
Abstract
Objective
This study aims to evaluate the efficacy and safety of an accelerated rehabilitation protocol for reverse shoulder arthroplasty (RSA).
Method
A retrospective analysis was conducted on 12 patients who underwent RSA between 2021 and 2022 at the Department of Orthopaedics and Traumatology, North District Hospital. All patients received rehabilitation under a newly developed accelerated rehabilitation protocol. The protocol was divided into three phases: immediate active mobilization (weeks 1 to 6), passive mobilization and early strengthening (weeks 7 to 12), and strengthening (week 13 onwards to 26 weeks and beyond). Motions such as combined axial loading, adduction, external rotation, and extension were avoided in all phases to avoid causing anterior dislocation. Primary outcomes included the range of motion (ROM) at 1, 6, and 12 months post-operatively, and the functional and pain scores at 12 months. Secondary outcomes included complications such as fracture, dislocation, and infection. Data were collected from clinical notes, allied health documentation, and telephone interviews with patients.
Results
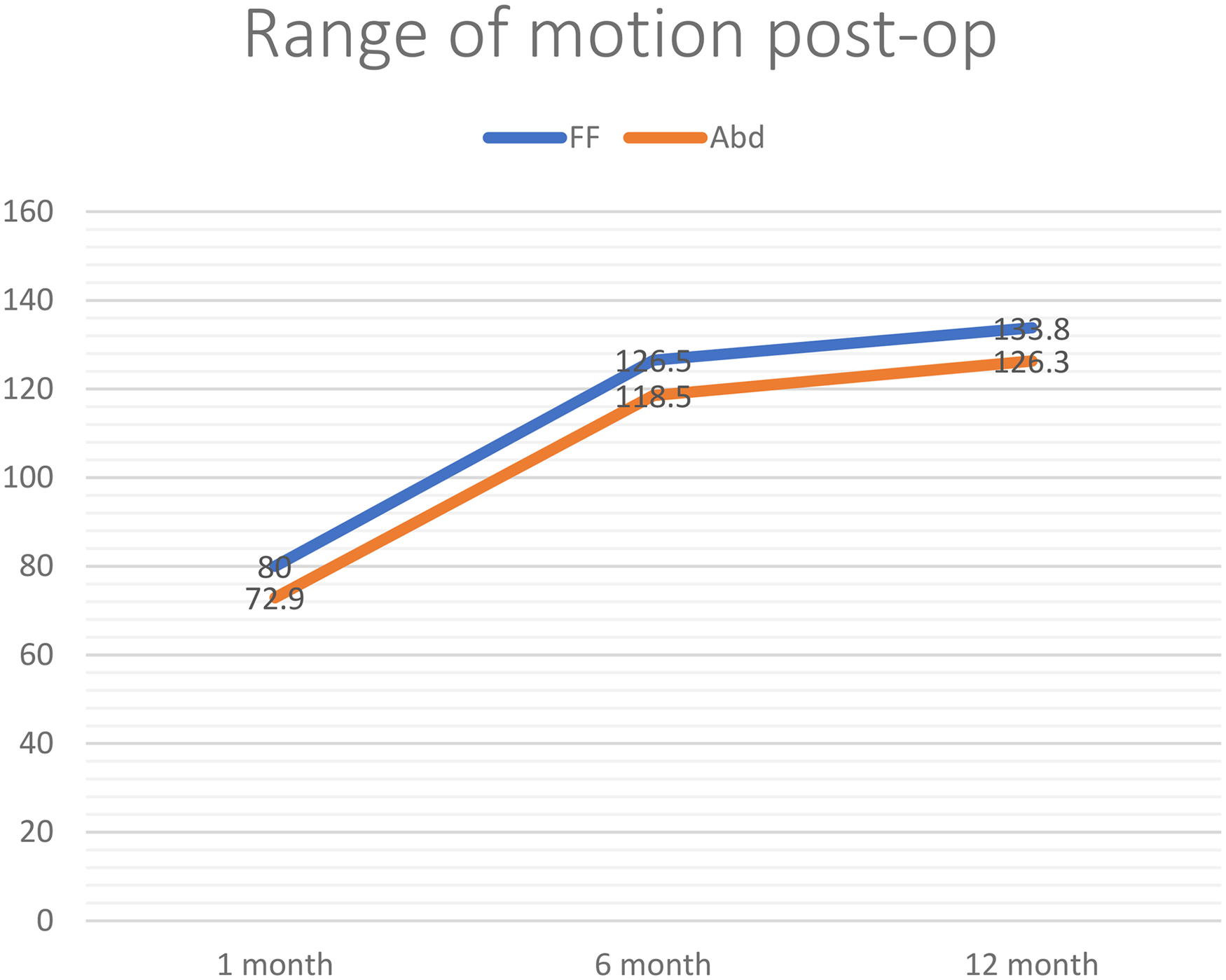
At 1 month post-operatively, the average ROM was 80° in forward flexion and 73° in abduction. At 6 months, the average ROM increased to 126° and 119°, respectively. At 12 months, the average ROM was 134° for forward flexion and 126° for abduction. The average pain score by numeric rating scale was 1.9 at 12 months. The mean Oxford shoulder score was 42.4 out of 48. No cases of dislocation, fracture, wound complication, or infection were observed.
Conclusion
This case series demonstrates that the accelerated rehabilitation protocol for RSA is safe and effective, with no observed complications. Future studies may focus on identifying poor prognostic factors that would predict an inferior outcome. Studies with larger sample sizes and comparative designs are needed to confirm these findings and optimize rehabilitation strategies.
Introduction
Reverse shoulder arthroplasty (RSA) has become increasingly popular in managing proximal humeral fractures, rotator cuff pathologies, degenerative shoulder conditions, and selected tumors. 1
However, no consensus exists regarding the optimal rehabilitation protocol. A systematic review found inconsistent rehabilitation protocols across different centers. 2
