
Abstract
Introduction
Osteoarthritis of the knee (OA) is one of the leading musculoskeletal causes of disability in elderly patient. In Hong Kong, similar to other developed regions, there is an increasing proportion of elderly patients and with that, an increasing number of patients who seek management for OA knees. Total knee replacement (TKR) and unicompartmental knee replacement (UKR) are well-established surgical interventions for patients suffering from advanced OA knee.1,2 The aims of knee replacement surgery are to alleviate pain, improve joint function and enhance the overall quality of life. 1 Despite its widespread use, patient outcomes can vary significantly based on a multitude of factors. 1 To better understand and predict these outcomes, it is crucial to employ comprehensive assessment tools that evaluate both pre-operative and post-operative states.
One such patient-reported outcome measure is the Short Form 36 (SF-36), a widely utilised health survey designed to assess a broad range of health domains including physical functioning, bodily pain and overall well-being.3,4 The SF-36 has been instrumental in capturing the nuances of health-related quality of life (HRQoL) in various patient populations, including those undergoing major orthopaedic procedures such as TKR. 3 This tool's robust framework allows for a detailed analysis of how surgical intervention impacts patients across multiple dimensions of health. These factors include gender, body mass index (BMI) and the Kellgren–Lawrence (KL) grading system for OA severity. Gender and BMI are known to influence surgical outcomes and recovery trajectories, while the KL score provides a measure of pre-operative disease severity, potentially impacting post-operative results.5–7
Currently there are paucity of studies examining HRQoL outcomes in patients in Hong Kong before and after joint replacement procedures. This is of particular importance in the local population as long waiting times in the public sector often result in severe debilitation before surgery that is likely unseen in other developed regions in the world. This unique scenario also allows for the determination of optimal cut-off values for various pre-operation assessment tools in order to predict post-operative outcome across the whole spectrum of disease severity.
This study investigates the relationship and interplay between various patient-specific factors and changes in HRQoL at different pre-operative and post-operative time points, as assessed by the SF-36, in patients undergoing total knee replacement within the Hong Kong population. By integrating various assessment tools, we seek to enhance our understanding of how demographic and clinical variables interact with surgical outcomes, ultimately allowing for more treatment strategies and expectation management for the patient as well as for resource-effective guidelines for policy makers.
Methods
Retrospective data were reviewed for all patients undergoing TKR or UKR for primary OA knee at a tertiary institute from 2017 to 2023. Patients included in the study must have pre-operative and post-operative SF-36, KSKS and KSFA questionnaires completed. Patients with bilateral TKR, secondary arthritis or those who underwent revision TKR were excluded. Ethics approval was obtained from the local ethics committee (UW 23-484).
Data collection
Patient demographics including age, sex and individual BMI were retrieved. KL grading of the degree of osteoarthritis7,8 was determined from radiographs that were taken immediately before operation. Patient reported outcome measures were assessed pre-operatively and post-operatively at regular out-patient department follow up at 3, 6 and 12 months post-operatively.
Patient reported outcome measures
Short Form 36 health survey
The SF-36 is a generic 36-item, patient-reported survey of health that is commonly used to determine health care outcomes in adult patients. The survey contains eight domains: physical functioning; physical role limitations; bodily pain; general health perceptions; energy/vitality; social functioning; emotional role limitations and mental health. 3 The eight components contribute to the physical component summary (PCS) and the mental component summary (MCS) scores. 3 The score ranges from 0 to 100, with a higher score representing a better health status. 3
Knee Society Knee Score and Knee Society Functional Assessment score
The Knee Society Knee Score (KSKS), initially developed in 1989 and revised in 1993, was designed to provide both an objective and a subjective assessment of knee function following TKR. The objective score evaluates pain, knee stability and range of motion (ROM), with a total maximum of 100 points: 50 points for pain, 25 points for stability and 25 points for ROM. Deductions are made for deformity or malalignment in either the native or the arthroplasty knee. The functional score, also out of 100 points, is based on patient-reported outcomes, assessing walking distance (50 points) and stair use (50 points). Points are subtracted for the use of walking aids. 9
Kellgren–Lawrence Grading System
Knee radiographs in anteroposterior and lateral views were evaluated using the KL grading system. The KL score is based on osteophyte formation, joint space narrowing, presence of sclerosis and joint deformity and is graded on a five-grade scale.7 Grade 0, normal; grade 1, minute osteophyte and doubtful joint space narrowing; grade 2, definite osteophytes; grade 3, moderate osteophytes with definite narrowing of joint space; and grade 4, severe osteophytes and marked joint space narrowing with subchondral sclerosis. 8
Study outcome measures
The primary outcome of this study was to determine change in HRQoL, as reflected by SF-36 scores after TKR surgery. Secondary outcomes included changes in the KSKS and KSFA scores. The interaction between these outcome measures with patient and disease factors such as sex, BMI and degree of pre-operative osteoarthritic changes was also assessed.
Minimal clinical important difference
A minimal clinical important difference (MCID) of 10 was considered to have a clinically significant improvement after surgery.10,11 Patients with an increase of 10 or more in SF-36 PCS scores at post-operative 12 months was considered to have a successful surgical outcome.
Statistical analysis
Descriptive statistics were presented in mean with standard deviation or median with quartiles, and frequency in numbers and percentages. Data normality was tested, with non-parametric measures being used if data was not normally distributed. Comparison of pre-operative and post-operative ROM, scores of KSKS, KSFA and SF-36 were performed using Wilcoxon signed rank test at each post-operative time point. For each post-operative time points, the relationships of parameters at baseline and the changes of KSKS, KSFA and SF-36 scores were investigated via Spearman's correlation test and rank biserial correlation test for continuous and categorical variables, respectively. The strength of correlation was assessed by the correlation coefficient, rs or rrb. A comparison of outcomes between patients with difference severities of osteoarthritis based on KL grading scales was performed using the Mann-Whitney U test. Subgroup analyses based on gender and BMI were also conducted with scores and changes of scores being compared between groups through Kruskal-Wallis with Bonferroni correction for multiple tests in post hoc analyses.
Patients were stratified into the following groups based on BMI at the time of operation: normal weight 18.5 to 25.0 kg/m2, overweight 25.01 to 30.0 kg/m2, obese 30.01 to 40.0 kg/m2 and morbidly obese > 40 kg/m2.
Essential to any patient related outcome measures are the associated meaningful values such as the MCID and the minimal clinical important changes, which are needed to aid interpretation of results and power of the studies.10,11 Receiver operating characteristic (ROC) analyses were used for defining the cut-off value of pre-operative assessment measures for indicating surgical successful outcome as defined by an increase of SF-36 PCS score reaching the MCID (Figures 1 and 2). SPSS v.29.0 (USA) was used to conduct all analyses. Statistical significance level was set at P < 0.05.
Results
A total of 97 patients met the including criteria for analysis, with mean age of 70.1 +/− 6.7 years. There were 71 females and 26 males. The mean age in females was 70.4 +/− 6.1 years and in males it was 69.4 +/− 8.0 years; mean BMI was 28.2 +/− 3.9 kg/m2 (Table 1). The mean pre-operative KSKS and KSFA scores were 50.8 +/− 13.2 and 51.2 +/− 14.9, respectively. There was an even distribution of knees with 47 (48.5%) KL grade 3 and 50 (51.5%) patients with KL grade 4.
Patient characteristics at baseline pre-operatively.
