
Abstract
Purpose
To compare the long-term oncological outcome of neoadjuvant bisphosphonates and denosumab in extremity giant cell tumor of bone (GCTB) with curettage.
Methods
Fifty-five patients were retrospectively reviewed from 2003 to 2023. All patients underwent curettage and cementation and received three doses of postoperative zoledronate. They received either preoperative zoledronate (n = 41) or denosumab (n = 14). Both groups’ local recurrence (LR) rate and LR-free survival were calculated.
Results
The mean follow-up time for the zoledronate and denosumab group were 10.7 and 5.1 years, respectively (p = 0.006). The LR rate in the denosumab group (57%) was significantly higher than the zoledronate group (27%), p = 0.039. The zoledronate group had significantly greater LR-free survival than the denosumab group (p = 0.020). There was no correlation between the number of upfront denosumab doses and local recurrence (p = 0.573).
Conclusion
Upfront zoledronate showed a higher LR-free survival for extremity GCTB with curettage at a mean follow up of 9.3 years.
Introduction
Giant cell tumor of bone (GCTB) is an intermediate-grade and locally aggressive bone tumor that usually involves the metaphyseal-epiphyseal region of the long bones. Intralesional curettage and local adjuvants can achieve local disease control while preserving the limb functions, causing fewer disability than en-bloc resection. However, local recurrence (LR) can be problematic with this treatment modality, with a wide range LR rate of 10% to 50%.1–3 Hence, antiresorptive medications such as zoledronate and denosumab are used as adjuvants to tackle LR.
Bisphosphonates were shown to induce apoptosis in neoplastic GCTB stromal cells with a dose-dependent antitumor effect in in-vitro studies. 4 Among all the tested bisphosphonates, zoledronate was the most potent. 4 With a mean follow up of 48 months in a case-control study, adjuvant bisphosphonates was shown to reduce LR in GCTB patients treated with curettage. 5 Recently, a meta-analysis of 13 studies showed that using zoledronate following curettage of GCTB could reduce LR rate. 6
Denosumab is a fully human monoclonal antibody that inhibits RANK ligand and prevents the RANK-RANK ligand interaction and subsequent bone destruction. In basic studies, denosumab exhibited potent antiosteoclastic effects since RANK ligands were overexpressed in GCTB stromal cells. However, it has no antitumor effect on GCTB stromal cells in contrast to zoledronate.7,8 Clinically, it is agreeable to use denosumab in GCTB with resection and inoperable GCTB, yet the use of denosumab in GCTB with curettage is controversial. Denosumab has been proposed as an effective agent in surgical downstaging for GCTB patients, decreases tumor vascularity, 9 and reduces bone tumor-related pain in phase 2 study. 10 The United State Food and Drug Administration has approved the use of denosumab for treating adults with GCTB in 2013. On the contrary, there are also reported cases with increased local recurrence risk in GCTB patients with curettage post neoadjuvant denosumab.11,12
Studies comparing the neoadjuvant use of zoledronate and denosumab in GCTB patients with curettage were limited. One retrospective study with a 2-year follow up showed no difference in clinical outcome between the 2 groups. 13 This study aimed to compare the long-term outcome of neoadjuvant zoledronate and denosumab in extremity GCTB) with curettage. We hypothesized that both groups had comparable LR rates in the long-term follow up.
Methods
Inclusion/exclusion criteria and follow-up regime
The study was conducted according to the ethical standards of our institution's clinical research ethics committee (CRE Ref. No. 2024.227).
From 2003 to 2023, 55 patients with extremity GCTB diagnosed histologically by computed tomography (CT) guided biopsy were included (Figure 1). They underwent surgical curettage and bone cementation. Patients received either preoperative zoledronate (n = 41) or denosumab (n = 14), and all of them (n = 55) received three doses of zoledronate postoperatively (Table 1). We have excluded the axial skeleton (spine and pelvis) GCTB cases, cases with bone grafting to the curetted cavity, cases that underwent wide resection, and cases with less than a 2-year follow up.
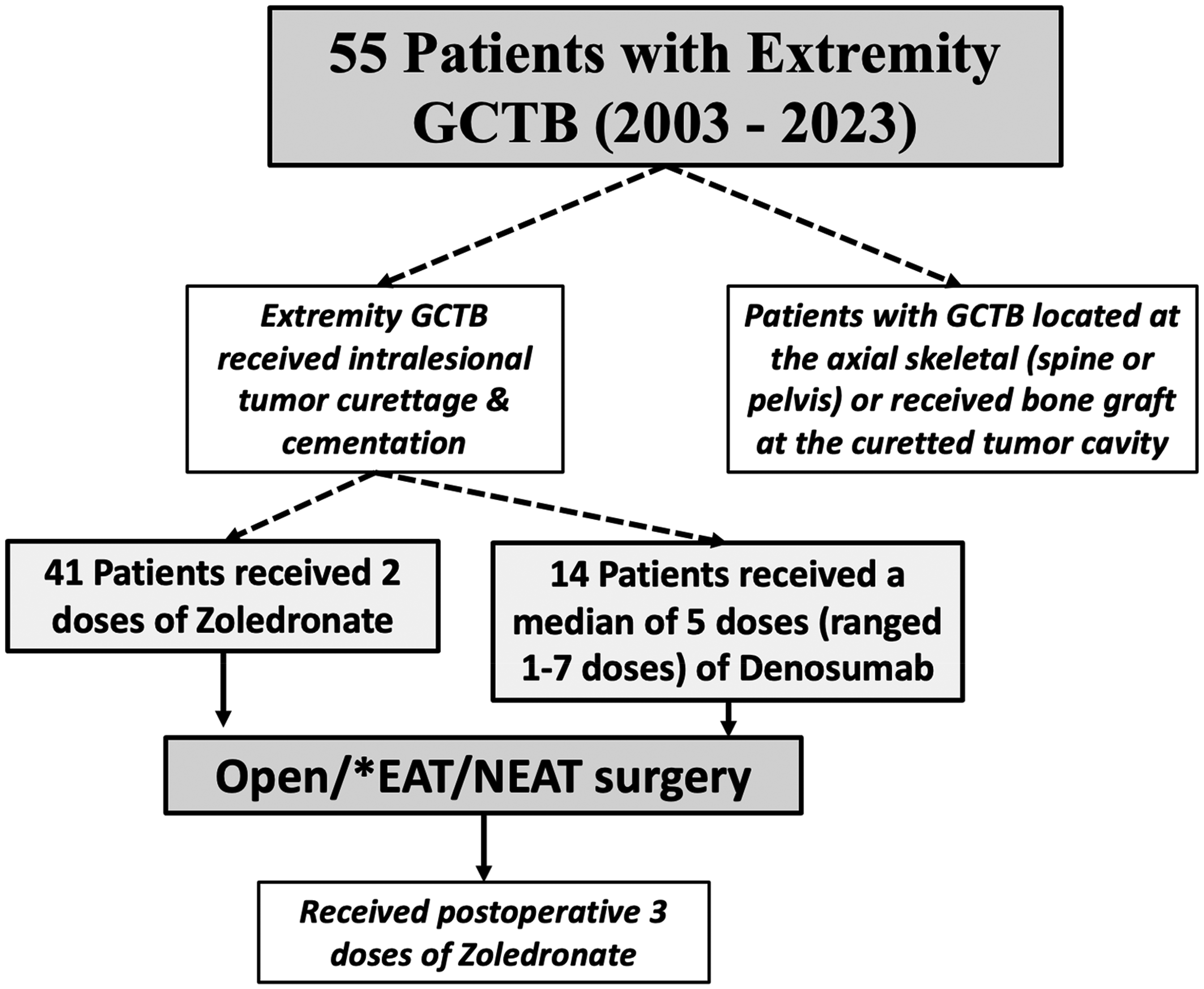
The GCTB patient selection, and the treatment they received in the study. GCTB: giant cell tumor of bone.