Conventional practice often involves shoulder immobilization for 2 to 6 weeks to protect soft tissues and allow healing. While sling use can aid recovery, prolonged immobilization may increase the risk of joint stiffness and functional impairment. 3
The deltopectoral approach, commonly used in RSA, often involves partial or complete subscapularis detachment. Friedman et al. 4 compared cohorts in RSA with subscapularis repaired or non-repaired, showing no difference in clinical outcomes. de Boer et al. 5 also suggested that there were no significant differences in range of motion (ROM), functional outcome scores, or strength between the two groups.
A meta-analysis also found no advantage in repairing the subscapularis in terms of reduction of complication rates, instability with lateralized implants, or improvement in functional outcomes. 6
The accelerated rehabilitation protocol was thus proposed, aiming to start early mobilization for patients undergoing RSA without the need for immobilization for soft tissue healing. Lee et al. 7 studied 320 patients undergoing primary RSA, dividing patients into three groups based on immobilization duration (0, 3, or 6 weeks). The early mobilization group showed non-inferior outcomes. 7 Patients were able to return to normal function earlier and regain independence.
Sabesan et al. 8 similarly demonstrated that early mobilization leads to better function and ROM without added complications.
Despite international data, no local experience with such a protocol had been reported. This study aims to evaluate the efficacy and safety of a standardized three-phase accelerated rehabilitation protocol at our institution.
Methods
This retrospective cohort study was conducted at the Department of Orthopaedics and Traumatology, North District Hospital. Twelve patients who underwent primary RSA between 2021 and 2022 were included. All procedures were performed by the same surgical team using the standard deltopectoral approach with the patient in a beach-chair position under general anaesthesia. Implants used included the Delta Xtend (10 patients) and the Zimmer Comprehensive system (two patients), with cemented humeral stems in all cases. A surgical drain was inserted postoperatively in every patient. All of them received the new accelerated rehabilitation protocol.
Indications for RSA included complex proximal humeral fractures, rotator cuff arthropathy, osteoarthritis, avascular necrosis, and metastatic lesions to the proximal humerus. Revision RSA cases were excluded from the study.
