
Abstract
Objective
To determine the characteristics of ultrasonographic abnormalities findings of shoulders in persons with spinal cord injury (SCI) in a 5-year interval.
Methods
Persons with SCI who attended the rehabilitation clinic, Srinagarind hospital were evaluated the baseline characteristic, physical examinations and the ultrasonography of both shoulders. Prevalence of abnormal shoulder ultrasonographic findings was compared between baseline and 5-year following study.
Results
Out of 91 SCI participants, 52 individuals were enrolled in the study (57%, 27 in persons with a paraplegia and 25 in persons with a tetraplegia). Most of the participants had incomplete SCI and used wheelchair for mobility. The prevalence of shoulder pain in persons with SCI was 19.2% (10/52). In 5-year interval, the prevalence of biceps tendon effusion and supraspinatus tendinosis was increased significantly (p = 0.004, p < 0.001), respectively, while the prevalence of subdeltoid-subacromial bursitis was decreased significantly (p = 0.018). In persons with paraplegic group, the prevalence of supraspinatus tendinosis was increased whereas the prevalence of the subdeltoid-subacromial bursitis was decreased significantly (p < 0.001, p = 0.035) accordingly. In persons with tetraplegic group, the prevalence of biceps tendon effusion was increased significantly (p = 0.013). The prevalence of abnormal shoulder ultrasound findings in persons with SCI compared between baseline and 5-year following study was increased significantly (p = 0.002).
Conclusion
In 5-year interval, the study shows progression of abnormal shoulder ultrasound findings in persons with SCI. The prevalence of biceps tendon effusion and supraspinatus tendinosis was significantly increased.
Introduction
Spinal cord injury (SCI) is a condition in which the spinal cord was damaged resulting in alteration of neurological function such as weakness, numbness and spasticity. The persons with SCI have an increased demand for upper extremities for many activities, for example, transferring in and out of wheelchair, wheelchair propelling, performing daily activities living. 1 However, the shoulder is not plotted to be used in these types of tasks. The repetitive use of both shoulders increases intra-articular pressure which risk for development of shoulder pain. 2 In addition, the shoulder muscle imbalance which are causing by relative muscle weakness of the humeral head rotators and adductors and shortening of antagonists to the weak muscles are believed to have a major role in the development of shoulder pain.2,3
Shoulder pain is common in persons with SCI with the report of 39.8–70%.4–7 The risk factors that are highly associated with shoulder pain are older age, longer time since injury, higher level of SCI, the completeness of the injury and manual wheelchair ambulatory.5–9 The shoulder pain is found to develop in the first 6 months after the onset of injury and 35% continue having the pain up to 18 weeks results in limitation of patient's functional activities.10,11 In addition, the increased musculoskeletal pain was strongly associated with maladaptive psychosocial behaviors of pain catastrophizing and kinesiophobia leading to a reduction and limitation of activity. 12 The persons with shoulder pain also showed significantly lower perceived health and higher depressive scores than those without shoulder pain. 13
The history and physical examination including the special tests of the shoulders take a major part in identifying the source of the pain. However, special tests may lack sensitivity and not be able to diagnose and differentiate between pathologies.14,15 Several diagnostic tools can be great help in identifying shoulder abnormalities. Musculoskeletal ultrasound (MSK US) is also widely used because it is non-invasive, inexpensive, portable and allows both static and dynamic assessment of shoulder structures. The MSK US can also identify the presence of ultrasonographic abnormalities in patients with negative clinical special tests.16,17 Moreover, some systematic review and meta-analysis studies show that the accuracy of MSK US is similar to MRI in diagnostic of full-thickness rotator cuff tears.18–20
Regarding to the literature reviews which involved shoulder MSK US in persons with SCI, Ninomyia et al. found that 87.5% of the persons with SCI presented changes in at least one of the structures assessed by MSK US. It was found that tendons of the rotator cuff muscle especially the subscapularis muscle tendon and the long head of the biceps were the most frequently injured structures. 21 Kivimaki et al. also found that wear and tear changes of the glenohumeral joint appear to be more frequent in subjects with SCI than in able-bodies. 22 The study of Sirasaporn et al. found that the most common ultrasonographic abnormalities in persons with SCI were unilateral subdeltoid-subacromion bursitis. 23
The previously published studies were assessed only one time point and no clinical follow-up. Therefore, it could not determine whether the shoulders would remain either abnormality or normality. Moreover, the most of shoulder pain and pathology is found to be increased with time after SCI.8,9 To the best of our knowledge, there is no previous published studies which followed-up MSK US of the shoulders in persons with SCI in a 5-year interval. The objective of the study is to determine the prevalence of ultrasonographic abnormalities findings of shoulders in persons with SCI in a 5-year interval.
