
Abstract
Objective
To examine shoulder ultrasound imaging in both tetraplegic and paraplegic spinal cord injury (SCI) patients with shoulder pain.
Methods
All 28 individuals with SCI with shoulder pain were enrolled in this study. Fifty-six shoulders were evaluated by ultrasound (US) imaging.
Results
Fourteen tetraplegics and 14 paraplegics were enrolled (age 45.4 ± 13.8 years [mean ± SD]). Median time post-SCI was 8.6 years. Twenty-three individuals (82.1%) were independent in transfer and four individuals (14.3%) were partially independent in transfer. The prevalence of shoulder pain was 78.6% in manual wheelchair ambulators, 10.7% in gait aids users, 7.1% in wheelchair sitters, and 3.6% in no assistive device individuals. Abnormal US imaging was found in 24/28 (85.7%) individuals. Total shoulder US abnormalities were 38 units. Most common abnormal US imaging was supraspinatous tendinosis (42.1%), biceps tendon effusion (23.7%), positive dynamic supraspinatus impingement (21.1%), and subdeltoid bursitis (18.4%).
Conclusions
Shoulder ultrasonographic abnormalities were common in the patients with SCI with shoulder pain. The supraspinatus tendinosis is the most common abnormal US imaging in patients with SCI with shoulder pain.
Introduction
Patients with spinal cord injury (SCI) usually have neurological performance deficits which directly affects quality of life. The level of neurological symptoms is depend on the severity of SCI which can be categorized by the American Spinal Injury Association Impairment Scale (AIS) into tetraplegia and paraplegia. 1 The tetraplegic patients have poor muscle power and sensory deficits in both upper and lower limbs which directly disturbs the physical competency and functional autonomy. 2 The imbalance of shoulder muscle which can be caused by impairment in muscular strength and spasticity is one factor of shoulder pain in tetraplegic patients. 3 The paraplegic patients have to adapt their routine activities living by using the upper limbs for various type of weight-bearing tasks such as wheelchair ambulation and transferring.4,5 The shoulder is not invented for these type of activities which cause excessive overload on the shoulders which is a cause of shoulder pain in patients with paraplegic SCI. 6
Despite early rehabilitation program and advanced rehabilitation technology, shoulder pain in patients with SCI which found about 69–76% remain a significant problem. These patients had lower levels of physical activities to avoid hurting shoulder movement which can be affected to their quality of life.7,8 Predictors of shoulder pain after SCI are older age, complete injury, longer time since injury, manual wheelchair users, high body mass index (BMI), tetraplegia, poor motor power, and shoulder stiffness.9–13
There are a lot of shoulder special tests, but these tests are insufficient for definite diagnosis and are not sensitive as US is a noninvasive imaging technique for investigating cause of shoulder pain. Previous research studies reported US abnormalities in patients with normal shoulder special tests.14,15 Study of Ninomyia et al. 16 showed that patients with SCI who were included in rehabilitation program had 87.5% shoulder US abnormalities at least one structure and from these 71.43% complained shoulder pain. A previous study showed that common shoulder pathologies in patients with SCI with or without shoulder pain were subdeltoid-subacromion bursitis, biceps tendon effusion, and supraspinatus tendinosis. 17 The study of Brose et al. 18 found that common ultrasound abnormalities in manual wheelchair users with SCI were supraspinatus tendinopathy, cortical irregularity, and supraspinatus impingement.
Currently, there is a limited understanding of the US characteristics of shoulder in patients with both tetraplegic and paraplegic SCI with shoulder pain. The knowledge of definite pathology by US is a potential key for directly plan of treatment. The objective of the study was to examine shoulder US imaging in patients with both tetraplegic and paraplegic SCI with shoulder pain.
Materials and methods
Research design
A descriptive study.
