
Abstract
Background/Purpose
Enhanced recovery after surgery (ERAS) for total knee replacement (TKR) is a multi-modal and multi-disciplinary approach designed to enhance patient outcomes. ERAS was first introduced in 1997 and further refined with published guidelines for TKR in 2020. Our institute has been adopting ERAS for TKR since 2017. This study aimed to outline our local ERAS protocol for TKR and assess its outcomes in terms of length of stay (LOS).
Methods
A retrospective cohort study was carried out comparing total knee arthroplasty patients treated by ERAS (2021–2023) with conventional cohort (2013–2016). Data from pre-operative, immediate after TKR, and 3 months post-TKR were collected through clinical and medical records through hospital electronic record system.
Results
A total of 1283 patients who underwent TKR (708 patients in ERAS group and 575 in conventional group) were recruited. Both median pre-operative (0.00 vs 1.00 day; P < 0.001) and total LOS (6.00 vs 8.00 days; P < 0.001) were significantly reduced in the ERAS group. Mean interval between hospital admission and surgery was significantly shorter in the ERAS group (0.01 months) compared to the conventional group (0.04 months) (P = 0.049). Notable higher proportion of conventional group underwent surgery without navigation was reported (13.0% vs 1.4%, P < 0.001). In terms of deep vein thrombosis (DVT) prophylaxis, Pradaxa was predominantly prescribed in the ERAS group (83.7%), while Clexane was more commonly used in the conventional group (56.9%). Regarding the type of anaesthesia, percentage of patients who received spinal anaesthesia was significantly higher in the ERAS group than the conventional group (87.3% vs 76.9%; P < 0.001). In a step-wise linear regression analysis, applying ERAS remained a statistically significant predictor for a reduced LOS (r2 = 0.064; coefficient (95% confidence interval) = −1.01 (−1.89, −0.13); P = 0.024) after controlling for surgical side, using navigation, DVT prophylaxis and anaesthesia.
Conclusions
After implementation of ERAS in patients after TKR, length of hospital stay was significantly decreased, with or without using navigation, the choice of DVT prophylaxis or choice of anaesthesia. Further investigations were warranted to implement a multi-centre large-scale long-term study to explore long-term outcomes and quality-of-life measures post-TKR.
Keywords
Introduction
Enhanced recovery after surgery (ERAS), also known as a fast-track programme, for total knee replacement (TKR) is a multi-modal and multi-disciplinary approach designed to enhance patient outcomes. The programme emphasizes pre-operative patient education, improves patient satisfaction and post-operative pain management, reduces post-operative complications, shortens length of stay (LOS), and promotes faster recovery. 1
ERAS was first introduced in colorectal surgery in 1997 by Professor Henrik Kehlet, aiming to expedite post-operative recovery. 2 ERAS was first refined in Denmark and in the United Kingdom to speed up post-operative recovery. 2 Since then, ERAS protocols have been adopted across various surgical specialties, including orthopaedics, demonstrating promising results in improving clinical outcomes and reducing hospital stays. 3 In the field of orthopaedic surgery, a few hospitals in the United Kingdom pioneered its use for joint replacements. 4 The ERAS Society has published guidelines to implement enhanced recovery protocols in lumbar spinal fusion, total hip replacement, and TKR surgeries. The ERAS Society's 2020 guidelines for total hip and knee replacements recommend pre-operative education, optimization, physiotherapy, local analgesia, tranexamic acid, multi-modal pain relief, anti-thrombotic prophylaxis, and early mobilization to improve outcomes and shorten hospital stays. 4
In the United States, clinical pathways for total joint replacement started in 2003, 5 with ERAS for TKR implemented in a county hospital by 2017. 6 Denmark introduced an ERAS protocol for TKR in 2008, 7 enhancing it by 2013. 8 The United Kingdom adopted ERAS for TKR in 2008, 9 supported by a national programme from 2009 to 2011.10,11 Finland and Sweden began ERAS for TKR in 2011 12 and 2012, 13 respectively, while Canada started in 2012. 14 In Oceania, New Zealand implemented ERAS for TKR in 2013, 1 followed by an Australian regional hospital in 2018. 15 In Asia, China began ERAS for selected TKR patients in 2014, 16 India in 2016, 17 and Singapore in 2020. 18
ERAS implementation in total joint replacement has reduced hospital stays, lowered complication rates, and boosted patient satisfaction in New Zealand. 1 Studies in Asia, including China 16 and Singapore, 19 confirm these benefits, showing shorter hospital stays and faster recovery after TKR, underscoring ERAS's potential to improve perioperative care and patient outcomes in the region.