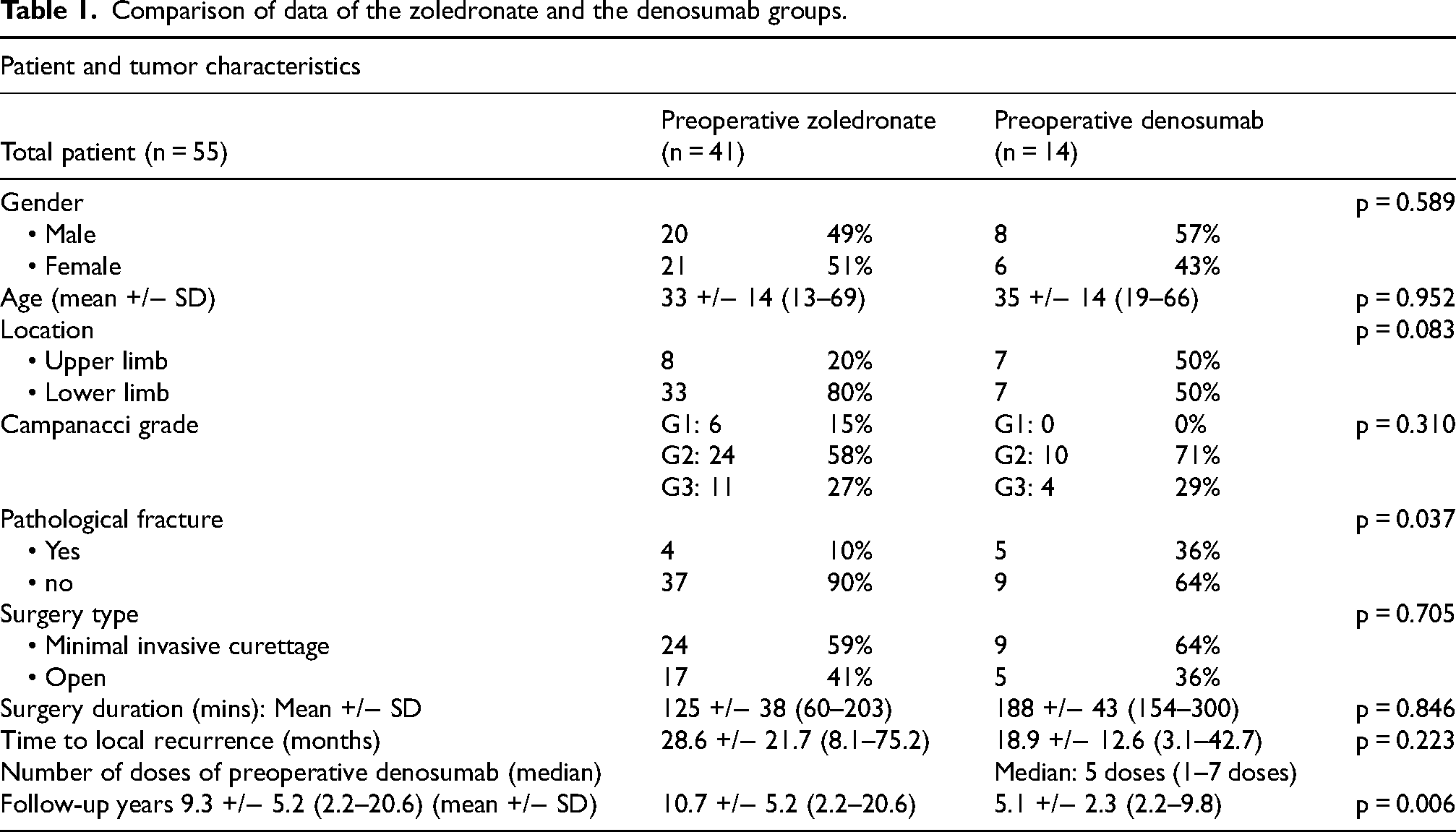
Comparison of data of the zoledronate and the denosumab groups.
All patients followed our standard protocol: at the time of the first postoperative zoledronate infusion and postoperation, 1 month, 2 months, then every 3 months for 2 years, every 6 months until 5 years, and then annually. Radiological assessment using plain radiographs and clinical evaluation were performed at each follow up (Figure 2a to f). We recorded parameters such as LR, surgical complications, and adverse drug reactions.
