
Abstract
Recent studies suggest that removing post-total hip arthroplasty precautions may not increase dislocation risk but can improve functionality and reduce costs. Unclear guidance on individual precautions necessitates clearer recommendations based on current clinical evidence. A systematic search of PubMed, EMBASE, and Cochrane Library until May 2024 was conducted using PRISMA extension guidelines for scoping reviews. Specific terms related to total hip arthroplasty, dislocation, and hip precautions were searched. Two reviewers independently screened the title and abstract for eligibility, and one reviewer reviewed the full texts—the Oxford Centre for Evidence-Based Medicine Levels of Evidence assessed publication quality. Upon evaluation of individual hip precaution modalities, most studies indicate that many hip precautions can be omitted without compromising dislocation risk. Specific recommendations for each precaution were based on at least one piece of level 2 evidence. Limited evidence exists on the use of dressing aids and on resuming sexual activities postoperation.
Introduction
Although mild cases of dislocation can often be resolved with closed reduction, severe cases may require revision surgery, which can be problematic. Being the second most common complication following total hip arthroplasty (THA), data showed that approximately one-third of post-THA dislocation will require surgical treatment and 20% of all prosthetic revision surgeries are performed due to dislocations. 1
Despite the prevalence of these complications, hip precautions have traditionally been prescribed post-THA to mitigate the risk of dislocation. 2 The surgical approach, particularly the posterior (posterolateral) approach has been reported to be the most commonly performed approach chosen by surgeons. 3 Nevertheless, the posterior (posterolateral) approach has been claimed to be associated with a higher risk of dislocation, with a higher demand for hip precautions. 2
Advancements in implant technology and the introduction of robotic-assisted systems have greatly improved implant survivorship and reduced dislocation risks in THA. Hence, some argued that hip precautions are no longer necessary. Restrepo et al. 4 concluded that a no-restriction protocol in the anterior approach did not increase early dislocation incidence.
Growing evidence has indicated that minimal precaution or no precaution for THA patients may not increase the dislocation risk. Previous systematic reviews have questioned the necessity of prescribing strict hip precautions post-THA, unveiling that postsurgical protocols with minimal postoperative restrictions may lead to improved hip function, reduced healthcare costs and less demand on clinical staff.2,5–9 Notably, three reviews set strict eligibility criteria to only include evidence from a posterior approach,2,6,7 and two reviews assessed the certainty of the evidence.2,9
However, the current systematic reviews did not provide clear guidelines regarding the advisability of individual precautions, the format in which they should be prescribed, or their duration. This ambiguity leaves open questions about how patients can effectively reduce the burden of standard precautions and resume daily activities more quickly without substantially increasing the risk of dislocation. This paper aims to summarize and offer specific recommendations for each precaution, grounded in the existing clinical evidence.
Methods and materials
Information sources and search strategy
The review was conducted with the PRISMA extension guideline for scoping reviews. PubMed, EMBASE and Cochrane Library were searched from the start date to May 2024. Appropriate search terms focusing on the “total hip arthroplasty,” “dislocation,” and different modalities of hip precautions (i.e. “abduction pillow,” “movement restrictions,” “sleep position restriction,” etc.) were applied and combined with the AND operator. MeSH terms for “arthroplasty, replacement, hip” and “hip dislocation” were utilized.
Eligibility criteria and study selection
We included studies with patients after the primary posterior approach THA, while excluding those studies with anterior approach patients involved. All diagnoses were included. The selected studies were required to address at least one of the hip precautions protocols relevant to our investigation. Studies lacking reports on dislocation post-THA were omitted. Due to limited level 1 evidence, all published clinical study designs were included including systematic reviews, randomized control trials (RCTs), retrospective cohort and case-control studies. Additionally, in vitro, CT-based or three-dimensional (3D) simulation trials were also included. Only English publications were considered for inclusion.
Two reviewers (AC and BL) independently screened the title and abstract for eligibility, consensus was reached by discussion in case of uncertainty. Next, full-text manuscripts of all initially selected studies were reviewed and the key clinical recommendations regarding particular hip precaution modalities were extracted by one reviewer (AC). Our searches identified 383 unique references, of which 62 were screened in full text. Of these, 42 were excluded, leaving 20 for inclusion (Figure 1).