Materials and methods
Study design and participants
This cohort study was conducted from 2018 to 2023. The participants were persons with SCI who attended a rehabilitation clinic, the Srinagarind hospital, Khon Kaen, Thailand. Inclusion criteria were age over 18 years old and had a history of SCI longer than 6 months. Exclusion criteria were history of traumatic injury to either side of the shoulder, history of shoulder surgery on either side of the shoulder joint, inability to cooperate during the examination, inability to sit in a wheelchair for more than 30 min
This study was approved by the Khon Kaen University Ethics Committee for Human Research (HE641303). Written informed consent was obtained from all participants.
Methods
All subjects were assessed their clinical and ultrasonographic examination of both shoulders. The informed consent was obtained beforehand. The information about their demographic data including age, weight, underlying disease, neurological level, American spinal injury association classification (ASIA), duration of SCI, activity of daily living (ADL), and transfer were collected. If persons with SCI have shoulder pain, they will be evaluated the site, duration and the severity of shoulder pain by numerical rating scale which classified 0 as no pain and 10 as worst pain ever experienced. All of information was obtained by a physician who was not a musculoskeletal ultrasonographic examiner.
The subjects then were examined both shoulders to identify the area of maximal tenderness by palpating the anterior, posterior, medial and lateral site of shoulder. Both passive and active ranges of motion were tested. The physical examination of the shoulder was obtained by performed specific shoulder examination included the biceps tendon, the supraspinatus tendon, the acromioclavicular joint, the Neer sign, the Hawkins–Kennedy impingement sign, the painful arc, the empty can test, the resisted external rotation, the resisted internal rotation, the O’Brien test for the labrum and the O’Brien test for the acromioclavicular joint.8,24 Each test will be reported as negative or positive results.
The musculoskeletal ultrasound
The MSK US was performed on both shoulders by a specialist in rehabilitation medicine who was experienced in musculoskeletal ultrasonography and was blinded to the clinical assessment. Ultrasonography is performed in a standard manner22,23,25 with LOGIQ e and using 9 to 14 Hz linear transducer for collect images. During the ultrasonographic examination, participants were made to sit straight by a wheelchair or a chair. The data gathered included assessments of the biceps tendon, supraspinatus tendon, subdeltoid bursa, subscapularis tendon, infraspinatus tendon, acromioclavicular joint and glenohumeral joint. The interpretation of ultrasonographic abnormalities were based on international guidelines of the outcome measures in rheumatology (OMERACT 7).
26
The sequence of ultrasonographic examination as follows.
23
(Figure 1)
The biceps tendon was evaluated with the transducer kept in horizontally and vertically at the level of the bicipital groove. The standard posture is elbow flexion 90 degree and forearm supination. The abnormal results were classified as effusion, partial rupture and full rupture. The subscapularis tendon was evaluated with the transducer kept in horizontally at the level of the bicipital groove. The standard posture is elbow flexion 90 degrees forearm supination and external rotation for 10 degree. The abnormal results were classified as tendinosis, partial tear, full tear and calcification. The acromioclavicular joint was evaluated with the transducer kept in horizontally above the acromioclavicular joint. The abnormal results were classified as calcification, synovial hypertrophy and effusion. The supraspinatus tendon was evaluated with the transducer kept in short and long axis at the greater tuberosity. The standard posture was modified crass position. The abnormal results were classified as tendinosis, partial rupture, full rupture and calcification. The subdeltoid-subacromial bursa was evaluated the same as the supraspinatus tendon. The abnormal result was bursitis if the bursa has hypoechoic thickness more than 2 mm. The infraspinatus tendon was evaluated with the transducer kept in long axis at the greater tuberosity. The standard posture was the arm placed on the opposite shoulder. The abnormal results were classified as tendinosis, calcification and partial rupture The glenohumeral joint was evaluated with the transducer kept in short axis at the posterior glenohumeral joint. The standard posture was the arm placed on the opposite shoulder. The abnormal results were classified as calcification, irregularity of joint margin and effusion. The dynamic supraspinatus impingement test was evaluated with the transducer kept in horizontally lateral to acromion. The examiner gentle elevate the arm in abduction position. The results were classified as negative, positive and not testable.
