
Abstract
Introduction
The optimal thickness of the cement mantle in cemented total knee arthroplasty (TKA) has been proposed to be 3–5 mm. This study aims to assess the association between cement mantle thickness in TKA and radiolucent lines (RLLs). A secondary objective was to investigate the significance of cement penetration into the anterior tibial pin tracks.
Methods
100 primary TKA performed by five surgeons in the total joint replacement team were included from 2017–2018. Initial postoperative radiographs were assessed to measure the cement penetration at the tibial component at different zones according to the Knee Society Scoring System and the presence of cement penetration into pin tracks. Postoperative radiographs at 2 years were evaluated for RLLs at each zone.
Results
TKA were grouped by cement mantle thickness into <3 mm, 3–5 mm and >5 mm. There was a significantly higher incidence of RLLs at the implant–cement junction from the <3 mm cement thickness group at the anteroposterior Zone 6, corresponding to the distal end of the tibial keel/stem. Five out of 12 patients (41.7%) had RLL in the <3 mm group, compared to 7 out of 64 (10.9%) in the 3–5 mm group and 2 out of 24 (8.3%) in the >5 mm group (p = .003). At the other zones, there was no difference in RLL around the tibial tray in the different cement thickness groups. In the different cement thickness groups, there were no significant differences in the incidence of pin track cement penetration.
Conclusion
Below the tibial tray, there were no differences in RLLs between the cement thickness groups, which may challenge the importance placed on the accepted optimal cement thickness of 3–5 mm. However, at the tip of the tibial keel/stem, a cement thickness of >3 mm for TKA is suggested, which was associated with less RLL.
Introduction
The optimal thickness of the cement mantle in cemented total knee arthroplasty (TKA) has been proposed to be 3–5 mm for implant stability.1–3 A cement mantle that is too thin may result in poor fixation strength or be at increased risk of cement fracture, leading to early component loosening.3–5 However, a cement mantle that is too thick may induce thermal osteonecrosis.1,6
There are multiple factors that may influence cement penetration into bone. The depth of cement penetration has been shown to increase with lower cement viscosity and osteoporotic bone.7,8 Cementing techniques play a crucial role in influencing cement thickness. Bleeding at the bony interfaces reduces the shear strength of the bone–cement interface by up to 50%.9,10 Cleansing of the bone surface with pulsatile lavage has been shown to improve cement penetration.2,11–13 Kopec showed that compared to hand packing, the use of a cement pressurization gun did not significantly increase the thickness of the cement mantle under the tibial tray. 14
Regarding implant design, early Attune tibial trays (Attune total knee system, DePuy, Warsaw, IN, USA) lacked cement adhesion in retrieval studies, in contrast to other designs. This was partly attributed to the implant's lack of cement pockets, which allows a thicker cement mantle. 15 It was noted that with certain knee arthroplasty designs, the pin tracks drilled to stabilize the tibial cutting jig communicate with the cement fixation interface (Figure 1). This shows up as cement filling of the pin track on the lateral radiograph (Figure 2). Theoretically, this should be associated with the pressurization and penetration of the cement and hence may be reflected in the cement mantle thickness.

Intraoperative photograph showing the pin tract communicating with the tibial implant–cement interface.

Cement penetration into pin tracks.
There is a paucity of studies investigating the effect of variable cement mantle thickness on radiolucent lines (RLLs) in TKA. The aim of this study was to assess the association between cement mantle thickness in TKA and RLLs, a predictor of loosening. We hypothesize that a thinner cement mantle may be associated with an increased incidence of RLLs. A secondary hypothesis is that cement penetration into pin tracks is associated with thicker cement mantles.
Materials and methods
A retrospective review of total knee arthroplasties in 2017–2018 for primary knee osteoarthritis with a posterior stabilized prosthesis of the same model (Attune total knee system, DePuy, Warsaw, IN, USA) was performed. Fulfilling the above criteria, the 20 most recent total knee arthroplasties performed by each surgeon of the arthroplasty team at a single institution were selected, with five surgeons to make up a total of 100 total knee arthroplasties. Implants with stem extension, and patients with secondary osteoarthritis (for example: rheumatoid arthritis, post-traumatic) were excluded. TKA was performed by a standard medial parapatellar approach. The bone surface was prepared using pulsatile lavage. All surgeons used the same brand of cement (Palacos, Zimmer, Warsaw, IN, USA), and the cement was vacuum mixed and applied by hand onto the tibial and femoral bone surface as well as the implant, in particular with cement applied to both under the tray and the keel of the tibial component. After component insertion, the knee was held in extension until the cement set. There was slight variation in cementing techniques between the surgeons. One surgeon used a technique of finger packing of cement to pressurize the intramedullary cavity before insertion of the implant. One surgeon did not use a tourniquet during cementation, and the other surgeons used a tourniquet from skin incision until the cementation was completed.