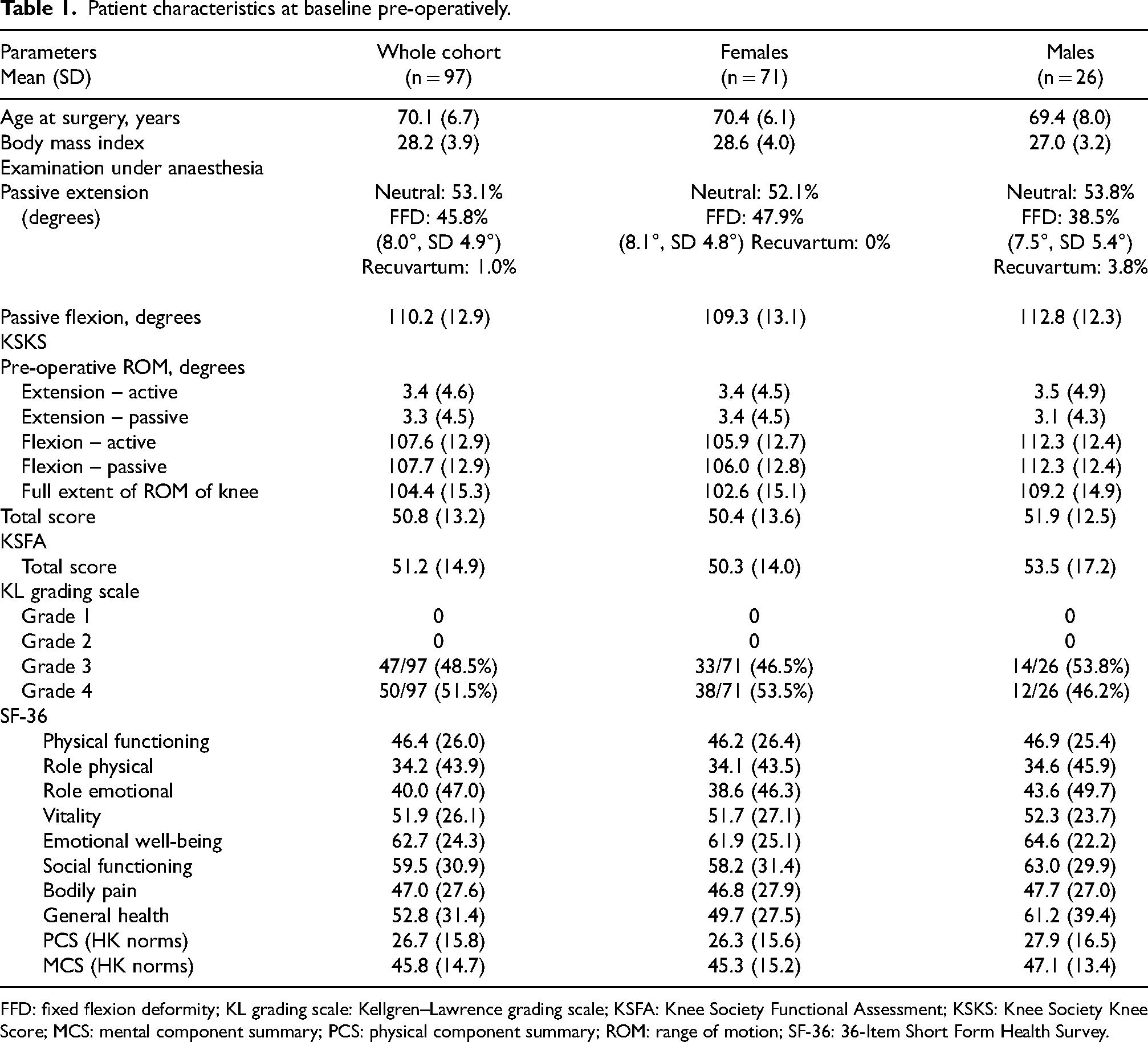
FFD: fixed flexion deformity; KL grading scale: Kellgren–Lawrence grading scale; KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; ROM: range of motion; SF-36: 36-Item Short Form Health Survey.
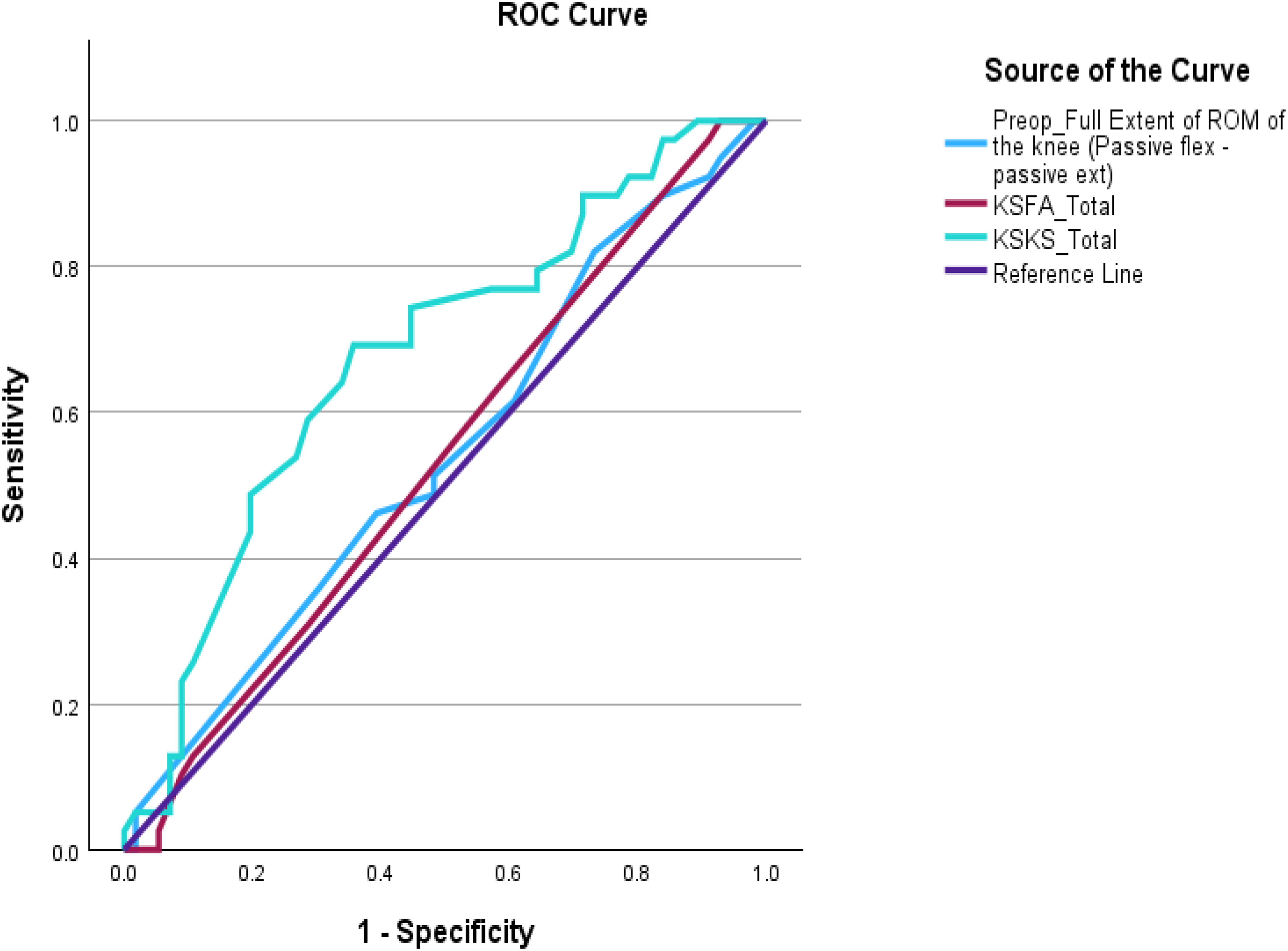
Total KSKS, total KSFA and pre-operative passive ROM of the knee were assessed and found that total KSKS scores encompassed the largest area under the curve (AUC) (0.676). This cut-off score was based on the SF-36 PCS MCID. Based on Figure 1, we defined a total KSKS score of 53.5 as the threshold value in predicting patient satisfaction; with a sensitivity of 69.2% and specificity of 64.3%; patients with a pre-operative KSKS lower than this were more likely to have a successful surgical outcome (SF-36 PCS improvement of 10 points or more compared to pre-operation level) (Tables 2a and 2b).