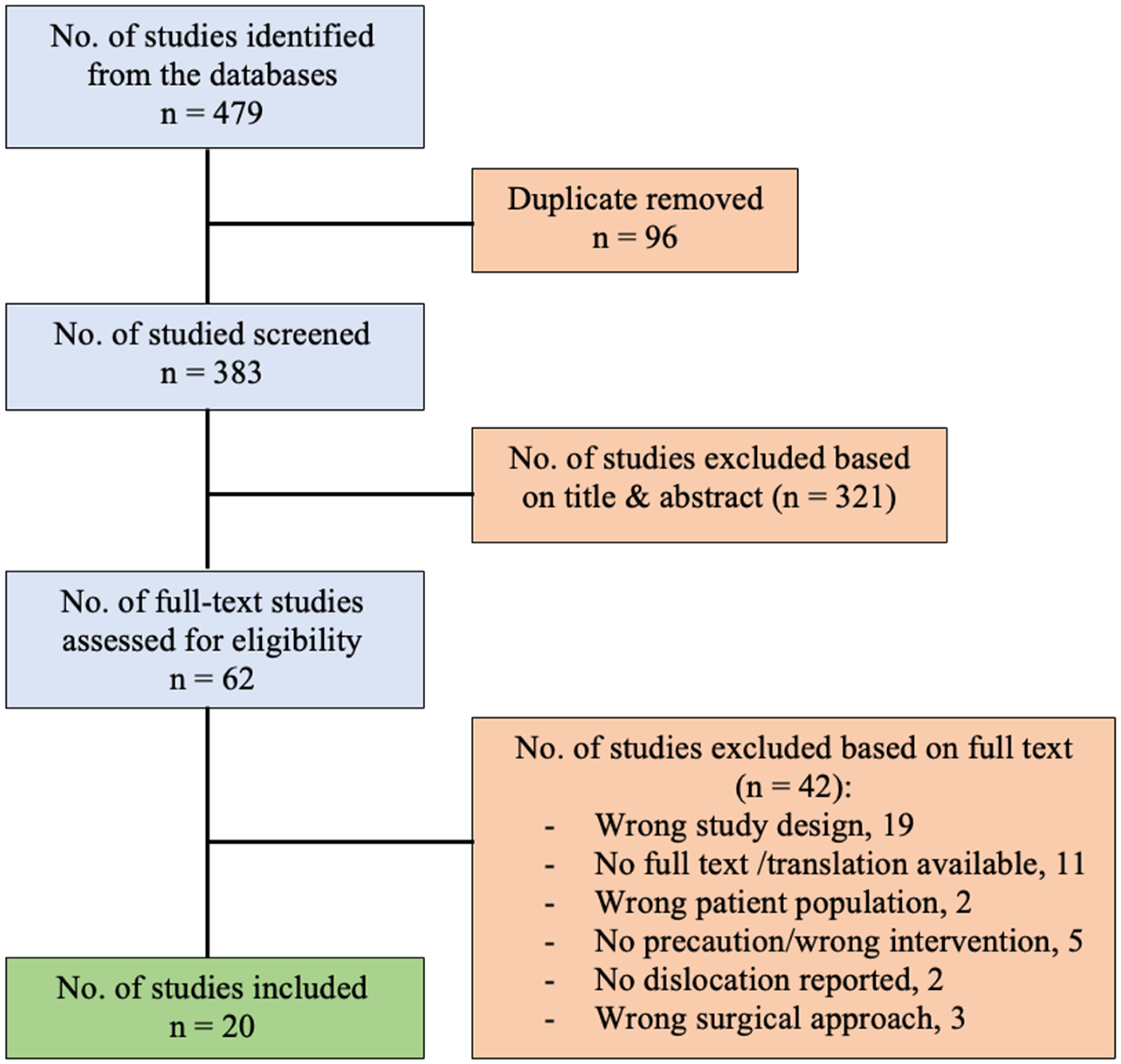
Flow diagram illustrating selection of studies.