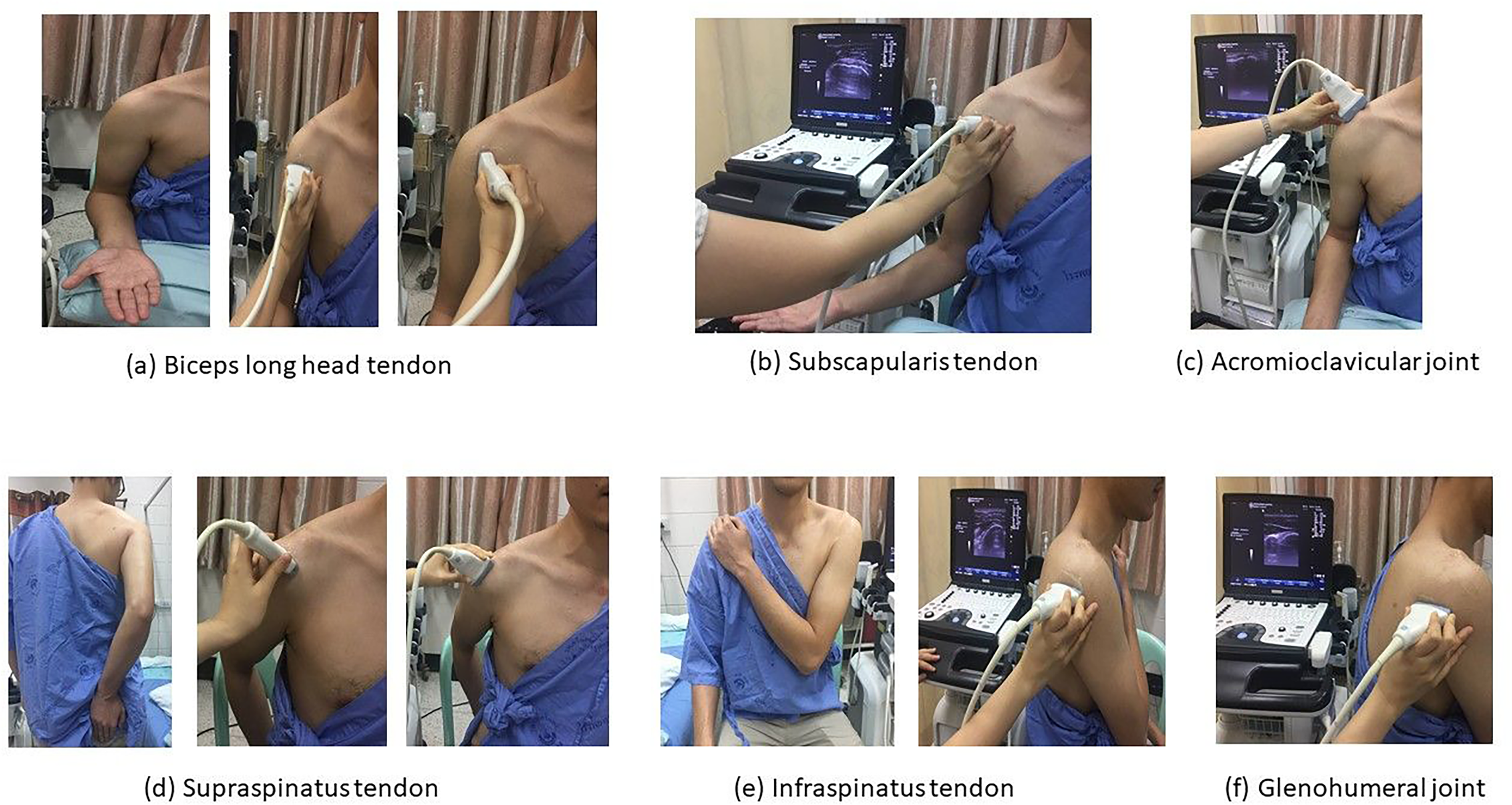
Musculoskeletal ultrasound.
Statistical analysis
All statistical analyses were performed using SPSS 19.0 (IBM SPSS statistics Version 19). The continuous data were presented as mean and standard deviation. The ordinal data were shown as frequency and percentage. Prevalence of the shoulder ultrasonographic abnormalities at baseline and 5 years was presented as a percentage. The prevalence of the abnormal ultrasonographic findings at baseline and 5-year follow-up study were compared by McNemar's test. Data from all participants were analyzed according to data being available. No imputation was implemented to missing data.
Results
Out of 91 SCI participants, 39 subjects dropped out: 2 died and 37 were lost to follow-up. The number of completed participants were 52 (57.1%), out of whom 27 (52%) were persons with a paraplegia and 25 (48%) were persons with a tetraplegia. Regarding to 5-year interval, in both persons with paraplegic and tetraplegic groups, most of the participants were male. The mean age of persons with paraplegic group was 50 ± 18.9 years while in persons with tetraplegic group was 46.9 ± 13.7 years. The average body mass index was 23.3 ± 5.0 kg/m2 and 21.4 ± 3.8 kg/m2 in persons with paraplegic and in persons with tetraplegic groups respectively. The duration of the SCI in persons with paraplegic group was 11.2 ± 4.9 years and in persons with tetraplegic group was 10.3 ± 5.2 years. The majority of the participants in both groups had incomplete injuries, independent in ADL, transferring and used wheelchair for mobility. (Table 1)
Baseline characteristics.