All patients followed a three-phase accelerated rehabilitation protocol. Precautions were made to avoid the combined motion of axial loading, adduction, external rotation, and extension in all phases to prevent dislocation. Phase one, covering weeks 1 to 6 postoperatively, focused on immediate active mobilization, aiming to optimize pain control, improve soft tissue swelling, and avoid stiffness. Patients were encouraged to begin mobilization on the first day after surgery. Pain control measures included ice therapy and standardized pharmacological analgesia. Physiotherapists assisted and supervised in active assisted exercise and ROM exercise with progression from lying to sitting, standing, scapular plane elevation, and external rotation.
Phase two, from weeks 7 to 12, emphasized passive mobilization and early strengthening, aiming to optimize pain-free ROM, increase shoulder strength, and normalize the kinematic pattern of the shoulder complex. Active and passive movements were continued within the limits of pain tolerance. Deltoid rehabilitation regimen was also commenced at this phase while continuing active scapular mobilization exercise.
Phase three, the final phase, beginning at week 13 to 6 months onwards, aims to improve the strength of the shoulder musculature, improve arm strength, and improve functional activities of the shoulder. All previous mobilization and strengthening exercises were continued during this phase, while rotator cuff and deltoid strengthening exercises with a thread band or light weights and progressive functional training were commenced.
Patients’ demographics and perioperative parameters were reviewed. Perioperative data were collected, including choice of implant, operative time, intraoperative blood loss, and length of stay after operation. Patients’ medical records and radiographs were reviewed to investigate for any complications, including but not limited to fractures, dislocations, wound complications, and infection related to the surgery and rehabilitation protocol.
The post-operative rehabilitation documentations by both surgeons and allied health colleagues, including physiotherapists and occupational therapists, were reviewed as objective measurements of ROM after operation at 1-month, 6-month, and 12-month intervals.
The average pain scores were measured with a numeric rating scale (NRS) at 1-month, 6-month, and 12-month intervals. The average functional scores by Oxford shoulder score (OSS) were measured over phone interviews at a 1-year interval after the operation.
Results
Twelve patients were included in the study, with a mean age of 74.3 years at the time of surgery. There were seven females and five males. The surgical indications were proximal humeral fractures in six patients, rotator cuff arthropathy in four patients, osteoarthritis of the shoulder in one patient, and proximal humeral metastasis in one patient. All patients received cemented humeral stems, with the Delta Xtend implant used in 10 cases and the Zimmer Comprehensive in two cases.
The average operative time was 163.4 min, with a mean intraoperative blood loss of 437.5 mL. The average post-operative hospital stay was 8.25 days.
One patient developed transient axillary nerve palsy. The condition resolved spontaneously without surgical intervention. No cases of wound infection, dislocation, or fracture were observed, and no immediate complications were directly attributable to the accelerated rehabilitation protocol.
At 1 month post-operatively, the average ROM was 80° for forward flexion and 73° for abduction. By 6 months, the average ROM for forward flexion and abduction increased to 126° and 119°, respectively. At 12 months, average ROM reached 134° in forward flexion and 126° in abduction.
