
Abstract
Keywords
Introduction
Ultrasound guided popliteal sciatic nerve block is proven to be a safe and effective mean in providing anesthesia for foot and ankle surgery. 1 It shows excellent and consistent performance in terms of pain control over territories innervated by common peroneal and tibial nerves. 2 We previously described our experience of surgeon-administered popliteal sciatic nerve block in foot and ankle injuries. 3 Due to the shortage of anesthetist manpower in our hospital, we introduced the all-surgeon led regional anesthesia program in 2023 in which the surgeon in charge performed operations after induction of regional anesthesia by himself. 4 While providing adequate anesthesia to certain foot and ankle conditions, popliteal sciatic nerve block does not cover area innervated by saphenous nerve. Injuries involving medial side of foot and ankle requires additional nerve block. To overcome this limitation, we extended our practice by performing adductor canal block to cover saphenous nerve to allow more extended anesthesia. In this article, we shared our successful experience in performing ultrasound-guided combined popliteal sciatic nerve and adductor canal block for fixation of trimalleolar fracture.
To our knowledge, it is the first ever article describing a series of patients with their operations performed under surgeon-performed combined popliteal sciatic nerve and adductor canal block in Hong Kong. In fact, very limited studies have been conducted to share similar experience and to prove the efficacy of this mode of regional anesthesia performed by surgeons.
Patient and method
Study design and objective
This retrospective study is performed to review the performance of surgeon-administered ultrasound-guided combined popliteal sciatic nerve block and adductor canal block in our unit for patients underwent fracture fixation for trimalleolar fracture of ankle.
Inclusion and exclusion criteria
This study includes patients suffering from trimalleolar fracture with operation performed at our unit under surgeon-administered ultrasound-guided combined popliteal sciatic nerve block and adductor canal block from January 2024 to August 2024. Patients with their operation performed under other modes of regional anesthesia (e.g. isolated popliteal sciatic nerve block) were excluded from this study.
General exclusion criteria for this program includes uncooperative pediatric patients, uncooperative psychiatric or demented patients, patients with uncontrolled bleeding tendency, patients with poor soft tissue condition at the site of anesthesia injection and surgeries performed under general anesthesia or regional anesthesia by anesthetists.
Data collection
Patients’ demographic details such as age, sex, medical comorbidities classified by American Society of Anesthesiologists Classification (ASA) classification and side of injury were extracted from their medical records. The type of operation, operative time, and blood loss were retrieved from their operative records. Postoperative length of stay was referred by the discharge summary of patients. Patients’ pain control by Visual Analog Scale (VAS), motor blockage intraoperatively and pain control at 6 h postoperatively were assessed and documented.
Anesthesia technique
Application of regional anesthesia was performed by trained orthopedic surgeons who would subsequently perform the operation. Anesthetic agent which consisted of 10 mL 2% lignocaine with 1:200,000 adrenaline and 10 mL 0.5% levobupivacaine was prepared. The total dose of mixture used was calculated according to patients’ body weight with consideration of their hepatic and renal functions. Ultrasound imaging was utilized for direct visualization of related anatomical structures. Tactile feedback passing through paraneural sheath and muscle fascia provided additional confirmation regarding the needle position. Aspiration would be performed before injection to avoid introduction of anesthetic agent into the systemic circulation directly. Resistance free injection was ensured to avoid intraneural injection.
Popliteal sciatic nerve block
The patient involved would undergo ultrasound guided popliteal sciatic nerve block followed by adductor canal block. Popliteal sciatic nerve block was carried out in lateral decubitus position with the patient's knee put at a slightly flexed manner (Figure 1). Ultrasound probe was placed over the popliteal fossa to identify the level at which sciatic nerve just divided into common peroneal and tibial nerves. A 100-mm 21 gauge insulated stimulating needle was placed in in-plane manner from lateral to medial to area underneath the common paraneural sheath which surrounded the common peroneal and tibial nerves (Figures 2 and 3). Accurate infiltration was ascertained by the separation of common peroneal and tibial nerves by the anesthetic agent after injection (Figure 4).
