documented.
Inclusion and exclusion criteria
Inclusion criteria encompassed adults aged over 18 years presenting with displaced pelvi-acetabular fractures, complete radiological and functional outcome records and admission within study period. Exclusion criteria were paediatric cases, non-displaced pelvi-acetabular fractures, isolated pelvic fractures and those treated conservatively.
Primary and secondary outcomes
Primary outcomes assessed were functional and radiological results following 3D-guided navigation MIS percutaneous screw fixation. Secondary outcomes included identification of factors influencing functional outcome (ISS, patient age, time to definitive surgery, reduction quality).
Statistics
Statistical analysis was completed using SPSS for Windows version 21.0.0 (SPSS Inc., Chicago, IL, USA). Spearman's rank correlation coefficient was used to delineate potential correlation between numerical variables. A p-value of 0.05 was considered statistically significant.
Operative details
All patients with pelvi-acetabular fractures underwent definitive fixation by a team of Orthopaedic trauma surgeons. Some patients necessitated trauma activation in the Accident & Emergency resuscitation room. Haemodynamically or mechanically unstable cases required 3-in-1 damage control protocol with external fixation, retroperitoneal packing, angiography and embolization. Additional femoral spanning external fixation was performed in certain cases. Haemodynamically stable cases were initially managed with pelvic binder and sent to Intensive Care Unit for close monitoring or directly admitted to the general Orthopaedic ward. The protocol devised in our tertiary centre guided subsequent management (Figure 1).
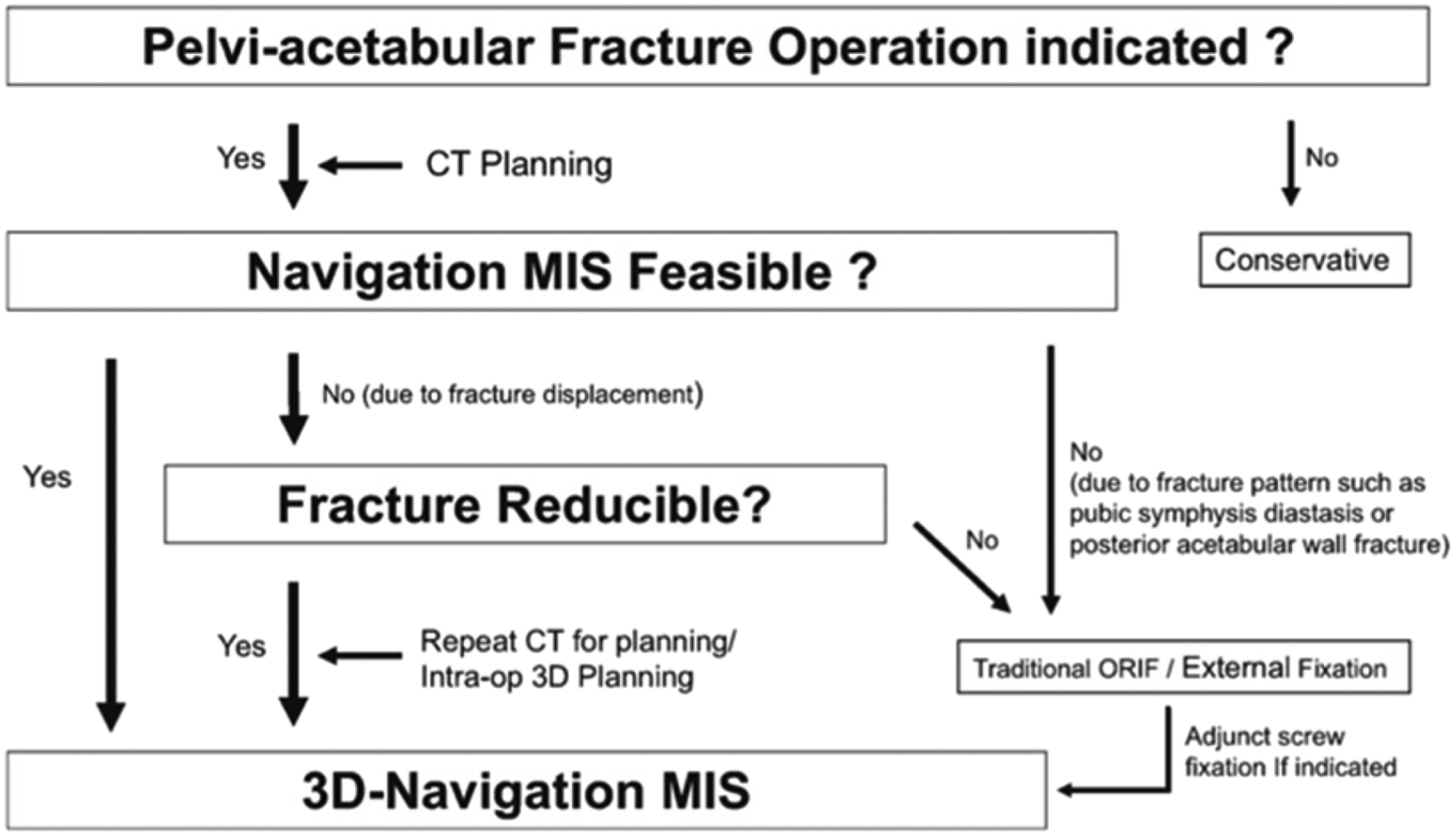
Protocol for definitive fixation of pelvi-acetabular fracture in our centre.
Fracture characteristics, local and patient factors are important selection criteria that dictate MIS feasibility. Fracture step and gap must be reducible by interfragmentary compression. Posterior acetabulum fractures with associated posterior hip dislocation require ORIF for buttressing of posterior wall. Open fractures or those with Morel-Lavallee injuries are relatively contraindicated for ORIF. Patients with concomitant injuries, need for prolonged bedrest and low premorbid functional status may be more suited for MIS. Nevertheless, patients should always be consented for possible conversion to traditional ORIF.
Pre-op navigation planning, assess MIS feasibility
Digital Imaging and Communications in Medicine data was extracted from the pelvic computed tomographic (CT) scan and analyzed on the navigation computer for planning of screw position, trajectory and length. Standardized screw fixation was performed for specific fracture patterns (Figure 2).
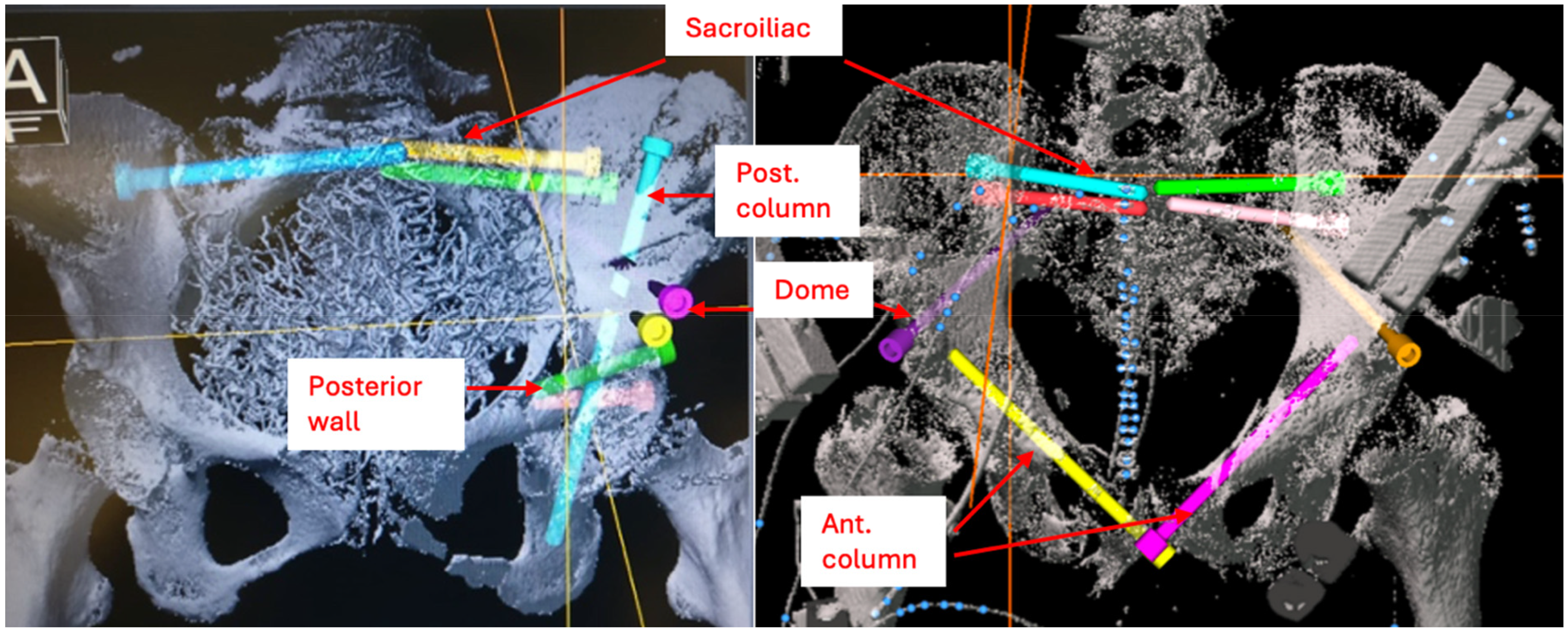
Pre-operative planning images showing the different screw strategies used to tackle pelvi-acetabular fractures. Pre-operative CT scan of the pelvis is analyzed with 3D navigation computer software. Ideal screw entry, trajectory, length and diameter can be adjusted to obtain maximal bone purchase and fracture stability within the narrow bony corridors of the pelvis and acetabulum. In this example, bilateral sacroiliac, posterior column, dome and posterior wall screws. Each set of screws is colour-coded to differentiate between them in pre-operative planning and intra-operative execution. 3D: three-dimensional; CT: computed tomography.
