
Abstract
Introduction
Current studies indicate that delayed soft-tissue coverage for Gustilo III open fractures of extremities is associated with higher complication rates. However, achieving the recommended time frame for coverage is often not possible, and may result in worse outcomes.
Objective
Our goal was to determine infection rates and complications of prolonged recumbency in patients with delayed coverage.
Methods
A retrospective review of patients from January 2018 to March 2023 with Gustilo IIIB and IIIC fractures of the distal tibia, ankle, and foot that underwent free flap reconstruction was performed. We excluded patients with less than 2 initial debridements, less than 6 months of follow-up, and those with locoregional flaps.
Results
18 patients were included, with a mean follow-up duration of 13.9 months. The mean time to coverage procedure was 12.9 days. 16 patients had delayed coverage performed 8 or more days from index injury, of which, only 1 developed a soft-tissue infection, and none in either group developed osteomyelitis or complications of prolonged recumbency.
Discussion
Contrary to published literature, our study showed that delayed coverage did not yield a very significant infection rate. We postulate that these lower rates may be due to: (i) multiple debridements performed (mean = 4), (ii) consultant-led debridements, (iii) the use of adjuncts including antibiotic cement beads, local vancomycin powder, and gentamicin-collagen sponge.
Introduction
The management of open fractures of the distal leg, ankle and foot pose a huge challenge even to the experienced orthopaedic surgeon. These complex injuries are frequently seen, and require timely, multidisciplinary care for management of these fractures and potential soft tissue defects. Open fractures are linked with higher complications, especially infections and non-union, and have considerable socioeconomic impact, including increased long-term cost, longer returns to employment, and overall poorer quality of life.1,2
Current studies indicate that delayed soft tissue coverage for Gustilo IIIB and IIIC open fractures of lower extremities have increased complication rates.4,5,11 There has been considerable discussion with regards to the optimal timing for soft tissue coverage in the management of these fractures, with differing views on what is considered as early coverage. 3 Godina, 4 Gopal, 5 and Sinclair et al. 6 all described the early group as having received coverage procedure within 72 h of the initial injury, while Hertel et al. divided patients into the early (immediate) and delayed (mean delay of 4.4 days) groups. Currently, the American College of Surgeons recommends to complete soft tissue coverage within 7 days of injury. 7 Despite differences in recommended timings, there was unanimous support for early coverage. However, meeting the recommended time frame for soft tissue coverage is often difficult to accomplish due to a variety of reasons. Delays in coverage may occur due to patient factors, such as the unstable polytrauma patient who is unable to withstand the long operative time required for a coverage procedure, and logistical factors, including the lack of manpower and facilities. These in turn may lead to poorer patient outcomes.
Our study aims to measure the time to free flap coverage after open fractures of the distal tibia, ankle and foot and determine if delays are associated with complications in our institution.
Materials and methods
Study population
A retrospective analysis of all consecutive patients who had open fractures of the distal tibia, ankle and foot being treated at a single institution (Khoo Teck Puat Hospital, Singapore) from January 2018 to March 2023 was performed. We included all patients with Gustilo IIIB and IIIC fractures of the distal tibia, ankle, and foot who had 2 or more debridements, and at least 6 months of follow up. At least one of the debridements was a consultant-led surgery. As free flap coverage remains the standard of care for the reconstruction of these type of injuries, 8 we only included patients who underwent a free flap reconstruction procedure, and excluded those who received locoregional flap coverage. Patients were also excluded if none of the initial debridements were performed by a consultant.
Data collection
The data analysed includes age, gender, body mass index, smoking status, co-morbidities, mechanism of injury, and Injury Severity Score (ISS). For treatment data, we measured the times to debridement, definitive fixation, and flap procedure (with the start time taken as the time of arrival in hospital), number of debridement procedures before flap coverage procedure, types of pathogen, antibiotics used, and types of antibiotic beads used.
Outcome measures
We divided the patients into 2 groups depending on the time to coverage procedure. The early group was defined as having undergone coverage procedure within 7 days of index injury, and the delayed group included those who had coverage procedure performed 8 or more days after the injury.
This was done with the aim to study two main outcomes; firstly, to establish infection rates as defined by the Centers for Disease Control and Prevention, 9 and secondly, to identify complications associated with prolonged recumbency in patients with delayed coverage, specifically looking at patients who developed deep vein thrombosis, pulmonary embolism, pressure injuries and pneumonia.