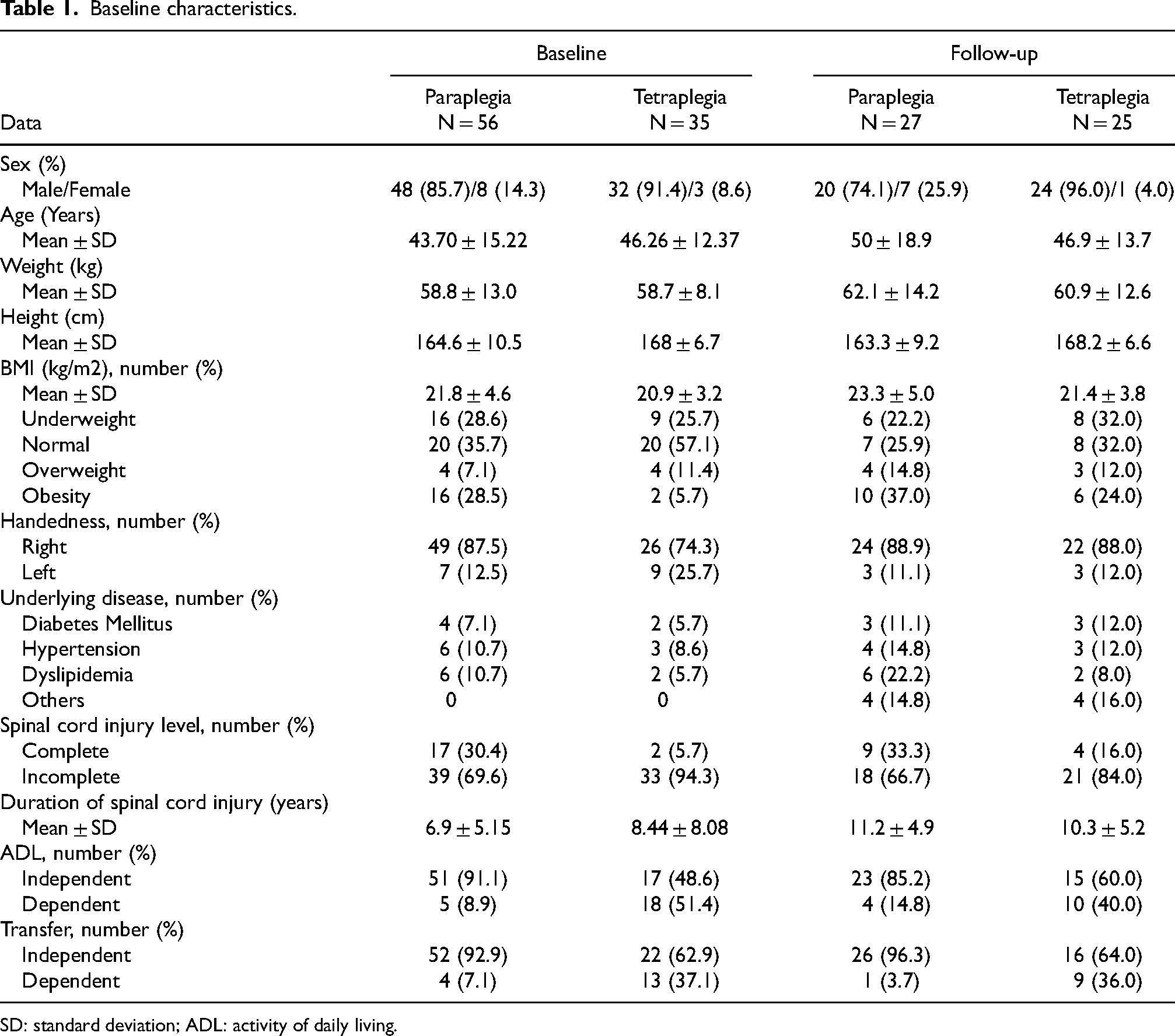
SD: standard deviation; ADL: activity of daily living.