Operative setup
All patients were stabilized for early appropriate definitive surgery. Definitive fixation was performed with patient supine on radiolucent table. The Stryker NAV3i navigation system was positioned at caudal end of radiolucent table, and connected to the Ziehm Flat Panel 3D C-arm, placed on contralateral side of acetabulum (Figure 3). Ipsilateral lower limb was draped for intra-op manipulation and traction during reduction (Figure 4).

Operative setup for navigation minimally invasive percutaneous screw fixation (MIS) surgery.
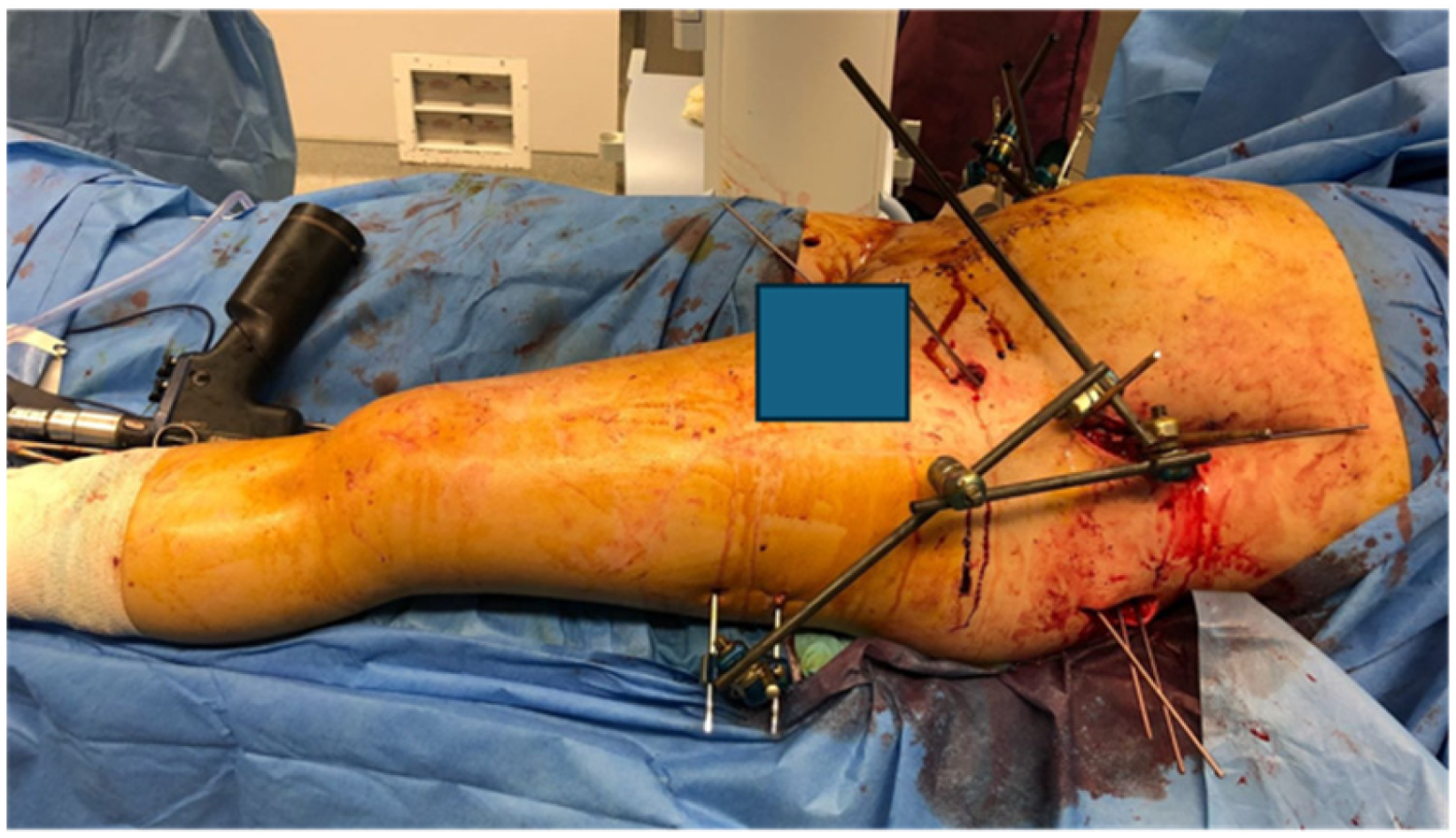
Draping of lower limb for femoral pin insertion and reduction manoeuvres.
Patient reference trackers were calibrated after fracture reduction. Intra-operative 3D fluoroscopic scan of the pelvis was merged with pre-operative 3D scan. If complete match was established, guidepin insertion can proceed (Figure 5). Mismatch suggests fracture displacement and requires re-planning or repeated closed reduction. Patient tracker position must remain static throughout to ensure accuracy of navigation system.
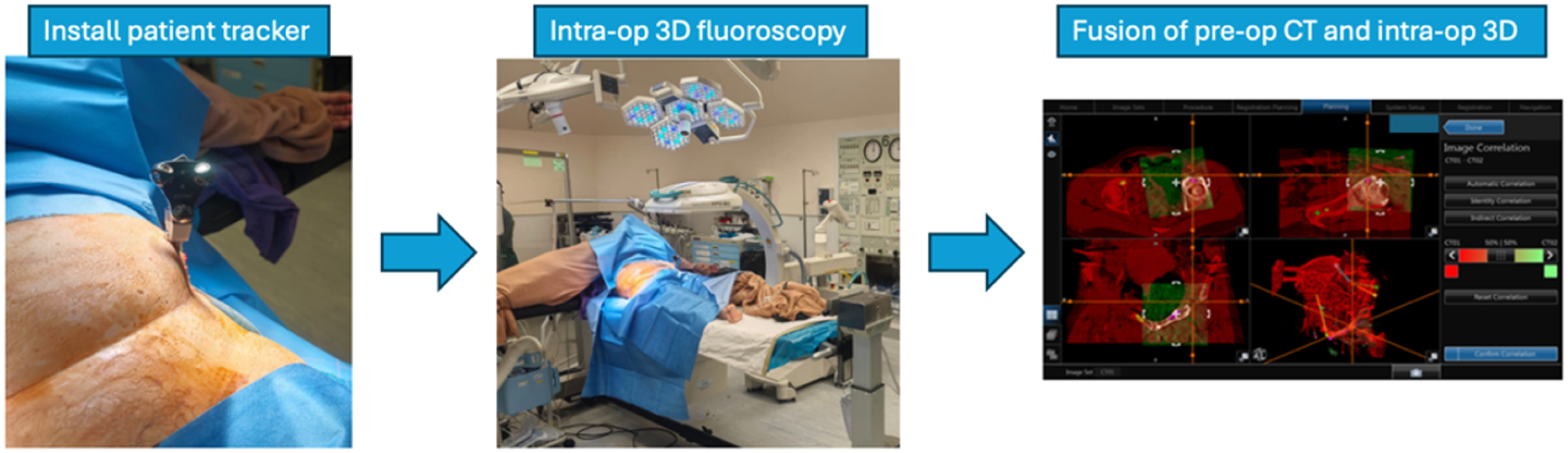
Flowchart for ensuring pre-operative planning can be replicated intra-operatively.
Fracture reduction and fixation strategy
Fracture reduction was achieved with external fixator frame and manoeuvres including longitudinal traction, combined with hip abduction, external or internal rotation. Direct pressure to the ischial tuberosity can be applied. Joystick extension and rotation of the iliac crest fragment realigns high anterior column fractures.
Navigation execution
3.2 mm drill-tip guidepins were inserted with reference tracker calibrated onto the rigid drill sleeve. Its position was verified with both navigation system and fluoroscopy. Partially-threaded 6.5 mm cannulated titanium screws with washers were inserted. Fully threaded screws were used in osteoporotic bone if interfragmentary compression was not required. Washers were avoided if screw heads were near joint edge to reduce femoral head impingement. Sequential tightening provided interfragmentary compression. Final x-rays were checked. Post-operatively, patients underwent limb mobilization and appropriate weight-bearing walking exercises.
Results
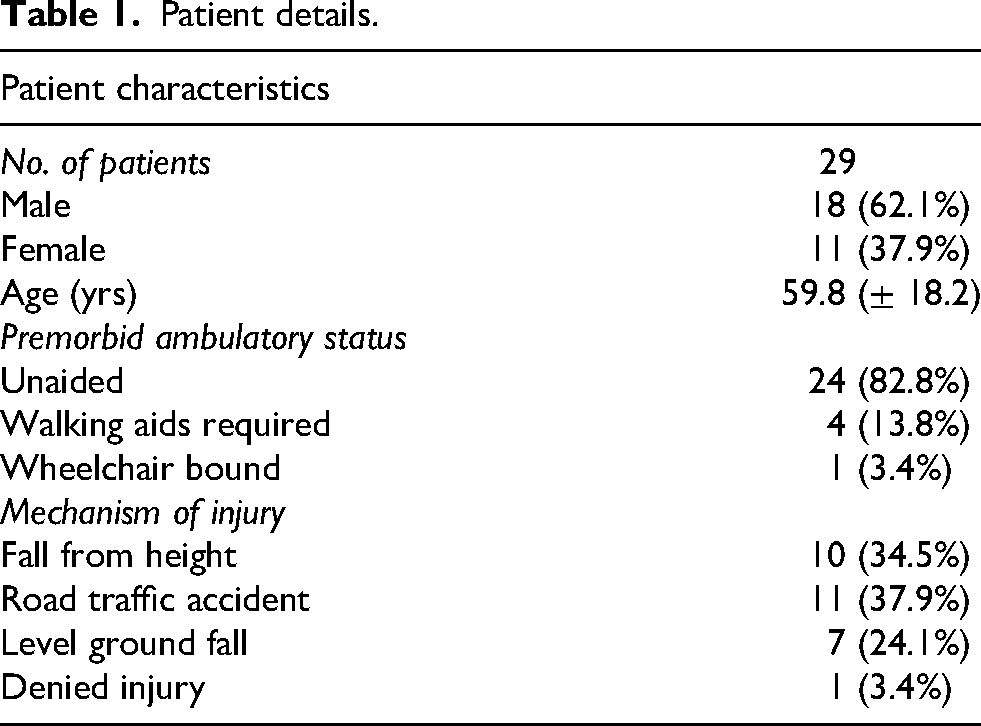
In total, 29 patients with displaced pelvi-acetabular fractures were managed with 3D-guided navigation percutaneous screw fixation from 2018 until 2024. Their patient details and characteristics are shown in Table 1. The mean age was 59.8 years (17–90 years), with bimodal distribution. The mean ISS was 18.6. Elderly patients generally suffered from a level ground fall (24.1%). Younger patients generally suffered from high-energy injury, including fall from height (34.5%) and road traffic accident (37.9%). One elderly gentleman with delirium claimed not to have sustained any injury. Prior to injury, twenty-four patients walked unaided, three ambulated with stick, one with frame and one patient was wheelchair dependent.