Quality assessment
The quality of the publications was assessed using the Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence. 10
Modalities of hip precautions
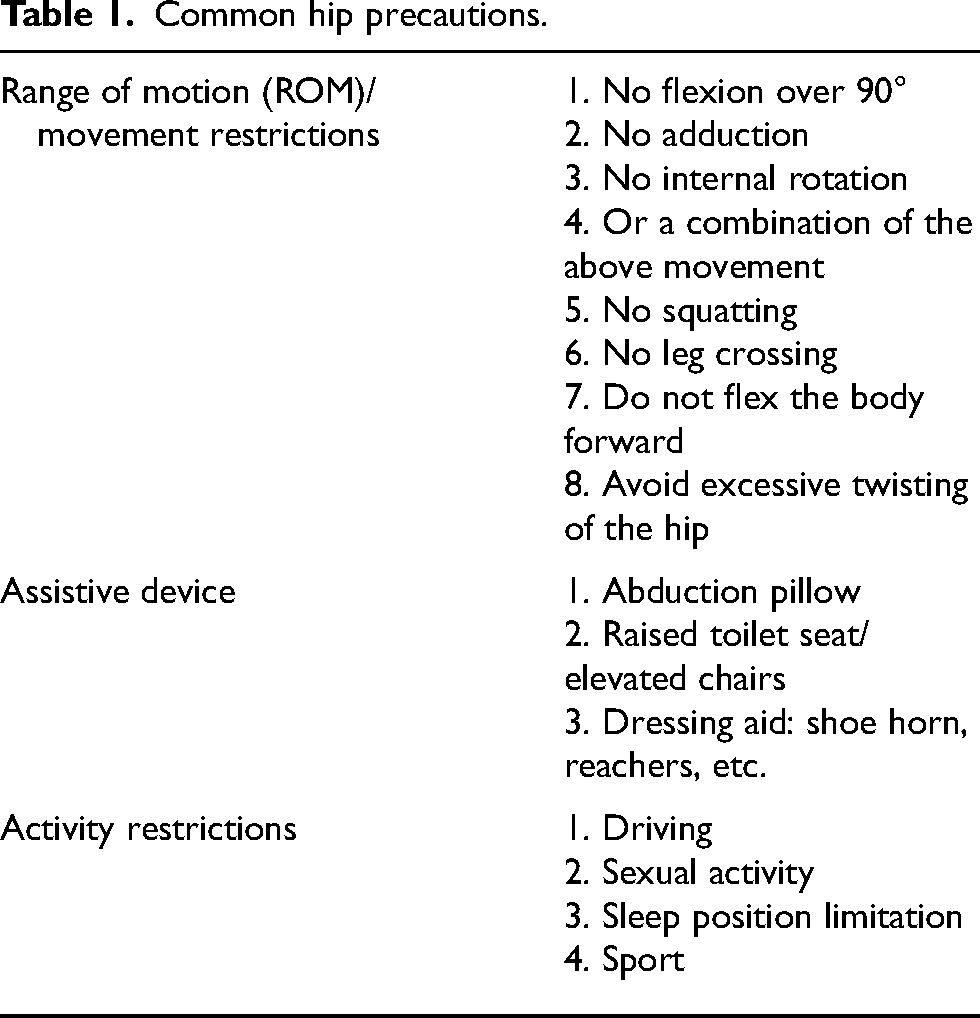
Table 1 outlines common hip precautions that will be discussed in this review. The study results regarding each modality of hip precautions are summarized in Table 2.
Common hip precautions.
Summary of study results for hip precautions including “ROM/movement restrictions,” “assistive device,” and “activity restrictions.”