Participants
This study examined patients with SCI who presented with shoulder pain on either side or both sides visited the Srinagarind hospital which is the largest super tertiary care hospital in Northeast region of Thailand. Inclusion criteria were age more than 18 years, a history of SCI over 6 months, and provision of written informed consent. Exclusion criteria were history of shoulder pain or injury prior to SCI, history of shoulder surgery and impotence to sit in a chair more than 30 min.
Methods
Written informed consent was collected from all patients. Demographic data included sex, age, BMI, handedness, underlying disease, neurological level, SCI type, duration of SCI, ambulatory assistive device, capabilities of daily activities living, and transfer were evaluated. In addition, the involved pain site, onset of shoulder pain, duration of shoulder pain, severity of shoulder pain during activities of daily living, transfer, and ambulation were assessed. Physical examination was composed of the point of maximal tenderness and shoulder passive range of motion in all directions by a goniometer. These information were performed by a physician who was not a musculoskeletal US viewer.
US of both shoulders were examined by a physiatrist who was experienced in musculoskeletal US more than 10 years. The musculoskeletal US viewer was blind to the patient's physical examination results. This process was performed according to previous standard manner with LOGIQ e and using 9–14 Hz linear transducer. The studied shoulder structures were the biceps tendon, the subscapularis tendon, the acromioclavicular joint (ACJ), the supraspinatus tendon, the subdeltoid-subacromial bursa, the infraspinatus tendon, the glenohumeral joint (GHJ), and the dynamic supraspinatus impingement test.19,20 The interpretation of US abnormalities were based on international guidelines of the outcome measures in rheumatology (OMERACT 7). 21