ROC analysis with cut-off value of pre-operative assessment measures for indicating surgical successful outcome.

KSKS: Knee Society Knee Score; ROC: receiver operating characteristic.
TKR and UKR ROC analyses for defining the cut-off value of preoperative KSKS total score for indicating surgical successful outcome.
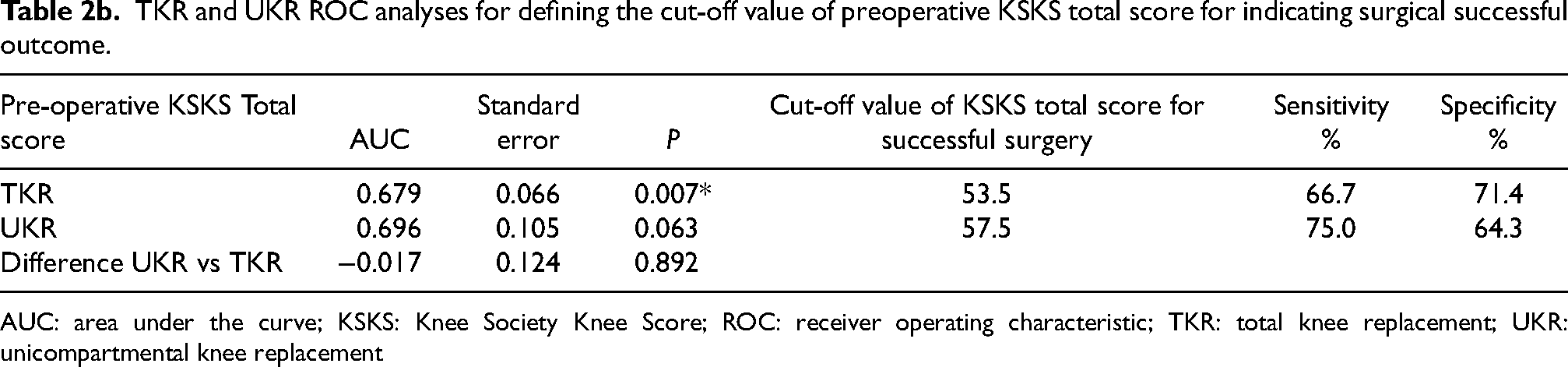
AUC: area under the curve; KSKS: Knee Society Knee Score; ROC: receiver operating characteristic; TKR: total knee replacement; UKR: unicompartmental knee replacement
ROC analyses with cut-off value of pre-operative assessment measures for indicating surgical successful outcome. ROC: receiver operating characteristic.
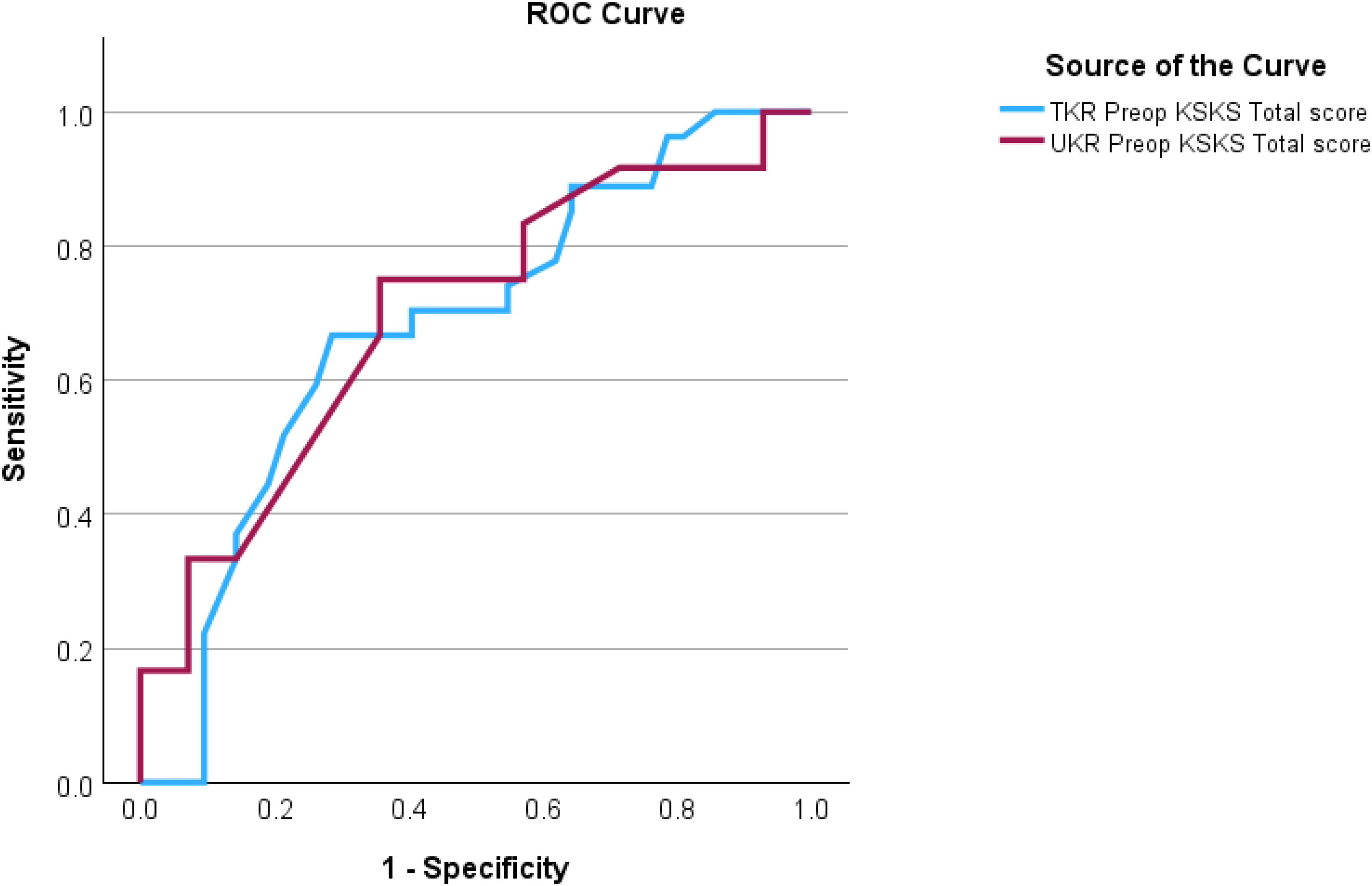
TKR and UKR ROC analyses for defining cut-off value of pre-operative KSKS total score for surgical successful outcome. KSKS: Knee Society Knee Score; ROC: receiver operating characteristic; TKR: total knee replacement; UKR: unicompartmental knee replacement.
Overall, significant improvements in KSKS, KSFA and SF-36 scores were seen at all time points post-operation compared to pre-operative levels. However, it was noted that KSKS scores peaked at 6 months then plateaued, whereas the KSFA scores continued to improve until 12 months post-operation (Table 3). Interestingly, although initial improvements in SF-36 scores for both PCS and MCS components were observed at both 3 and 6 months post-operation, however, this was followed by a decline at 12 months post-operation (Table 3).
Comparison of pre-operative and post-operative scores for KSKS, KSFA and SF-36 for the whole cohort.