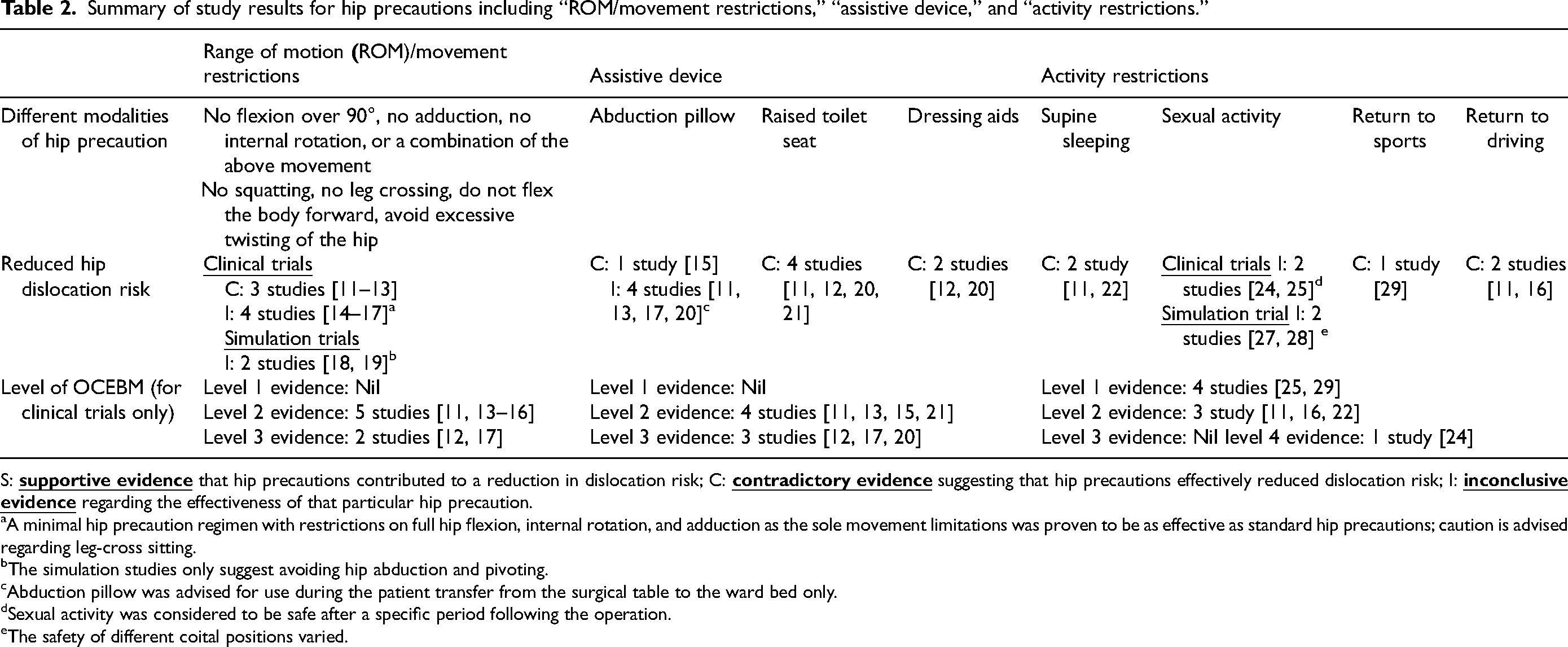
S:
A minimal hip precaution regimen with restrictions on full hip flexion, internal rotation, and adduction as the sole movement limitations was proven to be as effective as standard hip precautions; caution is advised regarding leg-cross sitting.
The simulation studies only suggest avoiding hip abduction and pivoting.
Abduction pillow was advised for use during the patient transfer from the surgical table to the ward bed only.
Sexual activity was considered to be safe after a specific period following the operation.
The safety of different coital positions varied.
Result
General hip precautions
There is substantial level 1 evidence demonstrating the fact that hip precautions may not be as effective as previously thought in reducing the dislocation risk after THA with a posterolateral approach.2,6,7 According to Korfitsen et al.'s review, 2 the quality of evidence was assessed by the GRADE approach and the risk of bias assessment using the Cochrane risk of bias tool was performed. It concluded that the current evidence did not support the routine prescription of hip precautions for patients undergoing THA to prevent hip dislocations. However, this conclusion could be revised pending the results of future high-quality studies.
