
Abstract
Background:
Dislocation is one of the most common causes of revision after total hip arthroplasty (THA). Standard hip precautions are thought to enhance soft-tissue healing and reduce dislocations. However, lifestyle restrictions affect a patient’s rehabilitation, quality of life (QOL), and satisfactions. We aim to compare conventional (CP) and minimal hip precautions (MP) after THA.
Methods:
Retrospective review of prospectively collected data in posterolateral approach THA. Chief surgeon assigns patients to CP or MP group. CP group had to sleep supine, used elevated toilet seats and chairs, avoid hip flexion greater than 90°, and no internal rotation or adduction for 6 weeks. MP group had no restrictions in hip movements, except for the combined flexion, adduction and internal rotation. All had a minimum 1-year follow-up. The number of dislocations, length of stay (LOS), time to independent toileting, Harris Hip Scores, QOL, and health perceptions, assessed by EuroQol 5D-5L, was compared between CP and MP groups.
Results:
Fifty-five THAs were included. CP group consisted of 17 primary and 12 revision THAs; MP group consisted of 21 primary and 5 revision THAs. There were two dislocations and both are revisions in CP group. Overall rate of dislocation was 6.9% in CP group and no dislocation in MP group (p-value > 0.05). MP group had shorter LOS (12 vs 19 days, p-value 0.04), higher EQ5D-5L health perception scores at 1-year (81.7 vs 70.9, p-value 0.01).
Conclusion:
MP group had shorter LOS and better health perceptions 1-year after THA with no increase in dislocation rates.
Introduction
Osteoarthritis is the most common type of arthritis and is one of the 10 most disabling diseases in developed countries. 1 Most patients with osteoarthritis have limitations in their joint movements and 25% cannot fulfill their major activities of daily living all across the world. 1 Although hip osteoarthritis is less common in Asian, it still has a prevalence of 3–15% in patients older than 65 years old in Asian regions. 2
Total hip arthroplasty (THA) is highly effective in decreasing pain, restore function, and improve quality of life (QOL) in patients with end-stage hip osteoarthritis. 3,4 However, dislocation after THA is a catastrophic complication for both patients and surgeons. Despite all the advances in THA, dislocation remains the most common cause of revision, accounting for 17.3% in the United States. 5 There are various risk factors for THA dislocation, including patient-specifics, surgical techniques, and postoperative factors. Traditionally, standard hip precautions avoid placing the hip in at-risk position, aims to nurture soft-tissue healing during the early postoperative phase to reduce the risk of dislocations. However, recent studies showed that more relaxed or minimal restrictions after posterolateral approach THAs did not increase the rate of dislocation, 6 –9 while the use of hip precautions slow down the pace of functional recovery and reduce patient’s satisfaction. 10 –12
There are only several studies specifically examining hip precautions in posterolateral approach THA, 6 –10 and even fewer exploring patient’s function and quality of with different degrees of restrictions after THA. 10 Therefore, we design this study to investigate the role of convention and minimal hip precautions in dislocation rate and patient’s functional outcomes after posterolateral THA.
Patients and methods
A retrospective review of prospectively collected data in patients undergoing total hip arthroplasties (THA) in a tertiary-referral academic hospital. Our Institution Review Board has approved this study with reference number UW 20-627. Patients scheduled for THA from 2016 to 2017 in our institution were recruited. Patients were included if they suffer from unilateral hip disease or if contralateral hip successfully treated with THA, able to follow commands for rehabilitation training, THA performed with the posterolateral approach, and allowed full weight-bearing walking postoperatively. Exclusion criteria include requiring protected weight-bearing postoperatively, known dementia or other neuromuscular diseases, and any surgical complications, such as wound problems, infections, fractures, or nerve injuries. Patients with unsatisfactory hip stability during the intra-operative assessment (hip dislocatable at 90° flexion, 30° adduction and 45° internal rotation) were also excluded from current study. All THA and perioperative care were managed by the same team of surgeons and occupational therapists.
