
Abstract
Background
Hallux valgus (HV) remains a common forefoot deformity with a global prevalence of 19%. It is largely agreed that surgical correction of HV with minimally invasive techniques have good outcomes. Options include the percutaneous minimally invasive screw fixation (SF) and the intramedullary plate fixation (IPF) technique, with both employing different fixation techniques and hence stability of fixation. In this article, we aim to compare these 2 minimally invasive correction techniques and analyze the radiologic and clinical outcomes, including their time to consolidation.
Methods:
A retrospective study was conducted using data from a single tertiary hospital involving 89 feet who underwent SF (n = 42) and IPF (n = 47) procedures. Radiologic grading of callus formation was determined based on 2 components, the visualization of callus formation and the obliteration of the fracture line. Sequential radiographs were evaluated postoperatively across a 6-month period looking for callus formation.
Results:
A Fisher exact test was performed to examine the relation between both surgical procedures and the grade of callus formation. At 6 months, full callus formation was seen in both methods. However, at 3 months, there was a statistically significant difference between the 2 methods (P ≤ .05). IPF showed higher grades of callus formation than those in the SF group. In comparing the 2 groups, IPF also showed higher rates of full callus formation than those of the SF group (P ≤ .05).
Conclusion:
IPF of HV appears to be associated with faster callus formation at 3 months postoperatively than SF, with a greater proportion showing full callus formation.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
Hallux valgus (HV) remains a common forefoot deformity with a global prevalence of 19%. 1 In the case of athletes, the prevalence can be as high as 54.9%. 2 Management options are multitudinous but studies largely agree that surgical correction of HV with minimally invasive techniques have shown good outcomes. 3 Commonly employed options include the minimally invasive screw fixation techniques (SF) and the intramedullary plate fixation (IPF) technique, with both using different fixation techniques and hence stability of fixation. Interval healing of the first metatarsal osteotomy and callus formation at the osteotomy site can assist surgeons in deciding on when their patients may return to higher impact activities.
In the current literature, most studies have investigated the recovery and return to sports of patients post scarf or Lapidus surgery, with few to none looking into minimally invasive surgical procedures. 4 Although there are several studies that describe the progression of callus formation as by Blitz et al 5 and more recently by Lewis et al 6 in SF techniques, there are currently no methods to compare between various minimally invasive techniques.
In our knowledge, this is the first study that compares these 2 techniques of minimally invasive correction bunion correction, and we aim to analyze their radiologic and clinical outcomes.
Methods and Materials
Institutional review board approval was obtained prior to the start of the study. A retrospective study of prospectively collected data was conducted in a single tertiary hospital using retrospective data that was collected and analyzed from the medical records of 74 patients (total 89 feet) between the years of 2022-2024. Patients that were selected for the study were determined based on several inclusion and exclusion criteria:
Inclusion criterion:
Patients who had undergone either SF or IPF.
Exclusion criteria:
Presence of other mid or hindfoot deformities.
Patients who had defaulted follow-ups.
Data Collection and Definitions
For qualifying cases, perioperative data were collected, including demographic data, clinical scores (visual analog scale [VAS]), and post-operative radiographs. Bone mineral density is not routinely measured in our department for cases of HV.
Minimally Invasive Screw Fixation Technique
Minimally invasive bunion surgery (MIBS) with screw fixation technique is similar to recently described surgical technique by Lewis et al. 7 The patients in our study underwent the fourth-generation MIBS with the use of a 2 × 20-mm burr to create a transverse distal osteotomy in the first metatarsal head, followed by a shift of the head laterally to achieve correction of the bunion. Two parallel guidewires were inserted followed by 2 cannulated beveled screws using the “in-out-in” technique to secure the new positioning of the head. An Akin osteotomy procedure was then performed in the proximal phalanx of the first ray and secured with a cannulated screw. The authors did not use a jig for the procedure, and all guidewire and screw placements were done freehand. The wounds were closed and bulky dressings applied.
IPF Technique
The IPF technique was performed with the Spear Plate system (Aplus Biotechnology). This is a curved plate with different offset options depending on the amount shift of the first metatarsal head required for bunion correction (Figure 1). A 2-cm longitudinal skin incision was made medially just proximal to the level of the first metatarsophalangeal joint (Figure 2). This is a mini-open technique with the medial capsule incised and medial prominence excised. Subsequently, the same Bosch transverse distal osteotomy was performed with a microsagittal saw. The first metatarsal head was translated laterally with correction of the axial plane pronation of the head. The depth of the proximal metatarsal was measured, and the corresponding plate length was chosen. The intramedullary Spear Plate was inserted into the medullary canal while maintaining the lateral shift of the first metatarsal head (Figure 3). Two locking screws were inserted to maintain stability of the correction. A medial plication could be performed before closure of the skin incision. Additional first ray osteotomies such as the Akin osteotomy were also performed if required.