Results
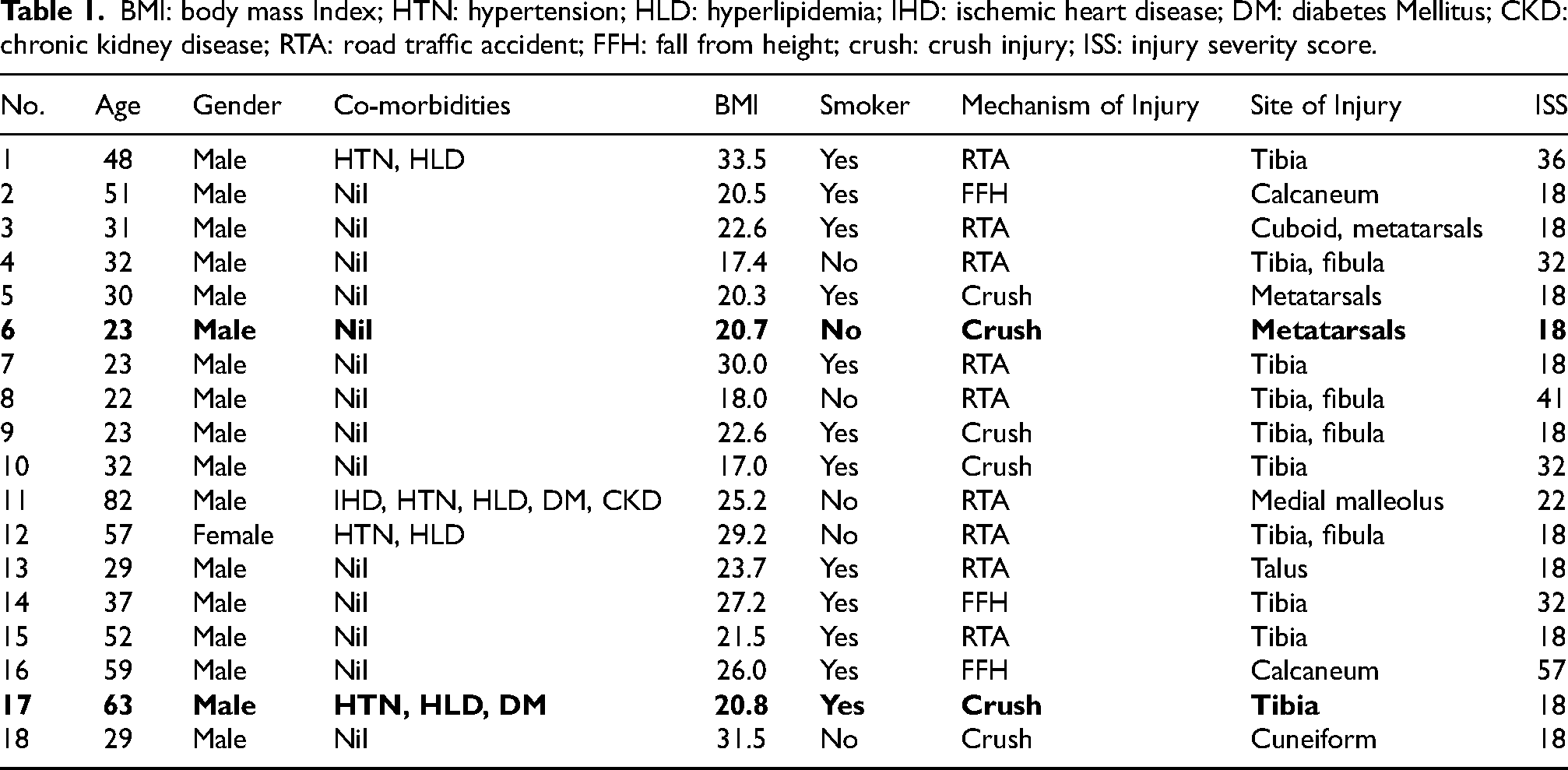
From January 2018 to March 2023, 18 patients with Gustilo IIIB and IIIC fractures of the distal lower extremity were identified to fit the inclusion and exclusion criteria. These patients had a mean follow up duration of 13.9 months, with a mean of 4.1 initial debridement procedures performed before the flap coverage procedure. Of patients evaluated, 17 were male and 1 was female, with mean age of 40.1 years (range: 22 to 82 years), and a mean BMI of 23.8 kg/m2. Of the 18 patients, 12 (67%) were identified as habitual smokers, and 4 patients (22%) had other risk factors for atherosclerotic disease, including diabetes mellitus, hypertension, and hyperlipidemia. 9 patients (50%) sustained the injuries through road traffic accidents, 6 (33%) through crush injuries, and 3 (17%) through fall from height. Sites of injury included tibia, fibula, calcaneum, cuboid, cuneiform, and metatarsals (Table 1).