Patient details.
Fracture characteristics are listed in Table 2. The mean time from admission to definitive fracture fixation was 4.4 ± 3.0 days (CI 3.2, 5.5). Eleven (41.4%) of the patients required activation of 3-in-1 damage control protocol. Twenty-seven (93%) patients underwent MIS. One case required combined MIS and ORIF via the modified Stoppa approach for fixation of anterior column and acetabular dome. One case required combined MIS and ORIF via Kocher-Langenbeck approach to access the posterior wall. Mean total operative time was 164 min (range, 67–306 min) and mean operative blood loss was 200 ml (range, 5–1200 ml).
Patient details and fracture characteristics.
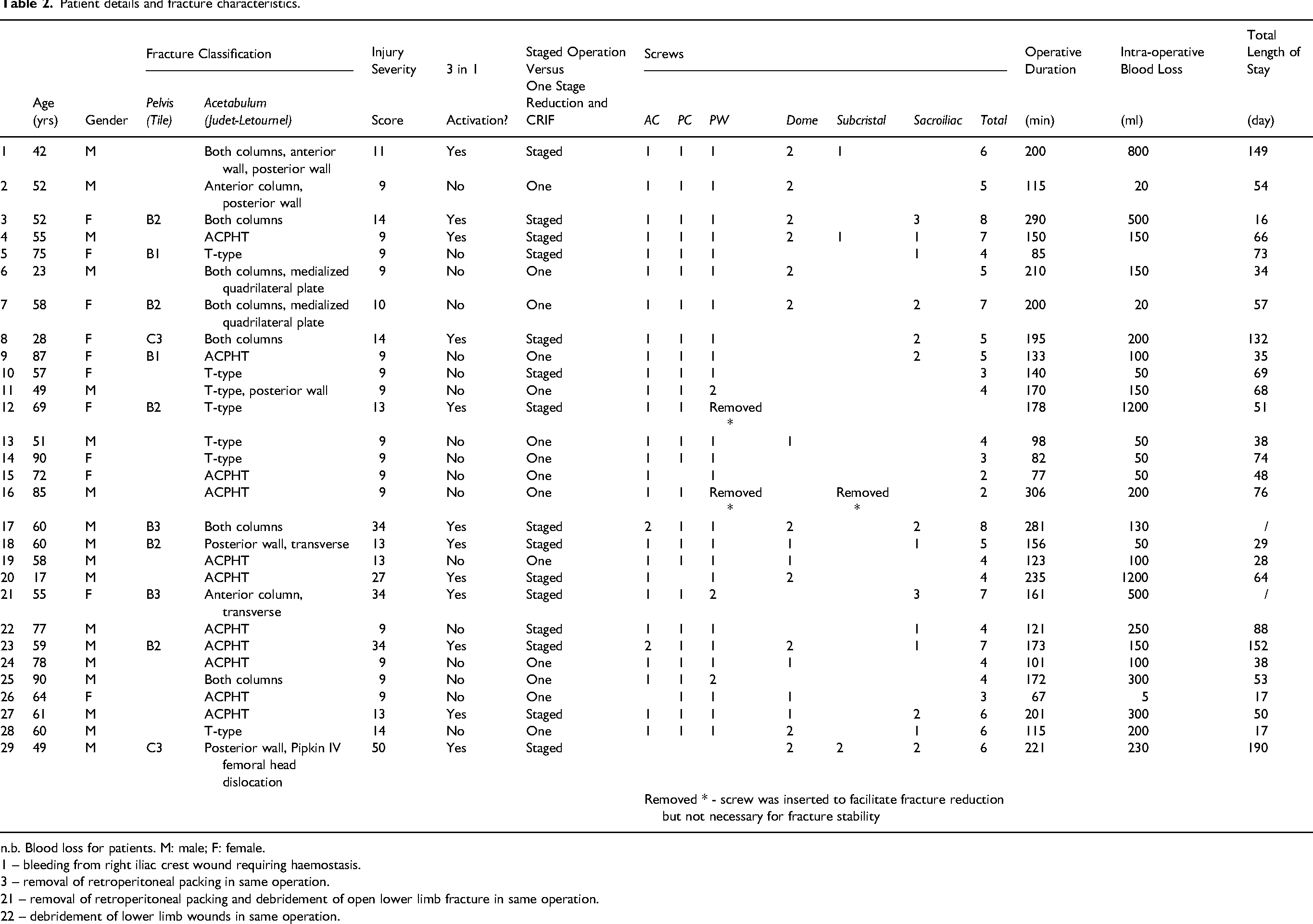
n.b. Blood loss for patients. M: male; F: female.
1 – bleeding from right iliac crest wound requiring haemostasis.
3 – removal of retroperitoneal packing in same operation.
21 – removal of retroperitoneal packing and debridement of open lower limb fracture in same operation.
22 – debridement of lower limb wounds in same operation.
Fifteen (51.7%) patients were permitted non-weight-bearing walking after definitive operation, ten (34.5%) patients partial weight-bearing and four (13.8%) patients immediately allowed full weight-bearing. Four patients that required non-weight-bearing suffered from concurrent lower limb peri-articular fractures.
Twenty-one of the 29 patients were admitted to Intensive Care Unit with average length of stay of 10 days. Average length of stay in general Orthopaedic ward was 23.0 days (range, 4–114 days), while average convalescent period was 42.9 days (range, 9–135 days).
Twenty-four patients were followed up post-operatively. Three patients returned to their home country and two patients passed away during hospitalization, one from injury-related sequelae and one from non-injury-related medical conditions. Eventually, 14 patients walked unaided and seven patients were ambulatory with walking aids. Three patients were wheelchair bound, of which one already required wheelchair prior to injury. Functional and radiological outcomes are listed in Table 3. The mean modified MDA score was 14.3 ± 1.3 points (CI 12.9, 15.6). The mean HHS was 86.2 ± 12.0 points (CI 74.2, 98.2)(Table 3).
Functional and radiological outcomes.
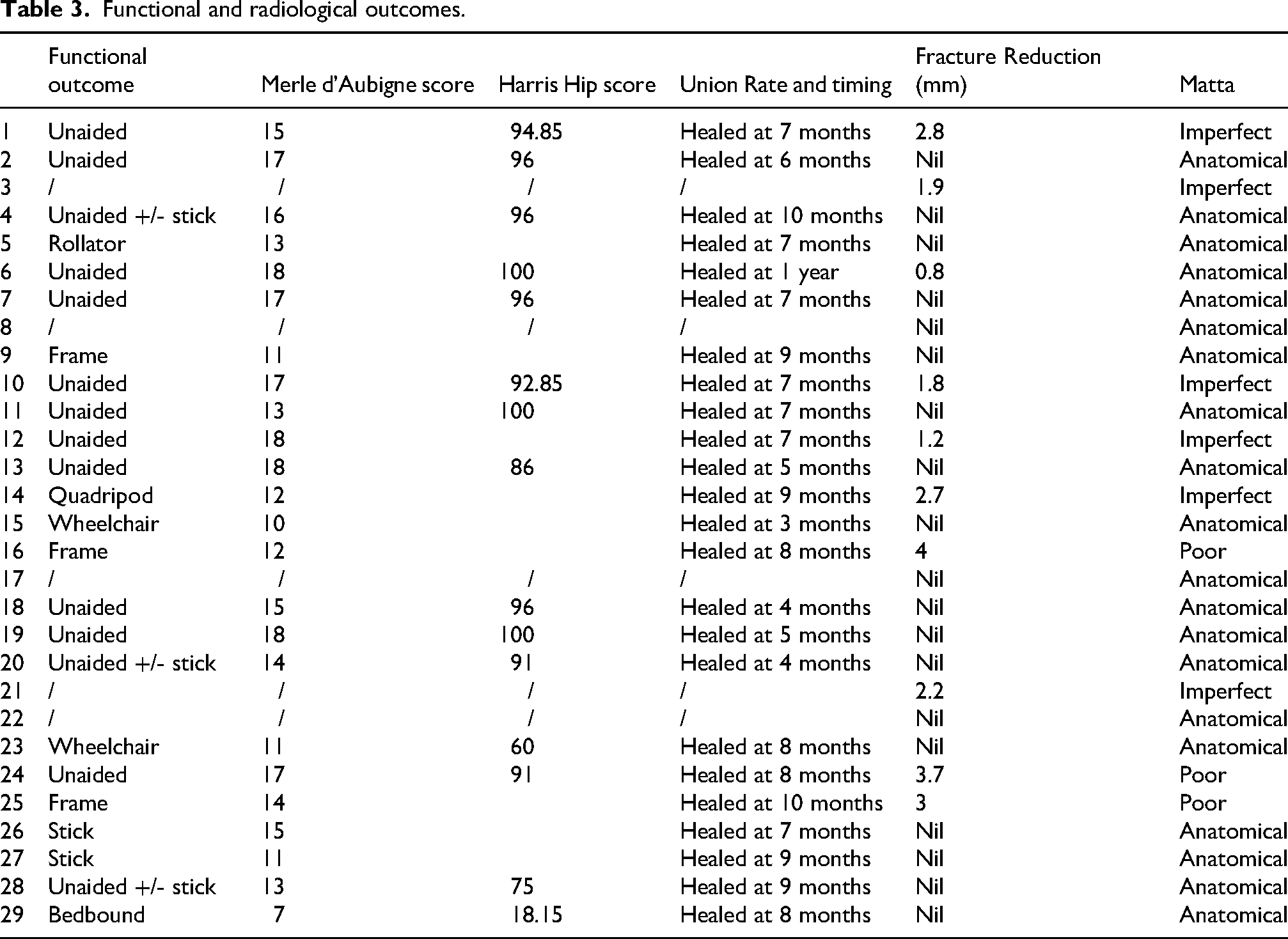
Radiological outcomes were satisfactory. Twenty patients had anatomical reduction (69.0%), six imperfect (20.7%) and three poor (10.3%). Twenty-four patients with continuous follow-up showed fracture union with mean union time of 7.3 months. The average follow-up duration was 33.4 months. Ten patients underwent CT assessment for fracture union between 6 and 12 months post-operatively, all showed interval or fully healed fractures. Six of 11 patients with follow-up of at least three years showed signs of hip joint osteoarthritis changes. All were asymptomatic with good range of motion.