The radiographs were assessed by a single surgeon who did not participate in the surgeries. The cement mantle thickness in the initial postoperative anteroposterior (AP) and lateral radiographs was measured for the tibial component at each zone according to the Knee Society TKA roentgenographic evaluation and scoring system shown in Figure 3. 16 In the AP view, zones 1 and 2 (medial) and zones 3 and 4 (lateral) represent the zones under the tibial tray. Zones 5 to 7 represented the area around the stem or keel. In the lateral view, zone 1 represents the anterior tibial tray, 2 is the posterior tibial tray, and 3 is around the stem or keel. Femoral component cement mantle thickness was not measured in view of potential inaccuracy due to the implant design. The metal artefact overlying the femoral condyle may cause obscuration of the implant–cement interface. All the radiographs are digital and measured by a standardized digital ruler. If there was any cement visualized in the pin tracks over the anterior tibia, this was a positive pin track sign (Figure 1). Postoperative radiographs at 2 years were evaluated for RLL at each zone, both at the implant–cement junction, and the bone–cement junction. RLL that were present in the initial postoperative radiographs were not counted.

Anteroposterior and lateral radiographs according to the Knee Society zones.
Statistical analysis was performed using SPSS Statistics version 24 (IBM Corp. Armonk, USA). Numerical data were analysed with one-way ANOVA and categorical data were analysed with the chi-square test. The significance level was set at p < .05.
This study has been approved by the Institutional Review Board (IRB) of the hospital.
Results
There were a total of 21 males, and 79 females included in the study. The mean age of the study population was 67.6 ± 7.28 years. The mean cement mantle thickness was lowest 1.6 mm over the AP view tibia zone 1 (medial tibial tray), and greatest around the tibial keel (AP view zones 5, 6, 7 and lateral view zone 3), with mean cement thicknesses >4 mm (Table 1).
Table showing the mean cement thickness and frequencies by zones (tibia).
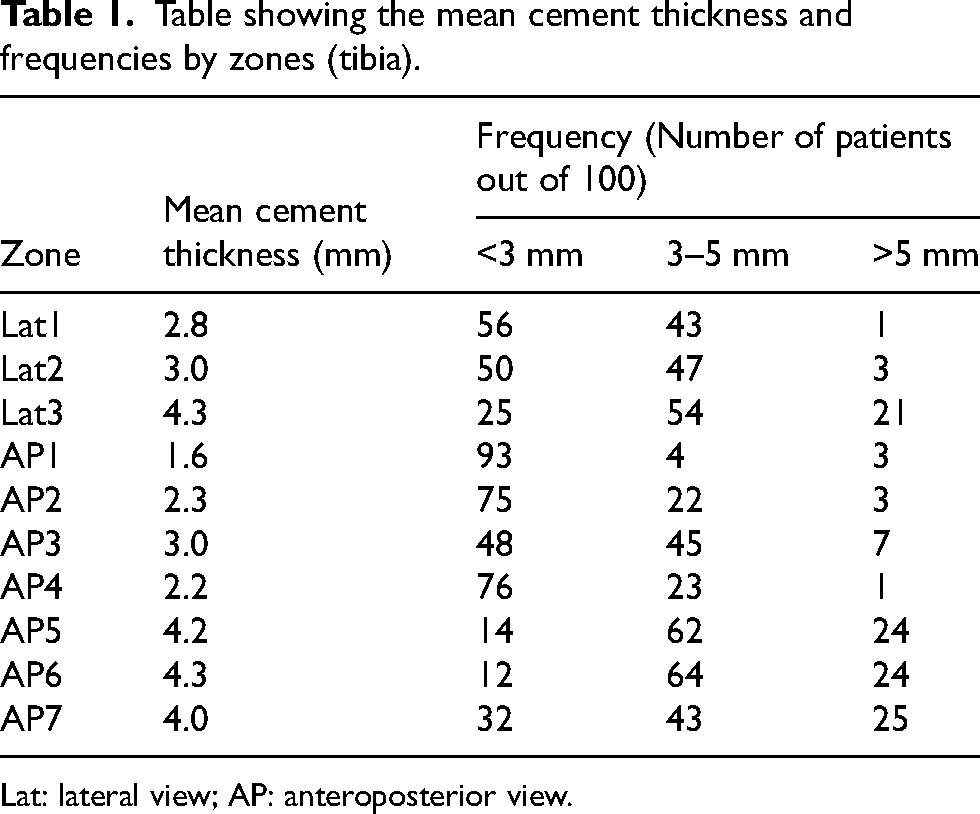
Lat: lateral view; AP: anteroposterior view.