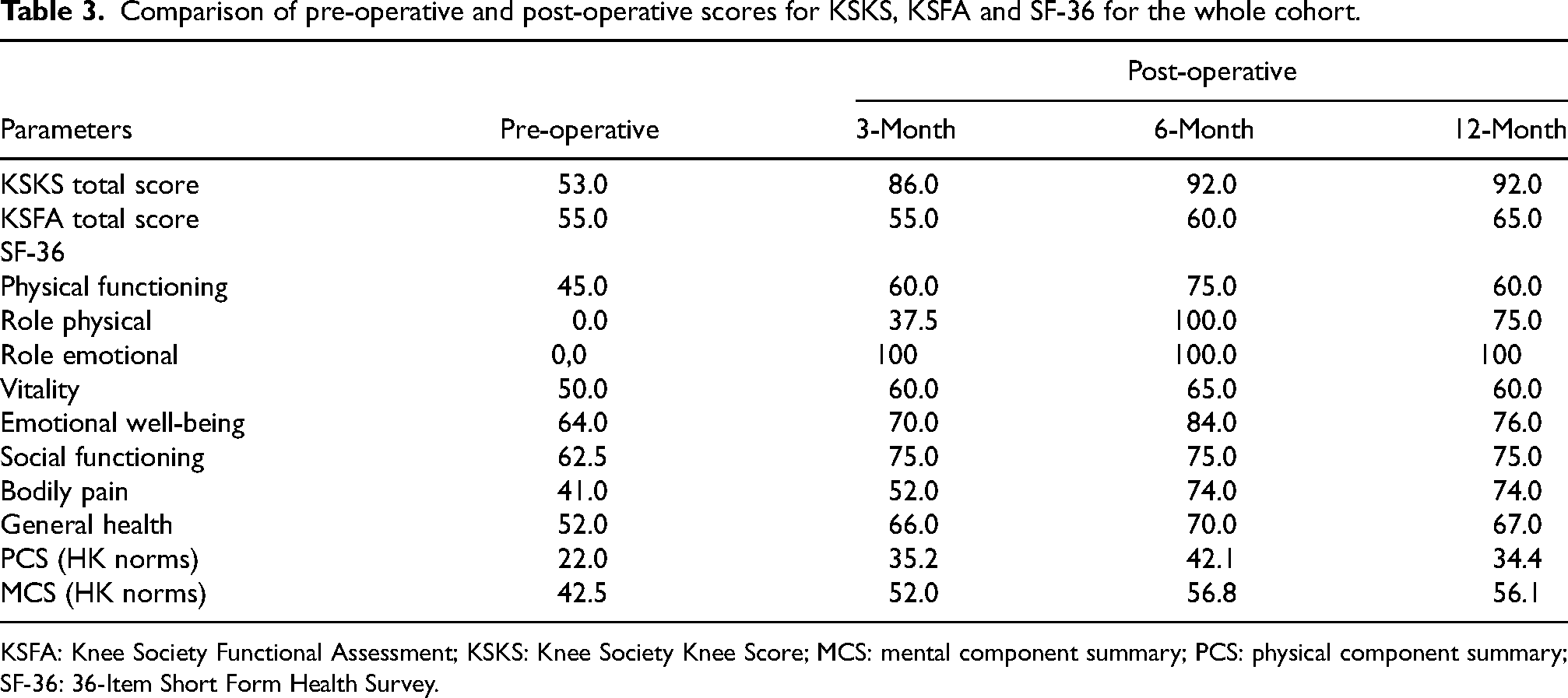
KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; SF-36: 36-Item Short Form Health Survey.
TKR versus UKR
When comparing outcomes of UKR and TKR, greater gains in KSKS were observed for TKR compared to UKR at all time points after surgery. This pattern was not observed for KSFA scores after surgery.
For TKR patients, gain in KSKS was maximal in the first 3 months after surgery, with further gains achieved up to 12 months post-operation. However, there was only a gain of 5 additional points from 3 to 12 months scores. However, for UKR, a gain of a further 10 points was seen from 3 to 12 months post-operation (Table 4).
Correlations of baseline parameters with changes of KSKS, KSFA and SF-36 scores whole cohort.
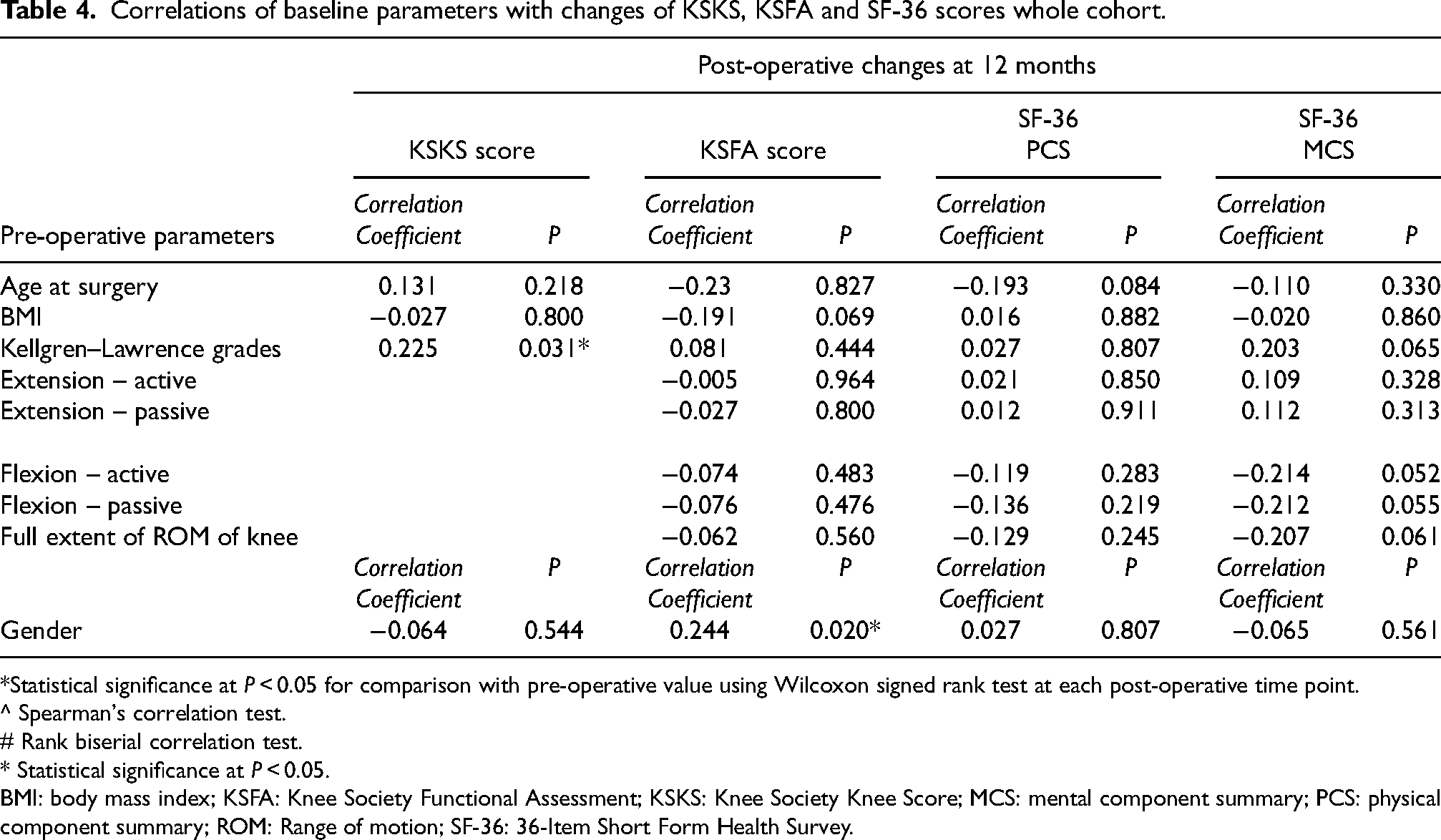
*Statistical significance at P < 0.05 for comparison with pre-operative value using Wilcoxon signed rank test at each post-operative time point.
^ Spearman's correlation test.
# Rank biserial correlation test.
* Statistical significance at P < 0.05.
BMI: body mass index; KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; ROM: Range of motion; SF-36: 36-Item Short Form Health Survey.