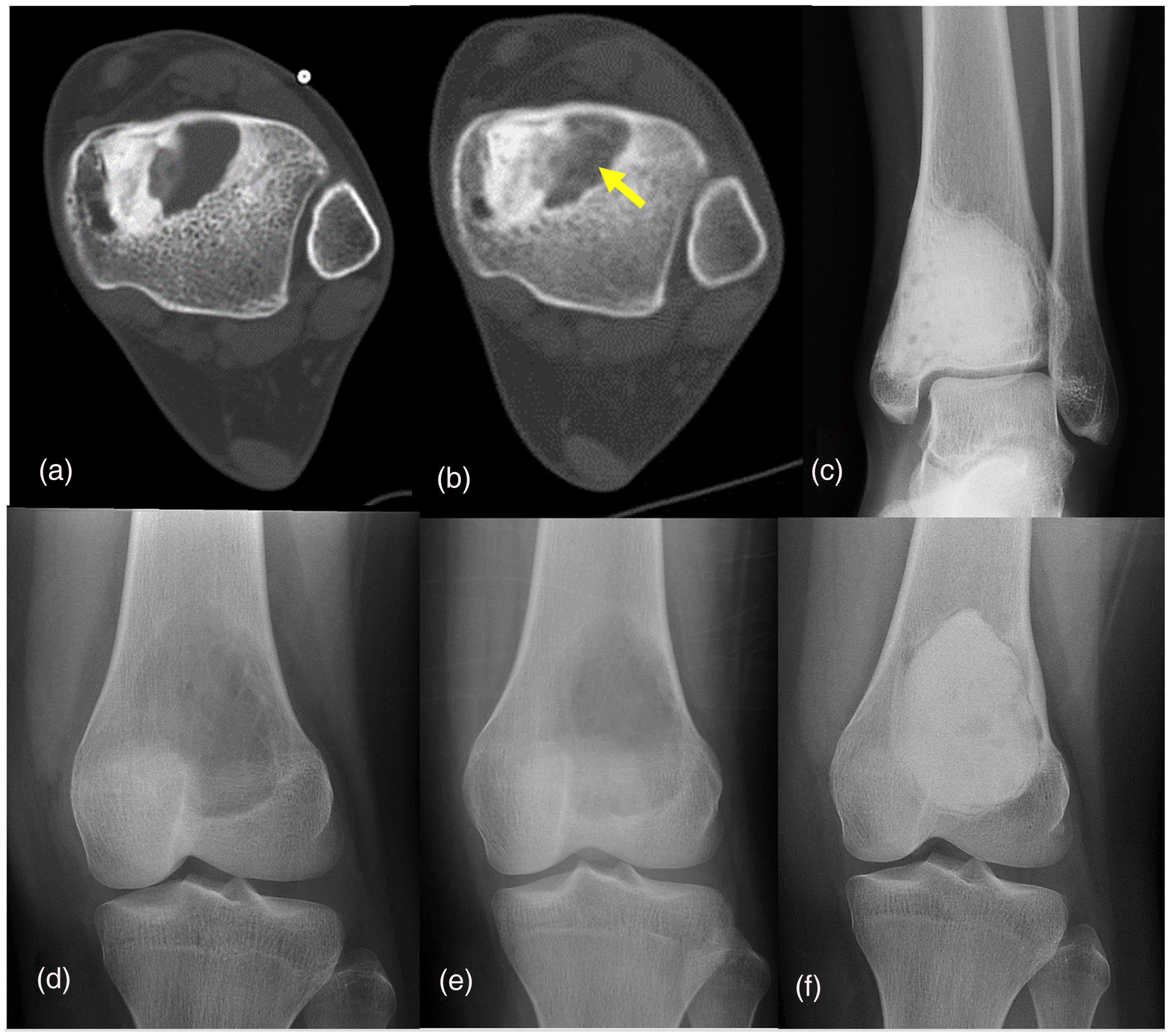
A 35-year-old lady had recurrent GCTB of the left distal tibia in 2017. Three-month denosumab was given preoperatively. Axial views of the CT image showed tumor recurrence, adjacent to the cement, before denosumab (a) and increased calcification (yellow arrow) of the tumor recurrence after denosumab (b). The plain radiograph of her ankle (c) in 2024 showed cement at the distal tibia without recurrence. A 15-year-old girl had left distal femur GCTB in 2019. One dose of zoledronate was given instead of denosumab due to her young paediatric age. The plain radiograph of the left knee showed a lytic metaphyseal lesion before zoledronate (d) and after zoledronate (e). The plain radiograph of the left knee in 2021 (f) showed a new lytic area adjacent to the cement at the lateral femoral condyle, she later underwent another currettage and cementation. CT: computed tomography; GCTB: giant cell tumor of bone.
Antiresorptive medications
Patients were admitted to the hospital on the day of drug administration to monitor and observe for any immediate adverse effects of the perioperative antiresorptive agents.
Preoperatively, the denosumab group received 1 to 7 doses of subcutaneous Denosumab of 120mg, which were given on days 1, 8, and 15 and then once monthly. On the other hand, the zoledronate patient group received 2 doses of preoperative intravenous zoledronate infusion, 1 month apart (4mg in 100mL normal saline over 15 minutes). In both groups, patients would then proceed to surgical curettage within 4 weeks.
Both groups received three doses of zoledronate postoperatively. The first dose was given after reviewing the wound on postoperation day 3. Then, the patients were given zoledronate once monthly for two more doses. Patients were also given calcium 1000 mg and vitamin D3 800IU supplements during the perioperative period.
Surgical curettage
All patients included received either open or endoscopic-assisted tumor (EAT) curettage. EAT curettage has been used since 2008 as it minimizes surgical trauma and allows direct and magnified endoscopic visualization of the curetted cavity in contrast to the open technique under the naked eye. 14 Better visualization facilitates complete tumor removal and avoids excessive curettage that may risk cartilage damage or fracture 15 (Figure 3). CT navigation assistance with image feedback was added to all EAT curettages for better tumor clearance in the bone cavity during curettage in the first three cases. In the later part of the study, to minimize the operative time spent on the navigation setup, the navigation was restricted to those cases with internal calcified septae initially presented in the GCTB or formed after denosumab treatment.