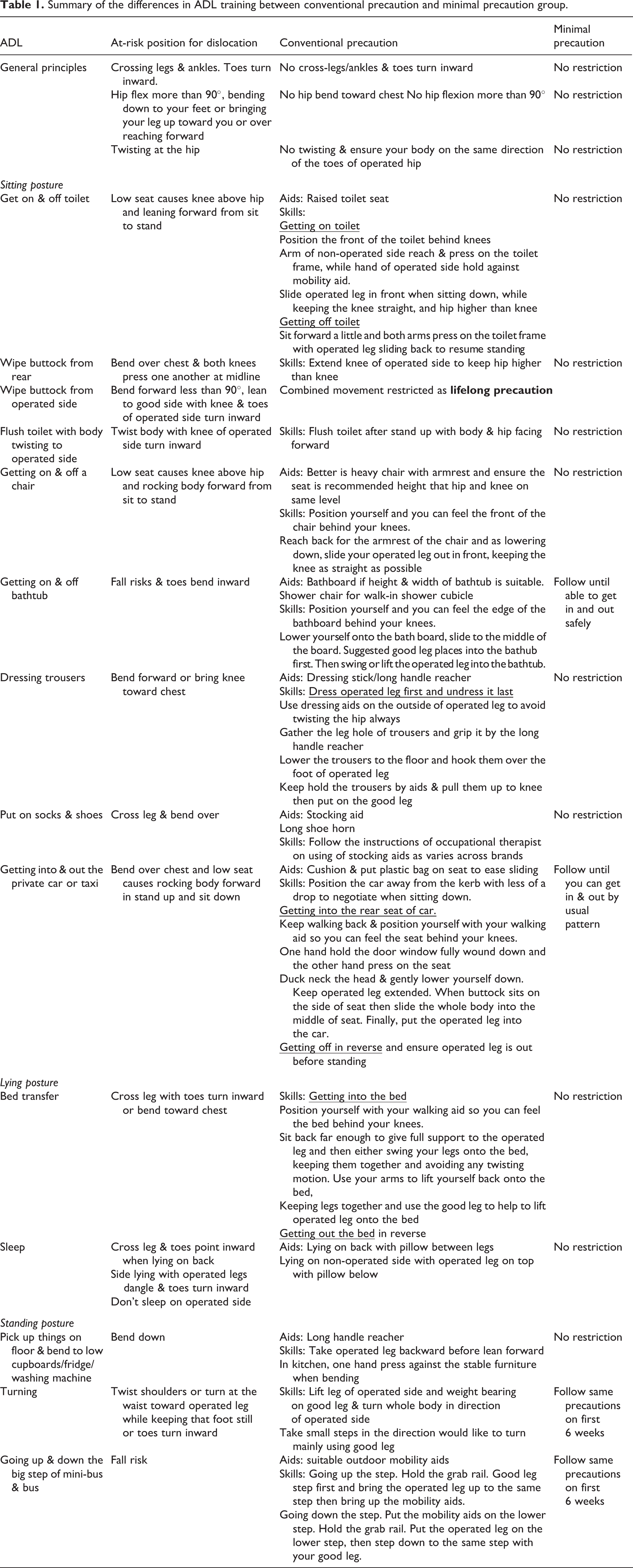
According to the chief surgeon’s decision, patients with satisfactory hip stability during the intra-operative assessment (hip not dislocatable at 90° flexion, 30° adduction and 45° internal rotation) were assigned to the minimal hip precaution (MP) or convention hip precaution (CP) group. The CP group received daily living (ADL) training by occupational therapists, consisting of patient education and ADL restrictions. The CP group used an abduction pillow during the hospital stay and was advised to sleep supine, used elevated toilet seats and chairs, avoided hip flexion to greater than 90°, and no internal rotation or hip adduction was allowed for 6 weeks. On the other hand, the MP group was allowed to lean forward, cross-legs, and squat immediately after THA. The MP group had no restrictions in the hip range of movements, except for the combination of hip flexion to greater than 90° and adduction and internal rotation. MP group had no abduction pillow, no sleep restrictions, and no elevated toilet seats and chairs. Table 1 summarized the differences in ADL training.
Summary of the differences in ADL training between conventional precaution and minimal precaution group.
Both CP and MP groups were follow-up for at least 1 year after THA. Baseline characteristics and various risk factors for hip dislocation, such as diagnosis, femoral head size, and intra-operative hip stability were compared. All episodes of hip dislocation were collected via hospital admission records and telephone interviews. Hip functions were assessed using the Harris Hip Score (HHS, from 0 to 100). Patients’ quality of life (QOL) was assessed with the EuroQol (EQ) 5D-5L questionnaire. EQ5D-5L consists of six questions, and the first five questions assess five different dimensions of health, which are mobility, self-care, usual activities, pain, and anxiety in a five-point Likert scale, while the last question assesses the overall health perception from 0 (extremely poor) to 100 (extremely well). The EQ5D-5L rating from the first five questions was transformed into an index score that ranges from −0.281 (extreme problems) to 1 (no problem). Moreover, patients’ length of stay (LOS) and time to achieve independent toileting was used as a reflection of the patients’ rehabilitation progress. Readiness for discharge criteria was used to minimize the psychosocial effect on the LOS. Patients were considered fit for discharge if the medical and wound conditions were stable with adequate pain control (visual analog scale less than 5 out of 10) and ADL functions (independent walking and transfer).