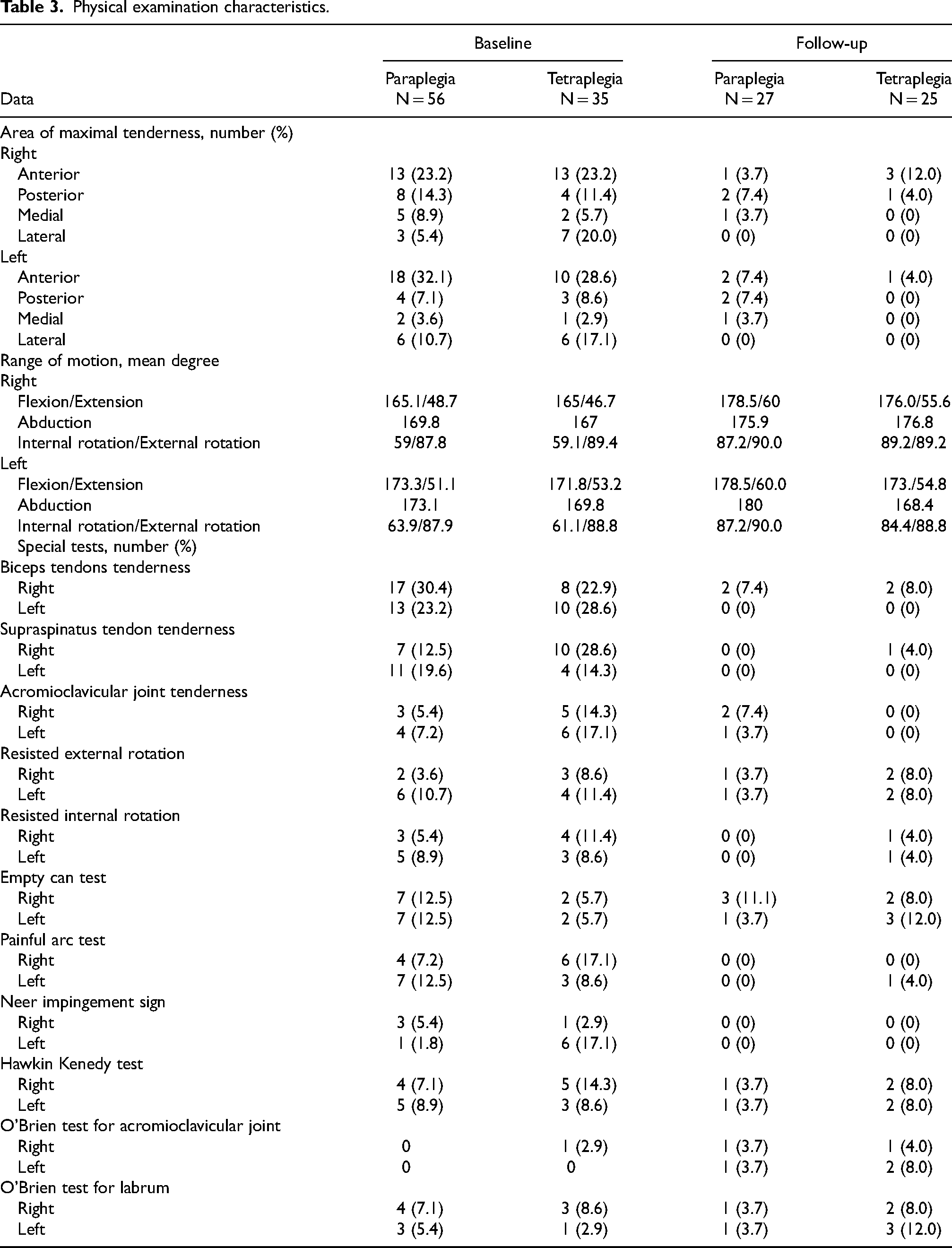
At baseline, 28 of 91 participants had shoulder pain (30.8%), 14 (25%) in persons with paraplegic group and 14 (40%) in persons with tetraplegic group. Mean duration of shoulder pain was 19.5 ± 32.4 in persons with paraplegic group and 37.7 ± 37.8 months in persons with tetraplegic group. The most common area of maximal tenderness in both groups was anterior region (55.3% in persons with paraplegic group, 51.8% in persons with tetraplegic group). The most common positive findings of shoulder special test in both groups were biceps tendon tenderness (53.6% in paraplegic group, 51.5% in tetraplegic group). In the follow-up study (5 years interval), a total of 19.2% (10/52) of the participants complained shoulder pain, 4 (14.8%) in persons with paraplegic group and 6 (24%) in persons with tetraplegic group, mostly on right side in both groups. Mean duration of shoulder pain was 1.6 ± 5.1 months in persons with paraplegic group and 2.4 ± 7.3 months in persons with tetraplegic group. The most common maximal tenderness shoulder area was posterior region (14.8%) in persons with paraplegic group and anterior region (16%) in persons with tetraplegic group. The most common positive findings of shoulder special test in paraplegic group were empty can test (14.8%) while in persons with tetraplegic group was empty can test and O’Brien test for labrum (20%). Other shoulder pain characteristics and physical examination are summarized in Tables 2 and 3.
Shoulder pain characteristics.