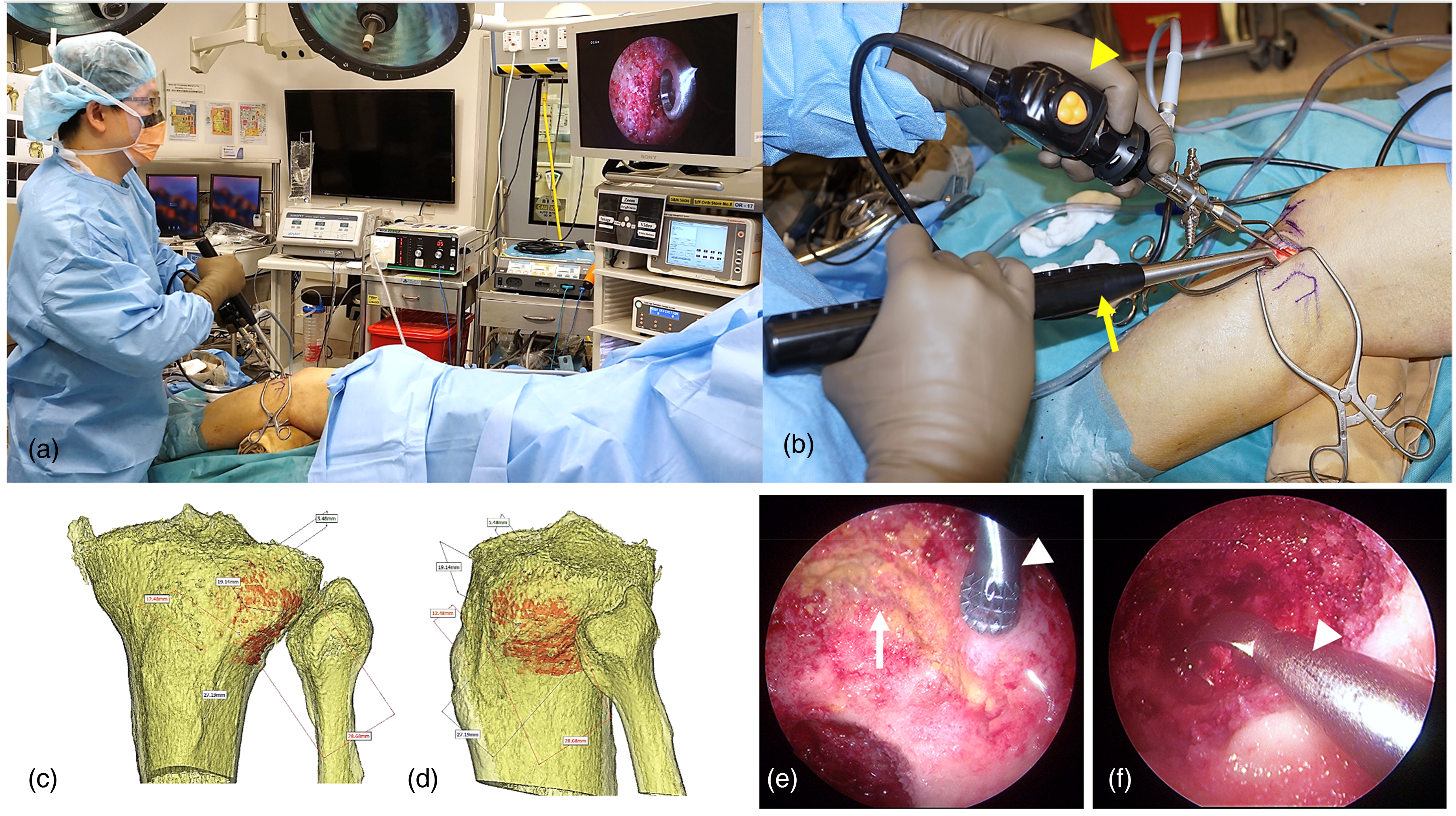
(a) The intraoperative setup for a 65-year-old man with left proximal tibia GCTB who underwent EAT curettage. (b) A 4.5 mm knee arthroscope (yellow arrowhead) was used to visualize the curetted bone cavity, while a bone curette (yellow arrow) was used to clear the tumor. The anterior (c) and lateral views (d) of the three-dimensional bone tumor models aid the surgical planning of the cortical window location and size, facilitate tumor curettage. (e) The arthroscopic view shows the yellowish tumor (white arrow), and an ultrasonic bone curette (white arrowhead) was used for tumor removal. (f) The arthroscope view shows a bone curette (white arrowhead) removing the tumor. EAT: endoscopic-assisted tumor; GCTB: giant cell tumor of bone.
Preoperative CT images of the affected areas were acquired at the same setting before CT image-guided biopsy. Axial images with 0.625 mm thickness slices were used for preoperative three-dimensional (3D) surgical planning. For navigation cases, the CT images in Digital Imaging and Communications in Medicine (DICOM) format were imported into the navigation system, where the sites of cortical bone windows were planned for the surgical access of intralesional curettage and removal of internal septae. Between 2008 and 2010, the CT-based navigation system (Spine, version 2.0.1, VectorVision, Brainlab, Feldkirchen, Germany) was used with the image-to-patient registration by the CT-fluoroscopy matching method. Another navigation system (OrthoMap 3D module, version 2.0, Stryker, Mahwah, New Jersey) was adopted after 2011 as it allows more accurate registration with intraoperative 3D image acquisition (Figure 4a).