The primary outcome is the difference in the hip dislocation rate between the CP and MP groups. The secondary outcomes include the differences in hip function and QOL index scores.
Patients’ demographics and various risk factors were analyzed with descriptive statistics and presented as means, range, standard deviations (SD), and percentages. The chi-square test was used to compare categorical variables, while the student t-test was used to analyze parametric variables. IBM SPSS statistic 26 software was used for statistical analysis. A p-value of less than 0.05 was considered significant.
Results
Fifty-five THA patients with 29 and 26 in the CP and MP group respectively were included for analysis. The mean age in the CP and MP group was 67 years old (SD 10.1, range 48 to 92 years old) and 65 years old (SD 14.9, range 36 to 83 years old) respectively. There were 16 females in the CP and 18 females in the MP group. The CP group included 19 cementless and 10 hybrid THAs, while the MP group comprised 17 cementless and 9 hybrid THAs. The CP group consisted of 17 primary and 12 revision THAs, while there were 21 primary and 5 revision THAs in the MP group. In both groups, the most and second most common diagnosis for primary THA was avascular necrosis (AVN) of the femoral head and osteoarthritis of the hip respectively. AVN accounted for 65% and 48% of the primary THA in the CP and MP group respectively. The 12 revision THA in the CP group included eight insert exchange for wear, one femoral and three cup revision for loosening; while the MP group included three insert exchange for wear, one femoral and one cup revision for loosening. In the CP group, the preoperative EQ5D-5L Index score, EQ5D-5L health perception score, and HHS were 0.68 (SD 0.27), 68 (SD 17) and 50 (SD 24) respectively; while the above scores were 0.67 (SD 0.28), 67 (SD 16), 50 (SD 23) in the MP group respectively. 