Range of motion (ROM)/movement restrictions
Traditionally a standard ROM precaution involved refraining from flexing the surgical hip beyond 90°, internally rotating the surgical hip, and crossing the legs/adducting the hip beyond the midline of the body.11–13 Our analysis, incorporating data from three single-center RCTs, evaluated 607 patients who were instructed to adhere to these precautions for a period of 6 weeks. The analysis revealed no significant difference in dislocation rates compared to the control group with no movement restrictions, which consisted of 601 patients.14–16 Consequently, allowing movements such as hip flexion over 90°, adduction past the midline, and internal rotation might enable patients to resume activities of daily living more quickly without increasing the risk of hip dislocation based on all these existing level 2 evidence.14–16
Moreover, hip precautions on ROM were not completely eliminated in studies proposing a minimal or relaxed hip precaution, which preserved a combination of full hip flexion, internal rotation, and adduction as the sole ROM precaution after THA. This minimal hip precaution has demonstrated non-inferiority to the traditionally standard ROM precaution in terms of preventing hip dislocation.11–13,17 On the other hand, there is currently insufficient evidence to support the effectiveness of enforcing a combination of full hip flexion, internal rotation, and adduction in preventing dislocations, compared to a regimen involving no specific precautions. Notably, the prohibition of leg crossing remains a prominent restriction in most minimal hip precaution protocols examined in these studies.11,13,17
With the advent of robotic-assisted systems, 3D and computer simulations have been employed to evaluate safe ROM post-THA. Research by Eslam Pour et al. 18 in 2023 indicated that minor degrees of hip abduction could significantly reduce the risk of dislocation. Specifically, a combination of 20° of abduction and up to 20° of internal rotation, whether in a flexed sitting or forward bending position, was considered safe. 18 Further analysis by Tung et al. 19 assessed the risk of impingement across 11 common positions in daily life, identifying pivoting as a high-risk movement that should be avoided post-THA.
Assistive device
Abduction pillow
An abduction pillow is traditionally used to help prevent patients from unconsciously performing adduction movements (Figure 2). However, recent findings suggested that the use of abduction pillows may not be as critical as previously thought. According to an RCT by Mounts et al., 15 the dislocation rate did not increase when abduction pillows were omitted from postoperative care for THA patients. The use of the abduction pillow was only limited to the critical period immediately before transferring the patient from the operating table to the ward in minimal or relaxed hip precautions, whereas the abduction pillow was consistently used for the whole period of hospitalization in the standard precaution.11,13,17,20 An analysis of data from three studies that compared minimal hip precautions to standard precautions revealed 36 instances of dislocation among a total of 1795 patients in the standard precaution cohort and 26 cases in the minimal hip precaution cohort at a 6-week postoperative follow-up, with no significant difference found between the two groups.11,13,17

Abduction pillow.
Raised toilet seats/elevated chairs
Raised toilet seats and elevated chairs are traditionally employed to prevent excessive hip flexion following THA (Figure 3). Several studies indicated that the evidence supporting their impact on reducing dislocation rates was limited.11,12,20,21 Patients without the use of a raised toilet seat would be able to achieve independent toileting earlier. 20 Moreover, the prescription of a raised toilet seat may also increase the patient's anxiety postoperatively. Chan et al.'s study 20 also suggested that there is no need to specifically adopt elevated heavy chairs with armrests.

Raised toilet seat.
Dressing aids
Although with a limited level of evidence, dressing aids include shoehorns, ergonomic reacher, sock aids, dressing sticks, etc. which help THA patients to perform any at-risk positions for dislocation including crossing their leg, bending forward, bringing the knee towards the chest, etc., have been proven to be ineffective in preventing dislocation.12,20 Patients may choose to use dressing aids based on personal preference; however, their use is not a necessity. 12
Restrictions of activity of daily living
Sleep position restricted to supine
Peters et al.'s 22 RCT comparing the restricted group (post-THA patients with a supine sleeping position) to the unrestricted group (patients without any sleeping restriction) did not suggest any differences in their early dislocations within an 8-week follow-up. In his subsequent RCT, the same group explored patient compliance with the supine sleeping restriction. During the initial 8-week postoperative period, patients in the unrestricted group significantly spent fewer days per week sleeping in a supine position compared to patients in the restricted group, minimizing the risk of bias in the primary study due to non-adherence to assigned interventions. 23 Furthermore, the unrestricted group reported a significant reduction in the burden associated with sleeping restrictions. 23 The study by van der Weegen et al. 11 also indicated that restricting patients to supine sleeping positions did not effectively prevent dislocations following THA.