A study at a local public hospital in Hong Kong, 20 compared TKR outcomes in elderly versus younger patients under fast-track protocols. The elderly had longer hospital stays and slower functional recovery, but fast-track care improved outcomes in both groups without increasing complications. Similarly, research from a private hospital 21 demonstrated that ERAS practices in total hip and knee arthroplasty reduced post-operative LOS, highlighting the protocol's efficacy across different hospital settings.
At our hospital, we began adapting ERAS protocols for selected patients in the Department of Orthopaedics and Traumatology in 2017 by incorporating measures such as pre-operative patient optimization, local infiltration analgesia, intra-articular tranexamic acid, multi-modal analgesia, anti-thrombotic prophylaxis, and so on. Following a thorough review of the protocol and clinical pathway, full implementation of ERAS for all TKR patients commenced in 2019 (Appendixes 1 to 3 in the Supplemental materials). In 2022, our hospital further advanced this initiative with the establishment of a total joint replacement centre, which aims to improve both the quality and quantity of care by reducing waiting times and shortening hospital stays.
A registry-based study 22 showed that TKR with ERAS protocols has low revision rates and excellent long-term outcomes, highlighting the value of joint registries in improving surgical performance and patient care. These results reinforce the continued adoption of ERAS to optimize TKR outcomes.
This study aims to compare the LOS between the ERAS group and the conventional group in a Hong Kong public hospital, with the hypothesis that patients managed under the ERAS protocol will experience a shorter LOS compared to those treated with conventional methods.
Methods
Patient recruitment and inclusion and exclusion criteria
A retrospective cohort study of total knee arthroplasty patients treated by ERAS were compared with patients in a conventional (non-fast-track) pathway (i.e. conventional cohort), at Pamela Youde Nethersole Eastern Hospital, Hong Kong. Patients diagnosed with osteoarthritis who underwent primary TKR between 2013 and 2023 were recruited in this study, of which patients who underwent TKR in 2013–2016 were treated by conventional pathway (i.e. historical cohort), and patients who underwent TKR in 2021 and 2023 were treated by ERAS protocols. Inclusion criteria included primary unilateral TKR and one-staged bilateral total knee arthroplasty. Exclusion criteria included (1) patients with revision TKR performed, (2) patients with unicompartmental knee replacement performed, and (3) patients who underwent total knee arthroplasty between 2017 and 2020 (the time period that only suitable patients selected for ERAS).
Choices of deep vein thrombosis prophylaxis
For deep vein thrombosis (DVT) prophylaxis, Pradaxa (dabigatran), an oral direct thrombin inhibitor, suits patients with good renal function and a preference for oral medication, while Clexane (enoxaparin), a low-molecular-weight heparin, is favoured for its reversibility, use in bridging warfarin therapy, and suitability for patients with renal impairment.
Choices of implants
In comparing the ERAS and conventional cohorts at Pamela Youde Nethersole Eastern Hospital, differences in implant choice were observed. The common implants used across both groups included Attune, Insall-Burstein III, and Triathlon. However, the ERAS group more frequently utilized Attune RP, Journey II, Legion, and Persona, while the conventional group leaned towards Genesis and press fit condylar.
Choice of anaesthesia
In this study, patients in both the conventional and ERAS groups underwent either general anaesthesia or spinal anaesthesia for TKR, as determined by pre-operative assessment by the anaesthetist. The choice was tailored to individual patient factors, including medical comorbidities, surgical risk, and patient preference, ensuring optimal safety and perioperative management.
Our ERAS protocol
Per-operative nursing and allied health interventions, pre- and post-operative multi-modal analgesia, local infiltrative analgesia, structured rehabilitation protocol aimed at achieving earlier functional mobility (Appendix 4 in the Supplemental materials).
Data collection procedure
This study collected data through a retrospective review of clinical and medical records from patients who had undergone TKR surgery. The primary sources of data included the hospital electronic patient record system – Clinical Management System and hard copies of patient medical records when electronic records were not available.
Data collection time points
Data was collected at three key time points: (1) before TKR, (2) immediately after TKR, and (3) 3 months post-operatively, to assess length of hospital stay.