This study was approved by the Khon Kaen University Ethics Committee in Human Research (HE 601162).
Statistical analysis
All statistical analyses were analyzed by SPSS 19.0 (IBM SPSS statistics Version 19). If the data were normally distributed, continuous data were shown in mean and standard deviation (SD). If the data were not normally distributed, continuous data were described in median with interquartile range (IQR). Ordinal and categorical data were reported in frequency and percentage.
Association between factors and shoulder US abnormalities were analyzed by Fisher's exact test. Factors, which had P-value <0.2, would be further analyzed by logistic regression analysis (significant P-value < 0.05).
Results
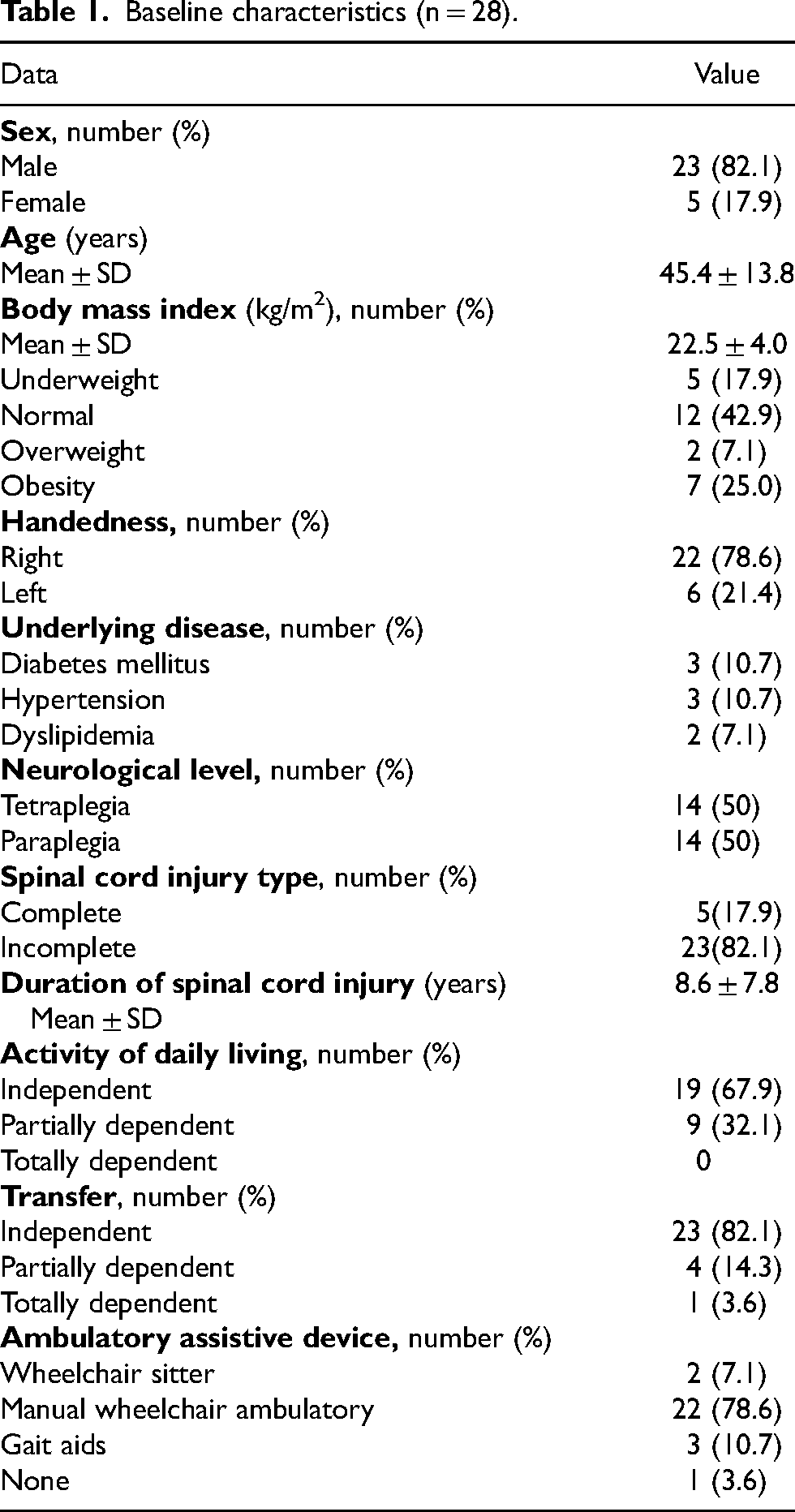
Of the 28 patients with SCI enrolled in this study, 23 (82.1%) were male. The average age was 45.4 ± 13.8 years. Most patients had right handedness (78.6%). According to ASIA, a number of tetraplegic group was 14 (50%) which was equal to paraplegic group. Most of the participants were incomplete (82.1%) which had duration of SCI about 8.6 years. Most of the participants had independent in both of ADL (67.9%) and transferring (82.1%). Manual wheelchair ambulatory was the most assistive device for mobility (78.6%) (Table 1).
Baseline characteristics (n = 28).
Regarding shoulder pain characteristics, most shoulder pain sites were right (39.3%). Shoulder pain occurred about 4 years post-SCI. Median duration of shoulder pain was 1 month. Most of participants had pain interfered with ambulation (67.8%). The most common point of maximal tenderness was right anterior region (50%). The more information about shoulder pain were summarized in Table 2.
Shoulder pain characteristics.
