
Abstract
Introduction
Distal radius fractures (DRF) are among the most frequently encountered upper limb fractures and account for up to one-sixth of the fractures seen in the emergency department. 1 The incidence peaks in the 50- to 60-year age group.2,3 Additionally, distal ulnar fractures commonly occur in conjunction with DRF, with an incidence ranging from just over 20% to more than 50%.4,5
Some studies have suggested that a concomitant fracture of the ulnar styloid with a DRF indicates poorer clinical outcomes. These include increased wrist pain, worse functional outcomes, 6 and distal radioulnar joint (DRUJ) instability and stiffness, regardless of the healing status post-injury. 7 However, this has not been widely reported.
Conversely, other studies indicate that an untreated ulnar styloid fracture (USF) is not associated with a worse functional outcome.8,9 A meta-analysis conducted in 2014 found no correlation between functional outcomes and the non-union status of the styloid process. 10 Furthermore, the consolidation status of an accompanying ulnar styloid process does not influence patient-reported outcomes, nor does it affect function, pain, or DRUJ instability after a DRF has healed. 11
The objective of this study was to analyse the differences in outcomes between local patients with and without a concomitant distal ulnar fracture who underwent surgery for a DRF, in order to provide implications for future treatment planning and patient selection for different treatment modality, thereby enhancing patient outcomes.
Patients and methods
This is a retrospective cohort study comparing DRF patients with or without USF, with the functional outcomes measured at two intervals: 3 months and 6 months. The functional outcomes included objective measurements of joint range of movement (ROM), Visual Analogue Scale (VAS), and the Disabilities of the Arm, Shoulder, and Hand (DASH) score. Patients aged 50–69, who were admitted to two regional hospitals (Tuen Mun Hospital and Pok Oi Hospital) with acute trauma service with a DRF and subsequently underwent surgery, were assessed for eligibility. The study protocol was approved by the New Territories West Cluster Research Ethics Committee. A total of 614 patients who were admitted to hospitals with operated DRF were assessed for eligibility for the study between November 2018 and October 2020.