Cement thickness vs radiolucent lines
The only significant differences were noted at AP view zone 6 (distal tip of tibial keel), which is shown in Table 2. In this zone, there were 12 patients in the <3 mm group, 64 in the 3–5 mm group and 24 in the >5 mm group. There was a significantly higher incidence of RLLs at the implant–cement junction from the <3 mm cement thickness group at the AP Zone 6, corresponding to the distal end of the tibial keel/stem. Five out of 12 patients (41.7%) had RLL in the <3 mm group, compared to 7 out of 64 (10.9%) in the 3–5 mm group and 2 out of 24 (8.3%) in the >5 mm group (p = .003). At the other zones, there were no differences in RLL and cement thickness.
Table showing the cement thickness and radiolucent lines at AP view zone 6 (tibia).
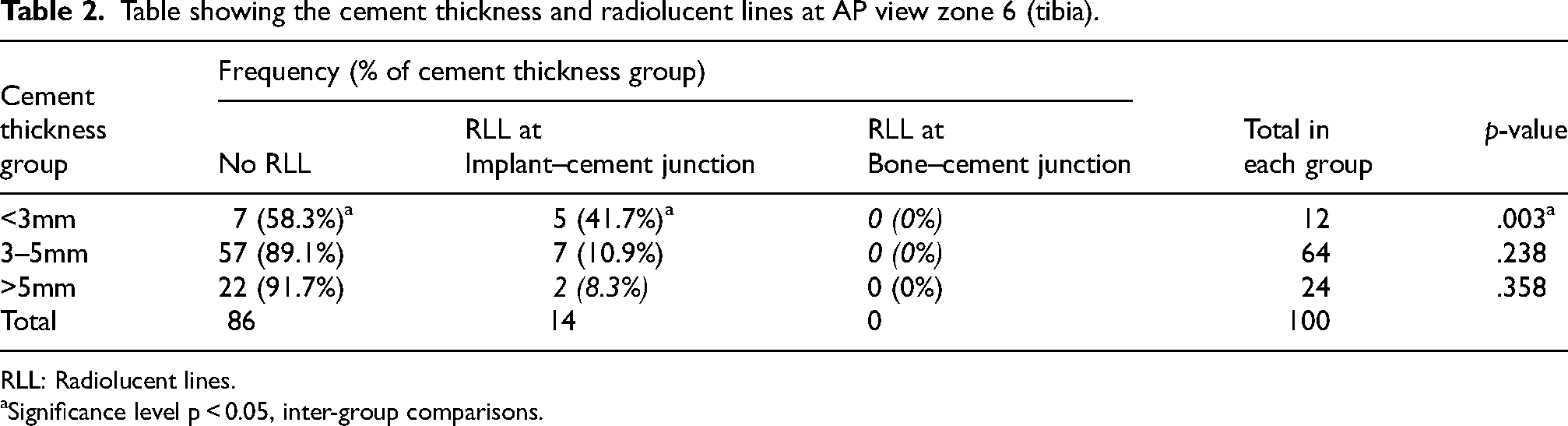
RLL: Radiolucent lines.
Significance level p < 0.05, inter-group comparisons.
Cement thickness vs pin tracks
Sixty-nine patients (69%) showed a positive pin track sign. There were no significant differences between the cement mantle thickness group and the incidence of the pin track sign (Table 3).
Table showing the cement thickness and pin track sign at each zone (tibia).