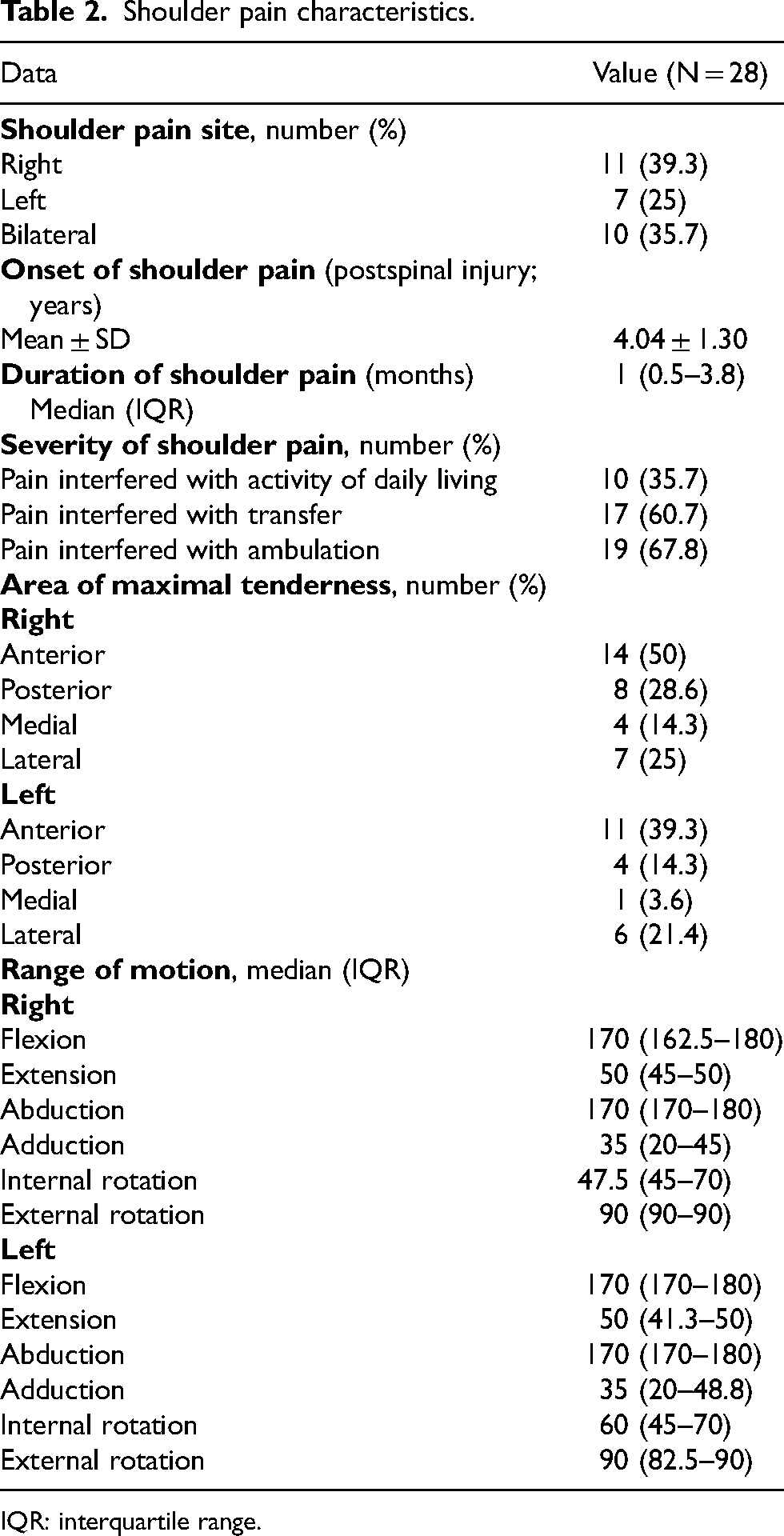
IQR: interquartile range.