The indications for internal fixation of distal radius included significant dorsal tilt, decreased radial inclination angle, radial height shortening, and significant ulnar variance differences compared to the contralateral side. Additional indications were the presence of intra-articular fractures, which may require more precise anatomical reduction and stabilisation. The exclusion criteria included multiple fractures on the same limb, bilateral wrist involvement, coconmitant ulnar fracture proximal to styloid, extreme age range, patients who preferred conservative treatment, loss of follow-up, and incomplete data. Elderly patients (age ≥ 70) were not included in the study because conservative treatment is generally adopted for this patient group. A meta-analysis has shown the clinical outcomes between surgical and nonsurgical methods were comparable and had no impact on the quality of life. 12 After exclusion criteria, 157 were included in the analysis. The study flow chart is illustrated in Figure 1.
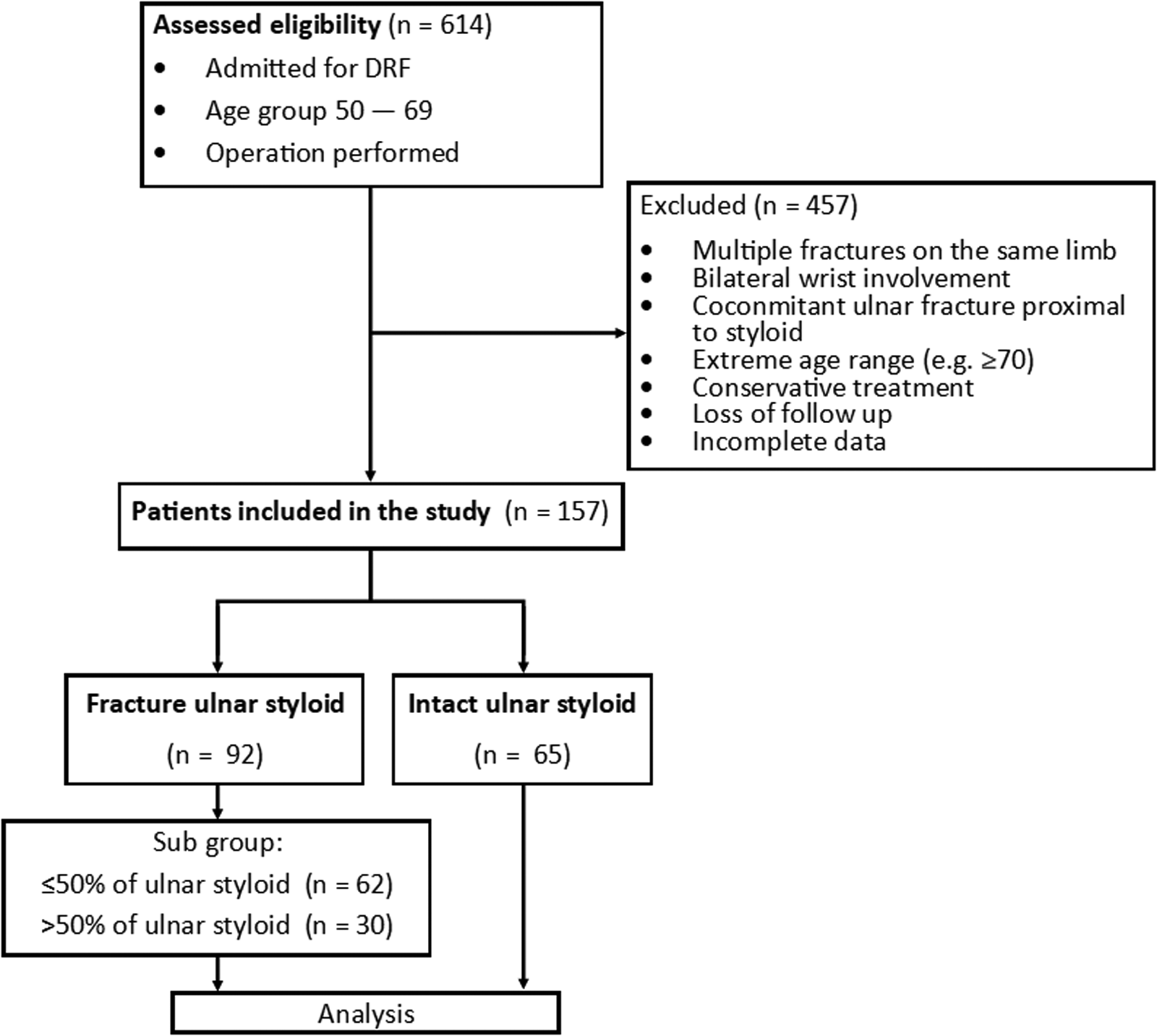
The study flow chart.
Data were gathered during each follow-up appointment at the aforementioned intervals. Joint ROM was measured by goniometer by trained personnel to ensure consistency and accuracy, and patient-reported outcomes, i.e. the VAS and DASH score, were collected via questionnaires administered during these visits. The data from the two groups were then compared to identify any significant differences in outcomes.
The concomitant USF group was further categorised into two groups according to the injury radiographs, depending on the size of the ulnar process styloid fragment: those with 50% or less of the ulnar styloid process and those with more than 50% of the ulnar styloid involved. Figure 2 shows how the height of the ulnar styloid was measured on the radiograph. A fracture fragment less than or equal to 50% of the height is considered the ‘tip’ involvement, and more than 50% is considered ‘base’ involvement. The data were stratified accordingly and compared at the specified intervals.