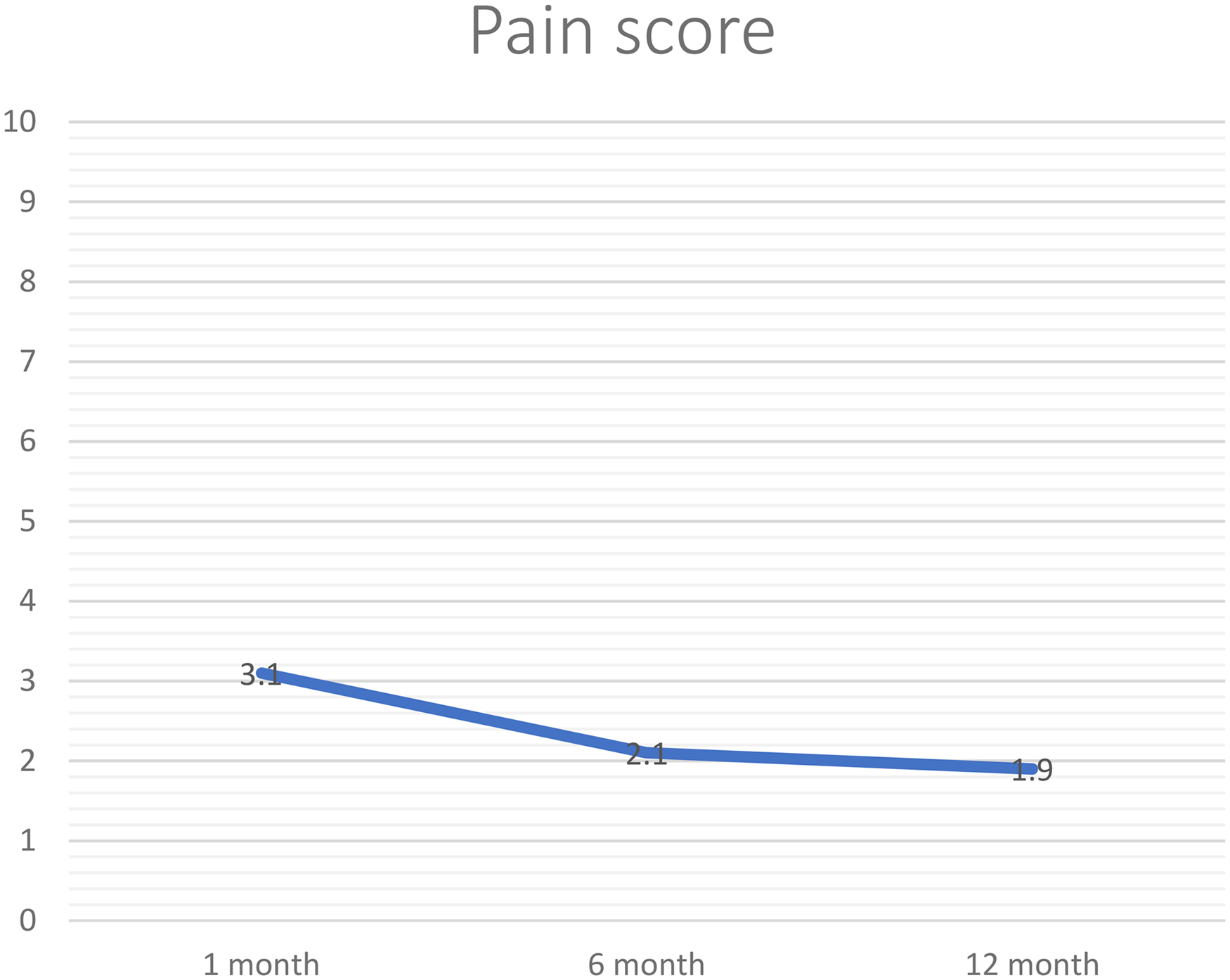
The postoperative pain control was measured with a numerical rating scale (NRS), with 0 representing no pain at all, and 10 representing the worst pain ever. Pain scores on the NRS improved over time, with averages of 3.1 at 1 month, 2.1 at 6 months, and 1.9 at 12 months.
OSS 9 was used as an objective measurement of functional outcome for patients undergoing RSA. OSS is a 12-item questionnaire for patients developed to evaluate the outcomes of shoulder surgery, including assessment of pain and activities of daily living. A higher score represents a superior outcome, with the highest being 48. The mean OSS at 12 months was 42.5 out of 48, indicating a high level of patient-reported shoulder function.
Discussion
This study demonstrates that an accelerated rehabilitation protocol for RSA, involving early active mobilization without post-operative immobilization, is both safe and effective.
Traditionally, rehabilitation often involves immobilization during the first few weeks after RSA. Some international studies proposed that accelerated rehabilitation and immediate mobilization after RSA are safe and effective.7,10,11
Therefore, in this study, we would like to investigate whether an accelerated rehabilitation protocol can be applied to our locality.