For KSFA scores, both UKR and TKR patients were able to achieve improvements compared to the baseline by 6 months post-operation, however, more functional gains were achieved in UKR patients compared to TKR patients. UKR patient function plateaued off at 6 months post-operation whereas continued improved was noted in the TKR group up to 1 year post-operation (Table 4). However, in comparing the significance of the surgical outcomes between UKR and TKR, UKR were shown to have statistically better outcomes at 6 months.
Male versus female
No significant difference was noted in terms of gain in KSKS and SF-36 PCS and MCS levels at all time points between males and females. However, it was noted that gains in KSFA were significantly greater in males compared to females at 6 and 12 months post-operation (Table 5).
Patient characteristics at baseline pre-operatively: TKR versus UKR.
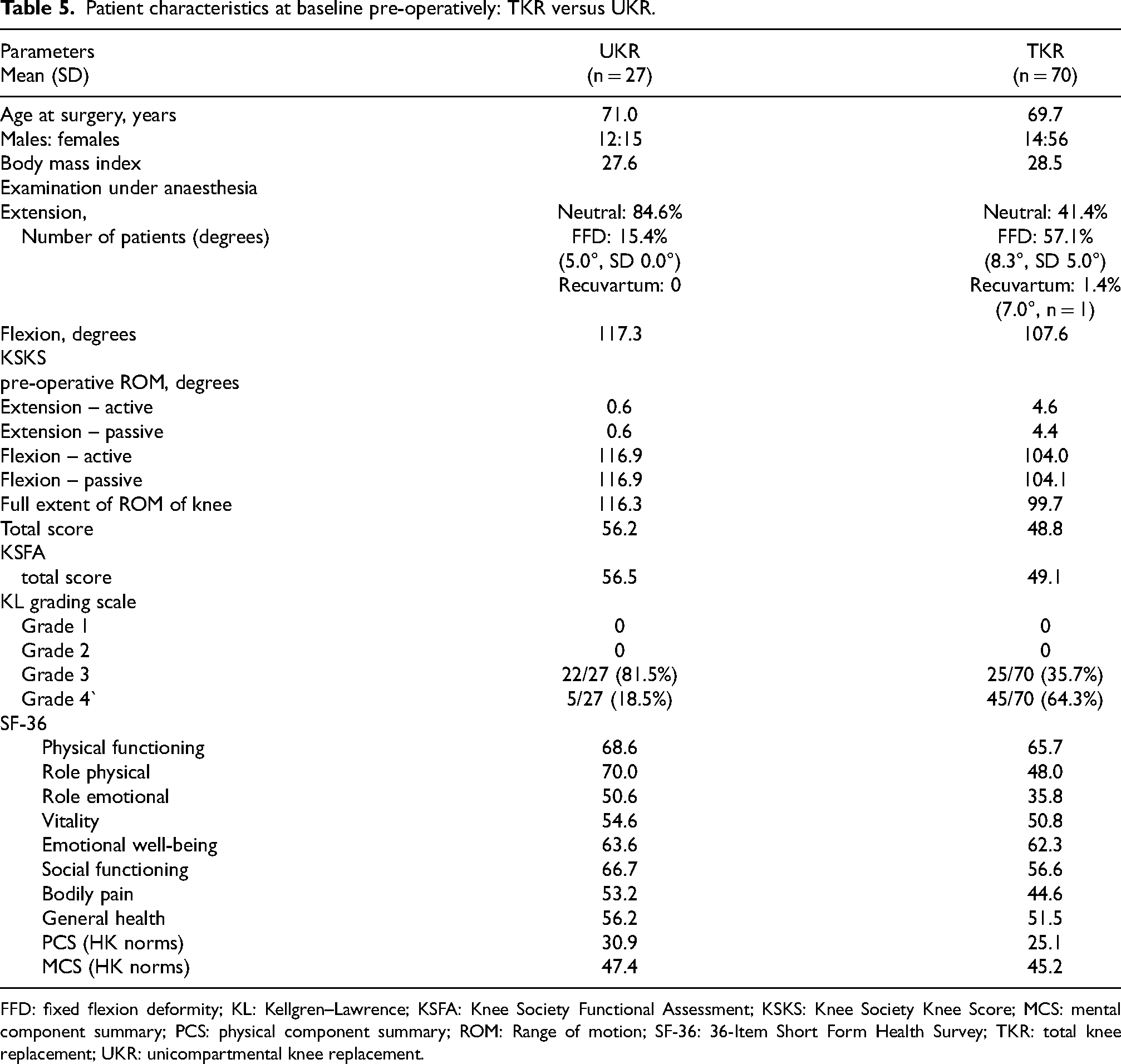
FFD: fixed flexion deformity; KL: Kellgren–Lawrence; KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; ROM: Range of motion; SF-36: 36-Item Short Form Health Survey; TKR: total knee replacement; UKR: unicompartmental knee replacement.
Severity of osteoarthritis
Improvements in KSKS, KSFA and SF-36 scores for patients with KL grades 3 and 4 at the time of operation were observed at all time points post-operation, with the most significant changes occurring with the KSKS scores at 6 and 12 months (Tables 6a and b). Notably, patients with KL grade 4 at the time of operation were found to have greater pains in KSKS at 6 and 12 months post-operation compared to that for KL grade 3 patients.
Pre-operative and post-operative scores for KSKS, KSFA and SF-36 comparing UKR and TKR.
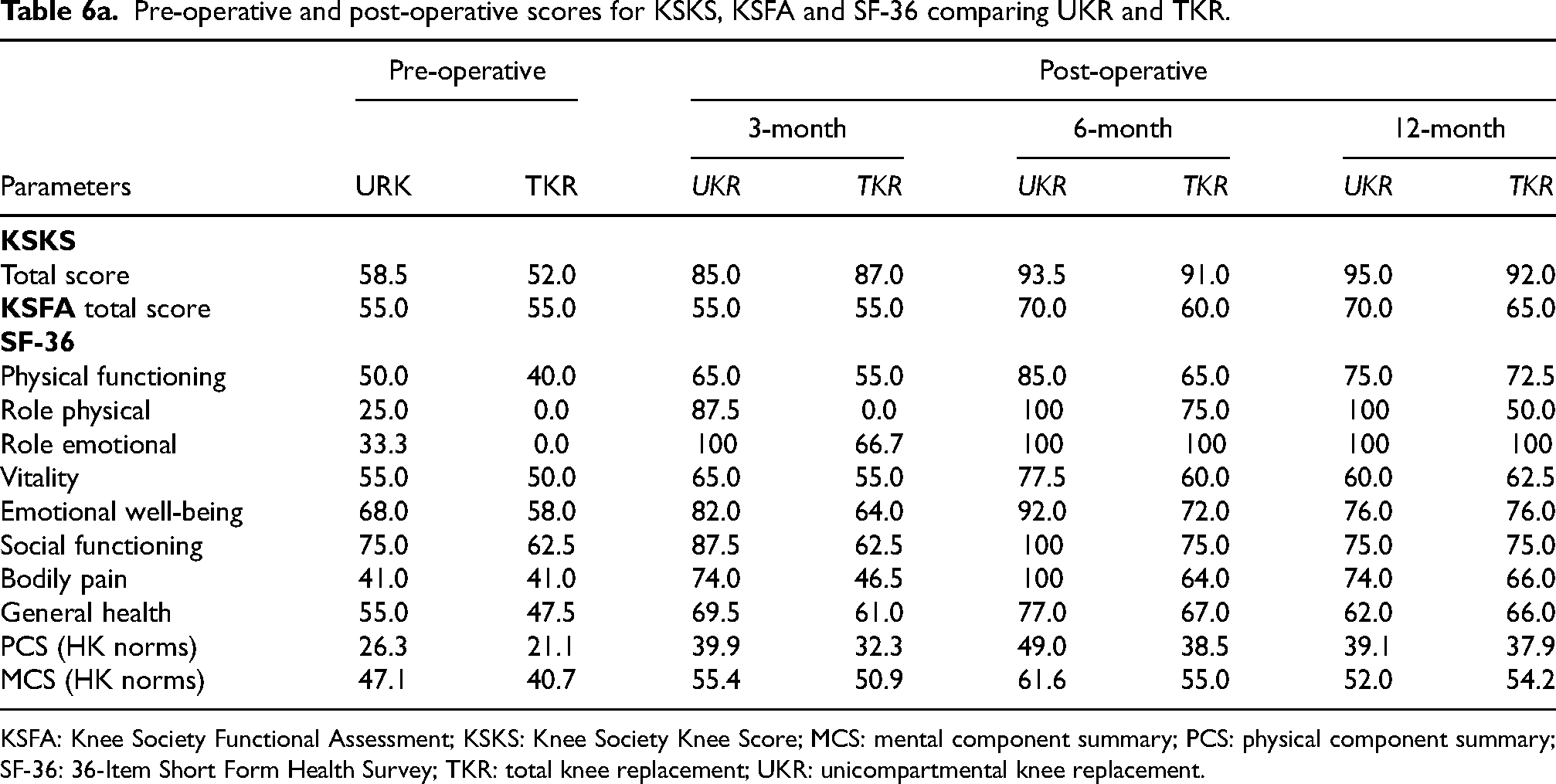
KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; SF-36: 36-Item Short Form Health Survey; TKR: total knee replacement; UKR: unicompartmental knee replacement.