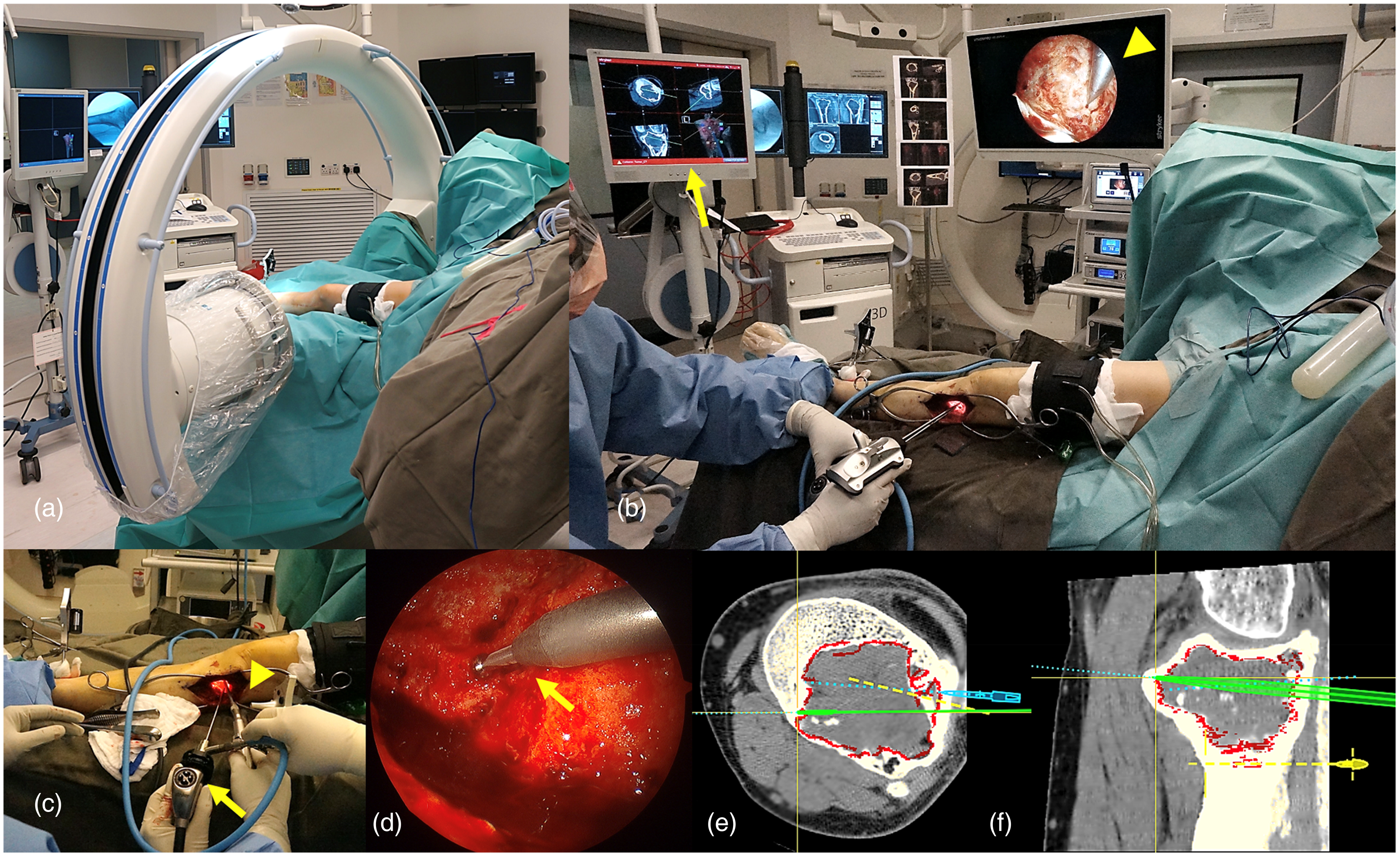
(a) The intraoperative 3D CT images that were acquired for a 55-year-old man with the left proximal tibia recurrent GCTB who underwent NEAT curettage. (b) The registered intraoperative 3D CT images were fused with the preoperative planning CT image datasets. The suitable skin incision and the cortical window were made under navigation guidance. The tumor was then curetted under direct vision of a 4.5 mm knee arthroscope (yellow arrowhead). At the same time, the exact location of the curetted tumor cavity was determined under navigation image feedback (yellow arrow). (c) The knee arthroscope (yellow arrow) and navigated bone burr (yellow arrowhead) in NEAT curettage. (d) The arthroscopic view of the tumor cavity and the navigated bone burr (yellow arrow). The navigation display shows the axial (e) and sagittal (f) views of the CT images of the proximal tibia GCTB with the tip of the navigation pointer (green) checking the clearance of tumor curettage. 3D: three-dimensional; EAT: endoscopic-assisted tumor; GCTB: giant cell tumor of bone; NEAT: navigation endoscopic-assisted tumor.
The skin was incised along the site of the planned cortical bone window. We initially utilized the two-portal technique in 2008, then refined it to the one-portal technique in 2009, allowing higher flexibility in manipulating the instruments. During burring, the tourniquet was inflated to reduce bone bleeding, allowing better visualization of surgical field and minimizing the risk of incomplete curettage. The core of the tumor was first removed with curettes. A dry 4mm 30-degree arthroscope was then inserted into the bone cavity. Under a magnified endoscopic visualization, any visible residual tumor was further removed with a high-speed bone burr. CT navigation was used to guide the removal of the bony septae and confirm the edge of the tumor border (Figure 4). After removing the GCTB, we filled the cavity with bone cement, using the cement gun with pressurization technique when possible. Postoperatively, patients were allowed immediate full range of joint movement, and full weight-bearing walking in lower limb cases.
Statistical analysis
The primary outcomes were the LR rate and LR-free survival of the zoledronate and denosumab groups. Secondary outcomes were the correlation between denosumab dosages and LR risk and potential predictor factors on LR risk. Statistical analysis was performed using SPSS version 24. The zoledronate and denosumab group results were compared by chi-square test, fisher's exact test, and the t-test. Kaplan–Meier survival analysis was calculated for the LR-free survival for both groups. The correlation of the denosumab dose and LR risk was assessed by the nonparametric test. Multivariable Cox regression was used to calculate the hazard ratio of LR on various patient, disease, and treatment factors. p < 0.05 was considered statistically significant.
Results
General data
Fifty-five extremity GCTB patients who underwent intralesional tumor curettage were included in the study (Table 1). The mean follow-up time was 9.3 years (2.2–20.6). And 61.8% of patients had Campanacci grade 2 GCTB, while 27.3% were grade 3. Nine patients (16.4%) suffered from pathological fractures at presentation. And 74.5% (n = 41) received upfront zoledronate, while 25.5% received upfront denosumab. Minimal invasive surgery (EAT curettage) and open curettage were performed in 60% and 40% of patients respectively. Overall, the local recurrence rate was 34.5% (19 out of 55 patients) in the study.