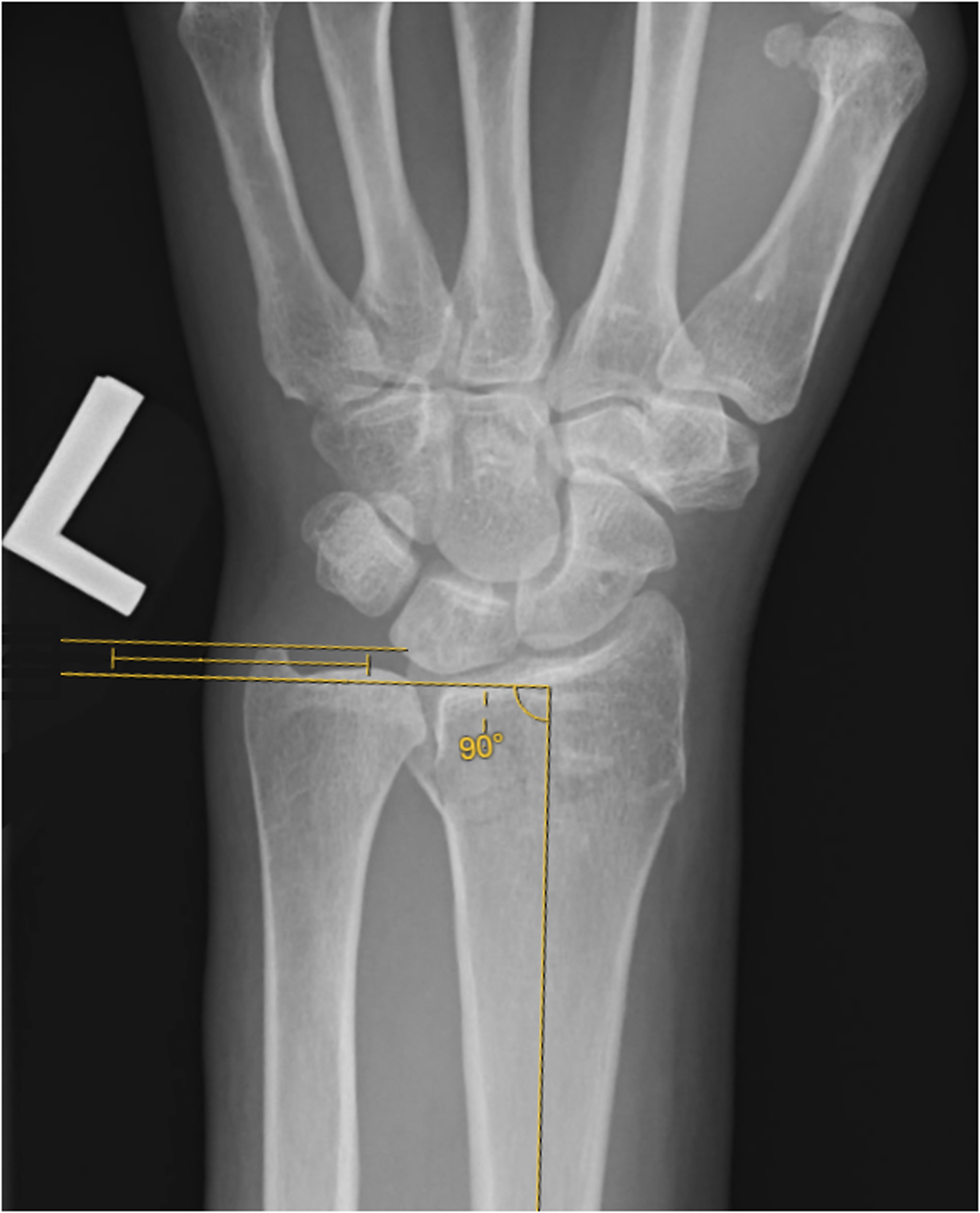
Fracture of the ulnar styloid base was defined as a fracture at least 50% of the total height on the posteroanterior radiograph of the wrist.
All results were expressed as medians with the interquartile range in brackets. A Shapiro–Wilk test was conducted to assess the normality of the data distribution. Differences between the two groups in age, ROM, VAS, and DASH score were evaluated using the Mann–Whitney U test. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed using the R Statistical Software (v4.4.0). 13
Results and outcome
The cohort comprised 102 women (65%) and 55 men (35%) with a mean age of 58.4 years. Of the participants, 86 patients (55%) had associated USF, while 71 (45%) had intact ulnar styloid. All USF in both groups were treated conservatively. All the DRF were closed fractures and treated by surgical fixation with plates by volar approach. Demographic data are presented in Table 1.
The demographic data.