Comparison of surgical outcomes between UKR and TKR surgeries.
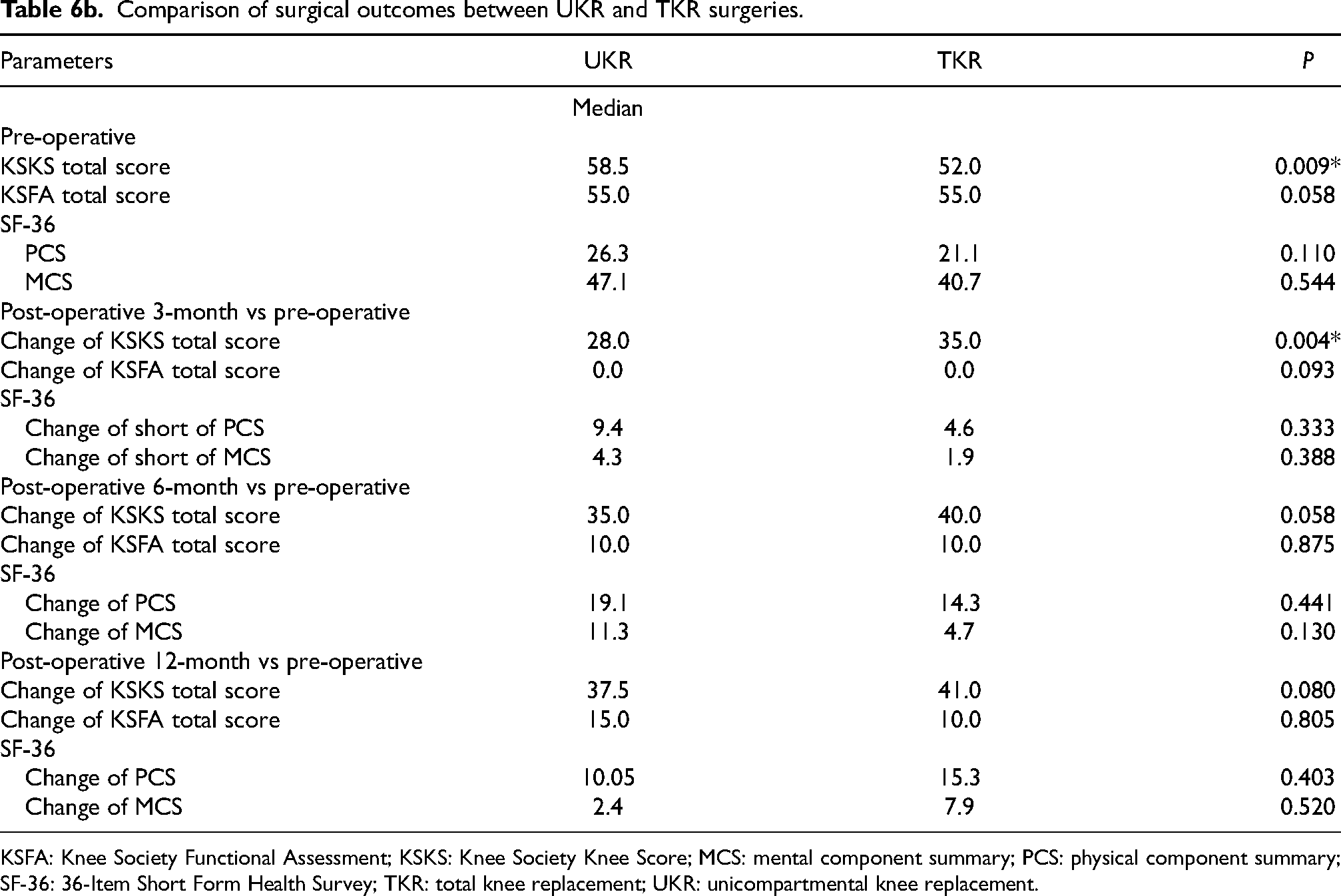
KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; SF-36: 36-Item Short Form Health Survey; TKR: total knee replacement; UKR: unicompartmental knee replacement.
Effect of age and BMI
No significant correlation was found between patient's age or BMI at the time of operation with SF-36 PCS and MCS (Table 7).
Comparison of outcome measures between gender.
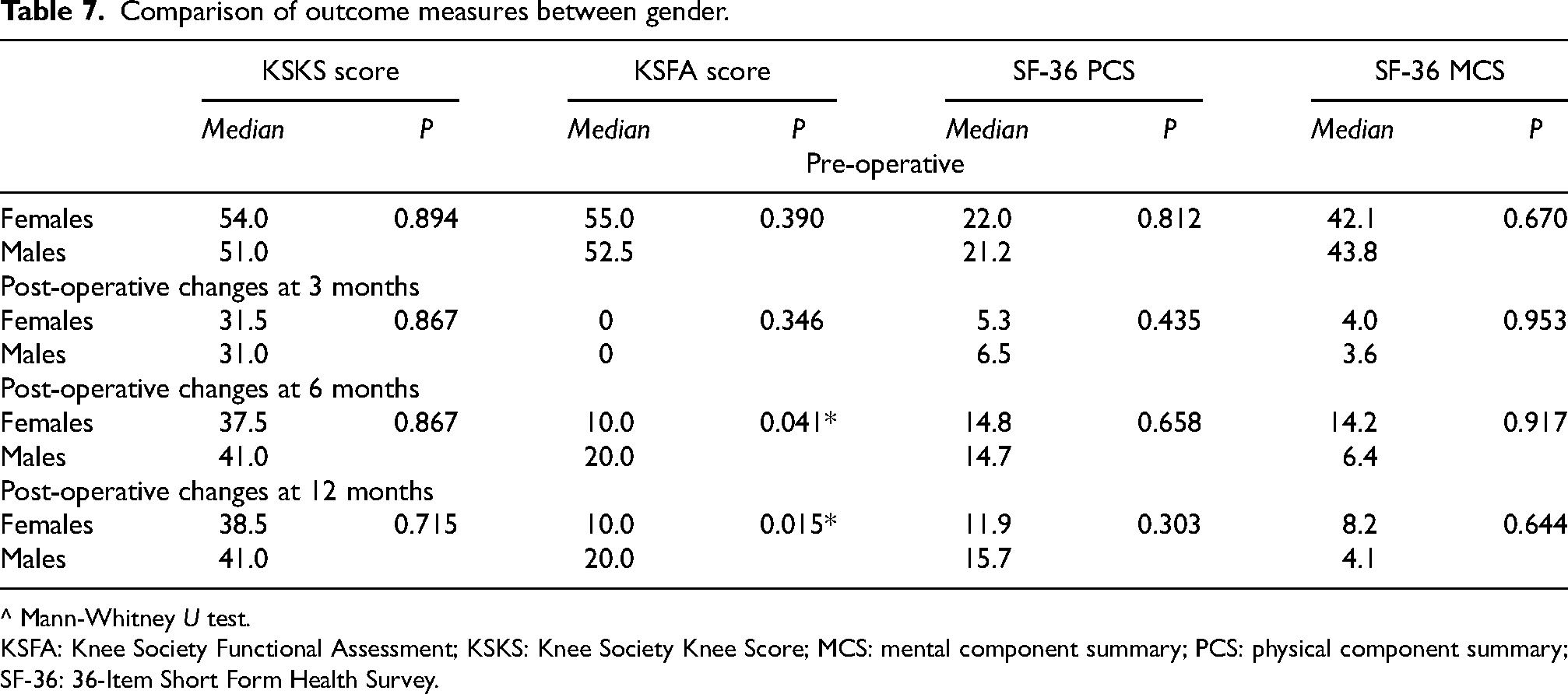
^ Mann-Whitney U test.
KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; SF-36: 36-Item Short Form Health Survey.
Discussion
TKR surgery is an effective treatment modality for treatment of end-stage arthritis of the knee. Currently, in the public health sector of Hong Kong, there is a long waiting list for joint replacement surgery which is the result of both the aging population and limitation in resources.
Our analysis revealed notable differences between men and women regarding recovery and perceived benefits from TKR. Specifically, men exhibited significant improvements in their KSFA scores at both the 6- and 12-month follow-up assessments compared to their female counterparts (Table 5). Current literatures have noted that men seem to benefit more from knee replacement surgeries than women in particular scores related to mobility and pain.12,13 However, it is also noted that women tend to delay consideration for TKR, which may further worsen their pain and disability prior to the surgery.12–14 In our study, female patients tended to be older in comparison to their male counterparts and they tend to score lower in the SF-36 in their pre-operation assessment especially in the sections for social functioning and role emotion. This suggests that male patients may experience a more favourable recovery trajectory following TKR and UKR, potentially reflecting differences in pain perception, physical resilience or rehabilitation engagement.12–15 These findings highlight the importance of considering gender-specific factors in the recovery process, as they may influence outcomes and the overall effectiveness of TKR interventions.
Patients undergoing UKR generally exhibit superior functional ability compared to those undergoing TKR, as demonstrated in our data, particularly in the KSKS total scores (Table 8; Figure 2) before surgery. This aligns with the broader literature, which often reports better baseline functional scores in UKR candidates. Notably, the differences in functional ability between the two groups become more pronounced after the 6-month mark, with UKR patients demonstrating superior SF-36 and KSFA. This delayed divergence could be attributed to the time required for TKR patients to adapt to the altered joint biomechanics and regain strength and mobility.16–19 In contrast, UKR patients might experience a smoother rehabilitation process due to the retention of more natural knee mechanics.16–19 Furthermore, the improved scores in UKR patients may also reflect the selection criteria for the procedure, as candidates for UKR often have better pre-operative functional status and less advanced joint disease.
Comparison of surgical outcomes between severity of osteoarthritis based on KL grading scales.
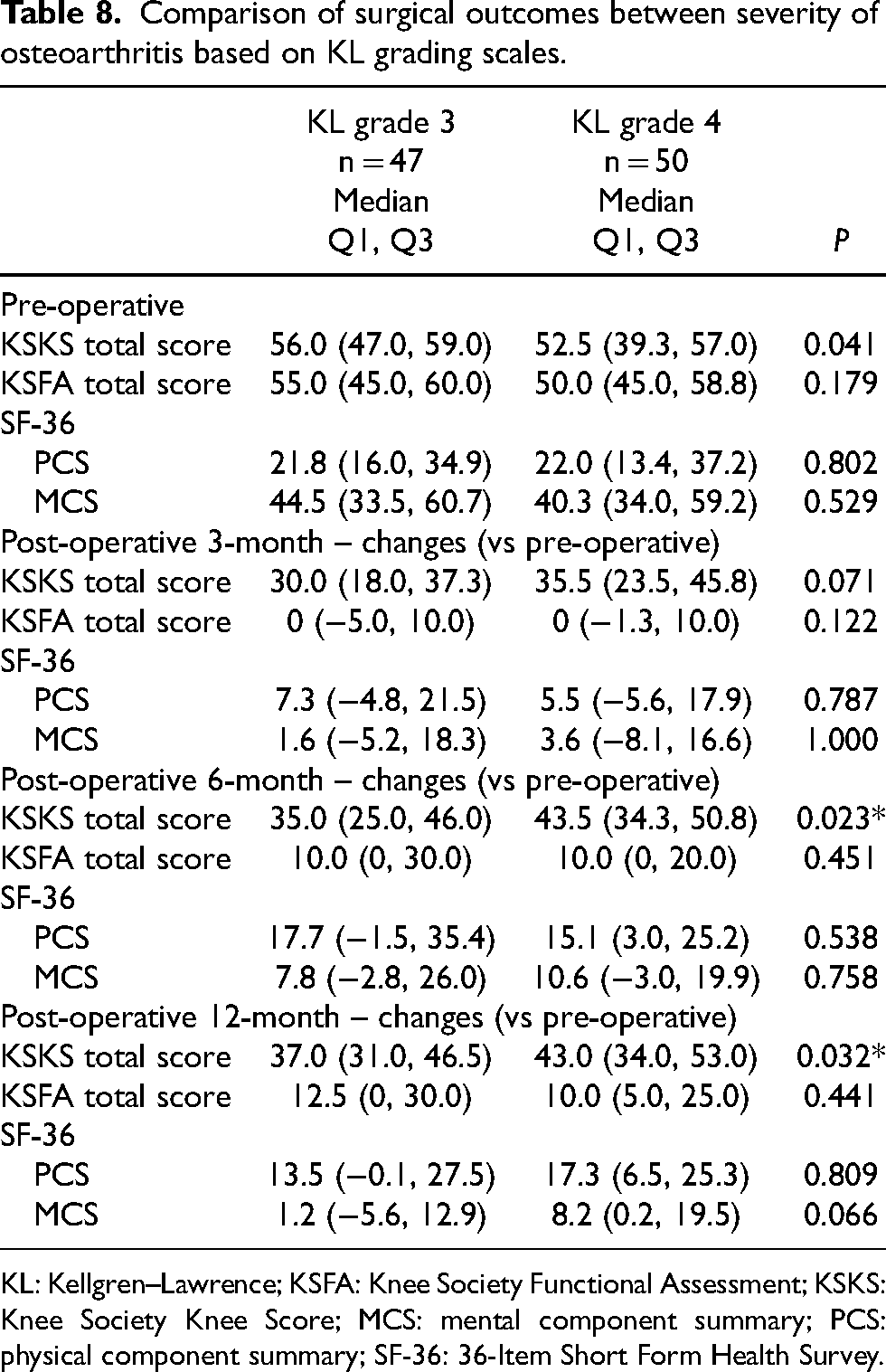
KL: Kellgren–Lawrence; KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; SF-36: 36-Item Short Form Health Survey.