Spearman rank correlation coefficient was utilized to measure the relationship between variables with eventual functional outcome (MDA and HHS), which included patient's age, ISS, time to definitive operation and reduction quality, which is presented in Tables 4 and 5.
Data for calculation of Spearman correlation coefficient for various variables with MDA score.
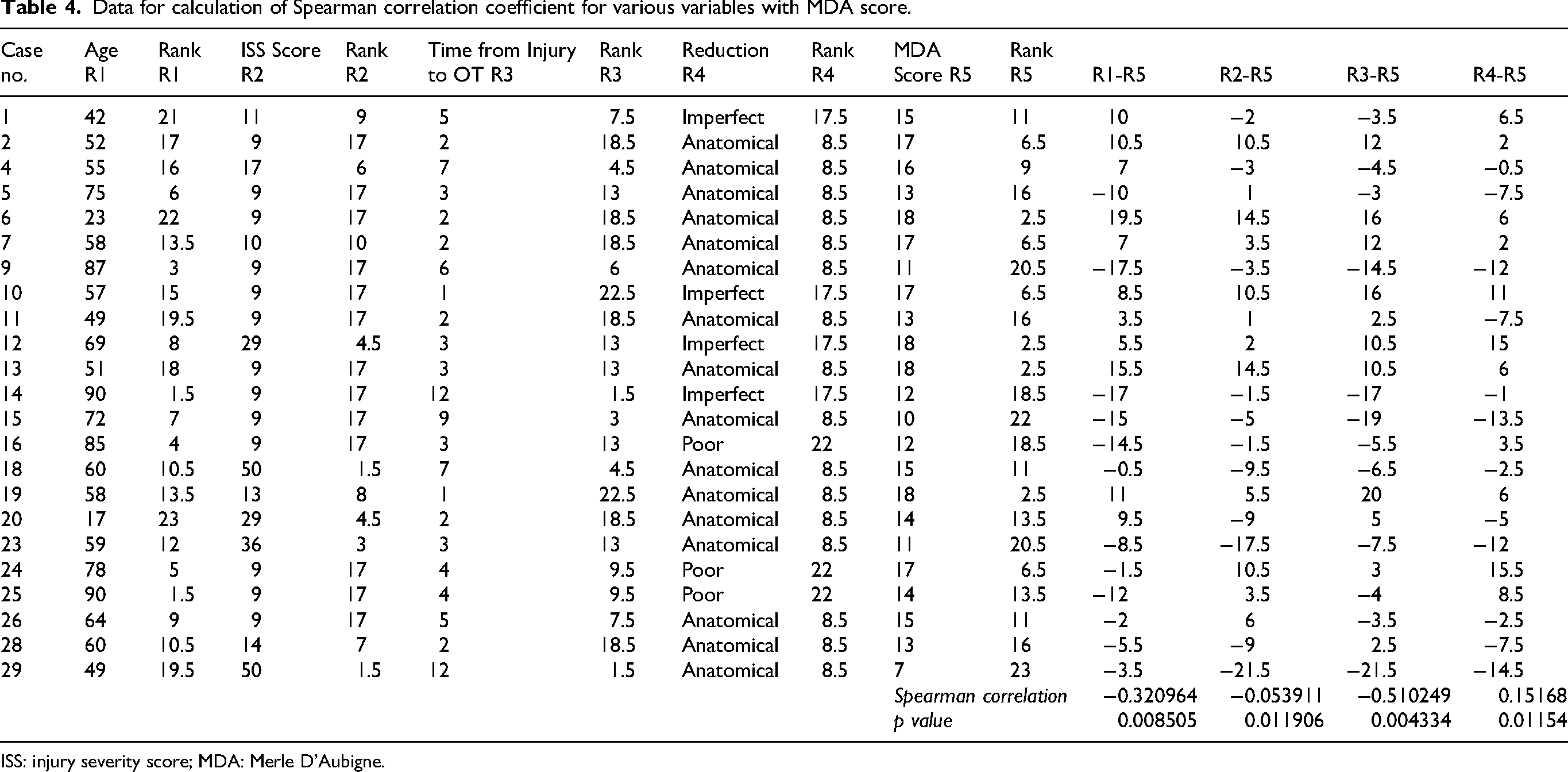
ISS: injury severity score; MDA: Merle D’Aubigne.
Data for calculation of Spearman correlation coefficient for various variables with HHS.
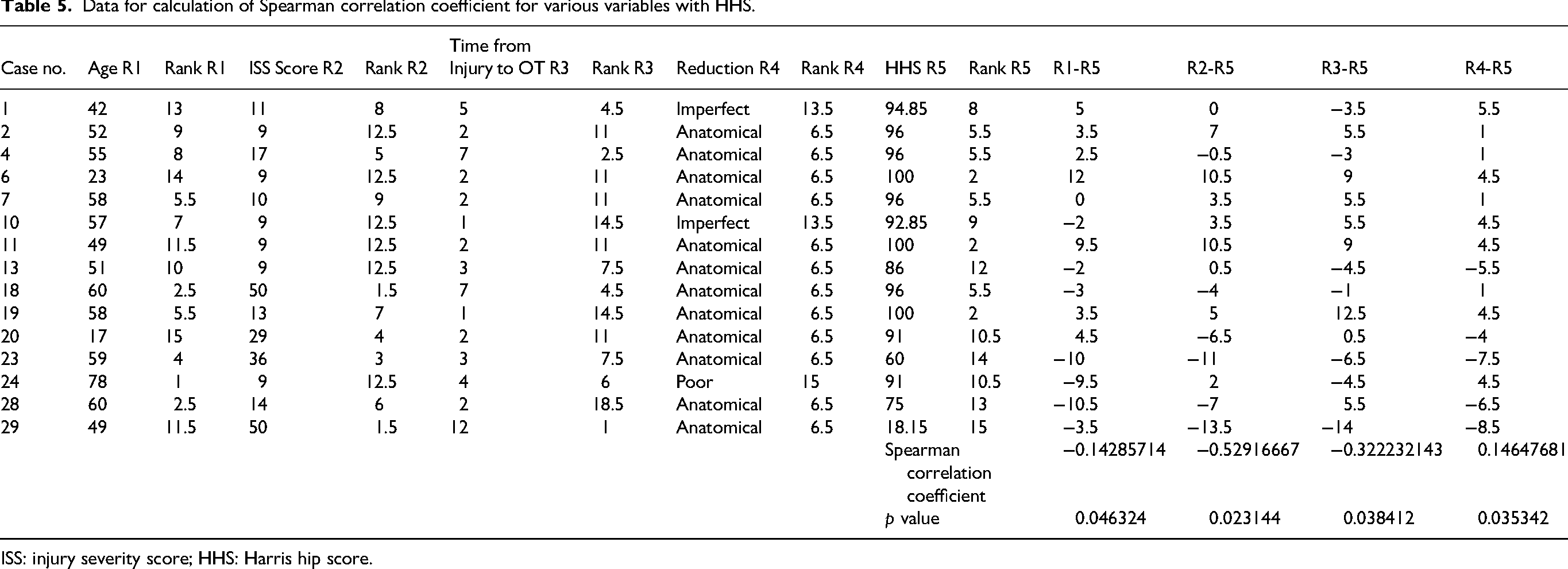
ISS: injury severity score; HHS: Harris hip score.
There were two cases of post-operative screw migration and one case of broken drill bit. The two screws had backout of 12.2 and 16.8 mm, both were asymptomatic and did not require removal. The broken drill-bit was identified intra-operatively. Avoid broken drill-bits by using single-use, straight-tipped drill-bit with linear advancement. One patient suffered from pseudoaneurysm over gluteus minimus due to iatrogenic vessel injury upon surgical incision. Wounds should be enlarged, explored if profuse bleeding and adequate haemostasis should be achieved, with drains inserted to avoid haematomas.