Sexual activity and safe coital positions
The recommendations for return to sexual activities after posterior THA were based on limited evidence. Laffosse et al.'s 24 cohort study concluded that a supine position between the first and second months postoperatively is considered to be safe and after 3 months post-surgery, there are generally no restrictions on sexual positions. Nevertheless, Issa et al. 25 conducted a systematic review of sexual activity after THA which included studies with limited evidence. The results from three of the included studies demonstrated a mean time to return to sexual activity of 4 months, ranging from 0.1 to 48 months. 25 According to the guidelines from the American Academy of Orthopaedic Surgeons (AAOS), sexual intercourse could be resumed at around 6 weeks after surgery. 26 In light of simulation trials, three positions were generally considered safe for both genders according to Charbonnier et al. 27 and Stegelmann et al. 28 : (1) supine/missionary position for male; (2) supine/missionary position for female; (3) both partners standing with the woman slightly bent and the male approaching from behind. However, there were inconsistent findings regarding at-risk sexual positions.27,28
Return to sports (RTS)
Hoorntie et al.'s systemic review reported a low risk of dislocation with RTS after THA. 29 Despite a significant number of level 1 evidence in the literature delineating the recommended timeframe for RTS after THA, as well as prognostic factors for RTS and appropriate categories of sports to engage in post-surgery, these recommendations primarily stem from concerns regarding aseptic loosening or implant wear. 30 Recommendations generally advocate for low-impact sports such as walking, cycling, swimming, and golf, while high-impact sports such as tennis, jogging, contact sports, and gymnastics were discouraged following the procedure.29–31 Moreover, Sowers et al. concluded that the advised period before RTS varied by sport, with an average of 6 months (ranging from 4 to 7 months). 31
Return to driving (RTD)
van der Weegen et al. 11 suggested that patients were permitted to resume driving once they could walk unaided, which was not associated with an increased risk of early hip dislocation. Tetreault et al. 16 also found that participants in the unrestricted group returned to driving significantly earlier than those in the restricted precaution group, with no significant differences in dislocation rates between the two groups. Abbas et al.'s systematic review suggested resuming driving within a timeframe of 4 to 6 weeks post-surgery. 32 However, such a recommendation was established considering additional factors extending beyond the risk of dislocation, encompassing complex skills required for driving, such as patients’ brake reaction time, vehicle type (automatic vs. manual), surgical side (right vs. left), ongoing medication, and concurrent comorbidities.32–34
Hip precautions in populations with lower-level risk of dislocation
Anterior approach
In a higher-risk patient population, the direct anterior approach demonstrated a lower dislocation rate compared to the posterior approach within the first year following surgery. 4 Peak et al.'s RCT in 2005 35 provided level 2 evidence indicating that total hip arthroplasty performed via an anterolateral approach was likely associated with a low dislocation rate, and the removal of several restrictions did not increase dislocation prevalence. Restrepo et al.'s study in 2011 reaffirmed the conclusion. 4
Dual mobility
Dual mobility cups are frequently applied as reducing the risk of dislocation following revision THA. Gibian et al. 36 suggested that traditional posterior hip precautions may be unnecessary due to the very low dislocation rate and increased patient satisfaction associated with the use of the Monoblock dual-mobility construct.
Discussion
In a qualitative study conducted in Switzerland, 37 surgeons expressed concerns about the nonspecific nature of hip precautions, which contributes to uncertainty regarding subsequent treatment approaches. One surgeon noted, “I have never seen specific hip precaution instructions on a prescription.” Hence, this review, in addition to the previously reported systematic reviews, organized thorough recommendations on whether the removal of certain hip precautions would be clinically safe, based on the current existing clinical evidence. Furthermore, it elaborated on detailed suggestions pertaining to individual hip precaution modalities for physicians to consider their applications to future patients.