The observed complication rate of 8.3% was lower than the generally reported rates of 15% to 24% for RSA. Importantly, there were no cases of instability, dislocation, or fracture attributable to early mobilization. The single neurological complication – transient axillary nerve palsy – resolved without intervention and did not affect the patient's functional outcome. The patient was able to achieve a forward flexion of 140° and abduction of 130° at 12 months, suggesting that early mobilization did not compromise recovery.
The reported rate of complications with RSA was approximately 15% to 24%.
The most quoted complications include peri-prosthetic infection, dislocation, peri-prosthetic fracture, neurological injury, scapular notching, acromion or scapular spine fracture, and loosening of the prosthesis. 12
The complication rate was 8.3% (1 out of 12) in our study. We had one case of axillary nerve palsy after the operation, presented with numbness over the deltoid skin patch. The motor function of the patient was preserved with a good functional outcome. The patient was able to achieve an early good ROM with forward flexion of 140° and abduction of 130°.
There were no reported complications potentially related to the rehabilitation protocol, including fracture, instability, including subluxation or dislocation.
Early mobilization without using a shoulder immobilizer might potentially improve the upper limb function in the early post-operative period. We observed that patients were able to perform simple tasks with the operated upper limb.
Studies had suggested that sling immobilization might result in gait impairment, increased risk of falls, and delayed functional return.13,14
Early mobilization might therefore potentially aid in the early return of function of the operated upper limb and reduce associated carer stress.
Some international studies had already shown that early mobilization can achieve a better ROM and functional outcome when compared with delayed rehabilitation (DR). 15
We compared our clinical outcome in terms of pain and ROM with the early mobilization group in these studies. We were able to achieve similar results in terms of pain control and ROM.
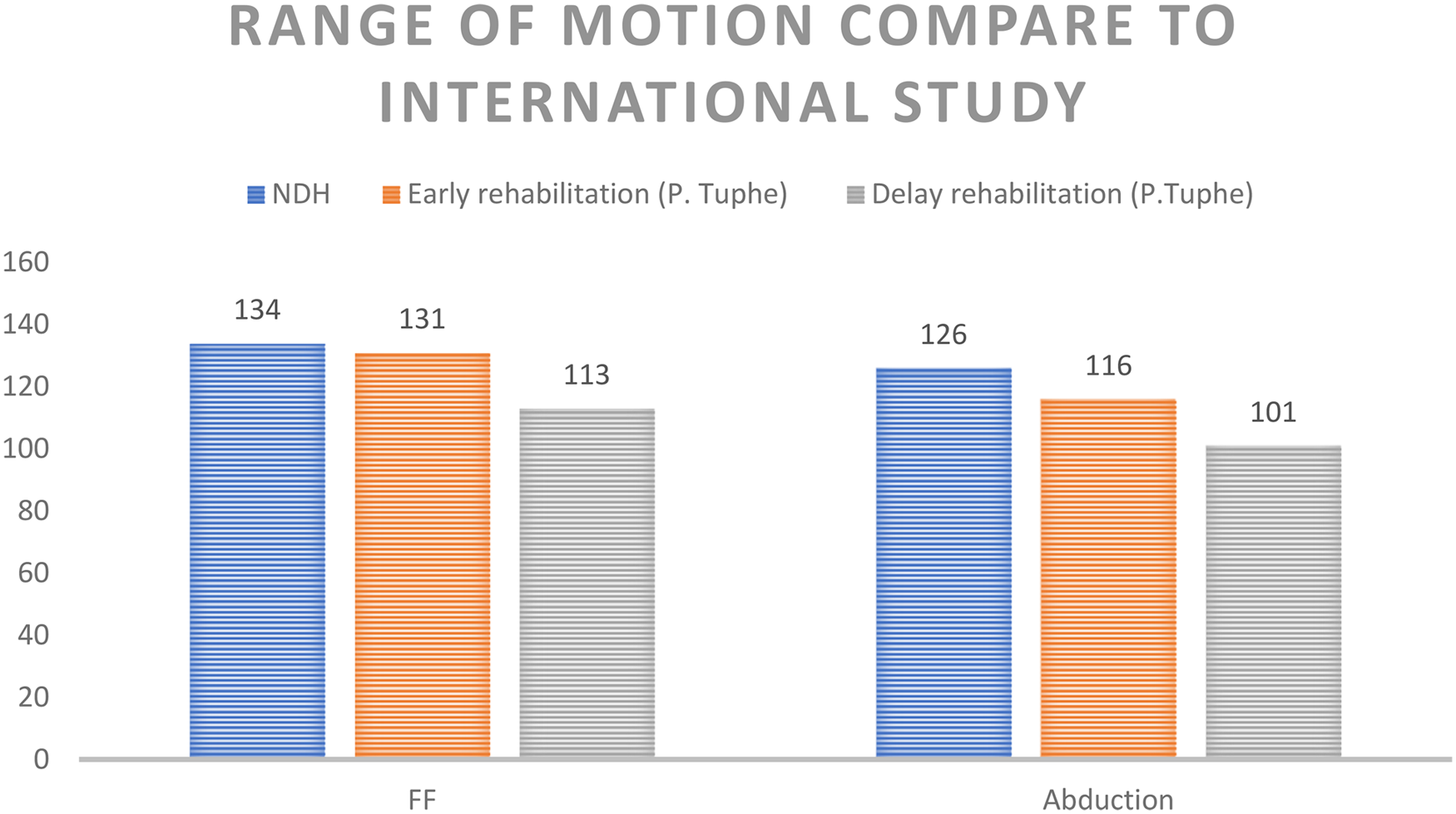
Tuphe et al. 15 included 94 patients who underwent RSA. Patients were stratified into early rehabilitation (ER) group (n = 45), that is, mobilizing since post-operative day 1, and DR group (n = 49), that is, mobilizing since post-operative day 30. 15
The ER group had shown significant improvement of ROM in forward flexion (131° in the ER group and 113° in the DR group) and abduction (116° in the ER group and 101° in the DR group).
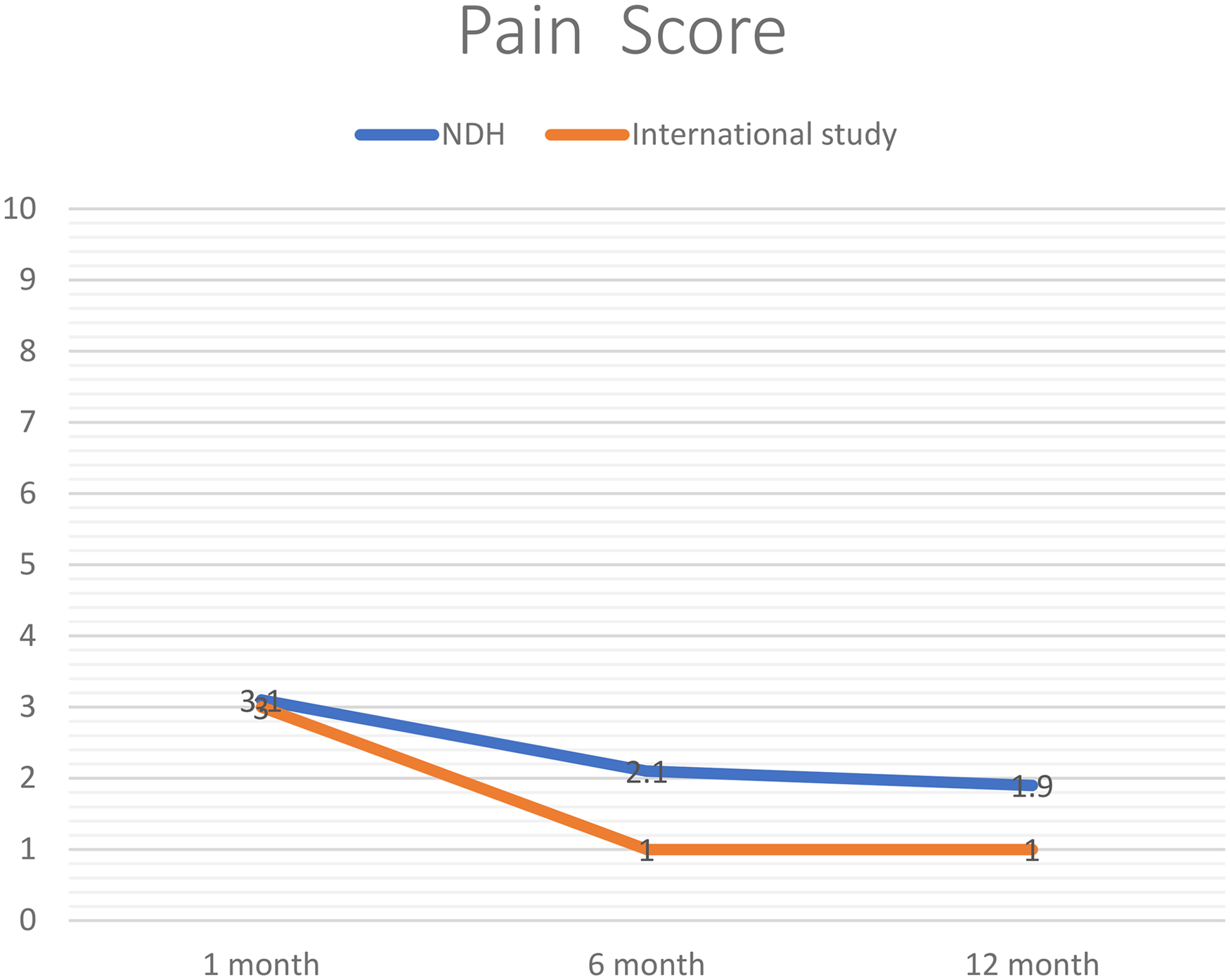
The average pain scores were 3.1, 2.1, and 1.9, at 1-, 6-, and 12-month post-operatively.