BMI: body mass Index; HTN: hypertension; HLD: hyperlipidemia; IHD: ischemic heart disease; DM: diabetes Mellitus; CKD: chronic kidney disease; RTA: road traffic accident; FFH: fall from height; crush: crush injury; ISS: injury severity score.
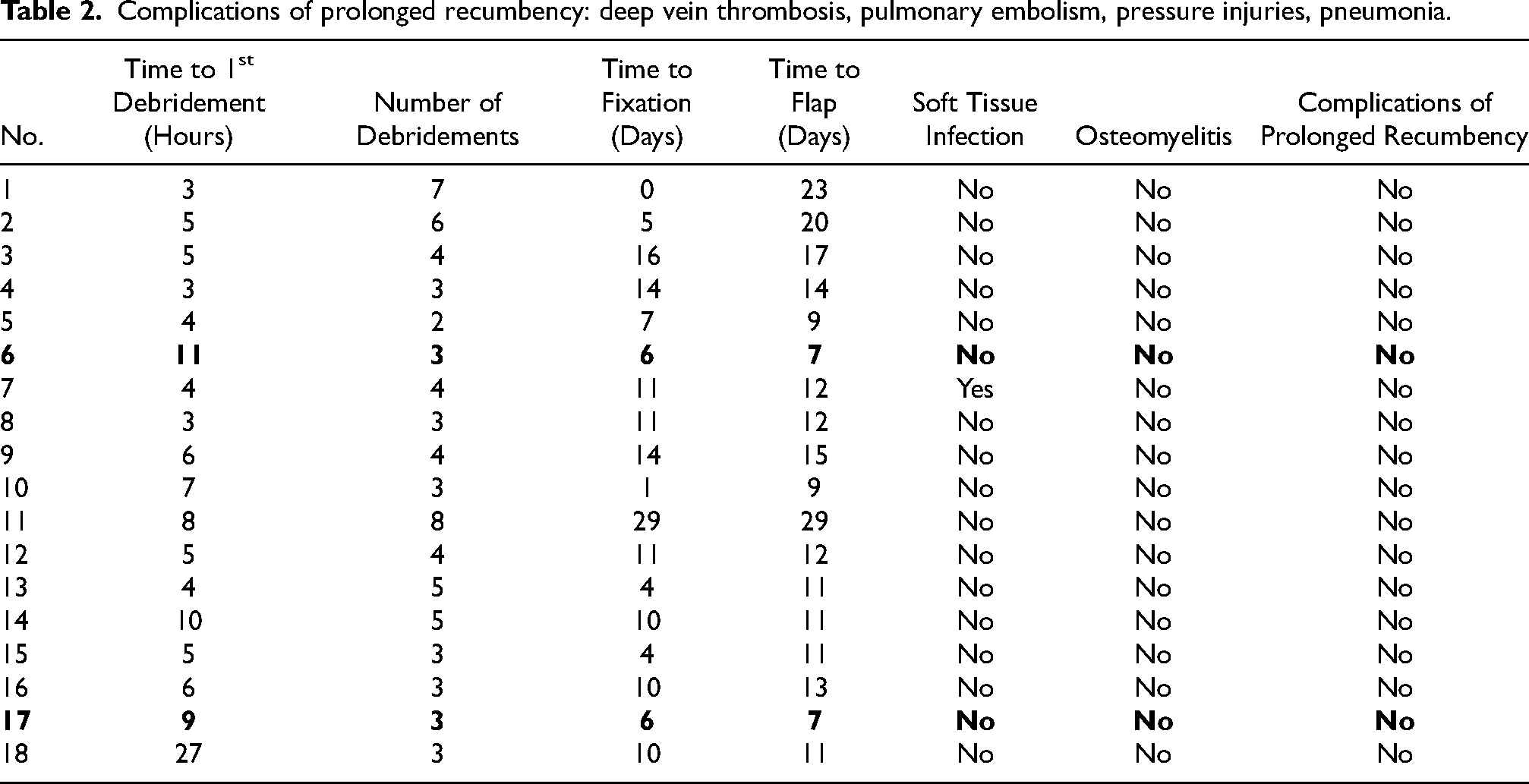
We defined the time to debridement, fixation, and free flap coverage, as the times between first presentation to our hospital and these events. The mean time to first debridement was 6.9 h (range: 3 to 27 h), while the mean time to fixation was 9.4 days (range: 0 to 29 days), and mean time to free flap coverage was 12.9 days (range: 7–29 days).