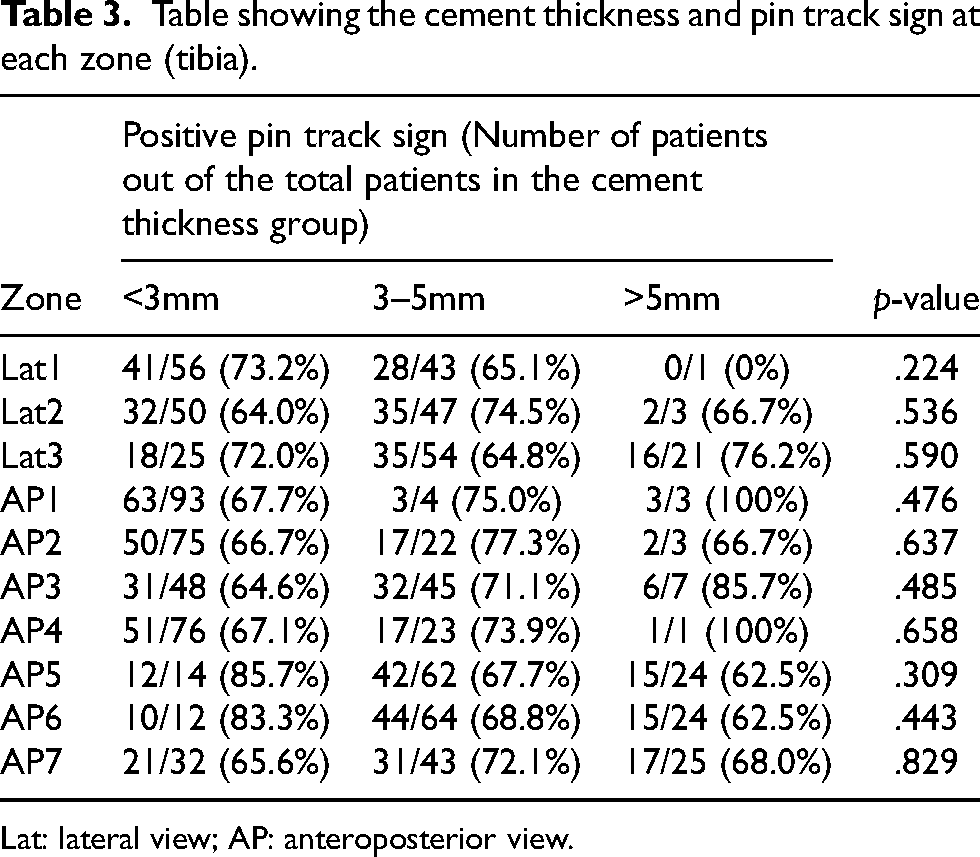
Lat: lateral view; AP: anteroposterior view.
Discussion
Thin cement mantles have been associated with decreased mechanical advantage at the bone–cement interface due to inadequate cement penetration into the cancellous bone, leading to micromotion and fixation failure.3,7 Cement penetration >5 mm did not further increase the interface strength and may cause harmful heat-induced osteonecrosis, which may lead to loosening.3,7 Impaction of the implant to bone is also important, as a thick cement mantle may reduce the gap balance. 17 Therefore, the optimal thickness of the cement mantle in TKA has been proposed to be 3–5 mm for implant stability.1–3 These suggestions typically refer to the cement mantle under the tibial tray. In the present study, there were no significant differences in the incidence of RLL and the cement mantle thickness at the tibial tray. The only significant difference was noted at the tibial keel/stem.
There are controversies regarding the mechanical advantages of full cementation (cementation to the tibial tray and stem) versus surface cementation (cementation of tibial tray only) of the tibial component.5,18–20 The theoretical advantages of surface cementation include less bone loss in the case of revision, and less stress shielding. A biomechanical study found that there was greater stress reduction at the tibial tray in full cementation compared to surface cementation, with more stress shielding theoretically resulting in more bone resorption.18,19 Bert showed that surface cementation was biomechanically inferior to full cementation if the cement mantle was <3 mm thick under the tibial tray. 21 However, when the cement penetration was >3 mm, there was no difference in stability between surface and full cementation.