Upfront zoledronate versus denosumab
Further data were compared according to the type of preoperative antiresorptive agents used, either upfront zoledronate or denosumab (Table 1). The demographic data of the zoledronate group and denosumab group were comparable (p > 0.05) in terms of gender, age, tumor location, Campanacci grade of GCTB, types of surgical curettage, surgical duration, and the time to LR. Pathological fracture was more commonly found in the denosumab group (p = 0.037). The mean follow-up period in the zoledronate group (10.7 +/− 5.2 years) was statistically longer (p = 0.006) than that of the denosumab group (5.1 +/− 2.3 years).
The local recurrence rate in the denosumab group was 57.1%, which was significantly higher (p = 0.039) than that in the zoledronate group (26.8%) (Table 2). Nevertheless, the LR-free estimate in 10-year in the zoledronate group was significantly greater than that in the denosumab group (73.2% vs 42.9%, p = 0.020, Figure 5).
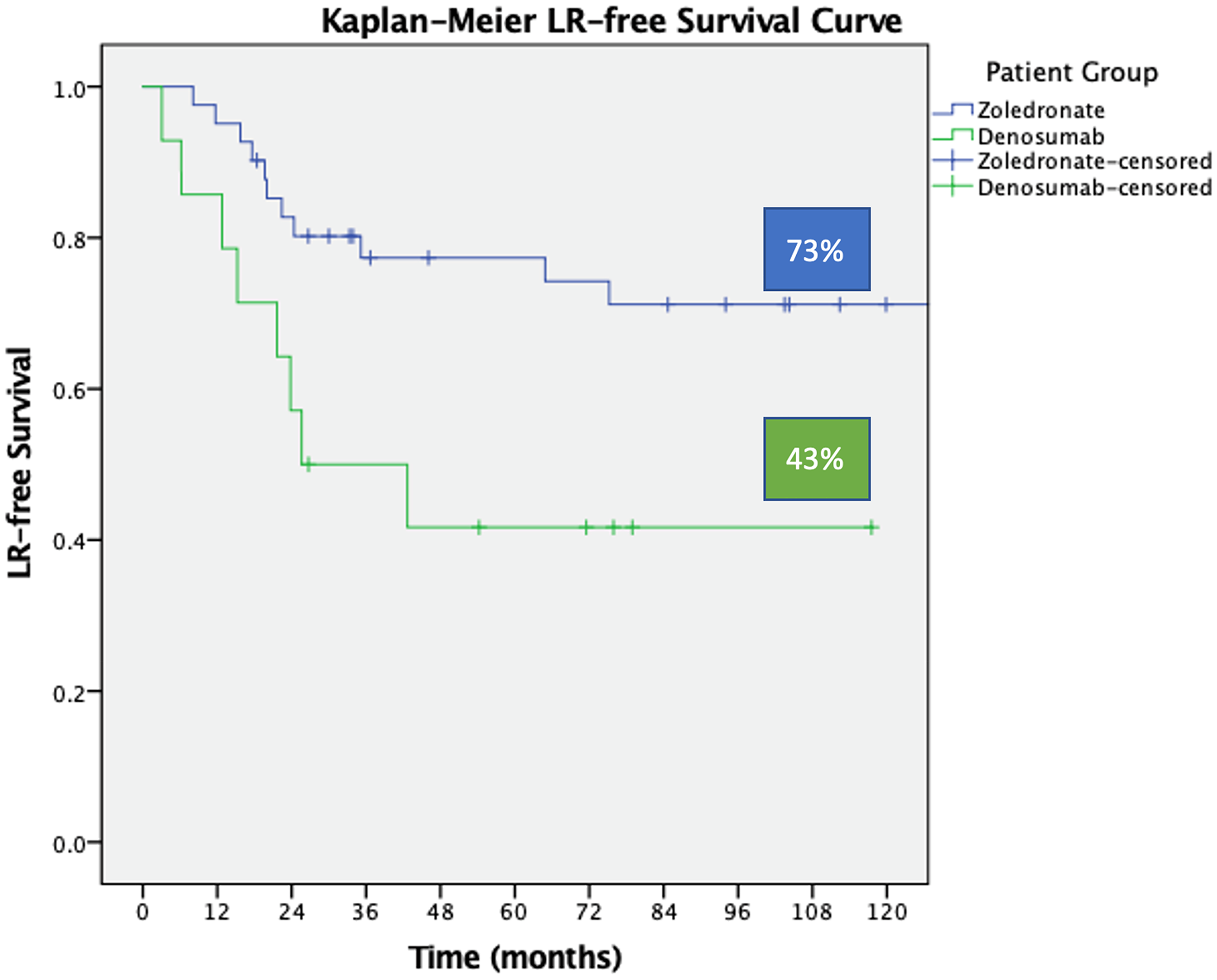
The tumor local recurrence-free survival curve in the preoperative zoledronate and denosumab groups. Patients of the zoledronate group had higher local-recurrence-free survival in 10 years, 73% versus 43%, p = 0.020 (log rank test).
Local recurrence rate in the zoledronate and the denosumab groups.

In the denosumab group, patients received upfront medications varying from one to seven doses, with a median of five doses. There was no correlation between the number of upfront denosumab doses and local recurrence (p = 0.573). Only one patient presented with skin rashes after denosumab administration, which subsided spontaneously. No adverse events, such as jaw osteonecrosis, atypical femoral fracture, electrolyte disturbances, pulmonary metastasis, nor sarcomatous change, were observed in both groups.