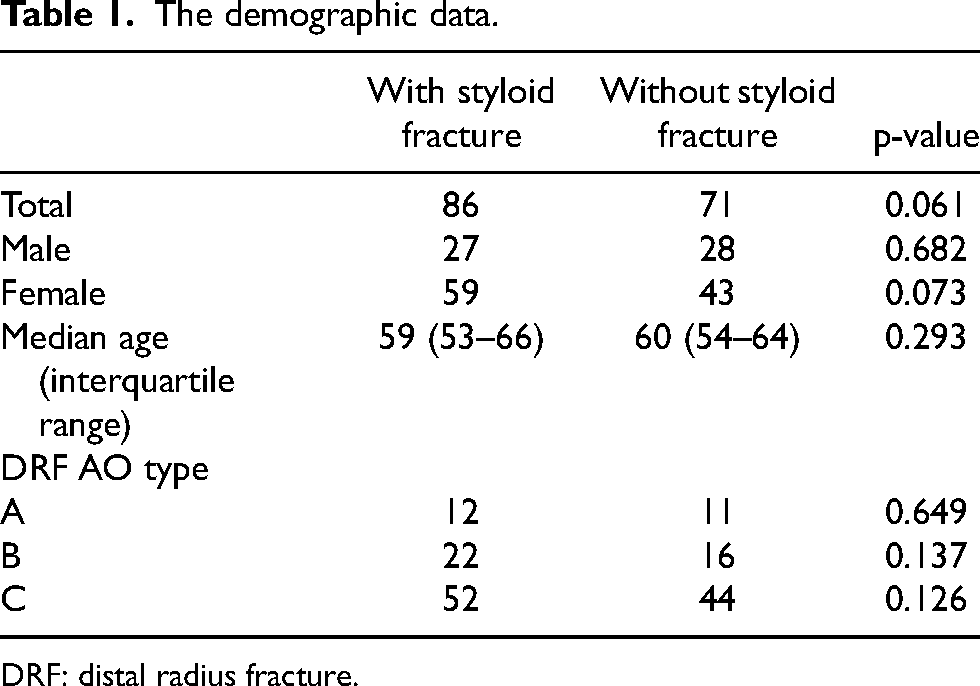
DRF: distal radius fracture.
The intact ulnar styloid group had the same median ROM in all directions when compared to the fracture ulnar styloid group at 3 months. At 6 months, the median ROM for all directions showed no significant differences between the two groups. Table 2 showed the ROM of the two groups at 3 months and 6 months respectively. The median VAS and DASH score showed no significant differences at both 3 months and 6 months. Table 3 shows the detailed outcome in VAS and DASH score of the two groups at 3 months and 6 months respectively.
ROM at 3 months and 6 months.
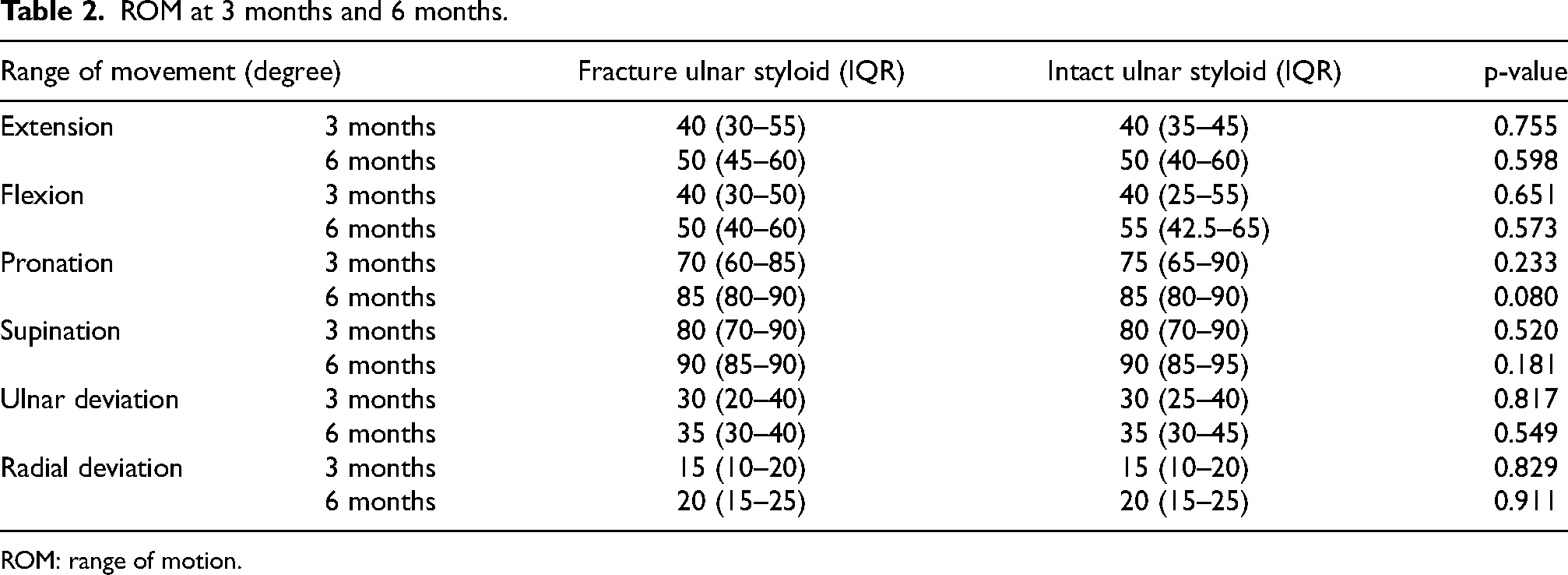
ROM: range of motion.
Detail outcome in VAS and DASH score at 3 months and 6 months.