36 mm was the most common femoral head diameter in the CP and MP and comprised 72% and 62% of THAs respectively. There were no statistically significant differences in the above baseline demographics, functional scores, and various risk factors for hip dislocation (p-value > 0.05) between both groups as shown in Table 2.
Baseline demographics, pre-operative hip function and various risk factors for hip dislocation in the Convention Precaution and Minimal Precaution group.
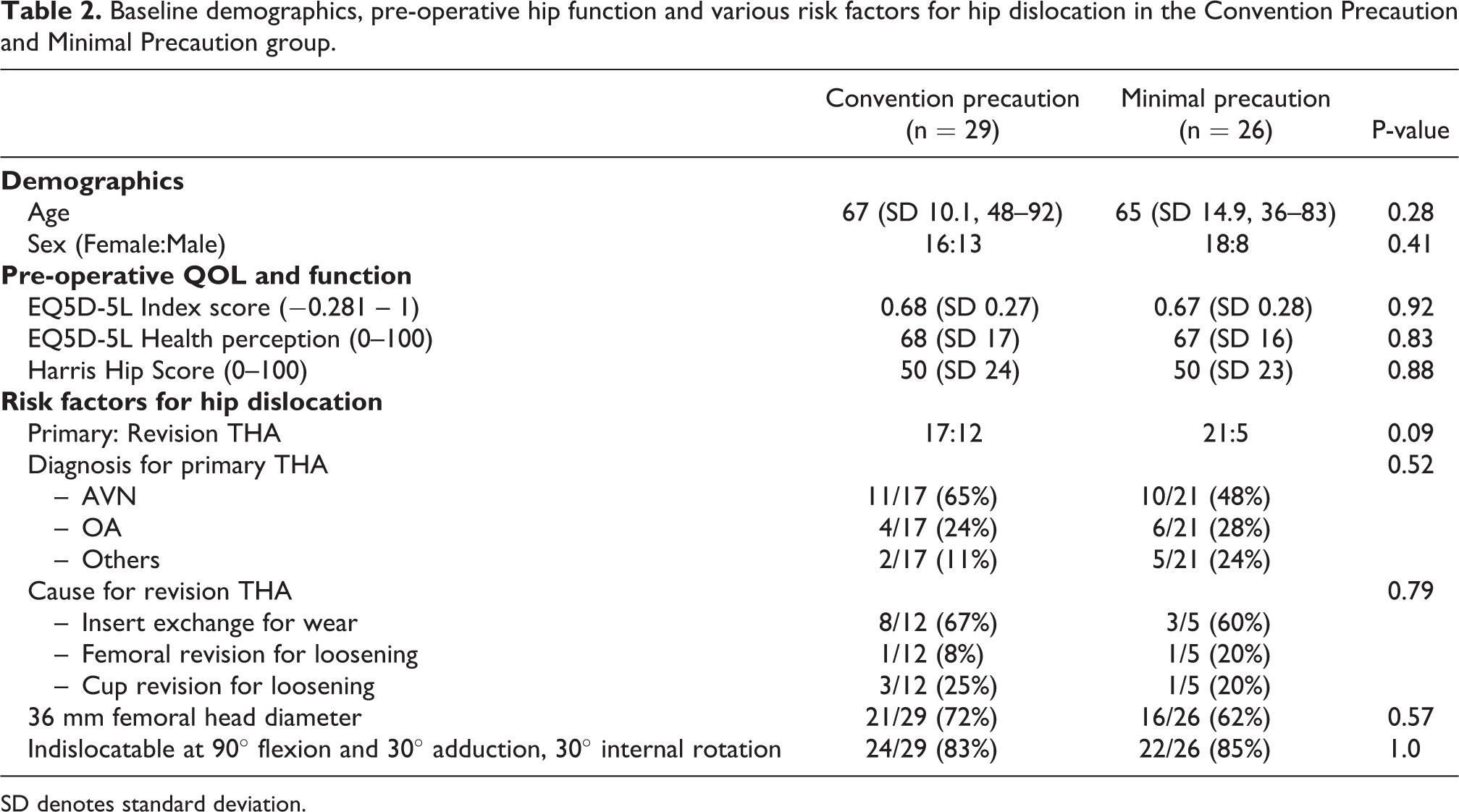
SD denotes standard deviation.
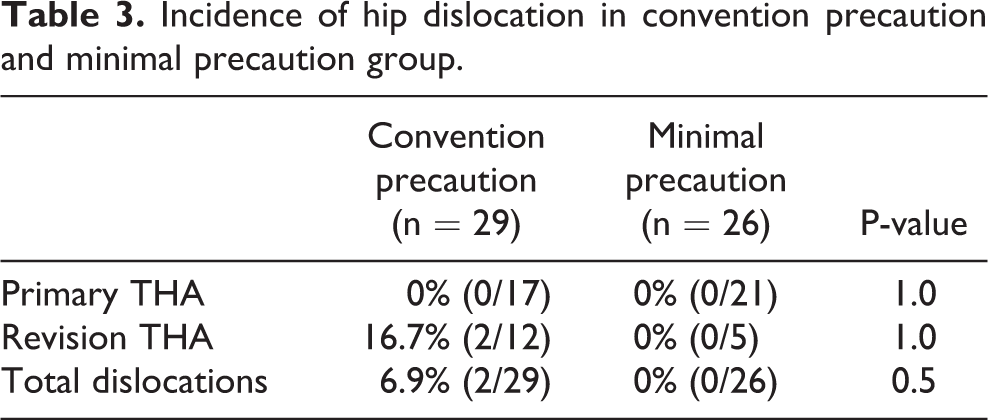
Concerning hip dislocations, there were two hip dislocations in this cohort and both were in the CP group and revision THA (Table 2). The overall incidence of hip dislocation was 6.9% in the CP group. There were no dislocations in the MP group. The differences between the CP and MP group dislocation rates were not statistically significant (p-value > 0.05), as shown in Table 3.
Incidence of hip dislocation in convention precaution and minimal precaution group.
Concerning postoperative rehabilitation progress, the MP group had a significantly shorter LOS than the CP group (12 days vs 19 days, p-value 0.04) (Table 3). Moreover, the MP group was able to achieve independent toileting earlier, however, this was not statistically significant (5.7 days vs 9.4 days, p-value 0.13) (Table 3). Regarding QOL scores, the MP group had significantly higher EQ5D-5L health perception scores than the CP group at 1-year post-operation (81.7 vs 70.9, p-value 0.01) (Table 3). The EQ5D-5L index score (0.81 vs 0.91) and HHS at 1 year (82.3 vs 80.7) were not statistically different between the CP and MP groups (p-value > 0.05), as shown in Table 4.
Post-operative hip function and quality of life scores in the conventional precaution and minimal precaution group.