Hazard ratio of various patient, disease, and treatment factors
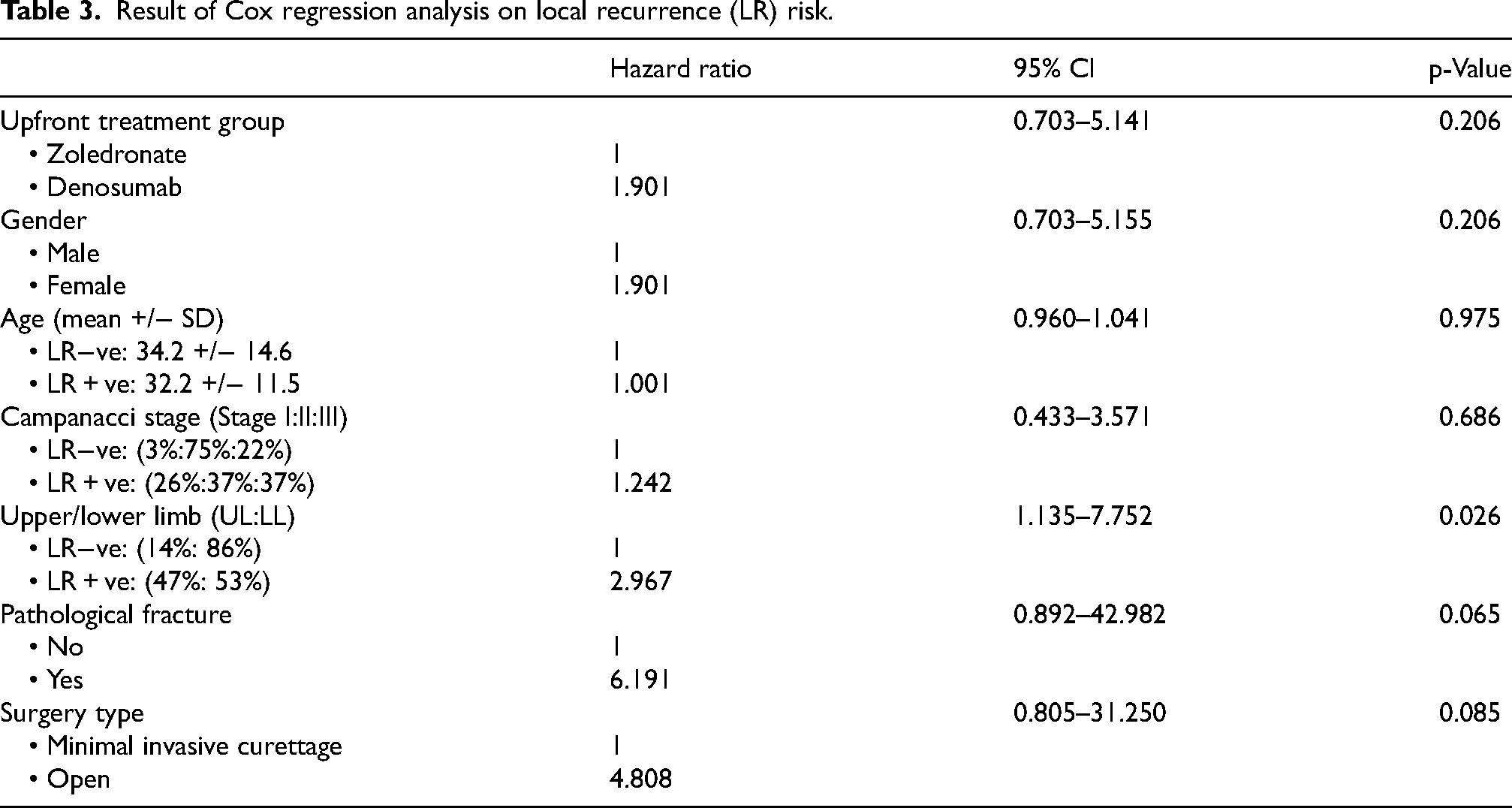
With multivariable analysis using the Cox proportional hazards model (Table 3), only upper limb tumor (p = 0.026) was a statistically significant predictor of LR, with adjusted hazard ratios of 3.0 (95% confidence interval (CI) 1.1–7.8).
Result of Cox regression analysis on local recurrence (LR) risk.
Discussion
Treating extremity GCTB should ensure adequate local tumor control, while maintaining the limb function. Intralesional curettage has been established as the preferred treatment method for GCTB 16 ; however, LR has remained as a concern. Antiresorptive agents, like zoledronate and denosumab, have been used, in an attempt to reduce LR in GCTB patients treated with intralesional tumor curettage. 16 However, there is scarce evidence to compare the use of the zoledronate and denosumab in an upfront setting in GCTB with curettage. This study is the first in our locality to compare the long-term outcomes of two groups with a mean follow up of 9.3 years.
In this study, the LR rate of the denosumab group was significantly higher than that of the zoledronate group (57% vs 27%, p = 0.039). This finding concurred with the current literature.
There are high-level evidences from literatures to support the use of zoledronate in lowering the LR of GCTB.6,17 Conversely, despite of the two large phase 2 studies published in 2010 and 2013 supporting the use of upfront denosumab,10,18 recent systemic reviews showed increased LR rate postadministration of upfront denosumab.19,20 The use of upfront denosumab in tackling the LR of GCTB has remained questionable. Firstly, this could be related to the increased bone sclerosis and consolidation after neoadjuvant denosumab. Therefore, it masks the bone-tumor margin, increasing the difficulty to achieving a complete curettage (Figure 6). Secondly, the remaining tumor could also be re-activated after the cessation of the denosumab. Thirdly, denosumab lacks of antitumor effect on GCTB neoplastic stromal cell, and only allows suppression of osteoclast activity.7,8

(a) The fleshy brownish soft tumor tissue from a GCTB patient treated with one dose of zolendronate. (b) A mixed fleshy and fibrotic tumor tissue from a GCTB patient treated with one dose of denosumab. (c) Whitish fibrotic tumor tissue from a GCTB patient treated after four doses of denosumab. GCTB: giant cell tumor of bone.
The LR rate of the denosumab group was high (57%) in our study. This finding echoes with other 5 existing publications (Table 4),11,13,21–23 with their LR rate ranging from 25% to 60%. Among all studies, our study has the longest follow-up time with a mean follow up of 61.2 months. It is understandable that more cases with pathological fracture were included in the denosumab group in our study (p = 0.037), as surgeons would like to restore the bone stock and downstage the surgery from resection to intralesional curettage with the use of upfront denosumab.
Comparison of our study to other studies (preoperative denosumab with curettage in GCTB).