We were able to achieve comparable results with an international multi-centre single-arm study, 10 where the reported pain scores were 3, 1, and 1 at 1-, 6-, and 12-month post-operatively.
OSS 9 is used to objectively measure patients’ post-operative functional outcomes, which include pain score and activities of daily living. A higher score suggests a better functional outcome.
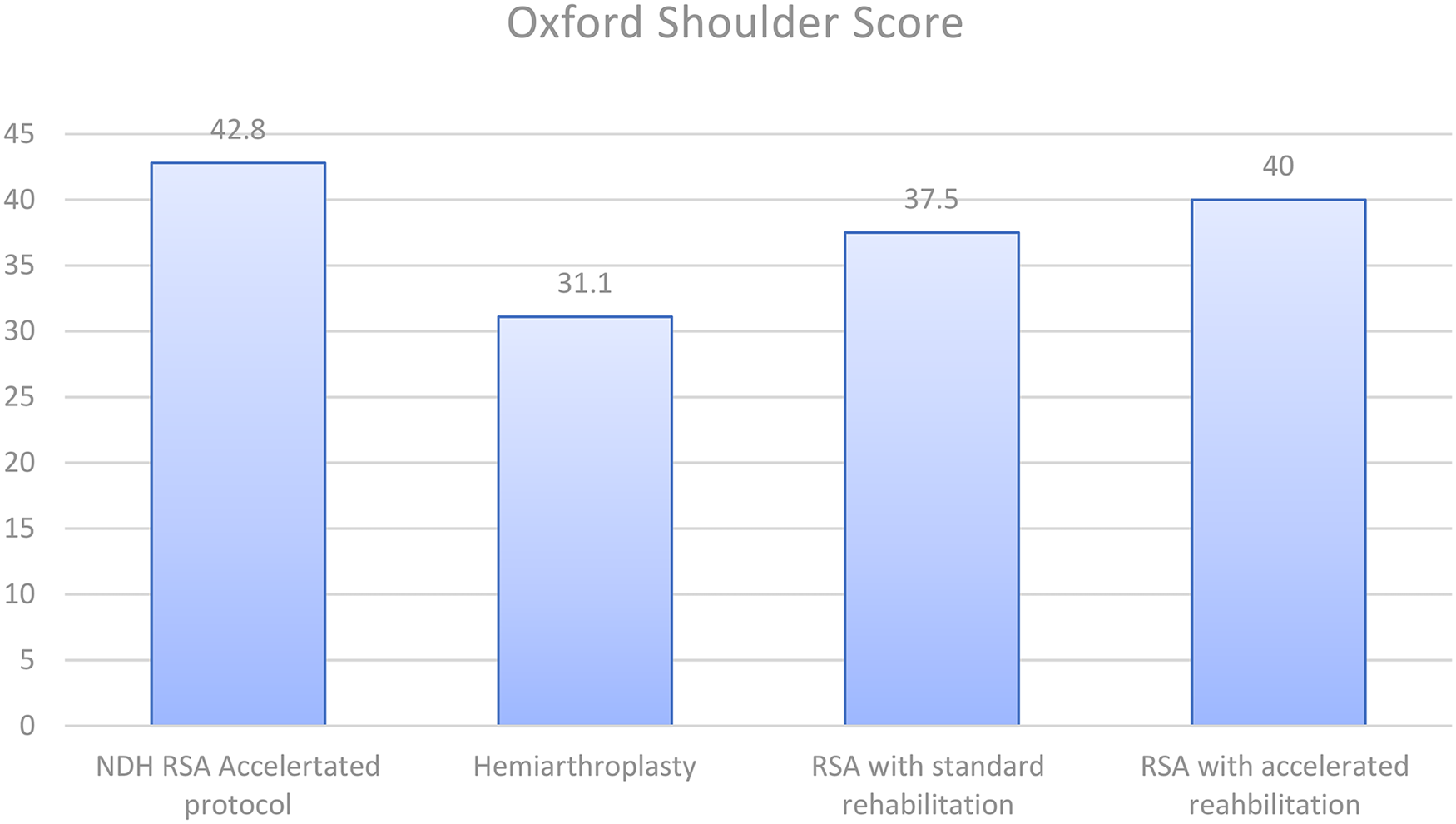
The reported average OSS in our study was 42.8 out of 48. Literature review 16 suggested OSS for hemiarthroplasty was 31.1 out of 48 and 37.5 out of 48 for RSA with standard initial immobilization rehabilitation, respectively.
Our functional outcome was therefore comparable with the literature in the early mobilization group (40 out of 48). We were able to achieve a good functional outcome comparable with international studies10 on accelerated rehabilitation after RSA.
There were a few biomechanical designs that provided RSA with the intrinsic stability. 17 This includes medialized joint centre of rotation with increased lever arm of deltoid, deltoid fibre retention by fistulisation of humerus, reduction of shear forces by placement of joint centre of rotation at the glenoid bone implant interface, and semi-constrained implant.
By literature review, 18 instability was found to be associated with scapular notching and too medial glenoid implants.
In our experience, in addition to the above intrinsic implant design, the intra-operative stability testing was equally important to ensure the shoulder joint was in a stable range to allow early mobilization. Whenever there are any features of instability, for example, opening up of joint space or scapular notching, we suggest further adjustment of the implant and insert to achieve adequate tension and a stable range.
Limitation
This study is limited by its retrospective design and small sample size. The absence of a control group receiving standard rehabilitation makes it difficult to draw definitive conclusions about the relative efficacy of the accelerated protocol. Therefore, we have compared results with the literature regarding the efficacy of the accelerated rehabilitation protocol. Future research should include larger cohorts and randomized controlled trials to further validate these findings.
Conclusion
Our experience suggests that an accelerated rehabilitation protocol involving early active mobilization after RSA is both safe and effective. Patients demonstrated satisfactory pain control, good ROM, and satisfactory functional outcomes without increased complications. Potential benefits, including early regain of upper limb functions and faster recovery, might be achieved. Further studies are needed to observe the long-term results.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.