Elderly and young patients are physiologically different in nature with different injury mechanisms and treatment goals. A further subgroup analysis was conducted for comparison and the data is presented in Table 6.
Elderly and young patients sub-group analysis.
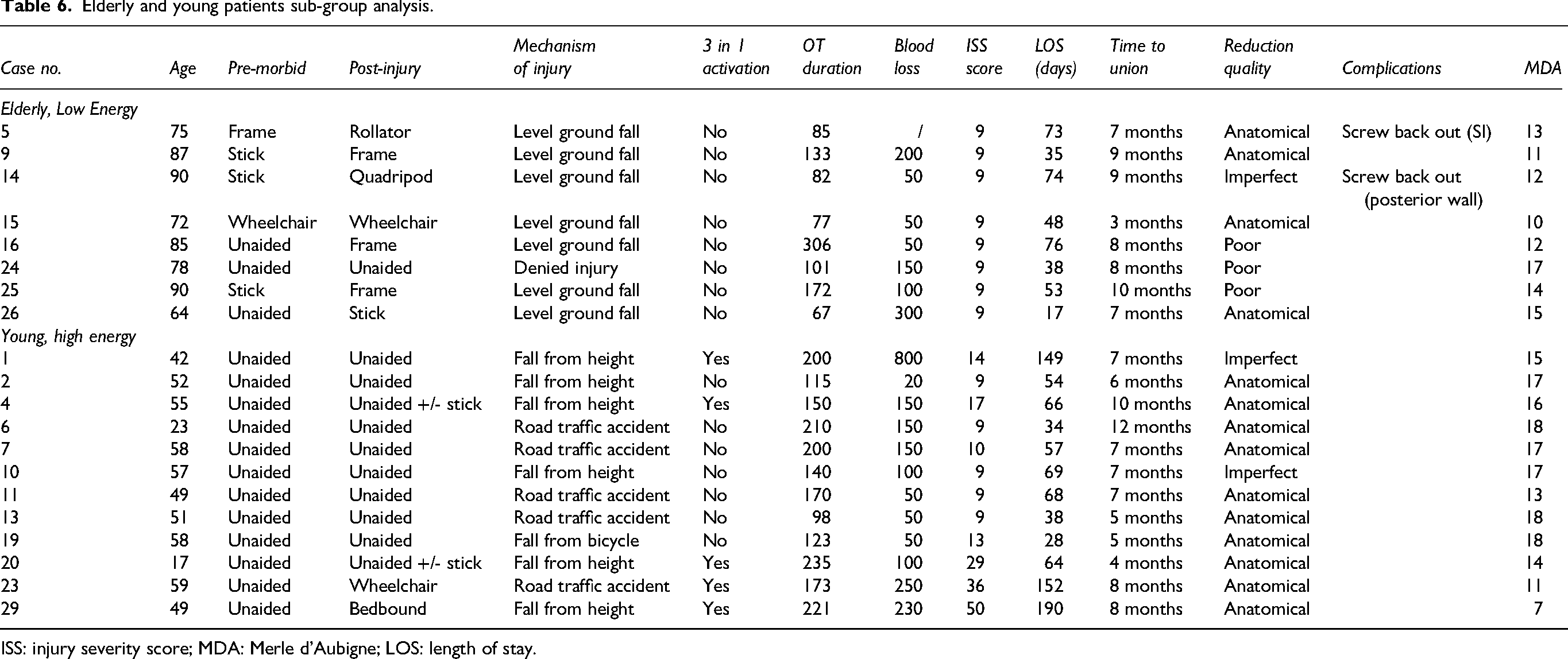
ISS: injury severity score; MDA: Merle d’Aubigne; LOS: length of stay.
Eight elderly patients with pelvi-acetabular fractures after low-energy injury were compared with twelve younger adults who suffered from high-energy trauma, with average ISS score of nine and 18 in the two respective groups. None of the elderly patients required activation of 3-in-1 protocol, as compared with five in younger patient group. Operative duration and intra-operative blood loss was lower in the elderly low-energy group, with average of 130 min and 130 ml blood loss, whereas the younger high-energy group had average of 170 min operation duration and 175 ml blood loss. Average length of stay of 52 days in elderly patients was lower than the average stay of 81 days in younger high-energy patients.
Two of eight patients maintained same ambulatory status compared to pre-morbid and only one was able to walk unaided. In contrast, 10 of the 12 younger patients regained same ambulatory status and walked unaided upon follow-up. All fractures in both subgroups healed, with average union time of 7.6 months in elderly patients and 7.2 months in younger patients. Four of eight elderly patients had anatomical fracture reduction, versus 10 of 12 younger patients, which may be due to underlying osteopenic bone quality of elderly patients and overall different treatment goal for surgical fixation. Two elderly patients suffered from eventual screw backout, potentially attributable to osteopenia. The average MDA score in the elderly subgroup was 13 points, versus 15.1 points in younger subgroup.
Discussion
Reduction techniques
One staged articular reduction, column reduction and fixation
Lag screw insertion of posterior wall for reduction of medialized quadrilateral plate depends on integrity and bone quality of quadrilateral plate fragment. Screw entry should be planned away from greater sciatic notch to avoid inadvertent injury to the exiting neurovascular structure. Screw tip should be planned inferior to and away from pelvic brim to avoid the corona mortis and external iliac vessels (Figure 6). 4 New, sharp, fluted drill bits should be inserted at full speed and slow advancement to avoid displacing fragment medially and overshooting when drilling through the quadrilateral plate. Bone quality contributes to the success of interfragmentary compression. Two screws can be inserted in osteopenic bone to share compression effect, thereby minimizing screw pull-out risk. Adequate screw length is necessary for interfragmentary compression to engage the far cortex. If considerable length of screw tip protrudes through quadrilateral plate, it may be removed after column stabilization. Sequential tightening of the screws ensures uniformly distributed stress across the fracture site and prevents malalignment. Figure 7 depicts the above technique.