There is a significant clinical implication for the omission of hip precautions. Socioeconomic benefits were created by reallocating healthcare resources such as staff time for individualized hip precaution education sessions towards evidence-based strategies to prevent falling, which has been proven to be strongly associated with post-THA dislocations. 7 Individual-wise, removing unnecessary hip precautions undoubtedly allows for an earlier return to work and daily activities. Chan et al. emphasized that removing restrictive hip precautions better aligned with the principle of fast-track arthroplasty, which aims at enhancing the patient's recovery, reducing the length of stay, and returning the patient to the function of ADL. Mikkelsen et al. 12 reported that a significantly higher number of patients in the unrestricted group were able to independently perform ADL and had returned to work at 6 weeks postoperatively. Enhanced patient satisfaction is achieved through faster functional recovery, while simultaneously reducing the financial burden related to lost wages, transportation costs, and dependence on caregivers.12,16 There are also concerns about the potential heightened patient anxiety and fear of dislocation brought by hip precautions, particularly if the individual was already experiencing anxiety before the surgery. 37 The removal of hip precautions may improve patients’ mental well-being by avoiding the perpetuation of their sick role, positively impacting the progress of recovery. 20
Although our study found that most hip precautions can be safely removed without increasing the risk of dislocation which corresponds to the findings and conclusions from previous reviews, the consideration of prescribing hip precaution post-THA with a posterior approach should be individualized based on the patient's physical condition, especially for patients with a higher risk of hip dislocation, 2 including those patients aged over 75, mental disability, revision THA, small head diameter, stiff spine, large anterior pelvic tilt, poor intra-operative stability, and suboptimal component placement. Furthermore, hip precautions should be individualized based on the patient's psychological status. Some patients find that hip precautions offer reassurance, which may contribute positively to their psychological well-being. 2 Specifically, regarding assistive devices, our study revealed that the prevailing evidence supports providing necessary devices or aids to patients who perceive a need for them. Therefore, we recommend that surgeons consider individualized advice in complex cases, while generally omitting most hip precautions. More specific suggestions and detailed recommendations could be formulated once further studies investigate different subgroups of patients who may benefit more from postoperative hip precautions after THA.
Several factors may account for the lack of observed differences between groups adhering to standard precautions and those following minimal or no precautions, as discussed in prior systematic reviews.2,7 Firstly, the study populations generally presented a low dislocation risk, primarily due to the use of a larger average femoral head size. Additionally, individuals at higher risk, such as those with severe osteoarthritis of the hip, were specifically excluded from the studies conducted by Dietz et al. 14 and Peters et al. 22 Furthermore, the study by Mounts et al. 15 was limited to patients demonstrating intra-articular stability. Secondly, while some research has explored patient adherence to assigned hip precautions, the level of adherence remains unreported in certain studies. This omission introduces uncertainty regarding whether the absence of significant differences can be attributed to the actual ineffectiveness of the hip precautions.
A limitation of this review is that our recommendations for prescribing individual hip precautions are only based on whether a post-THA dislocation would occur. It is unclear if the absence or prescription of hip movement precautions would contribute to increased rates of other complications such as implant loosening or accelerated wear. 7 Moreover, in postoperative care, hip precautions are commonly provided as a set of guidelines, making it challenging to evaluate the individual impact of each modality within the prescribed regimen. Notably, Peter et al.'s 22 investigation focusing on sleeping positions uniquely isolated sleeping posture restrictions as the sole variable among hip precautions for the two study groups. Consequently, future research could delve deeper into analyzing the specific effects of each modality contained within the standard hip precautions regimen routinely administered to provide more solid evidence regarding their individual effectiveness. Furthermore, our review was not registered with a pre-published review protocol, which may predispose to certain reporting bias.