Sample size calculation and study cohort selection
Between 2013 and 2016, under the conventional treatment pathway, the average number of patients undergoing primary TKR was approximately two to three per week, totalling around 150 procedures annually. In contrast, between 2021 and 2023, following the implementation of the ERAS protocol, the weekly average increased to approximately four to five patients, resulting in an estimated 240 procedures per year.
Applying the inclusion and exclusion criteria, a total of 1283 patients were included in this study cohort. The pre-protocol cohort (n = 575) consisted of patients who underwent surgery using the conventional method before ERAS implementation (2013–2016) and served as the control group (historical control). The protocol cohort (n = 708) included patients who underwent surgery after full implementation of ERAS (2021–2023) and served as the intervention group.
Statistical analysis
Demographic characteristics, pre-op and total LOS, types of implants, navigation (yes, no, robotic), DVT prophylaxis (Clexane, Pradaxa, unknown), and mean number of months among specific time points were summarized by mean ± standard deviation for numeric data or N (%) for categorical data where appropriate. These variables were compared between the ERAS group and the conventional group using Student’s t-test for numeric comparison or a chi-square test for categorical comparisons, where appropriate. Step-wise linear regression modellings on the potential factors, which were found to have statistical significance through the above comparisons, were followed. Both crude and step-wise controlling for confounding variables were carried out to eliminate the influence of possible confounding factors on total length of hospital stay. Dummy variables were created for confounding factors in categorical format. All data analyses were carried out using IBM SPSS 29.0 (Armonk, NY). A two-sided P value ≤0.05 was considered statistically significant.
Results
A total of 1283 patients who underwent TKR were included in this study, with 708 patients in the ERAS group and 575 in the conventional group. Results demonstrated that both the pre-operative and total LOS were significantly reduced in the ERAS group (Table 1). Specifically, the mean pre-op LOS in the ERAS group was 0.18 days (median = 0.00), compared to 0.59 days (median = 1.00) in the conventional group (P < 0.001). Similarly, the mean total LOS was reduced to 7.74 days (median = 6.00) in the ERAS group, versus 10.08 days (median = 8.00) in the conventional group (P < 0.001). Additionally, the mean interval between hospital admission and surgery was significantly shorter in the ERAS group (0.01 months) compared to the conventional group (0.04 months, P = 0.049). Notably, a higher proportion of patients in the conventional group underwent surgery without navigation (13.0% vs 1.4%; P < 0.001). In terms of DVT prophylaxis, Pradaxa was predominantly prescribed in the ERAS group (83.7%), while Clexane was more commonly used in the conventional group (56.9%). Regarding the type of anaesthesia, the percentage of patients who received spinal anaesthesia was significantly higher in the ERAS group than the conventional group (87.3% vs 76.9%; P < 0.001). When controlling for factors such as surgical side (with bilateral as the reference), navigation (with no navigation as the reference), DVT prophylaxis (with others as the reference), and anaesthesia (with general anaesthesia as the reference) in a step-wise linear regression analysis, the use of ERAS remained a statistically significant predictor for a reduced LOS (r2 = 0.064; coefficient (95% confidence interval) = −1.01 (−1.89, −0.13); P = 0.024) (Table 2).
Comparisons of variables between ERAS group and conventional group.