Percutaneous lag screw (in purple) insertion of posterior wall for reducing medialized quadrilateral plate. Screw entry should be away from greater sciatic notch (seen in 3D reconstruction of pelvis on the right) to avoid iatrogenic injury to sciatic notch and superior gluteal neurovascular bundle. Screw trajectory should avoid the pelvic brim to prevent injury to external iliac artery, corona mortis and obturator nerve as seen on coronal and axial section of the pelvic CT. 3D: three-dimensional; CT: computed tomography.
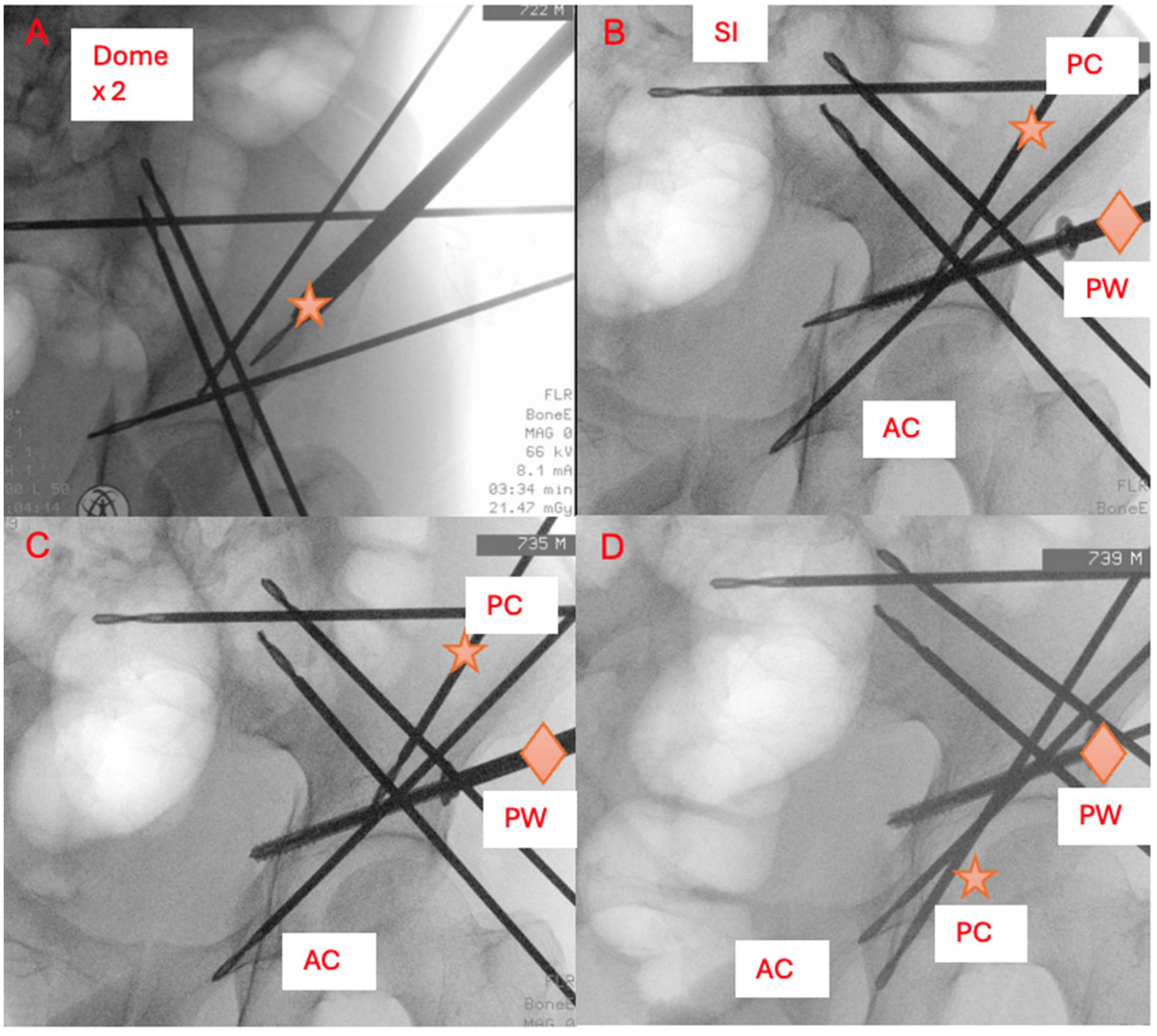
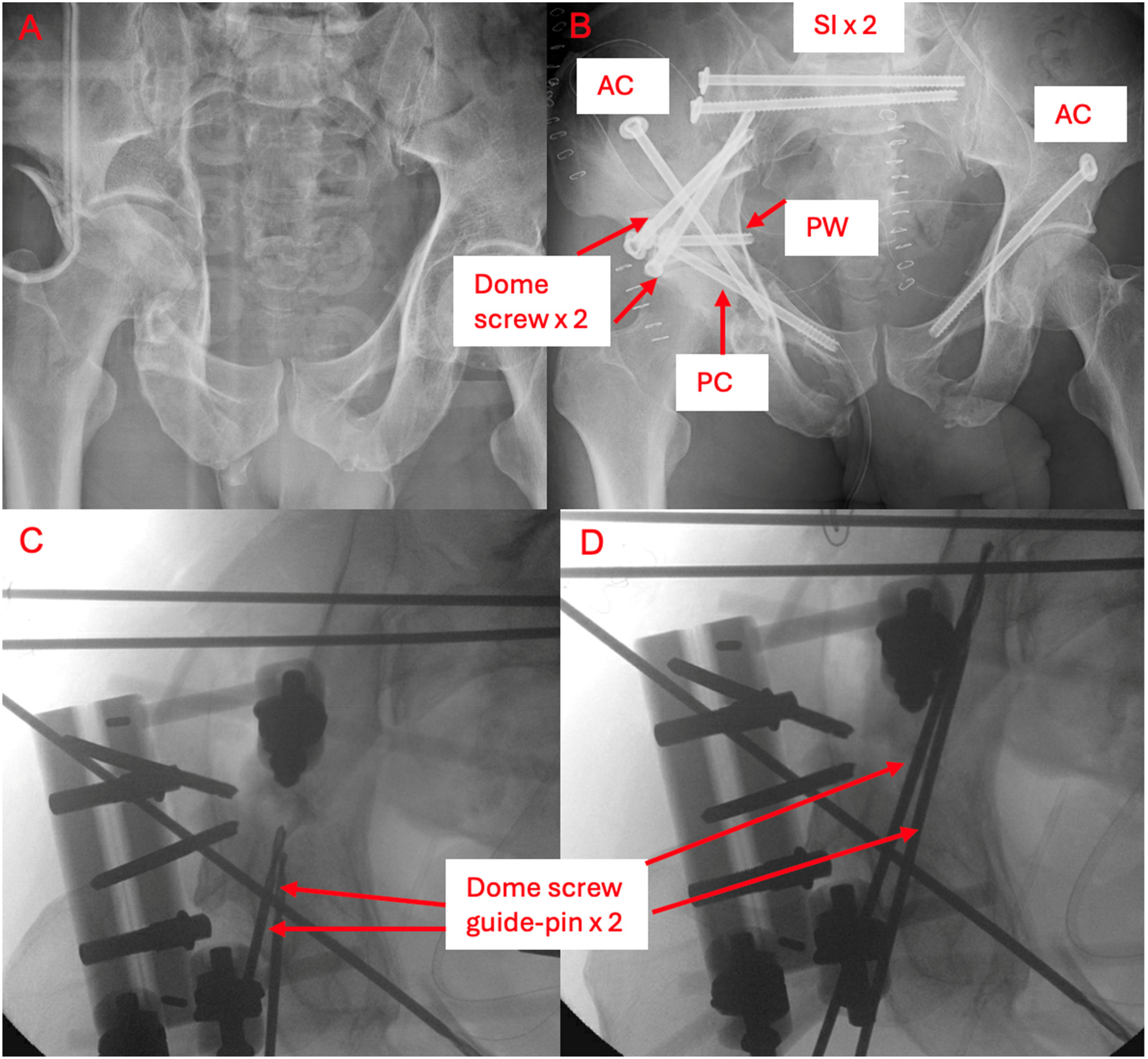
A 60-year-old male (Patient 28) suffered from a T-type fracture of the acetabulum. (a) Initial pelvic x-ray shows medialized quadrilateral plate. (b) Guide-pins for the sacroiliac screw, two dome screws, posterior wall screw, anterior column screw are first inserted and partial insertion of posterior column guide pin just proximal to the fracture site, all under navigation guidance. (c) Subsequently, the posterior wall screw is gently tightened under x-ray guidance to reduce the displaced quadrilateral plate. (d) After reduction, the PC guide-pin can be further inserted to the ischial tuberosity under x-ray guidance as the hip joint has been reduced satisfactorily.
Navigation-guided reduction of articular depression
Articular depression typically requires elevation with open method to attain a congruent articular surface. The navigation system can be utilized to simulate screw insertion to site of articular depression, which can be then used to create a window for placing instruments to dis-impact the articular depression (Figure 8).
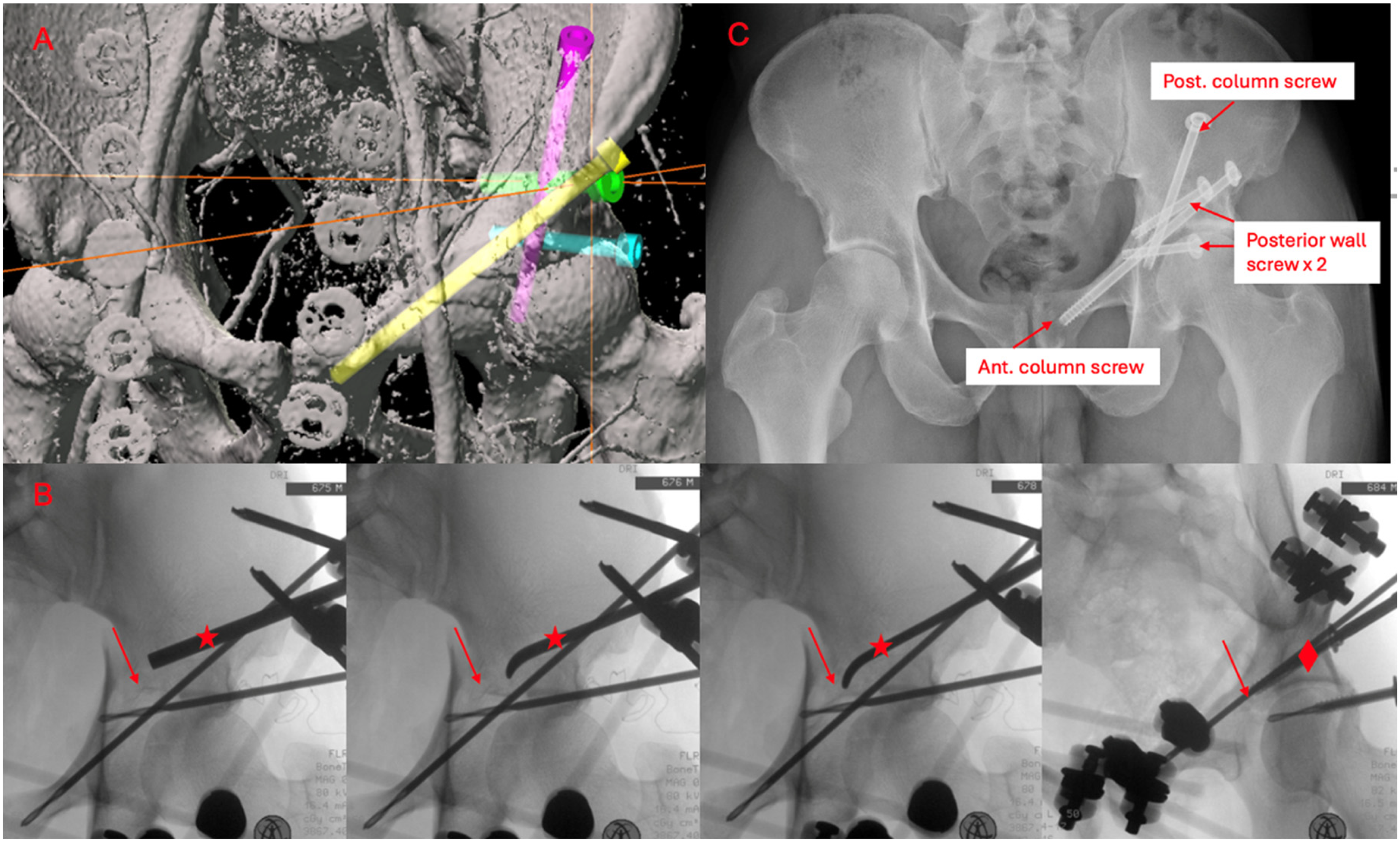
A 49-year-old male (Patient 11) suffered from transverse and posterior wall fracture with significant articular depression due to dome impaction after fall from height. Normally, elevation of articular depression requires open approach. (a) Navigation planning was performed for potential insertion of multiple screws over the dome impaction. (b) The first screw trajectory planning (green) was used for opening of the lateral iliac cortex and further widened with 6.5 mm drill for insertion of bone spike and bone punch for dis-impaction of articular depression. The blue screw ‘rafted’ the reduced congruent hip joint (a). (c) The fracture healed at 7 months post-operation and the patient was able to walk unaided.