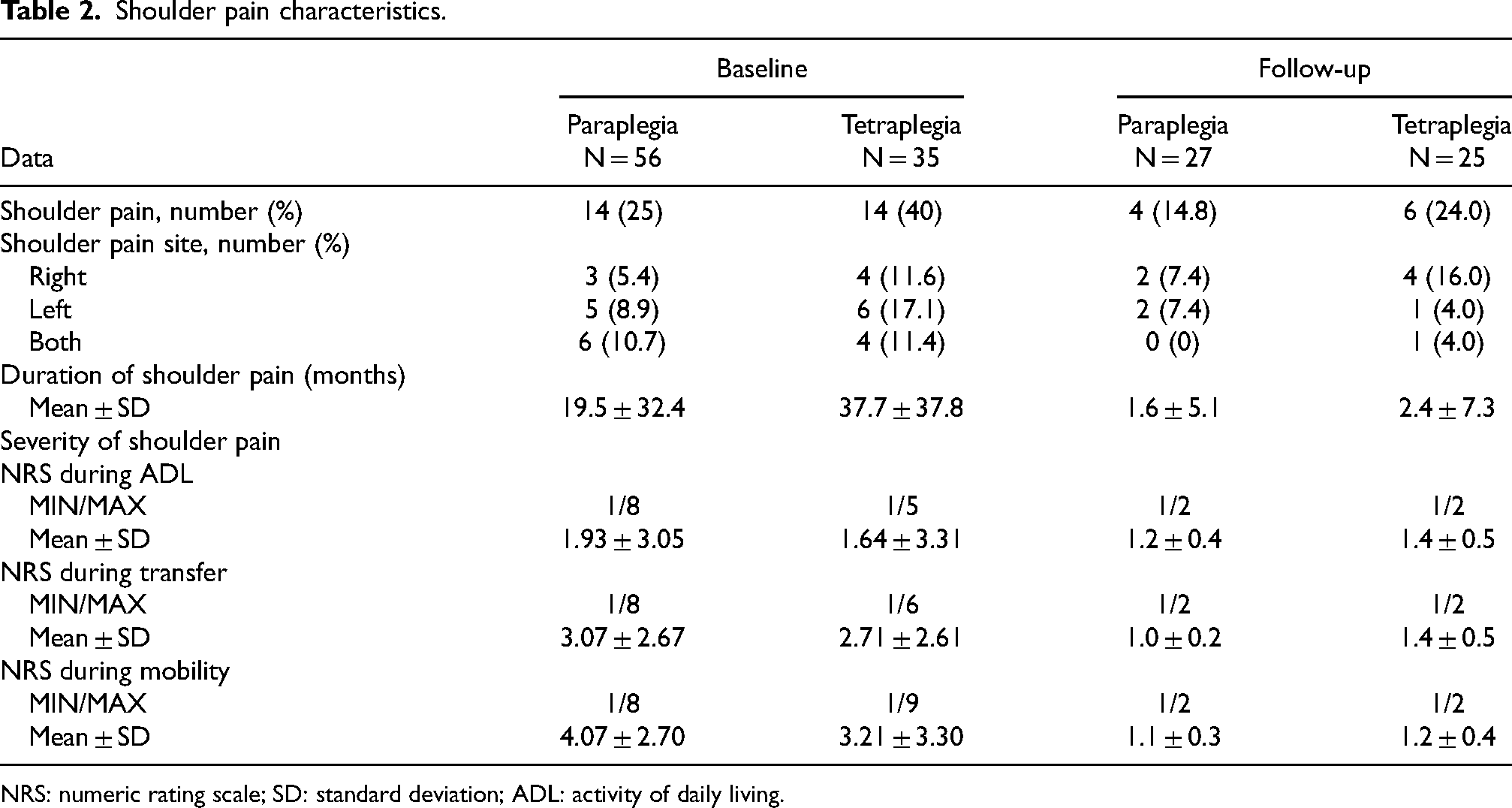
NRS: numeric rating scale; SD: standard deviation; ADL: activity of daily living.
Physical examination characteristics.
From the baseline, the top three abnormalities were subdeltoid-subacromial bursitis (28.8%), biceps tendon effusion (20.2%) and supraspinatus tendinosis (20.2%). In the 5-year interval following, the top three abnormalities were supraspinatus tendinosis (50%), biceps tendon effusion (37.5%) and positive dynamic supraspinatus impingement (20.2%). Compared to baseline, the prevalence of biceps tendon effusion and supraspinatus tendinosis was increased significantly (p = 0.004, p < 0.001) while the prevalence of subdeltoid-subacromial bursitis was decreased significantly (p = 0.018) (Table 4).
Ultrasound findings.