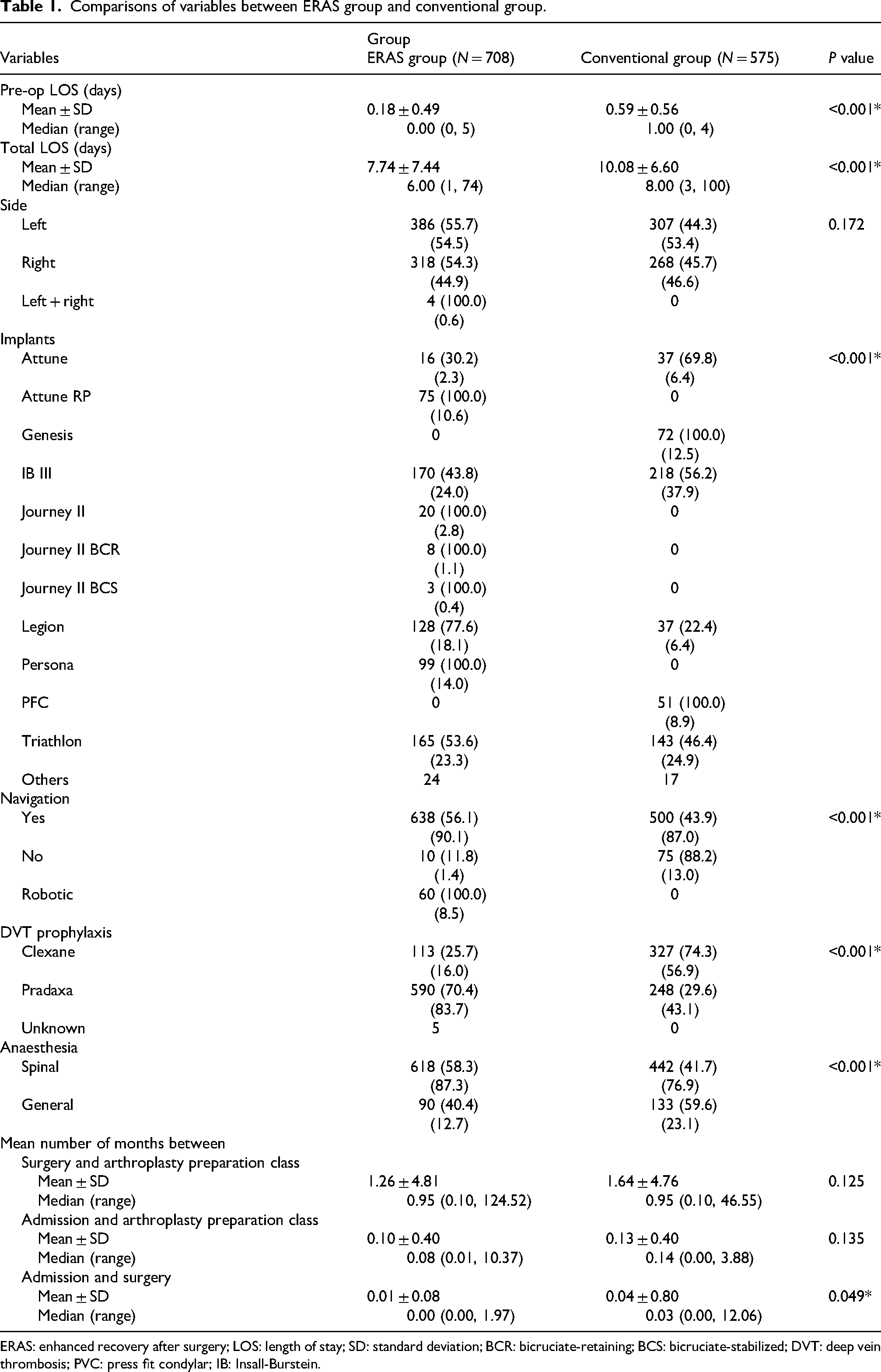
ERAS: enhanced recovery after surgery; LOS: length of stay; SD: standard deviation; BCR: bicruciate-retaining; BCS: bicruciate-stabilized; DVT: deep vein thrombosis; PVC: press fit condylar; IB: Insall-Burstein.
Step-wise linear regression analysis of applying ERAS with potential factors dependent variable: total length of stay (LOS).
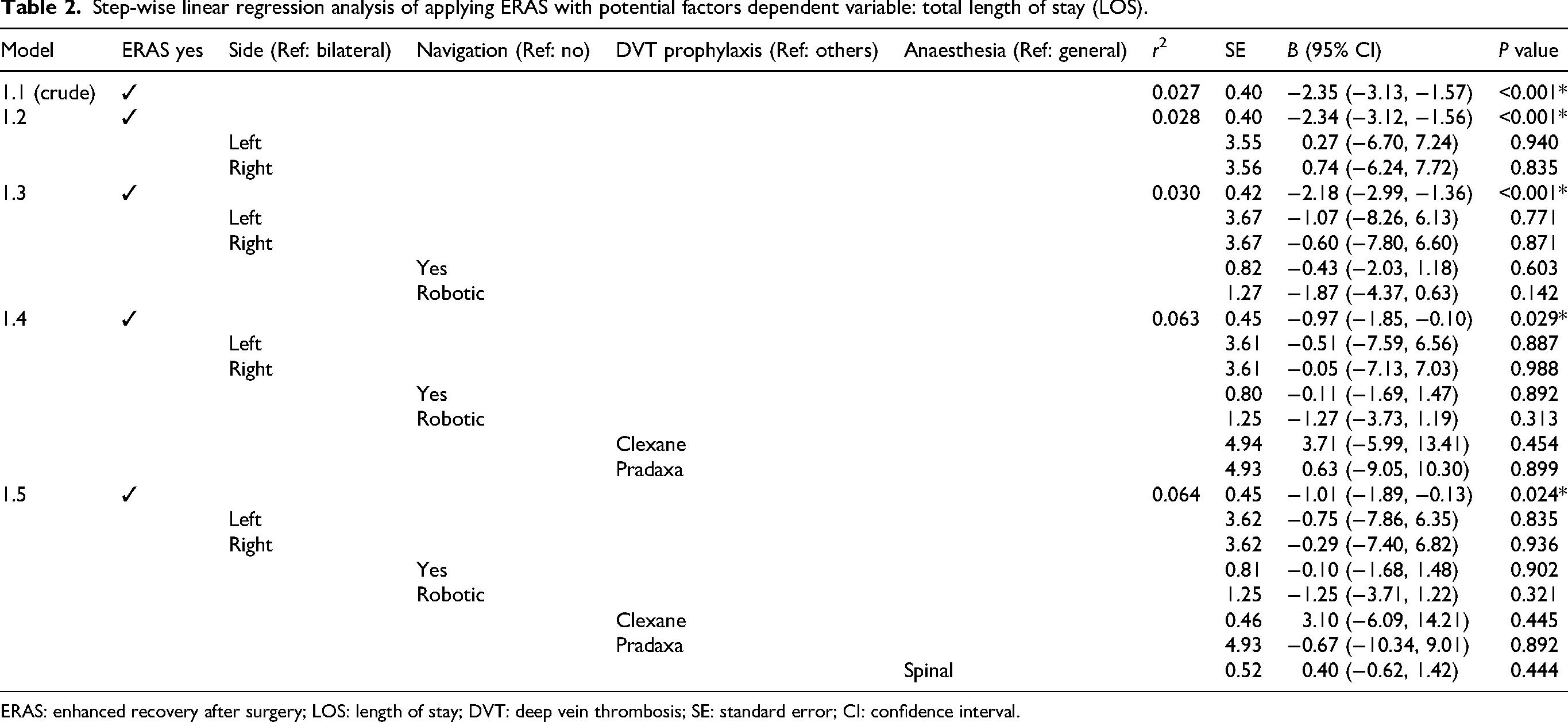
ERAS: enhanced recovery after surgery; LOS: length of stay; DVT: deep vein thrombosis; SE: standard error; CI: confidence interval.
Discussion
The primary aim of this study was to compare the length of hospital stay (LOS) between TKR patients managed under the ERAS protocol and those treated via the conventional pathway at Pamela Youde Nethersole Eastern Hospital, a Hong Kong public hospital. The results support our hypothesis that ERAS leads to a significant improvement in LOS outcomes. Specifically, patients in the ERAS group experienced significantly shorter pre-operative stays, which decreased from an average of 0.59 to 0.18 days, and a reduction in total hospital stays from 10.08 to 7.74 days. Additionally, the interval between hospital admission and surgery was reduced from 0.04 to 0.01 months. This suggests that the comprehensive, multi-disciplinary approach inherent in ERAS not only expedites the pre-operative preparation but also facilitates a faster post-operative recovery. These findings collectively underscore the potential of the ERAS protocol to streamline peri-operative care and enhance recovery in TKR patients.
Several international studies have demonstrated that the use of ERAS protocols in TKR significantly reduces hospital LOS. In New Zealand, the patients undergoing elective knee arthroplasty 1 experienced a reduction in mean LOS from approximately 5 days pre-ERAS to around 4 days post-ERAS. In Denmark, the introduction of fast-track programmes in joint replacement surgery reduced the average hospital stay from 8 to just 3.8 days. 23 Similarly, in Singapore, the adoption of ERAS protocols for TKR reduced the average hospital stay from 5.4 to only 2.9 days. 19 Moreover, data from the UK National Joint Registry indicate that NHS trusts observed a decrease in average LOS for TKR from 5.8 to 3.7 days following ERAS implementation. 24 These international findings are particularly compelling when considering that the NHS and Hong Kong's public healthcare systems share similar operational frameworks. Such comparisons suggest that Hong Kong could experience comparable benefits, including expedited patient recovery and optimized resource utilization. At Pamela Youde Nethersole Eastern Hospital, the post-ERAS LOS of 7.74 days is higher than that reported in regions like Denmark (3.8 days), Singapore (2.9 days), and the United Kingdom (3.7 days), but it still reflects a significant improvement over the pre-ERAS LOS of 10.08 days.