From our study, only 2 patients (11%) had coverage procedure performed within 7 days of the index injury, with the other 16 (89%) having this procedure performed 8 or more days after the injury.
Out of the 18 patients, 1 patient (6%) from the delayed coverage group developed a complication of soft tissue infection of free flap cellulitis (green discharge with surrounding erythema) 20 days after free flap coverage. This was resolved with a course of oral antibiotics. None of the patients developed osteomyelitis or complications of prolonged recumbency (Table 2).
Complications of prolonged recumbency: deep vein thrombosis, pulmonary embolism, pressure injuries, pneumonia.
All 18 patients in this study had no bacterial growth on wound cultures taken during their management. This was consistent across both early and delayed flap coverage groups.
Discussion
The optimal time for soft tissue coverage in Gustilo IIIB and IIIC injuries has remained a controversial topic, but since the introduction of the microvascular free flap by Daniel and Taylor in 1973, the practice of early flap coverage has been adopted, with the belief that this increases blood supply, promotes bone and soft tissue healing by improved vascularity and oxygen delivery to the wound. 5 D'Alleyrand et al. quoted a daily increase of 11% in risk for complication, with a 16% increase in risk for infection with delay of flap coverage beyond 7 days after injury, 10 while Pincus et al. similarly found a significant rise in complications when flap coverage was delayed beyond 7 days, with an estimated 40% increased adjusted risk with each additional week of delay. 11
Current literature focuses on the timing to coverage procedures and not on the number of debridements as a predictor of clinical outcomes in patients with open fractures. A retrospective cohort study by Sacks et al. compared the outcomes of patients with Gustilo IIIB and IIIC open tibia fractures treated at trauma centers with differing debridement practices. They concluded that patients treated at institutions prioritising early radical debridement underwent significantly lesser debridements prior to free flap coverage, and had lower rates of complications of infection and non-union compared to those treated at institutions which practiced serial debridements. This was attributed to patients receiving more radical debridements in those who underwent early debridement, whereas patients who underwent serial debridements were allowed to have non-critical hypovascular tissue (i.e., skin, subcutaneous fat) remain and declare themselves as non-viable before being excised subsequently, subjecting adjacent critical structures to infection. 12
The authors started this study as an audit to determine complications in our institution due to delays in free flap coverage after open fractures of the distal tibia, ankle and foot. The goal in sight was to improve support and resources in a logistical form such as a dedicated “fix and flap” operating theatre to facilitate early coverage in these type of injuries. The decision to only include patients who underwent free flap reconstruction and exclude those who received locoregional flaps was based on both clinical and logistical considerations. Locoregional flaps are typically less complex and shorter in operative duration, making them more feasible to perform within a shorter time frame following injury. As a result, they are often undertaken earlier, which limits their representation in a cohort assessing the impact of delayed soft tissue coverage. In contrast, free flaps are generally reserved for more extensive soft tissue defects and require greater surgical planning, coordination, and operative resources. By focusing exclusively on free flaps, we aimed to ensure a more consistent comparison of timing-related outcomes, particularly in relation to delayed coverage beyond 7 days.
Contrary to the published literature supporting early coverage, we found that delayed soft tissue coverage for open fractures of the distal lower extremity did not yield a significant infection rate in our cohort of patients. Of the 18 patients in our study, only 2 patients had a free flap performed on day 7 of injury while 16 patients had a delayed coverage, of which 1 (6%) patient had a soft tissue infection in the form of free flap cellulitis which was managed with a course of oral antibiotics. This is in contrast to the published literature where infection rates ranges between 14% 13 to 55% 10 after open fractures of distal extremities requiring free flap coverage. None of our patients had complications from prolonged recumbency.