VAS: visual analogue scale; DASH: Disabilities of the Arm, Shoulder, and Hand.
The fracture ulnar styloid group was categorised into two subgroups, involvement of the ulnar styloid tip and the base. These subgroups were compared to the intact group, and the data were analysed accordingly.
Regarding the ROM, both subgroups demonstrated comparable results to the intact group at both the 3-month and 6-month evaluations without any statistically significant differences. Table 4 detailed clinical outcomes of the subgroups.
ROM at 3 months and 6 months including the subgroups.
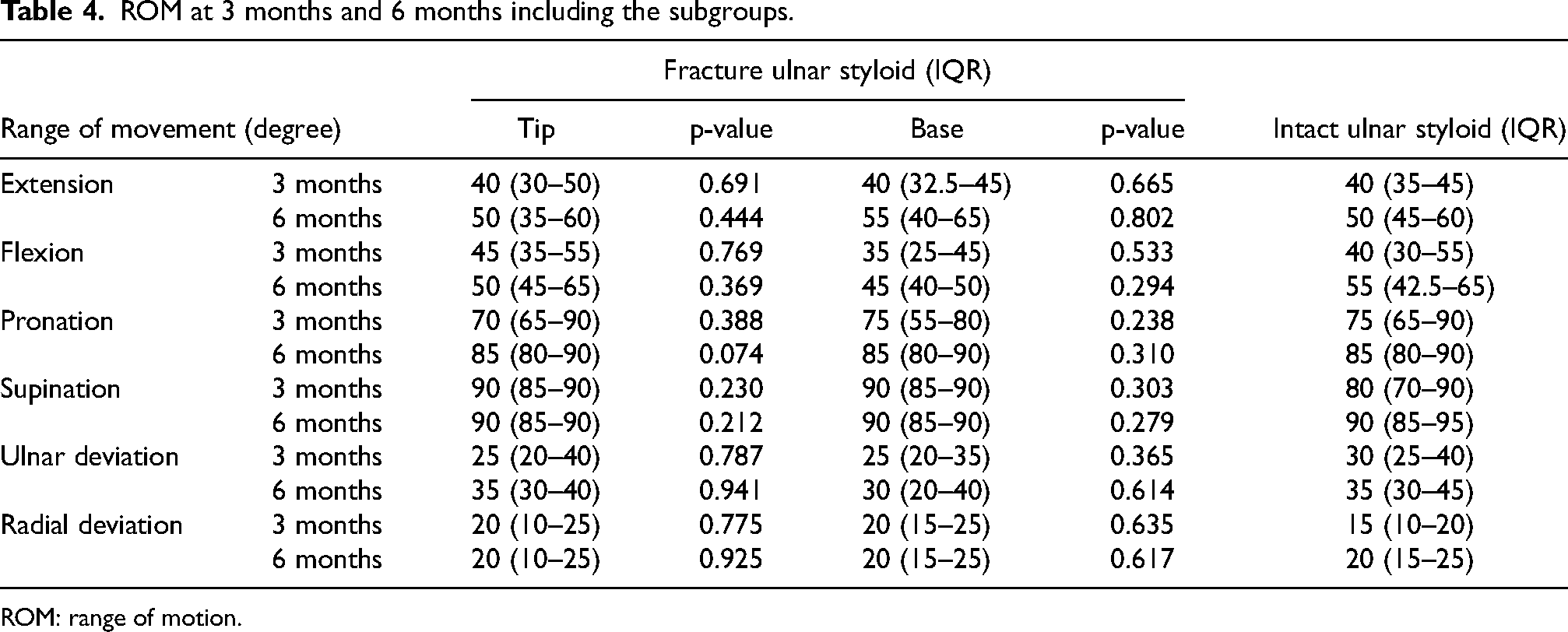
ROM: range of motion.