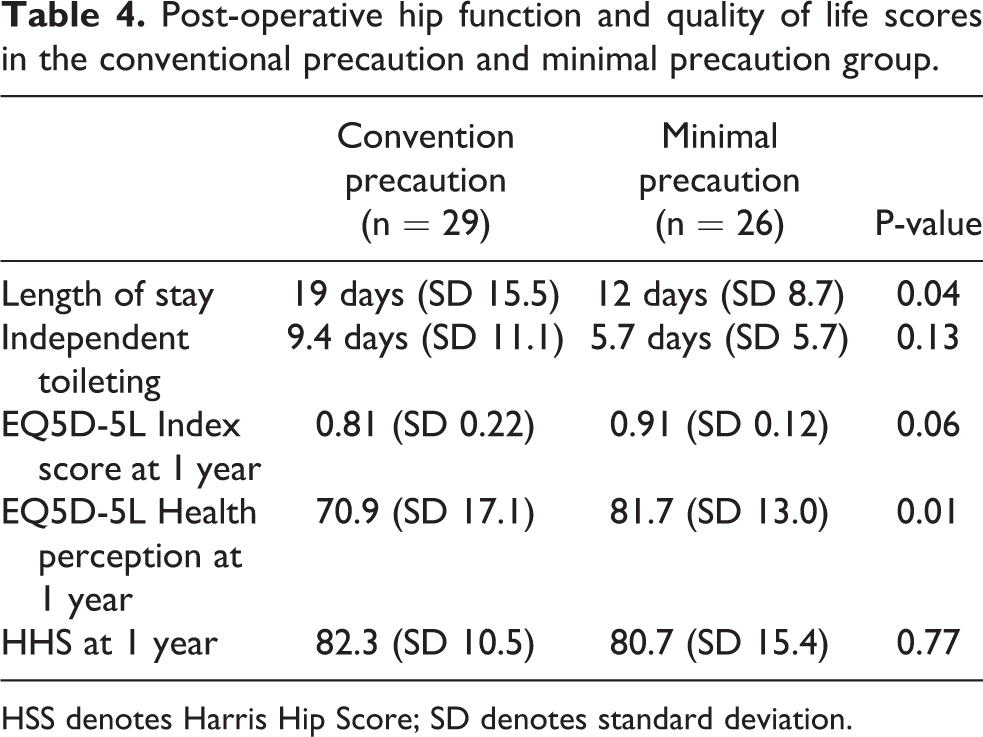
HSS denotes Harris Hip Score; SD denotes standard deviation.
Discussion
The main finding of this study is that patients with minimal hip precaution after THA have a significantly shorter length of stay and better health perception 1 year after surgery, while no differences in the rate of hip dislocation. This has important clinical implications, as conventional hip precautions restrict patient’s movement in daily life, such as sleeping supine, and use of elevated toilet seats and chairs, which causes inconvenience and induces extra-cost in purchasing additional equipment. Moreover, restrictive hip precautions also go against the principle of fast-track arthroplasty, which focuses on enhancing the patient’s recovery, reducing the length of stay, and returning the patient to the function of ADL. Hip precautions advise the patient to limit certain hip motions and perform daily activities with specific skills, which constantly reminds the patient of their post hip arthroplasty status, which might perpetuate their sick role and affect the progress of recovery.
THA is a successful treatment in end-stage osteoarthritis of the hip and shown to significantly reduce pain, restore function, and improved patient-reported quality of life. 13 –15 However, few studies have examined the effect of convention hip precautions on a patient’s quality of life and health perceptions. Mikkelsen et al. compared 365 posterolateral THAs with restricted and unrestricted rehabilitation protocol in terms of hip function in ADL, QOL, and ability to return to work. 10 There were no differences in QOL scores, but significantly more patients in the unrestricted group were able to perform ADL independently and returned to work at 6 weeks postoperatively. Ververeli et al. reported a randomized prospective study involving 81 anterolateral THAs and found that reduced hip precaution increases the pace of recovery compared with conventional hip precaution rehabilitations. 16 In this study, we used the EQ5D-5L, which is a valid and sensitive questionnaire to describe and value health in multiple dimensions. 17,18 We found that the minimal hip precaution group had better health perception at 1 year postoperatively (81.7 vs 70.9, p-value 0.01). Although the compliance to hip precaution varies, most patients do remember the limitation prescribed, 19 this constant mental reminder may contribute to the lower health perception in convention hip precaution patients even at 1 year.