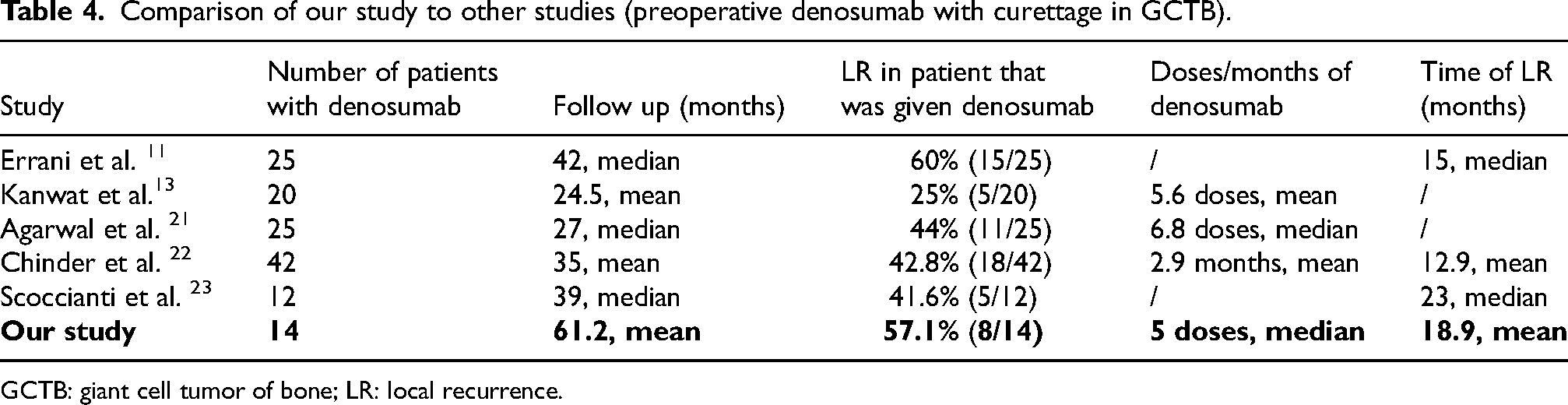
GCTB: giant cell tumor of bone; LR: local recurrence.
The number of upfront denosumab doses ranged from one to seven, with a median of five doses in our study. No correlation was found between the preoperative denosumab duration and local recurrence (p = 0.573). This coincides with the findings of a recent systemic review in 2020. 19 Up-to-date, there is no consensus reached with regards to the appropriate preoperative denosumab dosage, prior to curettage. One single-centre retrospective study 24 showed that a short course (≤3 doses) was associated with no difference in LR-free survivorship and clinical score compared with a longer-course (>3 doses). Other studies25,26 suggested a shorter duration of upfront denosumab treatment. A maximum of 3 to 4 months course was considered an optimal duration, for forming the cortical rim surrounding the bone tumor and the soft tissue component.
The LR rate of the zoledronate group in our study was 27%, which was greater than that without the use of zoledronate, comparing to Niu et al. findings. The reported LR rate after extensive curettage was only 8.6% in his series of 621 Chinese patients. 27 The variability of the extent of surgical curettage could possibly explain the difference of the LR rates. In our study, approximately 60% of our patients underwent EAT, which was a less extensive approach with higher bone and functional preservation.
Among all the various patient, disease, and treatment factors, only upper limb tumor (p = 0.026) was a statistically significant predictor of LR, with adjusted hazard ratios of 3.0 (95%CI 1.1–7.8). Lan et al. found that the LR rate in upper extremity GCTB with intralesional curettage was 48% in a retrospective series of eight two patients. 28 McCarthy et al. suggested using a short course of preoperative denosumab therapy to distal forearm GCTB, which responded well to medication and could possibly facilitate limb salvage surgery. 29 However, a recent systemic review demonstrated no significant difference in aggressiveness between the upper and lower extremities. 30
We have started using upfront zoledronate and denosumab in GCTB patient with curettage since 2004 and 2014 respectively in our institution. The cost of a single dose of zoledronate is approximately HKD 60, and that of denosumab is around HKD 4000. In this study, the LR-free survivorship in the zoledronate group is significantly higher than the denosumab group (p = 0.020). Especially with the higher cost and potentially higher LR of denosumab, apart from the drugs clincail profile, we should consider its economical efficiency when prescribing. It should be used cautiously and only for a short duration. In our opinion, denosumab should be reserved for patients with severe bone pain, pathological fracture, and bulky tumor with large extraosseous soft tissue component that surgical downstaging (i.e. curettage) was considered feasible and appropriate. Patients should be counseled for the probable risk and is allowed to share the decision making of their management. In our opinion, curettage of distal radius GCTB poses a surgical challenge. Complete tumor removal is difficult due to the bone geometry of the distal radius and the close proximity of the tumor to the wrist joint and subchondral bone.
Limitation
There are several limitations in our study. Firstly, this was a retrospective study with data obtained from electronic medical records, possessing possible risk of selection bias. Secondly, the study population was relatively small, with only 55 patients included. Nonetheless, strict inclusion criteria were employed to minimize co-founding factors and heterogeneity. Only patients with primary extremity GCTB treated with intralesional curettage, bone cement, and postoperative zoledronate were included. They received either preoperative zoledronate or denosumab. Only patients with more than 2-year follow-ups were included. Thirdly, the medication treatment for GCTB has been evolving, and denosumab has only been commenced in our institution since 2014. Therefore, comparing the two drugs, the follow-up period of the zoledronate group is longer than that in the denosumab group (10.7 vs 5.1 years, p = 0.006). Considering that most of the LR takes place early, at 2 to 3 years after surgical curettage, the comparison of LR-free survival in both groups is unlikely to be affected. Fourthly, the two groups shares similar patient demographics and tumor characteristics. However, some heterogeneity is unavoidable, such as the differences in pathological fracture in both groups (p = 0.037).
Conclusion
In a long-term follow up of 9.3 years, neoadjuvant zoledronate had a significantly greater LR-free survival than neoadjuvant denosumab in extremity GCTB with curettage. Given the high LR rate, neoadjuvant denosumab should only be used with caution in selected cases. Further studies are warranted to look for the optimal duration of neoadjuvant denosumab prior to GCTB curettage.
Footnotes
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee (Joint CUHK-NTEC CREC) (CRE-2024.227).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was approved to be waived by the Joint CUHK-NTEC CREC.