Our recommendations
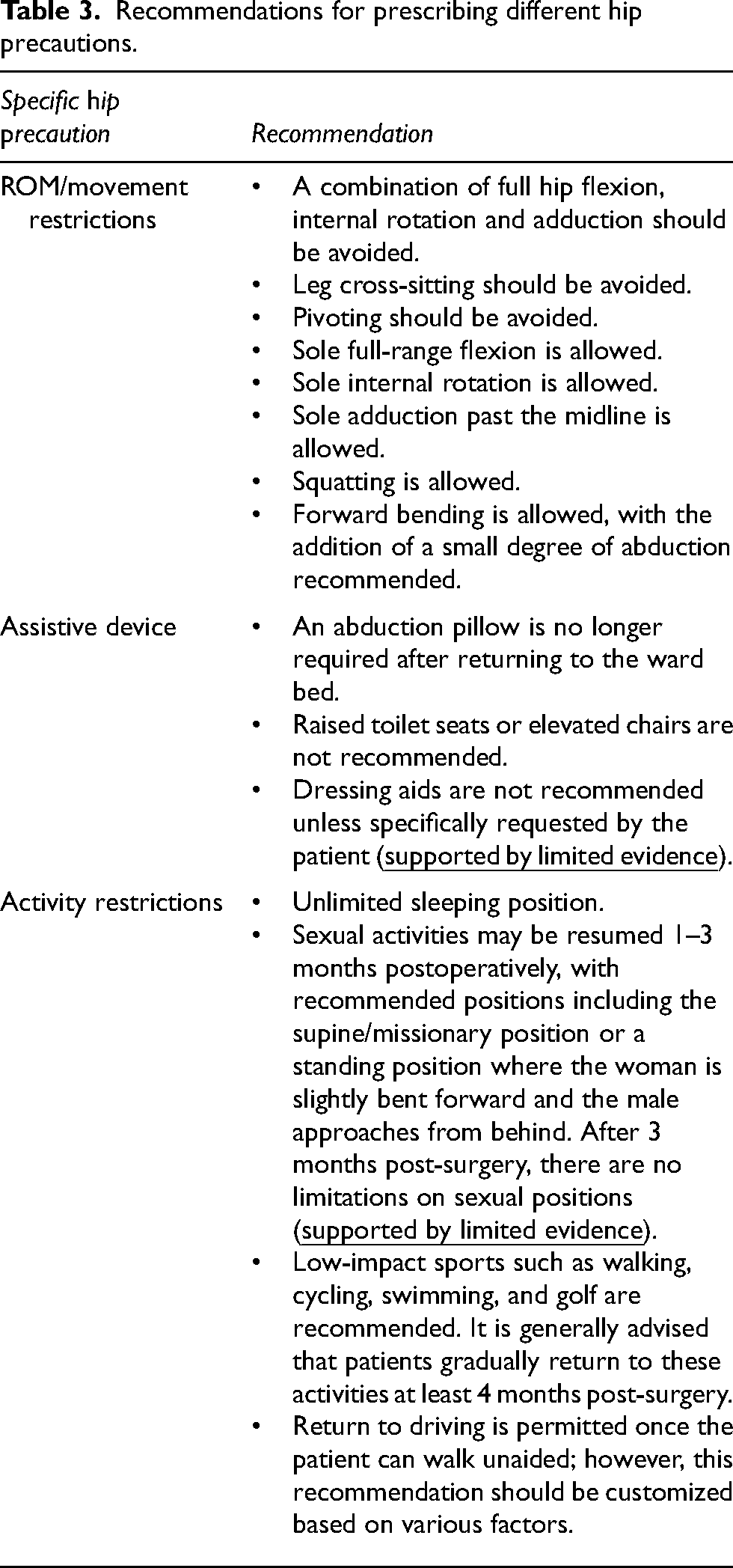
Table 3 summarizes the recommendations for hip precautions after THA with a posterior approach based on the study findings. Surgeons may recommend that patients resume their daily activities based on the recommendations and the intricacies of each patient's circumstances.
Recommendations for prescribing different hip precautions.
Conclusions
The existing body of research suggests that numerous hip precautions can be safely omitted without increasing the risk of dislocation post-surgery. Tailored recommendations for each precaution were formulated based on a minimum of level 2 evidence, ensuring a more precise and evidence-based approach to patient care.
However, the available evidence is limited regarding the use of dressing aids and the resumption of sexual activities following the operation. Further research in these areas is warranted to provide clearer guidelines and enhance postoperative care strategies for patients undergoing hip arthroplasty.
Footnotes
Authors’ contributions
HF conceived of the presented idea. All authors contributed to the methodology design and development of the framework. AC, BL, and CCH conducted the online article retrieval. AC and BL screened and reviewed the search results. AC wrote the manuscript. All authors had full access to the data, contributed to the study, approved the final version for publication, and took responsibility for its accuracy and integrity.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HF is a consultant of Stryker, Depuy, and Zimmer.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.