Side profile of Spear Plate implant showing 3 different offset options.

A 2-cm medial incision.

Spear Plate inserted into the medullary canal with lateral translation of the first metatarsal distal fragment.
Pre-operative protocol
Patients in our foot and ankle surgery clinic with symptomatic and radiographic hallux valgus were offered and counseled for surgery. An open discussion with the patient with regard to both fixation techniques with emphasis on the wounds and types of implants used with each technique was done, allowing the patient to decide on their preferred surgical method.
Post-operative protocols
The post-operative protocols for both groups of patients were largely similar. Immediate post-operative weightbearing was allowed for all patients from post-operative day 1 in a stiff-soled shoe. The patients in both groups start range of motion exercises of the hallux after 1 week and progressed to normal shoe wear after 4 weeks. The patients were followed post-operatively at 2 weeks, 1 month, 3 months, and 6 months, with sequential radiographs taken and VAS scored at each visit. Once full callus formation (CF) and osteotomy site bone healing was seen in the radiographs during the period of follow-up, the patients were allowed to return to impact sports.
Grading of CF
Weightbearing radiographs were taken at each visit, and the radiologic images were assessed and graded by 2 independent assessors. The radiographs are evaluated according to 2 components: the visualization of CF and the obliteration of the fracture line (OFL). Grade 1 is defined as no visualization of CF and fracture line present; grade 2 is defined as visualization of bony CF and fracture line still present; and grade 3 is defined as complete obliteration of the fracture line with full remodeling of bony callus seen (Figure 4). Inter-observer reliability for callus grading was assessed by the 2 independent assessors in a masked pair fashion using Cohen kappa coefficient and demonstrated excellent agreement (κ = 0.95).

Novel grading of callus formation.
Statistical Analysis
The data were analyzed using SPSS V.25.0 (IBM Corp) and Stata 17.0 (StataCorp). Shapiro-Wilk tests for normality were conducted for continuous outcome data, and either parametric, for normally distributed data, or nonparametric tests, for non-normally distributed data, were used. For dichotomous or ordinal outcome data, nonparametric tests were used. Statistical testing was completed using comparisons based on Mann-Whitney U tests as well as mean ranks for ordinal data, Fisher exact test for categorical data, and Student t test for continuous variables. Ordered logit regression was performed to evaluate the relationship between the SF and IPF groups and eventual callus grading at 3 months. Statistical significance was set at P <.05, and unless otherwise stated, descriptive statistics are percentages, means, and SDs.
Results
Demographic
A total of 89 feet were included in the study. Mean age of patients in the SF group was 50.7 ± 14.0 years and 48.9 ± 15.2 years in the IPF group. Pre-operative demographics and hallux valgus deformity were equal. See Table 1 for detailed patient demographics and baseline characteristics.
Demographics of the Included Patients.
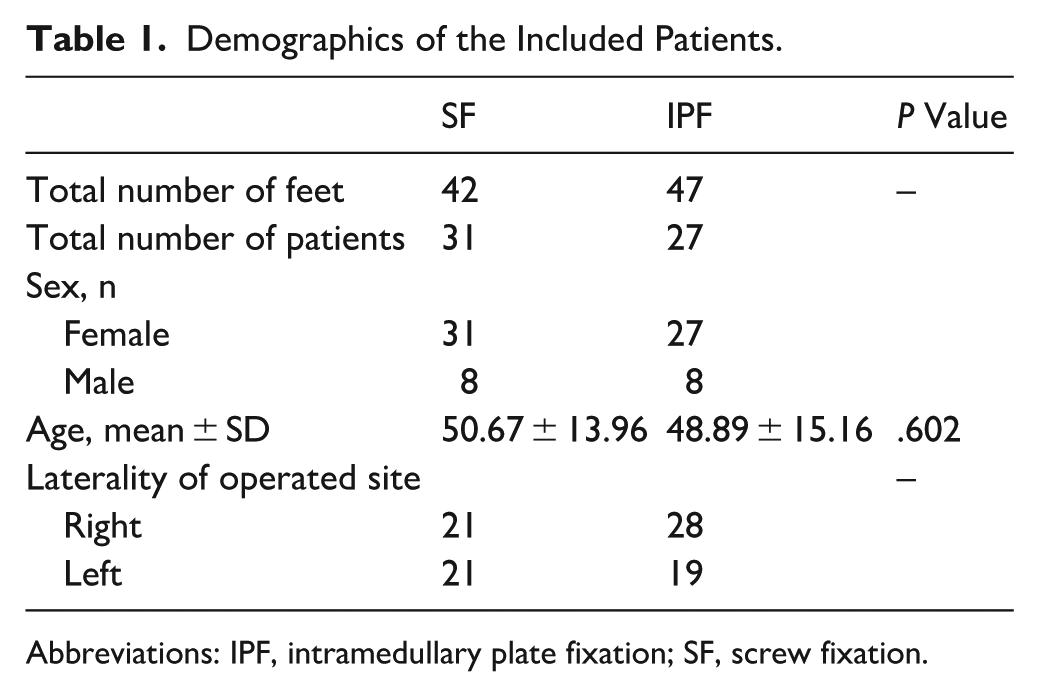
Abbreviations: IPF, intramedullary plate fixation; SF, screw fixation.
Callus Formation in IPF vs SF
Callus formation was one of the primary outcome measures of this study, and at 3 months, 15 (32%) in the IPF group and 3 (7%) in the SF group were noted to have a fully formed or grade 3 callus at the osteotomy sites. This difference in groups was noted to be statistically significant (P = .004, see Table 2). Grade 2 calluses were noted in 23 patients (49%) in the IPF group and 29 patients (69%) in the SF group, and grade 1 calluses were noted in 9 patients (19%) in the IPF group and 10 patients (24%) in the SF group. The difference in grade 2 calluses between groups was statistically significant (P = .044); however, the difference in grade 1 calluses between groups failed to reach statistical significance (P = .390). Mean ranks were used to determine an average ranking of callus gradings in each group at 3 months. Mean rank of callus grades in the IPF group was 49.87, compared with 39.55 in the SF group, and this difference was statistically significant (P = .033, see Table 3).
Number of Patients With Full Callus Formation at 3 Months in Our Study Cohort.