Open tibial fractures are uniquely prone to infection due to limited soft tissue coverage, compromised local vascularity, and higher Gustilo classification. This subgroup is therefore particularly sensitive to delays in soft tissue reconstruction.. While prior studies, such as D’Alleyrand et al., have emphasized the importance of early flap coverage to reduce infection risk in tibial fractures, 10 our findings suggest that even in delayed cases, meticulous surgical technique and thorough debridement may mitigate this risk, and play a more influential role in patient outcomes than timing alone. In our subgroup of 10 patients with open tibial fractures, the majority (90%) underwent flap coverage more than 7 days after injury. Despite this delay, only 1 of the 9 patients in the delayed coverage open tibial fracture subgroup (11.1%) developed a soft tissue infection, and no cases of osteomyelitis or complications related to prolonged recumbency were observed. However, due to the small sample size and the predominance of delayed cases, further investigation with larger datasets is required to more definitively evaluate this relationship.
None of the patients in our cohort demonstrated bacterial growth on tissue cultures. This contrasts with previous studies, notably the work by Patzakis and Wilkins, who reported infection rates of up to 24% in open tibial fractures not treated with antibiotics, and 4.5% even with antibiotic use in high-grade injuries. 14 Their findings underscored the importance of timely and appropriate antimicrobial therapy in reducing infection risk. In our series, all patients received early administration of intravenous cefazolin and a single dose of gentamicin on presentation, in accordance with institutional guidelines for open fracture management. Intravenous cefazolin was continued throughout the perioperative period and maintained until 24 h after definitive free flap coverage. Following this, patients were transitioned to oral amoxicillin-clavulanate, which was continued for an additional seven days. This standardized approach may have played a key role in suppressing early microbial colonization, even in cases where flap coverage was delayed beyond 7 days. The absence of positive cultures in our study supports the growing evidence that prompt, broad-spectrum antibiotic coverage, in conjunction with surgical debridement, remains a cornerstone of infection prevention in the management of open fractures.
We analyzed our cohort and postulated several theories that could account for our findings. Wound debridement remains a pivotal part of the management of open fractures, and adequate debridement before wound coverage is crucial. It is the belief of the authors that the initial debridement procedure is equally, if not more important than the role of antibiotics and hence coining the term “debride-domycin”. The low infection rates observed in our cohort may also be attributed to the approach taken during surgical debridement. All patients underwent multiple, consultant-led debridements, allowing for a more meticulous and radical removal of devitalised tissue. Debridement was performed through generous extensions of the original wounds along fasciotomy lines to ensure full exposure and visualization of non-traumatised tissue. This approach included the excision of loose or non-bleeding bone fragments, devitalised or contused soft tissue, subcutaneous fat, and skin that appeared thinned or compromised – rather than adopting a more conservative strategy of waiting for tissue demarcation. The wounds were irrigated with 9 litres of normal saline and 1 litre of chlorhexidine solution. Such proactive and thorough debridement may have played a significant role in minimizing bacterial burden and improving outcomes. The authors also frequently incorporated adjuncts during debridement procedures, inserting antibiotics impregnated cement beads with local vancomycin powder, application of Gentamicin-Collagen Sponge (Collatamp®G) with the goal of delivering therapeutic levels of antimicrobials locally to the open fracture site.
We do acknowledge the limitations of this study which include the retrospective design, small patient pool from a single center and imbalance in numbers between the early and delayed cohorts of patients that may have been underpowered to detect significant differences in outcomes. Details regarding confounding factors, such as diabetes mellitus control which may have caused increased infection rates, were not evaluated. Ideally, we would like to conduct a prospective study powered adequately to obtain statistically significant results to assess causality. With regards to surgeon performance bias, we mitigated this by having the same group of Orthopaedics and Plastic surgeons perform the debridement and fixation surgeries and coverage procedures respectively.
Conclusion
While the general consensus is still for early coverage in the management of open fractures of the distal lower extremity, more literature has emerged proposing that delayed coverage does not result in worse outcomes, with no significant differences in flap failure,15,16 osteomyelitis, or union. 17 Our study similarly suggests that perhaps time to coverage does not play such a significant role in outcomes, and management should be tailored to the individual patient, with emphasis placed on the quality of debridements and use of appropriate adjuncts.
Footnotes
Data availability statement
The corresponding author has full control of all primary data and this is available for review upon request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was determined not to be required by the NHG Domain Specific Review Board (Reference: 2024–3090).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.