A systematic review and meta-analysis in 2016 included six studies with a mix of anterolateral and posterolateral approaches, which reported the dislocation rate of the unrestricted and restricted group to be 1% and 1.5%, respectively. 11 Fewer studies examine the role of minimal hip precaution in the posterolateral approach. Traditionally, THA using a posterolateral approach has a higher dislocation rate. However, the advancement in surgical technique and increasing attention in soft-tissue repair reduces the dislocation rate in the posterior approach. Recent meta-analysis showed no differences in the risk of dislocations between posterior and anterior approaches. 20,21 A study by Brown and Ezzet reported no differences in early dislocations between standard and relaxed hip precautions with posterolateral approaches. 9 A large cohort study by Van der Weegen et al., included more than 2000 primary THAs performed with a posterolateral approach, found minimal restrictions was not inferior to usual restrictions in dislocation rates, however, more hips had a femoral head larger than 32 mm in minimal restrictions group. 7 In this study, there was no dislocation in all primary THA, while two (16.7%) dislocations in revision THA with conventional hip precautions. One of the reasons for a low dislocation rate is because of the use of a large femoral head, 62% and 72% of THA have 36 mm femoral head in the MP and CP group respectively. Revision surgery is a well-established risk factor for dislocation after THA with reported dislocation rates ranges from 6.6% to 21.2%. 22 –24 Although there were five revision THAs in the MP group, none of dislocated. However, the numbers are too few to draw any conclusions.
This study has several strengths. The same surgical team with four chief surgeons and comparable surgical techniques performed all the primary and revision THAs. The perioperative care and rehabilitation protocols are standardized and carried out by the same team of therapists to minimize confounding factors that affect hip dislocation rates. Most of the previous literature examining hip precautions after THR focused on its effect on dislocation, few look into the patient’s QOL and health perception. In this study, we assess the patient using the EQ5D-5L questionnaire and report on the effect on QOL and health perception with or without hip precautions. Moreover, all patients have at least 1-year follow-up, which is longer than most other studies examining this matter, 6,7,9,10 allowing us to identify any hip dislocation beyond the early postoperative phase.
Our study had limitations. One major limitation is selection bias. As the assignment to CP or MP group is determined by the chief surgeon after considering multiple factors, such as intra-operative assessment of hip stability, and patient compliance to rehabilitation regimens…etc. Although the difference in revision arthroplasty did not reach statistical significance, there are more revision surgeries in the CP group, which increases the overall dislocation risk. Furthermore, various factors are affecting the risk of THA dislocation that was not controlled in this study, such as implant position, co-existing spinal pathologies, soft-tissue repair, and soft-tissue tension,…etc. 20,25 –27 Whilst there are only fifty-five patients in this study, our results are encouraging and act as a pilot for larger scale study to explore minimal hip precautions on a patient’s functional recovery, QOL, and health perceptions. Despite insert exchange being the most common cause for revision in both groups, we understand that revision hip surgeries are heterogeneous, with various factors affecting hip stability. Nevertheless, we reported our experience with minimal hip precaution in revision THAs to motivate future studies to examine the role of hip precaution and enhanced recovery in the setting of revision hip arthroplasties.
Even though more and more evidence supporting the use of relaxed hip precaution does not increase hip dislocation rates, the idea of activity restriction after THA is deeply rooted in many surgeons, therapists, and patients. A survey in 2018 from the American Association of Hip and Knee Surgeons and the Canadian Arthroplasty Society reported 44% of respondents universally prescribed hip precautions after THA. 28 Another survey in 2016 to physiotherapist and occupational therapist in the United Kingdom reported 97% of respondents routinely advise hip precautions with the duration ranges from 6 weeks to lifetime restrictions. 29 Despite recent advocates of relaxing life-style restrictions after THA, it is still a matter of debate whether such practice can improve patient’s recovery and clinical outcomes. A multicenter randomized controlled study by Dietz et al. found that no hip precaution group had lower Hip Injury and Osteoarthritis Outcome Jr scores than standard precaution group at 2 weeks. 30 The author suggested that self-limiting behaviors of the patients with no hip precaution prescribed contributed to their results. 30 Hence, more studies are required to investigate the effect of relaxing traditional hip precaution after THA on the pace of recovery, QOL, health perceptions, and risk of dislocations.
Conclusion
Patients with minimal hip precaution had a shorter length of stay and better health perception scores 1-year after THA, while no increase in THA dislocation rates.
Footnotes
Acknowledgements
We would like to acknowledge the occupational therapists June Chao, Viola Wong, Milly Lee and personal care assistants for provind occupational therapy and longitudinal data collection for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.