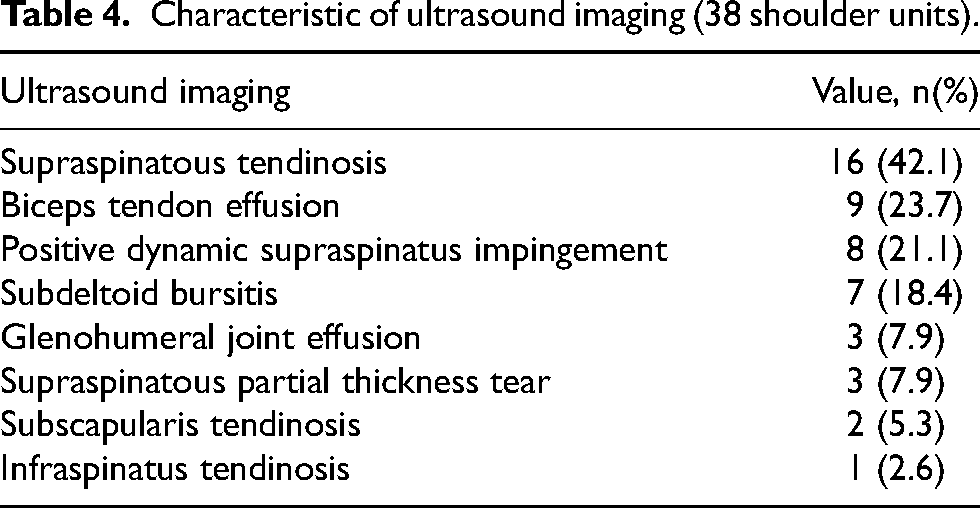
According to the US imaging, abnormal US findings in at least one of the structures assessed were found in 24/28 (85.7%) individuals (Table 3). Total shoulder US abnormalities were 38 shoulders. Most common abnormal US imaging were supraspinatus tendinosis (42.1%), bicipital tendon effusion (23.7%), positive dynamic supraspinatus impingement (21.1%), and subdeltoid bursitis (18.4%) (Table 4).
Ultrasound imaging in patients with spinal cord injuries with shoulder pain.