The group with tip involvement showed no significant differences compared to the intact group in both VAS and DASH score at 3 and 6 months. The group with base involvement exhibited a worse score on the DASH score compared to the intact group at both 3 months and 6 months, which was statistically significant. The VAS was significantly higher in the group with base involvement at 6 months compared to the intact group, but this difference was not present at the 3-month assessment. Table 5 shows the detail clinical outcomes of the subgroups at 3 months and 6 months, respectively.
Detail outcome in VAS and DASH score at 3 months and 6 months including the subgroups.
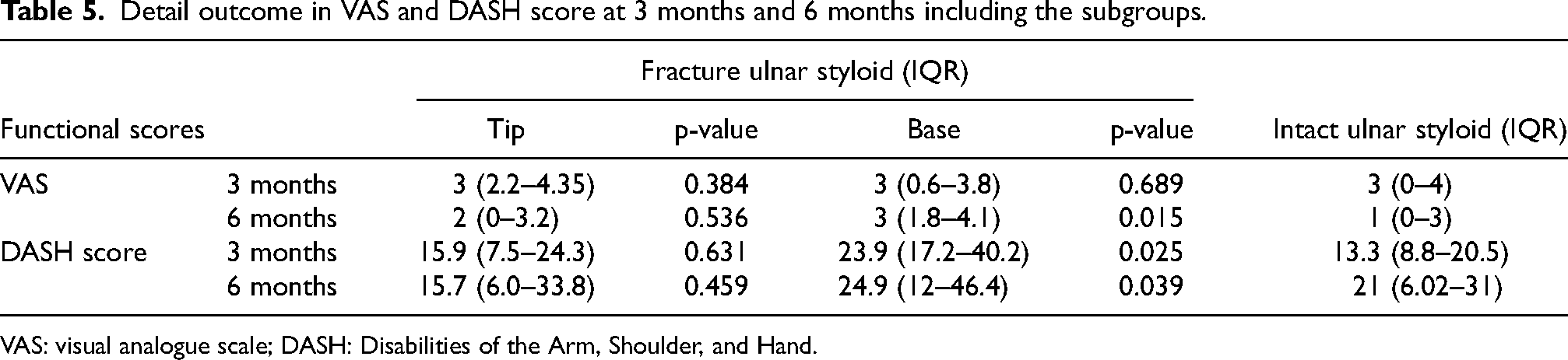
VAS: visual analogue scale; DASH: Disabilities of the Arm, Shoulder, and Hand.