Abbreviations: IPF, intramedullary plate fixation; SF, screw fixation.
Boldface indicates statistical significance (P < .05).
Grading of Callus Formation of SF and IPF.

Abbreviations: IPF, intramedullary plate fixation; SF, screw fixation.
Boldface indicates statistical significance (P < .05).
Ordered logit regression of callus grade against the type of fixation technique (SF vs IPF) displayed that patients in the SF group had a 40% lower likelihood of having a higher callus grade seen on radiographs at 3 months compared with those in the IPF group (OR = 0.40, CI 0.17-0.93, P = .03).
VAS Outcome Scores
Average VAS scores were 0.93 ± 1.00 (0-3) in the SF group and 1.02 ± 0.90 (0-3) in the IPF group, and this difference was not statistically significant (P = .647, see Table 4).
VAS Scores at 3 Months Postoperatively.

Abbreviations: IPF, intramedullary plate fixation; SF, screw fixation; VAS, visual analog scale.
Discussion
This retrospective study reveals that there is more high-grade callus formation seen in IPF than in SF at 3 months, suggesting that IPF has faster callus formation than SF techniques.
To our knowledge, this is the first study that compares the rate of callus formation of SF and IPF. The outcome of this study provides data on radiologic healing timelines between techniques, which may assist surgeons in deciding the weightbearing progression for the patient. In general, most surgeons allow immediate weightbearing after minimally invasive bunion surgery in a protective shoe. 8 In contrast to normal walking where the force on the first metatarsophalangeal joint is around 80% of the body weight, activities such as running and jumping that a sport involves leads to 400% body weight of force on the first metatarsophalangeal joint. 9 Adhering to the principles of fracture healing, as the presence of callus formation at the osteotomy confers stability, the authors suggest a possible correlation to this finding would be the possibility of allowing patients to return to impact sports earlier.
Our study aims to investigate and compare the rates of callus formation in these 2 groups of minimally invasive techniques for bunion correction at an earlier stage of recovery at 3 months. We postulate that the earlier callus formation in the IPF group may mean a possible allowance for earlier return to sports however this observation is not validated and it is at the discretion of the readers to interpret the study’s findings.
Potential Reason for quicker callus formation in IPF
Although both surgical methods can achieve adequate deformity correction and adequate callus formation with secondary bone healing, we hypothesize that the difference in rates of callus formation may be due to the difference in stability between the constructs used. In IPF, a plate-and-screw construct are used to achieve excellent stability in the coronal, sagittal, and rotational axes. Although, being a plate, it is inserted in an intramedullary manner and stability is achieved with the flared body of the plate engaging in diaphyseal bone with interference fit along with the spear tip engaging in metaphyseal bone proximally. Rotational stability, medial lateral and dorsal plantar stability of the metatarsal head is provided by the 2 distal screw fixations. In comparison, the stability achieved by the screw fixation technique is dependent on the quality of bone, position of the proximal screw, and purchase of the screw distally in the metatarsal head. The stability of the construct is reliant on a 3-point “in-out-in” position of the proximal screw starting at the medial cortex of the first metatarsal, exiting at the lateral cortex and entering the first metatarsal head. 10 Further stability is provided by the second distal screw, which also acts to control rotation. Blitz et al 11 have also further described a “cortical purchase zone,” which is defined as a region in the lateral first metatarsal cortex proximal to the osteotomy for the proximal screw to exit for maximum stability. Any failure to achieve the ideal screw positions will likely compromise the stability of the construct. Further biomechanical studies may be considered to see if less strain is achieved in the construct used in IPF compared with SF, resulting in faster secondary bone healing and hence callus formation.