When comparing TKR and UKR, it was noted that UKR has a slightly more favourable outcome especially during the initial post-operative period, while longer-term outcomes were similar. UKR patients gained better recovery than those in the TKR in respects to post-operative knee function, physical health and less pain.16–19 This difference has been well established in the literature and is related to the nature of the UKR procedure where only a single compartment is replaced, and the cruciate ligaments are protected. This minimises the changes in the patient's knee biomechanics, allowing for improved recovery. 16
Another notable finding was that the KSKS scores peaked at 6 months then plateaued by 12 months; whereas the KSFA scores continued to improve until 12 months. This aligns with common patterns observed in post-operative recovery, where pain relief and basic joint mechanics improve relatively quickly, while functional recovery continues for a longer period due to the demands of strengthening, endurance and adaptability. 13 With this data, surgeons can pre-empt patients to understand the stages of recovery in TKR that can be split into two; from 0 to 6 months, the recover focus is pain and swelling control and achieving a ROM of 0 to 110’; and from post-operation 6 months onwards, the rehabilitation focus will be on strengthening and hardening.
In this study, an initial improvement in SF-36 scores for vitality and emotional well-being was observed at 6 months post-operation, followed by a decline at 12 months (Table 9). This pattern may suggest that the early post-operative period provides patients with a sense of relief and optimism, likely driven by improvements in physical function and mobility. However, the subsequent decline at 12 months could indicate that the initial psychological and emotional gains are not sustained in the long term. Studies have shown that knee replacement itself may substantially relieve specific complaints and symptoms but may not enhance all aspects of health. 12 As TKR is associated with a degenerative disease, patients may experience more than one degenerative problem (e.g. low back pain/spinal stenosis), which may also add to the mental stress due to the physical limitation and ageing. Patient may also perceive their ability to be higher and as such, their expectation on themselves were much higher; therefore, they become less satisfied with their performance and quality of life. This trend underscores the importance of addressing long-term psychological and emotional support alongside physical rehabilitation in post-operative care.14,15 Further investigation is needed to identify specific causes for this decline and to develop interventions to support sustained emotional and mental well-being.
Comparison of pre-operative and post-operative range of motion, scores of KSKS, KSFA and SF-36 whole study cohort.
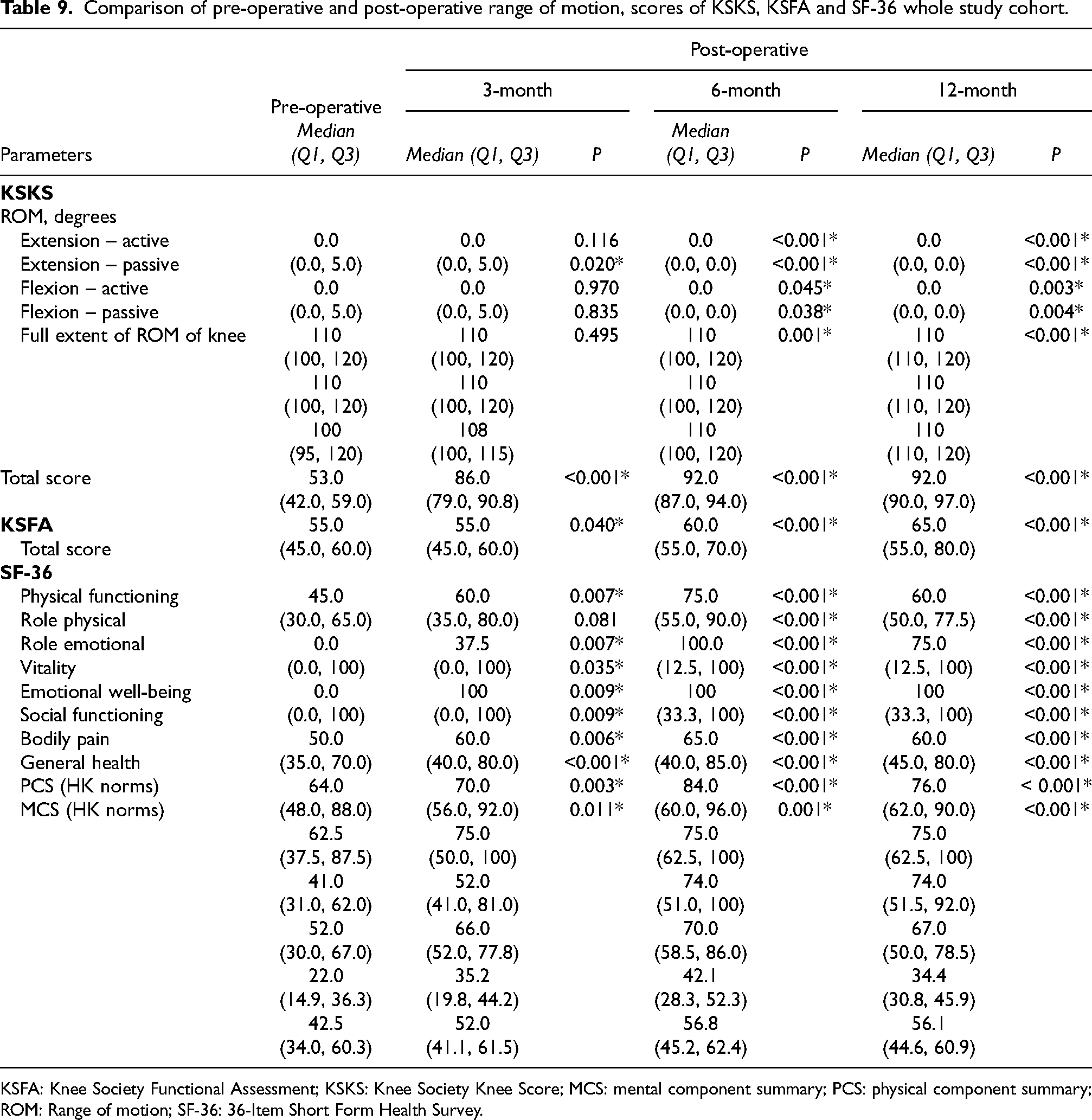
KSFA: Knee Society Functional Assessment; KSKS: Knee Society Knee Score; MCS: mental component summary; PCS: physical component summary; ROM: Range of motion; SF-36: 36-Item Short Form Health Survey.
Our findings include KSKS score of 53.5 being defined as the threshold value in prediction of success after surgery, with a sensitivity of 69% and specificity of 65%. This is the first study conducted in patients in Hong Kong attempting to define a predictor of success after knee replacement for our local population. This is of particular importance as in the public sector in Hong Kong, patients often need to wait for years for knee replacement. This population specific value can help clinicians to better select patients to be placed on waiting list for surgery and may even serve as a means of streamlining the waiting list process. This value is also very useful for pre-operative counselling and for management of patient's expectations before and after surgery.
With further study with a larger cohort size, a better threshold value can be refined with better sensitivity and specificity that can guide clinicians to create a better management protocol to cater to an ever-increasing demand for TKR.
This study shows that patient satisfaction with TKR is influenced by multiple factors. While group-level statistical improvements in outcomes may be significant, they do not always equate to satisfaction for each individual patient. Various personal, clinical and psychological factors contribute to how patients perceive their success with the procedure. However, we can note the overall improvement in quality of life for patients who underwent TKR with the maximum benefit occurring 6 months post-operatively.
Limitations
Our study is limited in the following areas. First, our sample size is relatively small for a retrospective 6 years, single centre cohort. Despite a small sample size, we noted some promising patterns in some of our parameters including the influence of BMI and different KL scores affecting the outcome of TKR that further study can illicit. Secondly, our study population contained those who underwent TKR and some who underwent UKR. Recently literature has shown that patients benefited more from UKR than TKR and those who underwent UKR had better functional scores including WOMAC, SF-36 and Oxford knee scores.12,13 As a result, this may have skewed our data. With a larger population, we would have been able to analyse the two groups separately and also make a comparison between the two; thereby giving us a clearer picture of the HRQoL improvements for each management.
Footnotes
List of Abbreviations
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the Ethics Committee of the University of Hong Kong / Hospital Authority Hong Kong West Institutional Review Board (HKU/HA HKW IRB).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.