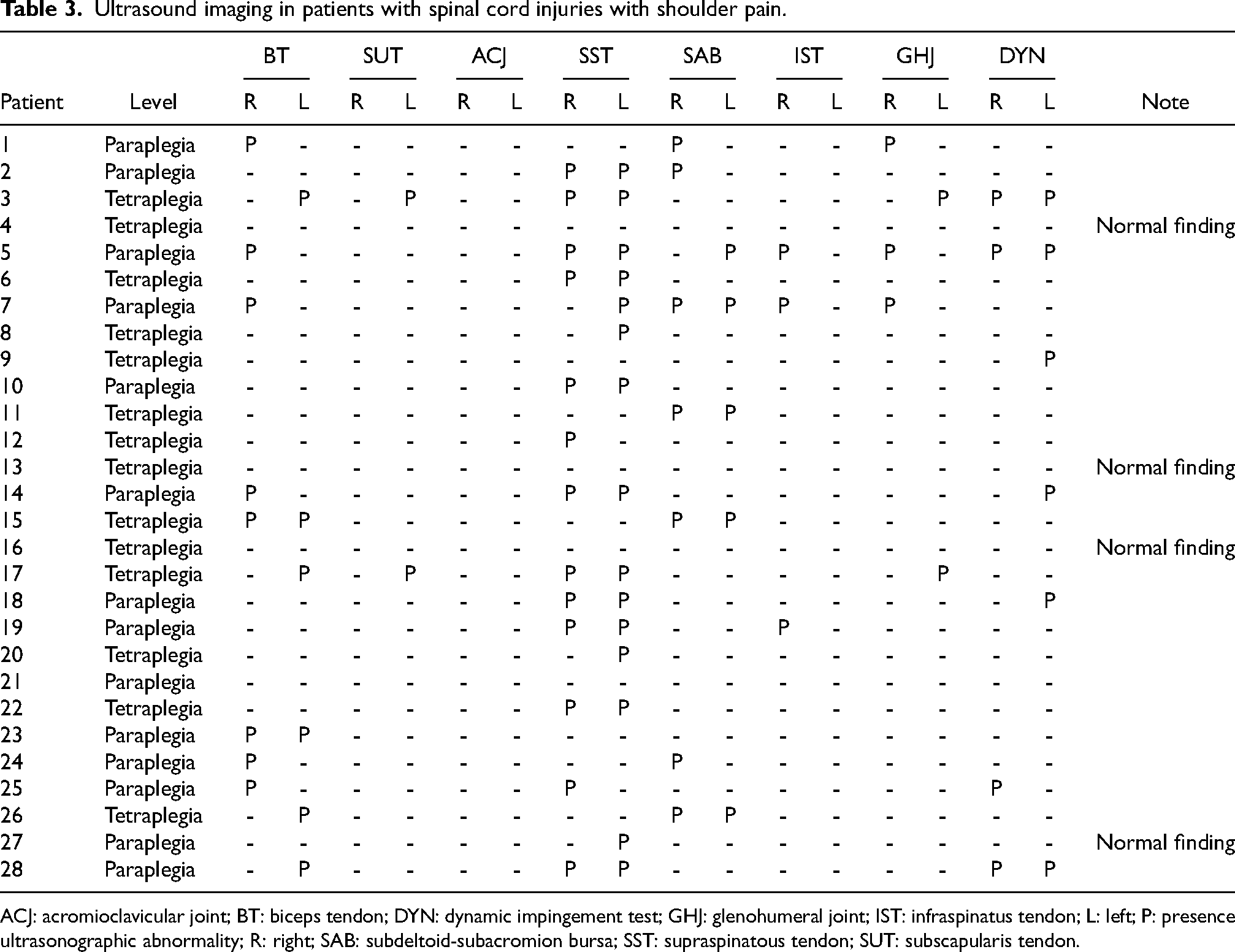
ACJ: acromioclavicular joint; BT: biceps tendon; DYN: dynamic impingement test; GHJ: glenohumeral joint; IST: infraspinatus tendon; L: left; P: presence ultrasonographic abnormality; R: right; SAB: subdeltoid-subacromion bursa; SST: supraspinatous tendon; SUT: subscapularis tendon.
Characteristic of ultrasound imaging (38 shoulder units).
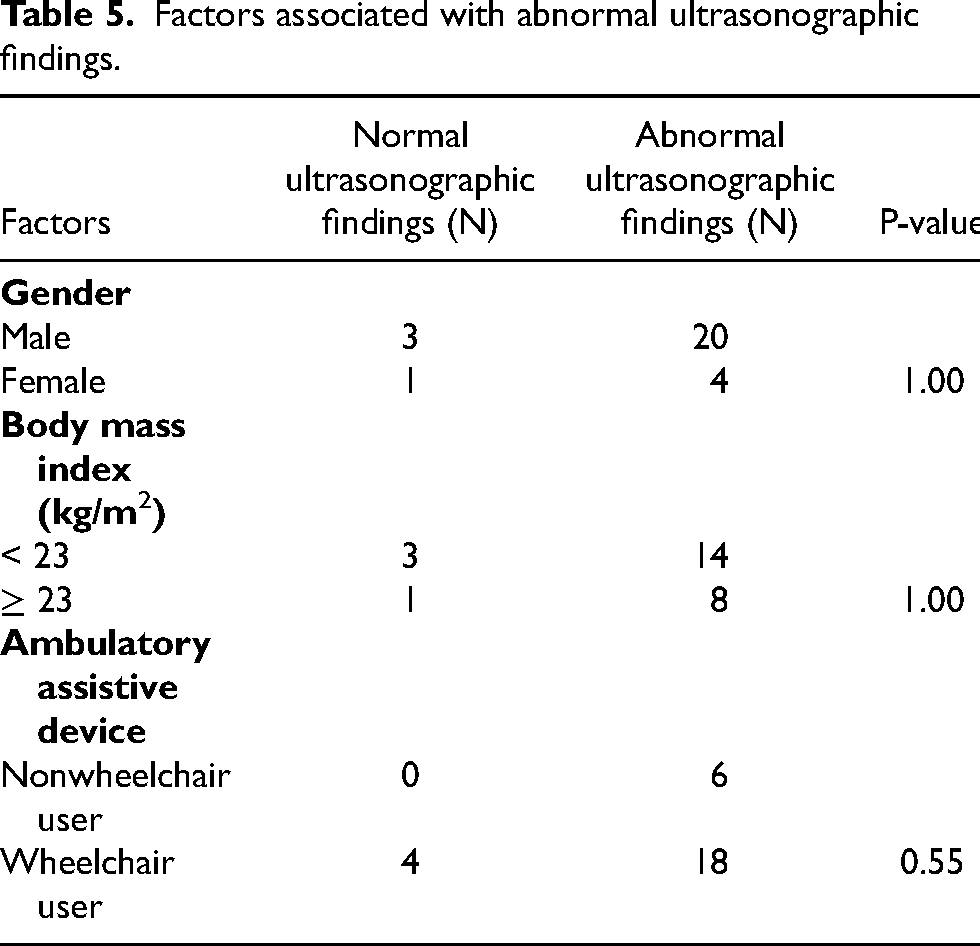
No association between gender, high BMI, wheelchair users, and abnormal US findings was detected (Table 5).