Discussion
Our study showed that, regardless of the presence of an associated USF, there were no significant differences in terms of functional and pain outcome. This finding aligns with previous studies conducted in regions such as Japan, The Netherlands, and the United States.8,10,11 The subgroup analysis revealed different findings. Patients with a fracture of the ulnar styloid involving more than 50% showed poorer patient-reported clinical outcomes when compared to the intact group, specifically showing increased VAS at 3 months post-operation and higher DASH score at 3 and 6 months post-operation. In terms of the objective measurement, namely the ROM, there were no differences when compared the subgroups. Other previous studies have reported similar findings, stating an associated USF results in worse functional outcomes and pain, but had no effects on the range.6,14
This conflicting finding suggests that the presence of a concomitant ulnar styloid tip fracture is clinically insignificant and does not warrant any surgical interventions. However, more extensive involvement of the ulnar styloid (>50% involvement) may lead to poorer clinical outcomes, in terms of pain and upper limb function. In a recent retrospective study, Velmurugesan et al. 15 discovered that a non-union fracture at the base of the ulnar styloid led to significantly poorer outcomes in terms of ulnar wrist pain and function, as measured by the QuickDASH score. The incidence of ulnar wrist pain was significantly higher if the styloid fragment was displaced by more than 2 mm. Since the Triangular Fibrocartilage Complex (TFCC) attaches at the base of the styloid and the ulnar fovea, a more proximal styloid fracture is associated with a higher incidence of TFCC tears and DRUJ instability, as demonstrated by Nakamura et al. 16 in cadaveric models. Chronic pain at ulnar styloid non-union sites, a reported consequence, can affect postoperative clinical outcomes. 17
Velmurugesan et al. 15 suggested that surgical management of styloid fractures could reduce the risk of non-union and alleviate ulnar-side wrist pain. Wrist arthroscopy can assess both contributing pathologies and perform necessary repairs during the fixation of DRF. However, Fok et al. studied the status of the TFCC after DRF union and found that most TFCC tears remained unhealed, though not all patients with tears were symptomatic. 18 Similarly, results from Zenke et al. indicated no significant differences between acute fixation of ulnar styloid base fractures and no fixation. 19 This added the value of our findings that, while patients with >50% USF often experience chronic pain, routine wrist arthroscopy or ulnar styloid fixation during acute stage operations in concomitant with distal radius fixation may constitute overtreatment and is not always necessary.
More practically, patients with persistent clinical symptoms of DRUJ instability or ulnar wrist pain after 3 months may warrant a second-stage arthroscopy. Park et al. suggested arthroscopic foveal repair of TFCC to stabilise the DRUJ could provide satisfactory clinical and functional outcomes and decreased ulnar-sided pain. 20 Future research could explore the correlation between the severity of USF and clinical outcomes, stratified by operated and non-operated cases, as well as post-injury healing status. These findings may enable surgeons to plan more tailored interventions for patients with DRF and >50% USF, ultimately improving early and long-term outcomes in terms of pain relief and functional recovery.
This study has yielded important findings, yet there are avenues to further enhance its impact. The retrospective design, while providing valuable insights, also lays the groundwork for future prospective studies that could help mitigate potential biases, such as selection and recall bias. Expanding the sample size in future research could increase the statistical power, allowing for the detection of more subtle differences and improving the study's generalizability.
The follow-up period of 3 and 6 months offers crucial insights into short to medium-term outcomes after completion of rehabilitation therapy; however, extending this timeline in future investigations could shed light on long-term effects and potential complications. Although self-reported measures like DASH score and VAS offer valuable perspectives from the patients, including objective assessments like grip strength or dexterity tests could provide a more comprehensive evaluation. Additionally, incorporating qualitative tools or alternative assessments might capture a wider range of functional recovery and patient satisfaction.
The variation in surgical techniques, implants, and postoperative care within this study reflects the diversity of real-world clinical practice, potentially enhancing the relevance of the findings. Future studies could consider standardising these variables to better understand their influence on outcomes. Similarly, while factors such as patient compliance, socioeconomic status, occupation, lifestyle, and comorbidities like diabetes and osteoporosis were not accounted for in this study, including them in future research could offer more detailed insights into the healing process and overall recovery.
Conclusion
There are no statistically significant functional outcomes when comparing the operated DRFs in middle-aged patients with or without associated USF. However, further dividing the extent of the associated USF, patients with >50% USF are associated with poorer functional scores (DASH) at the 3 month and 6 months, and pain scores (VAS) at the 6 month.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.