Moreover, our analysis indicates that the benefits of ERAS are independent of other influential factors such as the surgical side, the use of navigation technology, the choice of DVT prophylaxis, and choice of anaesthesia. Even after adjusting for these variables, ERAS maintained a statistically significant impact on reducing LOS. This supports the concept that the multi-modal interventions – ranging from pre-operative education and optimization to post-operative pain management and early mobilization – play a crucial role in enhancing recovery outcomes.
These findings are particularly relevant for healthcare settings like our Hong Kong public hospital, where optimizing patient throughput without compromising care quality is essential. By reducing LOS, ERAS not only improves patient satisfaction and clinical outcomes but also contributes to more efficient use of hospital resources. Future studies could build upon these results by exploring long-term outcomes and quality-of-life measures post-TKR further substantiating the widespread adoption of ERAS protocols in joint replacement surgeries.
Limitations of this study
This study has several limitations that may have influenced our results. As a retrospective study, we were unable to control for all potential factors, such as variations in patient comorbidities and subtle changes in clinical practice, for example, choices of implants, choice of anaesthesia over time. Additionally, relying on existing clinical records meant that some details – like patient adherence to post-operative rehabilitation – were not fully captured. These limitations may affect how broadly our findings can be applied, and further prospective research is needed to confirm these results.
Conclusions
After the implementation of ERAS in patients after TKR, length of hospital stay was significantly decreased with or without using navigation or the choice of DVT prophylaxis or choice of anaesthesia. Further investigations were warranted to implement a multi-centre large-scale long-term study to explore long-term outcomes and quality-of-life measures post-TKR.
Supplemental Material
sj-docx-1-otr-10.1177_22104917251382948 - Supplemental material for Results of enhanced recovery after surgery (ERAS) for total knee replacement in a Hong Kong public hospital
Supplemental material, sj-docx-1-otr-10.1177_22104917251382948 for Results of enhanced recovery after surgery (ERAS) for total knee replacement in a Hong Kong public hospital by Ho-Ken Fong, Wai-Wang Chau, Ying-Cheung Cheng and Man-Kwan Wong in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-docx-2-otr-10.1177_22104917251382948 - Supplemental material for Results of enhanced recovery after surgery (ERAS) for total knee replacement in a Hong Kong public hospital
Supplemental material, sj-docx-2-otr-10.1177_22104917251382948 for Results of enhanced recovery after surgery (ERAS) for total knee replacement in a Hong Kong public hospital by Ho-Ken Fong, Wai-Wang Chau, Ying-Cheung Cheng and Man-Kwan Wong in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-docx-3-otr-10.1177_22104917251382948 - Supplemental material for Results of enhanced recovery after surgery (ERAS) for total knee replacement in a Hong Kong public hospital
Supplemental material, sj-docx-3-otr-10.1177_22104917251382948 for Results of enhanced recovery after surgery (ERAS) for total knee replacement in a Hong Kong public hospital by Ho-Ken Fong, Wai-Wang Chau, Ying-Cheung Cheng and Man-Kwan Wong in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-docx-4-otr-10.1177_22104917251382948 - Supplemental material for Results of enhanced recovery after surgery (ERAS) for total knee replacement in a Hong Kong public hospital
Supplemental material, sj-docx-4-otr-10.1177_22104917251382948 for Results of enhanced recovery after surgery (ERAS) for total knee replacement in a Hong Kong public hospital by Ho-Ken Fong, Wai-Wang Chau, Ying-Cheung Cheng and Man-Kwan Wong in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Abbreviations
Ethical approval and informed consent statements
Ethical approval was obtained from the ethics review board of the Hospital Authority Central Institutional Review Board (Central IRB) (Ref. No. CIRB-2024-611-5). The study protocol complied with the Declaration of Helsinki. Informed consent has been obtained from all participants.
Author contributions
Ho-Ken Fong and Man-Kwan Wong conceptualized the development for the research. Ho-Ken Fong conducted literature search, assessed patients and carried out data collection, data extraction, data synthesis, and data integration. Ying-Cheung Cheng conducted data collection. Wai-Wang Chau performed data analysis. Ho-Ken Fong and Wai-Wang Chau drafted and revised for the important intellectual content of the manuscript. All authors reviewed, revised, and approved the final version of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.