Mini-open reduction followed by MIS
Additional carbon rods from the external fixator frame can be used to provide a manual buttressing effect for reduction of the fracture fragment via a small open wound, to allow for guidepin cannulation and ultimately screw fixation (Figure 9). This can be as an adjunct in addition to femoral traction and posterior wall interfragmentary compression screw.
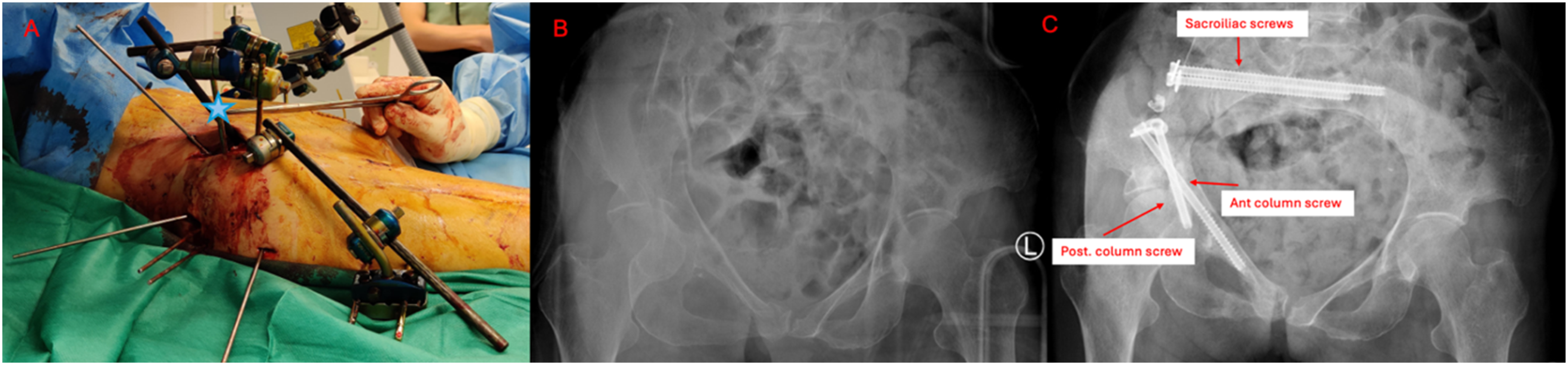
(b) A 69-year-old female (Patient 12) sustained a Tile B2 and T-type pelvi-acetabular fracture after road traffic accident. Femoral traction and posterior wall interfragmentary compression screw were inadequate for reduction of quadrilateral plate. (a) Further manual buttressing with locked carbon rod (blue diamond) through a lateral iliac window was required. The posterior wall screw was removed after insertion of the anterior and posterior column screws due to loss of screw purchase. (c) The reduced acetabulum was successfully held in place by two column screws.
One-stage repeated reduction and fixation
Repeated loosening and tightening of external fixator with reduction manoeuvres allows fixation of certain fracture fragments (Figure 10). With sequential partial reduction done, intra-op 3D fluoroscopy can be repeated to assess the congruency of the articular surface (Figure 11). Once articular congruent reduction is achieved, the remaining fracture fragments can be fixed percutaneously.
(a) A 60-year-old male (Patient 17) fell from height and suffered from Tile B3 and associated both columns pelvi-acetabulum fracture with femoral head protrusion. MIS fixation was infeasible due to significant fracture displacement. Articular comminution rendered anatomical reduction unachievable despite open reduction. Primary total hip replacement was not suitable due to ‘floating’ nature of acetabulum. The sizable and grossly displaced iliac wing fragment required multiple reduction techniques, including femoral traction, joystick manoeuvre with external iliac pins and direct open reduction. (c, d) The ilium reduction was stabilized with two guidepins for dome screws (lateral column). (b) Repeated intra-op 3D fluoroscopy revealed congruent articular reduction, allowing for MIS fixation of posterior column and posterior wall reduction screws. 3D: three-dimensional; MIS: minimally invasive percutaneous screw fixation.
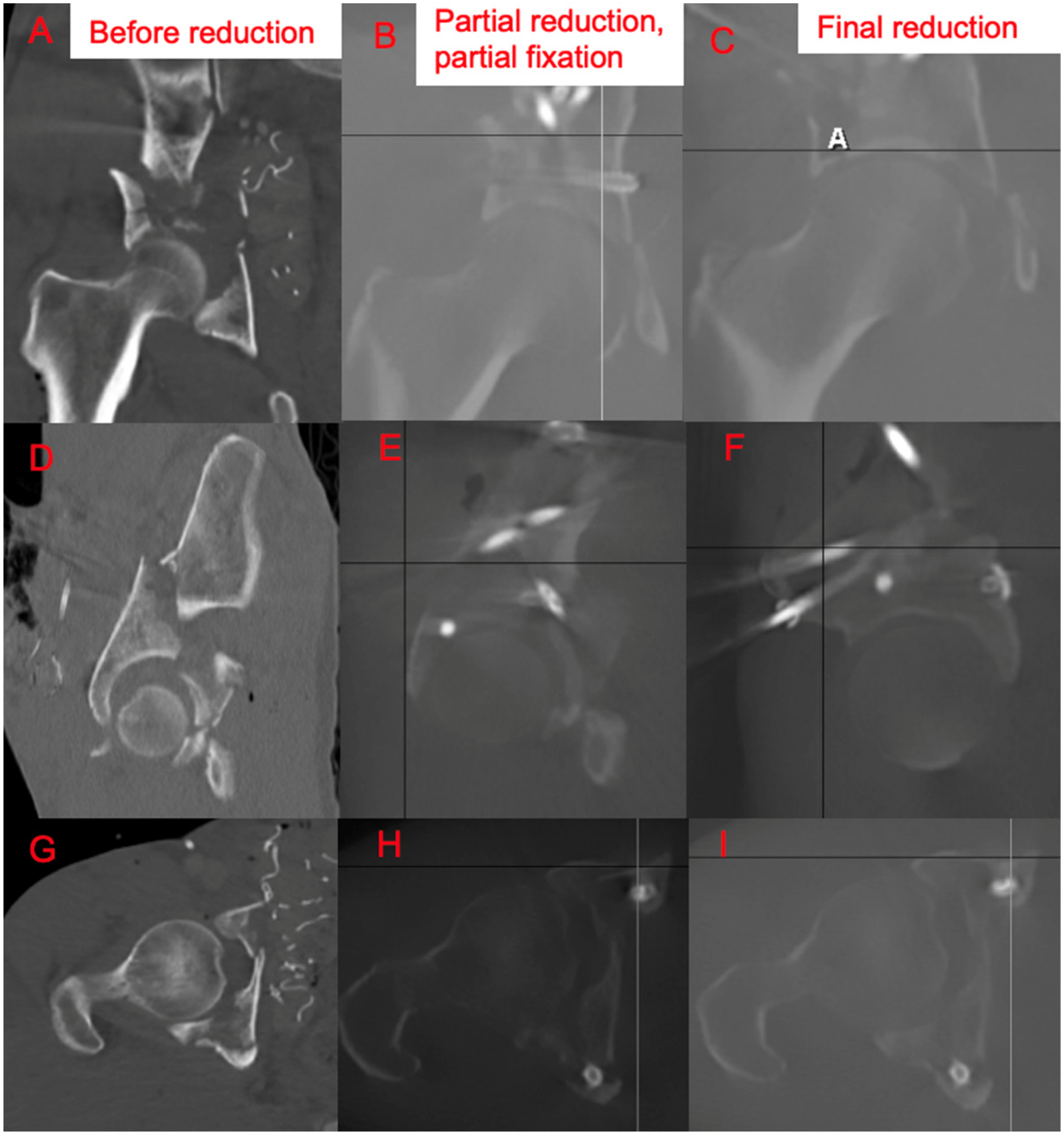
Patient 17 showing the effect of repeated partial reduction and screw fixation with final articular congruity on coronal, sagittal and axial planes of intra-operative three-dimensional (3D) fluoroscopy.
Partially infeasible MIS with conversion to open fixation
Combined approach with both ORIF and MIS navigation screw fixation (Figure 12) depicts the complementary manner of both techniques, shortening operative duration and lowering intra-operative blood loss.

A 49-year-old man (Patient 29) fell from height and suffered Tile C3 pelvic fracture and right side posterior wall fracture acetabulum and posterior hip fracture dislocation. (a) After initial reduction of the posterior hip dislocation, (b) CT scan shows sizable posterior wall fragment which requires buttress plating for stability. (c)However, the contralateral pelvis is amenable to MIS, with two sacroiliac screws (i), two dome screws (ii), anterior column screw (iii) and subcristal screw for fixation of iliac crest (iv). MIS: minimally invasive percutaneous screw fixation; CT: computed tomography
Benefits and pitfalls
The aim of acetabular surgery is anatomical reduction of articular surface, maintain hip joint congruity with stable fixation for early mobilization and appropriate weight-bearing. Traditionally, the universally accepted gold standard treatment for displaced acetabular fractures is ORIF. However, open approaches are associated with higher blood loss, longer operative time, higher rate of wound morbidity including infection, scarring and injury to surrounding structures. Daurka reported that open approach resulted in higher intra-operative blood loss up to 9000 ml and operating time up to 700 min. 5 Subsequently, patients have longer hospital stay and rehabilitation period (Figure 13).
Comparison of the extensive surgical incision of traditional ORIF versus MIS. ORIF: open reduction and internal fixation; MIS: minimally invasive percutaneous screw fixation.
MIS fixation allows shorter operative duration, less intra-operative blood loss, shorter hospital stay and fewer non-surgical related complications. Goyal suggested no difference in quality of fracture reduction between percutaneous and open fixation. 6 Chang's study 7 reported that screw fixation stiffness is equivalent to plate fixation, while Kraemer 8 concluded that lag screw stiffness for transverse acetabular fractures is superior to plate fixation. The screw backout identified in our two asymptomatic cases with timely fracture union could be attributed to dynamization of the intramedullary splintage, aiding secondary bone healing.