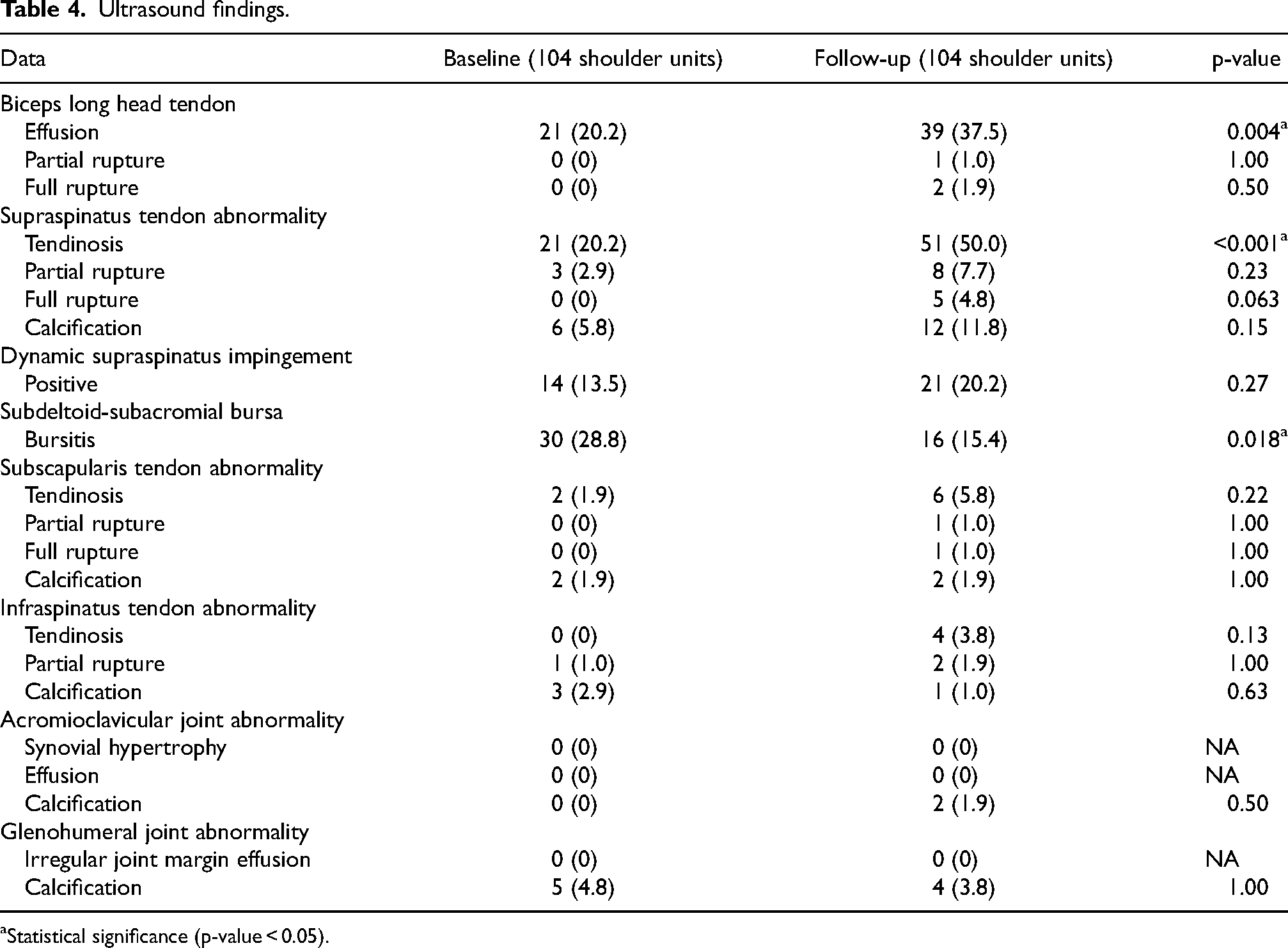
Statistical significance (p-value < 0.05).
According to table 5, ultrasound findings were categorized into two groups: tetraplegia and paraplegia. The biceps tendon effusion was increased in both groups but was significant in persons with tetraplegic group (p = 0.013), whereas the supraspinatus tendinosis was increased significantly in persons with paraplegic group (p < 0.001). The subdeltoid-subacromial bursitis was reduced in both groups with a significant difference in persons with paraplegic group (p = 0.035). The prevalence of abnormal ultrasound findings compared between baseline and 5-year following study was increased significantly (p = 0.002) (Table 6).
Ultrasound findings.
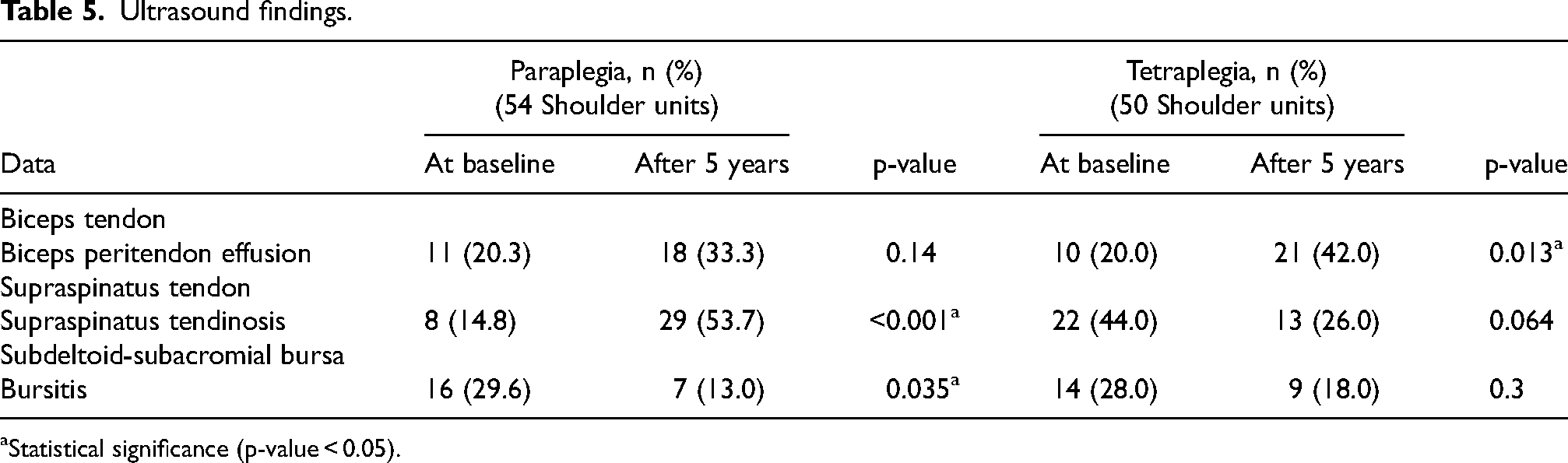
Statistical significance (p-value < 0.05).