The results from the present study challenge the importance of the cement mantle thickness under the tibial tray. There were no differences in RLL in the different cement groups. The thinner cement mantle <3 mm group had similar findings to the groups >3 mm. A biomechanical cadaver study by Peters also showed no difference in tibial component micromotion implanted with full or surface cementation. 5 This was further supported clinically by Galasso et al. who found no difference in revision rates for loosening in a group of 232 patients who underwent full or surface cementation at an average of 5.6 years postoperatively. 20
On the other hand, a thinner cement mantle <3 mm at the tibial keel/stem tip was associated with increased incidence of RLL. 47% of the <3 mm group was noted to have RLL at this zone, and all were at the implant–cement junction. A potential explanation for this phenomenon is that the thicker cement penetration at the tip of the keel/stem may contribute to minimize the toggling effect of the tibial component during motion of the knee, thus presenting with a lower incidence in RLL. That being said, it is debatable whether this small finite increase in cement mantle thickness at the keel/stem may actually translate to lower rates of loosening. Clinical studies with larger sample sizes and adequate follow-up durations to assess the rates of aseptic loosening with different cement mantle thicknesses will be useful to further explore the practical implications of this study.
The design features of the TKA implants play a crucial role in the cement mantle thickness and stability. The smooth undersurface of the Attune tibial implant has been criticized as a contributing factor for tibial debonding of the implant from the cement. Wang showed that shear strength was increased for cemented implants with higher roughness, 22 although a retrieval study by Cerquiglini of implants of different roughness showed no significant difference in cement adhesion after retrieval. 15 According to a retrieval analysis study, the Attune TKA prosthesis is designed with a peripheral lip to prevent cement escape, with of an average of 0.61 mm. 15 In contrast to other commonly used systems, the early Attune tibial component did not contain deeper cement pockets, designed for a thicker cement layer.15,23,24 The cement pockets may trap the cement and provide additional pressurization for deeper penetration into bone. The newer Attune S + prostheses have cement pockets with a dovetail design to provide a cement lock between the bone and implant interface. The implants used in this study were the traditional Attune implants from 2017 to 2018, before the introduction of the new Attune S + models.
The thinnest cement mantle was over the medial tibial tray and thickest around the tibial keel. A possible explanation is that the majority of osteoarthritic knees predominantly affect the medial compartment. Abnormal loading leads to sclerotic and denser bone, thus increasing the resistance to cement penetration. In contrast, the tibial keel is over the metaphysis, containing more porous cancellous bone of lower resistance, allowing deeper cement penetration. Additionally, finger pressurization of the cement around the keel was possible before implant insertion with this particular implant. Certain prosthesis models have a very thin and narrow tibial keel, which will not allow sufficient space for finger pressurization.
Cement filling of the pin tracks was not an uncommon finding – this was present in 69% of patients. There were no significant differences between the cement mantle thickness group and the incidence of the pin track sign. This radiological pin track sign may be a potential novel marker for cement penetration and the quality of bone, but its significance has yet to be determined. However, its use may only be limited to TKA models that have pin tracks that communicate with the cement interface. A grading system can also be developed to the quantify the proportion of the pin track occupied by cement.
A limitation was that this was a radiographic study, which is a 2D analysis. For instance, there may be a nonuniform thickness of the cement when assessed from the AP direction, but in the radiograph, we will only measure the opacity of the thickest cement mantle. It is difficult to achieve uniform cement penetration throughout the fixation interface. Cement penetration tends to be high centrally, and low around the periphery, which may be affected by peripheral irregularities and variable areas of sclerotic bone. A cement impactor has been proposed to create a more uniform cement mantle. 25 We may consider in vivo studies such as implant retrieval studies to assess the true cement thickness.
Conclusion
Below the tibial tray, there were no particular differences in RLLs between the cement thickness groups, which may challenge the importance placed on the accepted optimal cement thickness of 3–5 mm. However, at the tip of the tibial keel/stem, a cement thickness of >3 mm for TKA is suggested, which was associated with less RLL.
Footnotes
Author contributions
MHL collected the data, performed the statistical analysis and drafted the manuscript. AC, HF, and PKC participated in the design, and helped to revise the manuscript critically. CHY and KYC conceptualized the study and participated in the design and coordination. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent
This study has been approved by the Institutional Review Board (IRB) of the University of Hong Kong/Hospital Authority (IRB Reference: UW 19-633). Consent was waived as this was a retrospective study of past radiographs and there was no patient intervention.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.