Fluoroscopic-assisted screw fixation can be performed with inlet iliac oblique and outlet obturator oblique views, yet two-dimensional (2D) radiographic assessment of the three-dimensional (3D) acetabulum is difficult. Surgeons must identify non-universal landmarks of anterior and posterior columns for accurate placement of screws among different pelvic morphologies. This technique is overall technically challenging, and only 11 of 29 cases were performed by trainees under supervision of consultant orthopaedic surgeons. Repeated intra-operative fluoroscopy usage exposes surgeons, patients and operating theatre staff to elevated levels of radiation, a WHO-classified carcinogen.
Acetabular MIS fixation requires multiple screw strategies around the small peri-acetabular region. The 3D-navigation technique offers increased accuracy and versatility, with higher screw placement accuracy, lower blood loss and radiation exposure. Careful pre-op planning ensures bony corridors around the acetabulum can accommodate multiple screws. The authors believe that cannulated screws of minimum 6.5 mm diameter in acetabular columns function similarly to intramedullary nails in long bones, providing adequate strength with lower risk of implant failure. Screw position, trajectory and length can thus be optimized prior to definitive fixation. Concurrently, the quality of the fracture reduction and congruency of the hip joint can be assessed during pre-operative planning.
Functional and radiological outcomes
MIS technique for acetabular fracture fixation shows good functional and radiological outcomes. All 29 patients were permitted walking exercises post-operatively. Determining post-op weight-bearing status was a multifactorial decision. Patient factors included patients’ overall bone quality, osteoporosis, concomitant peri-articular fractures or spinal injuries with neurological deficit. Fracture factors included articular comminution, presence of bone void and surgeon's tactile feedback of periarticular screw purchase during insertion.
Eventually, twenty of the 24 patients with continuous follow-up were ambulatory. The mean modified MDA score was 14.3 points. The mean HHS was 86.2 points.
Younger age showed weak positive correlation with final MDA score and HHS (Table 7). Eight patients were older than 70 years at the time of injury, of which three required walking aids and one was wheelchair bound. The higher likelihood of medical co-morbidities, lesser physiological reserve may affect rehabilitation process and limit functional recovery.
Spearman correlation coefficient showing potential correlation between various factors with functional outcome.
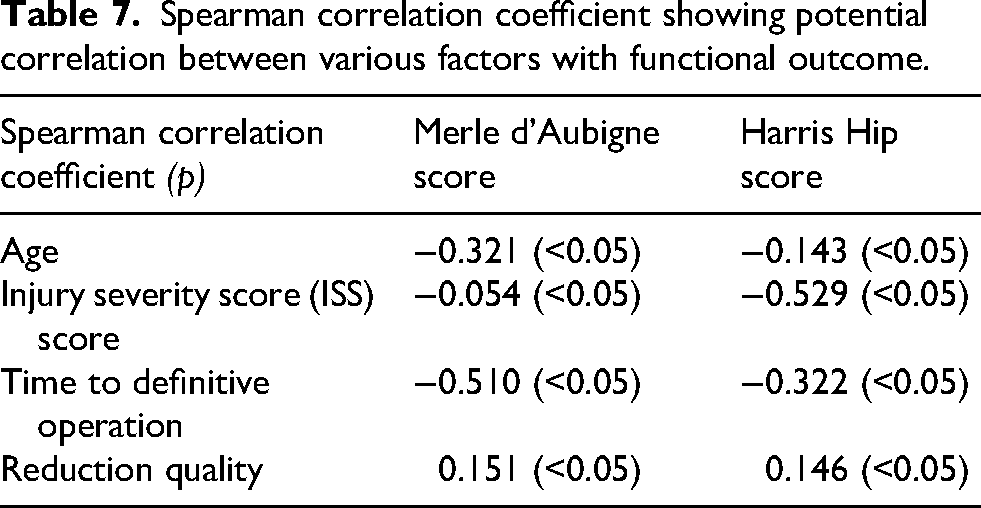
ISS showed moderate correlation with functional outcome (Table 7). A higher ISS correlated with a lower HHS. ISS has been validated to be a strong predictor of mortality, hospital length of stay and functional outcome.
Timely operation is important in achieving a successful reduction. According to Letournel, the ideal timing is 2–6 days after initial injury. 9 If definitive operation is delayed to more than 11 days after injury, possibility of anatomical reduction decreases due to the callus, organization haematoma and granulation tissue formation.10,11 We aim for early definitive care, with mean of 4.4 ± 3.0 days from admission to definitive fixation, partly limited by operating theatre availability and pre-operative CT arrangement difficulties. Our results showed moderate positive correlation between earlier definitive fixation and the final MDA and HHS (Table 7). Currently, the authors advocate for ‘early appropriate care’ with earlier closed reduction and definitive fixation, after the patient has been properly resuscitated and monitored under intensive care.
Fracture reduction is an important predictor of developing post-traumatic osteoarthritis. Matta's criteria classifies quality of fracture reduction by grading residual fracture gap or step on post-operative radiographs. In the beginning of the study period, patients frequently underwent CT assessment for fracture union. Towards the latter half of the study, post-operative CT assessment was less commonly performed, owing to the increasing experience of the surgeons with MIS technique. Quality of fracture reduction only correlated weakly to eventual functional outcome (Table 7). While Letournel found that perfect radiographic outcome correlated with good clinical outcome, we concluded that some patients displayed an excellent MDA or HHS despite imperfect or poor reduction. Starr theorizes that the poorly reduced fracture site lies outside the weight-bearing area of the hip joint. 12 Letournel hypothesizes that the femoral head remains congruent to portion of articular surface large enough to withstand the increased intra-articular pressure. 13 Another explanation may be the paper's relatively short follow-up time and overall advancements in post-operative care and physiotherapy.
Eleven patients were followed up for at least three years after their initial injury. Six showed radiological signs of osteoarthritic changes over the hip joint, three of which had anatomical reductions and three with imperfect reductions. All were asymptomatic with good range of motion of the hip joint observed.
Elderly and young
Elderly patients generally suffer from low-energy injuries which differ from high-energy pelvi-acetabular fractures in younger adults, with haemodynamic instability and fracture displacement less common due to intact ligamentous constraints. They may be unable to tolerate the magnitude of open acetabular surgery. Nevertheless, surgical fixation is recommended to improve pain control and allow early mobilization, reducing adverse effects of impaired ambulation such as major organ infections (e.g. urinary tract infections, pneumonia), pressure sores and thromboembolic events.14,15 Therefore, MIS navigation is a feasible solution for this patient group. Elderly patients typically had shorter operative duration and less intra-operative blood loss, reflecting the lesser magnitude of fracture displacement, thus require less intra-operative manipulation and reduction manoeuvres. The reduction quality in elderly patients was more likely to be imperfect or poor, possibly owing to underlying osteopenic bone quality and overall different goal for surgical fixation. Osteopenia could also explain the reason for two cases of screw backout.
Limitations include small sample size and retrospective design. The heterogeneity of the study population, injury and fracture patterns and concomitant injuries complicates statistical analysis. MIS percutaneous screw fixation demonstrates encouraging functional and radiological outcomes, but future studies with larger patient sample further validates our current results.
MIS percutaneous screw fixation technique does not replace open reduction internal fixation. Our attempted reduction techniques and MIS screw strategy relies on individual fracture lines and its displacement at different parts of acetabulum. Overall, the operative management is “fracture-based” rather than traditional “classification-based.” Both techniques are comprehensive and can be mutually supplementary. Certain fracture patterns or pelvic anatomy may not be amenable to minimally invasive surgery. Non-reducible fractures, comminuted fractures, posterior wall fractures and narrow bony corridor are situations that may require open reduction. Pre-operatively, the patient should always be consented on the possibility of conversion to an open approach if MIS technique is infeasible.
MIS navigation technique can be developed to enhance accuracy and reproducibility of screw fixation in pelvi-acetabular fractures. The use of robotic-guided navigation and reduction or augmented reality can be explored. Intra-operative fluoroscopy can be calibrated with navigation system for precise intra-operative x-ray views to confirm location, trajectory and position of screws.
Conclusion
The potential socioeconomic burden of patients with displaced pelvi-acetabular fractures necessitates prompt diagnosis, appropriate imaging and timely management to achieve pain relief, fracture healing and early mobilization. 3D guided navigation MIS percutaneous screw fixation is a safe, effective and feasible treatment approach for displaced yet reducible pelvi-acetabular fractures. It complements ORIF in achieving a unified operative goal. The heterogeneous nature of patients’ medical history and individual fracture characteristics requires patient-individualized treatment and a multi-disciplinary approach towards patients’ recovery.
Footnotes
Ethical approval
All authors agree that this research presents an accurate account of the work performed and all data presented is accurate and methodologies detailed enough to permit others to replicate the work. This manuscript represents entirely original work and if work and/or words of others have been used, that this has been appropriately cited or quoted and permission has been obtained where necessary. This manuscript has not been published in whole or in part elsewhere. This manuscript is not currently being considered for publication in another journal. All authors have been personally and actively involved in substantive work leading to the manuscript and will hold themselves jointly and individually responsible for its content.
All work was conducted in accordance with the Declaration of Helsinki and local statutory requirements and was approved by the Central Institutional Review Board of the Hospital Authority, Hong Kong (IRB-2025-307).
Informed consent
This study was a retrospective study. No human subjects were directly involved and there was no implication on future management. Data collection complies with existing policies regarding patient privacy. Informed consent was not required as per Central Institutional Review Board guidance.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.