Factors associated with abnormal ultrasonographic findings.
Discussion
In this study, we found shoulder pain in tetraplegia was equal in paraplegic groups which was differed from previous studies that found a high in patients with tetraplegic SCI.16,19,20 We hypothesized that most of our patients were incomplete SCI and living in Thai economic society which constrained independent survival. Patients with both tetraplegia and paraplegia SCI have to use both upper limbs for daily routine activities and mobility involving repetitive shoulder motion which was a risk of shoulder pain.
In this study, we found onset of shoulder pain occurred within the first 5 years of post-SCI which was similar to the previous study which found that upper extremities pain was highest in the first 5 years of postinjury. 22 Most of the patients reported pain on the right shoulder which was a major dominant side. It was in accordance with the hypothesis that hand dominance could have an influence on the scapular kinematics which was evident of pain due to recurrent microtrauma. 23 Moreover, most of the patients reported that shoulder pain interfered their ambulation which was consistent with a former study. 24 These results indicated that most of the patients with SCI were more likely to use the upper limbs for manual wheelchair ambulation which is prone to directly repetitive trauma to shoulder area.
Regarding shoulder examination, most of the point of maximal tenderness was anterior region which can be referred to various pathology such as supraspinatus tendinopathy, bicipital tendinitis, and subaromion-subdeltoid bursitis. Therefore, US imaging is an important investigation for potential definite cause of shoulder pain. In this study, the most common US abnormality was supraspinatus tendinosis which was consistent with previous studies which found supraspinatus tendinopathy as the most common shoulder lesion in patients with SCI.16,18 It suspected that most of the patients in the current study were ambulatory manual wheelchair users. Therefore, the abnormal distribution of tension transmitted across the shoulder during control a wheelchair was contributed to the high degree of rotator cuff tendinopathy in these patients.
Moreover, this study found that at least one US abnormalities imaging was found in patients with SCI with shoulder pain. Therefore, physicians should concern that shoulder pain in patients with SCI could be caused by rotator cuff and nonrotator cuff tendon lesions which can be approved by US imaging. Physicians should use US imaging together with physical examination for early identification of diagnosis. Among the US result, diagnosis of subdeltoid bursitis or biceps effusion, these pathologies can be treated by early intervention such as therapeutic exercise, physical therapy, and medications which lead to good outcome.25,26
Several limitations exist within this study. Firstly, the data design was assessed in cross-sectional study. We could not identify whether the abnormalities would remain still pain. However, the results of this study may guide the advantage of US imaging for investigating patients with SCI with shoulder pain. Secondly, this study focused on rotator cuff and nonrotator cuff lesion as mentioned. US imaging cannot detect other causes of shoulder pain such as myofascial pain or neuropathic pain which can also occur in patients with SCI. Thirdly, this study had no age-matched and sex-matched controls which might have provided more comparable data and allowed more insightful interpretation. Fourthly, the limitation of US study is operator dependent. Further studies by different physiatrists to decrease potential of interobserver variation and confirm imaging by shoulder magnetic resonance imaging should be considered.
Conclusion
The supraspinatus tendinosis is the most common abnormal US imaging in patients with SCI with shoulder pain. Ultrasound is an assisted tool for investigating cause of shoulder pain in patients with SCI.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was granted by the Faculty of Medicine Research Fund, Khon Kaen University (IN60304).