Our study shows that using IPF results in earlier callus formation than SF. A systemic review by Zaveri et al 12 showed use of IPF resulted in improvements in hallux valgus angle, intermetatarsal angle, and clinical outcome scores that were comparable to other techniques for HV correction. This finding is seen in our study, where both methods show comparable post-operative radiologic correction and VAS at 3 months post-operatively. There have also been no reported rates of non-union using IPF. A study by Karaduman et al 13 also showed superior results in using IPF methods with increased stability of the HV correction and fixation, increased function, and better radiologic outcomes as compared to correction with screws. Other studies have also shown superior results using IPF methods with good correction of the hallux valgus angle and intermetatarsal angle, with quicker return to function.14,15 The allowance of immediate weight-bearing post-operatively is also shown to help with reducing pain and quicker return to function. 16 Giotis et al 17 studied a group of athletes who underwent hallux valgus surgery corrected with the chevron osteotomy and found that all athletes returned to sport at around the 3-month post-operative period. Ciechanowicz et al 18 analyzed a group of patients who underwent scarf osteotomy correction and found that the mean return to sports was 15 weeks post-surgery. Clinically, a large majority of surgeons would allow their patients back to full work and activity beyond that period, especially from 6 months thereafter. Our study analyzed the rate of healing in both the SF and IPF methods of minimally invasive bunion correction specifically at the 3-month post-operative period with an aim to find out which method results in earlier callus formation to guide earlier progression of weight-bearing and activity. Our study showed that at 3 months post-operatively, the probability of both groups attaining grade 2 callus formation is similar. However, the IPF group had a 40% higher probability of obtaining grade 3 callus formation or complete osteotomy site healing.
Limitations
This study is limited by the smaller sample size of patients, shorter follow-up times, as well as non-standardized radiography settings. Ideally, a larger number of patients should be recruited and followed for a longer duration to assess the long-term benefits of using IPF over SF in function, pain, and radiologic outcomes. Power analysis was not performed for this study because of its retrospective nature, and furthermore, the retrospective nature of the study limits the ability to infer causality between fixation method and healing rates. We do acknowledge the lack of a power analysis to be a limitation in the design; however, because of the novelty of our comparison of the outcome measured (callous formation grading), there is no good way to estimate the expected incidence required for power analysis. Our study mainly focuses on the 3-month mark to determine if there was a significant difference in callus formation between the 2 groups. Although our method of grading for callus formation has not been validated, its ease of use and universal application may be considered in further comparison and evaluation of a variety of new techniques in MIBS. In view of these limitations, we advise readers to interpret the findings of our study with caution.
Conclusion
IPF is a promising method for HV correction. Our study suggests that IPF allows for faster callus formation and radiologic consolidation than SF techniques. The authors postulate that the clinical relevance of this finding may be earlier confidence in weight-bearing progression, although further prospective, controlled studies would be needed to correlate these radiologic findings with functional recovery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261427472 – Supplemental material for Time to Callus Formation With Minimally Invasive Bunion Surgery: Association of Intramedullary Plate Fixation With Earlier Consolidation Compared to Screw Fixation Techniques
Supplemental material, sj-pdf-1-fao-10.1177_24730114261427472 for Time to Callus Formation With Minimally Invasive Bunion Surgery: Association of Intramedullary Plate Fixation With Earlier Consolidation Compared to Screw Fixation Techniques by Hon Keng Pui Bryan, Fong Jiawen, Colin Wang Tzong-Yee, Zachariah Gene Wing Ow, Eric Cher Wei Liang, Chong Keen Wai and Png Wenxian in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
This is a retrospective study with de-identified patient data (reference number for the ethical approval: CIRB 2020/2381).
Consent for Publication
Not applicable
Author Contributions
All authors contributed equally to the process of conceptualization, data processing, and manuscript writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available because of personal data protection laws.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.