Ultrasound findings.

Statistical significance (p-value < 0.05).
Discussion
In this study, we observed a decrease in the prevalence of shoulder pain when compared to their baseline. It was correlated with the study of Silverskiold and Waters 10 which also reported a decrease in shoulder pain within the persons with tetraplegic group at 6 to18 months follow-up. In addition, our study was similar to the previous research which noted that the decrease of prevalence of upper extremities pain usually occurs after the first 5 years’ onset of injury.7,27 We hypothesized that in our study, the most of persons with tetraplegic groups had complete lesion and reliance on caregiver assistance for routine activities. This increased dependency may result in reduced usage of upper extremities, potentially leading to a lower prevalence of shoulder pain. Additionally, advanced age may further contribute to decreased activity levels, which could also be a factor in the decreased prevalence of shoulder pain observed. 27
The most common abnormal ultrasonographic findings in this study was supraspinatus tendinosis while at the baseline, the most common finding was subdeltoid-subacromial bursitis and the prevalence was increased significantly in persons with paraplegic group. It was in accordance with the study of Brose et al. and Alves et al. which found that the supraspinatus tendinosis was the most common abnormality imaging findings.8,28 Trevor et al. stated that as individuals with SCI had to perform ADL from a seated position in wheelchair despite the design of the environment for able-bodied, the repetition of arm elevation above the horizontal plane may increase the risk of supraspinatus tendon injury. 29 In this study, it was shown that most of persons with paraplegic group were independent in both ADL and transfer activity which leads to increased upper extremities usage.
The second most common abnormality found in this study is biceps tendon effusion which is the same as in the baseline and was increased significantly in persons with tetraplegic group. Kivinmaki et al. 22 demonstrated that the change in glenohumeral joint space in persons with SCI may cause biceps tendon effusion. Moreover, sonographic detected biceps tendon effusion was associated with rotator cuff pathologies such as subscapularis tendinopathy, subdeltoid bursitis, impingement syndrome and adhesive capsulitis.30,31 Recent study published in 2022, Omid et al. found that manual wheelchair users with SCI had progression of rotator cuff tendon pathology over 1 year which may represented as biceps tendon effusion in ultrasound findings. 32
On the other hand, the prevalence subdeltoid-subacromial bursitis was decreased significantly in 5-year interval. Farin et al. observed that the false-negative findings might occurred if the motions of the arm were restricted or if the bursa was adhesive and not distended with fluid. 33 In this study, it was possible that some participants had chronic subdeltoid-subacromial bursitis which no longer had inflammation and effusion resulting in normal ultrasonographic findings.
In addition, we also found that both symptomatic and asymptomatic shoulder had abnormal ultrasound findings. These results were consistent with those of previous studies.8,16,17,21 Only 2 of 11 shoulder units had normal ultrasound findings despite the shoulder pain. This may be caused by other musculoskeletal problems such as myofascial pain syndrome, overuse syndrome and degenerative joint disease. 29 On top of that, most of the participants had normal physical examination and special test but had abnormal ultrasound findings. This should be considered as physical examination alone may not be adequate for follow-up.
To our knowledge, this is the first study to explore the change in ultrasonographic findings of shoulder in persons with SCI over the 5-year period. There were limitations exist within this study. Firstly, our study had high percentage of drop out due to long-time follow-up and barriers to accessing health care services during the COVID-19 pandemic in Thailand. Secondly, this study focused on rotator cuff and non-rotator cuff lesion in shoulder region as mentioned. MSK US cannot be detected other causes of shoulder pain such as myofascial pain or neuropathic pain which can occur in persons with SCI. We hoped that the result of our study may help in providing program for preventing the shoulder complications in long-term care.
Conclusion
There is a progression of pathology in persons with SCI over 5-year interval. The prevalence of biceps tendon effusion and supraspinatus tendinosis was increased significantly.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was granted by the Faculty of Medicine Research Fund, Khon Kaen university [grant number IN65242].