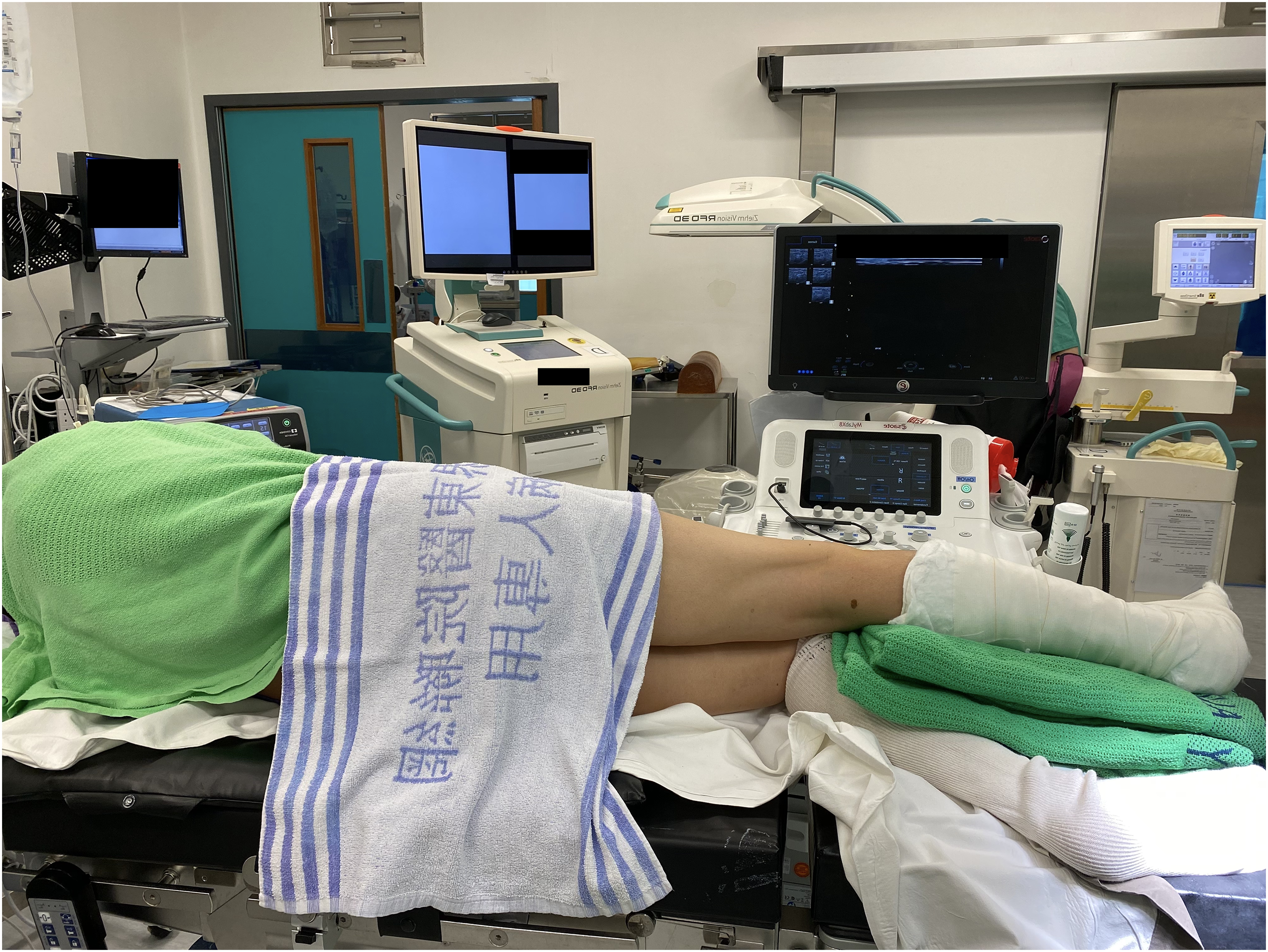
Patient positioning for popliteal sciatic nerve block.

Needle placement under ultrasound guidance.
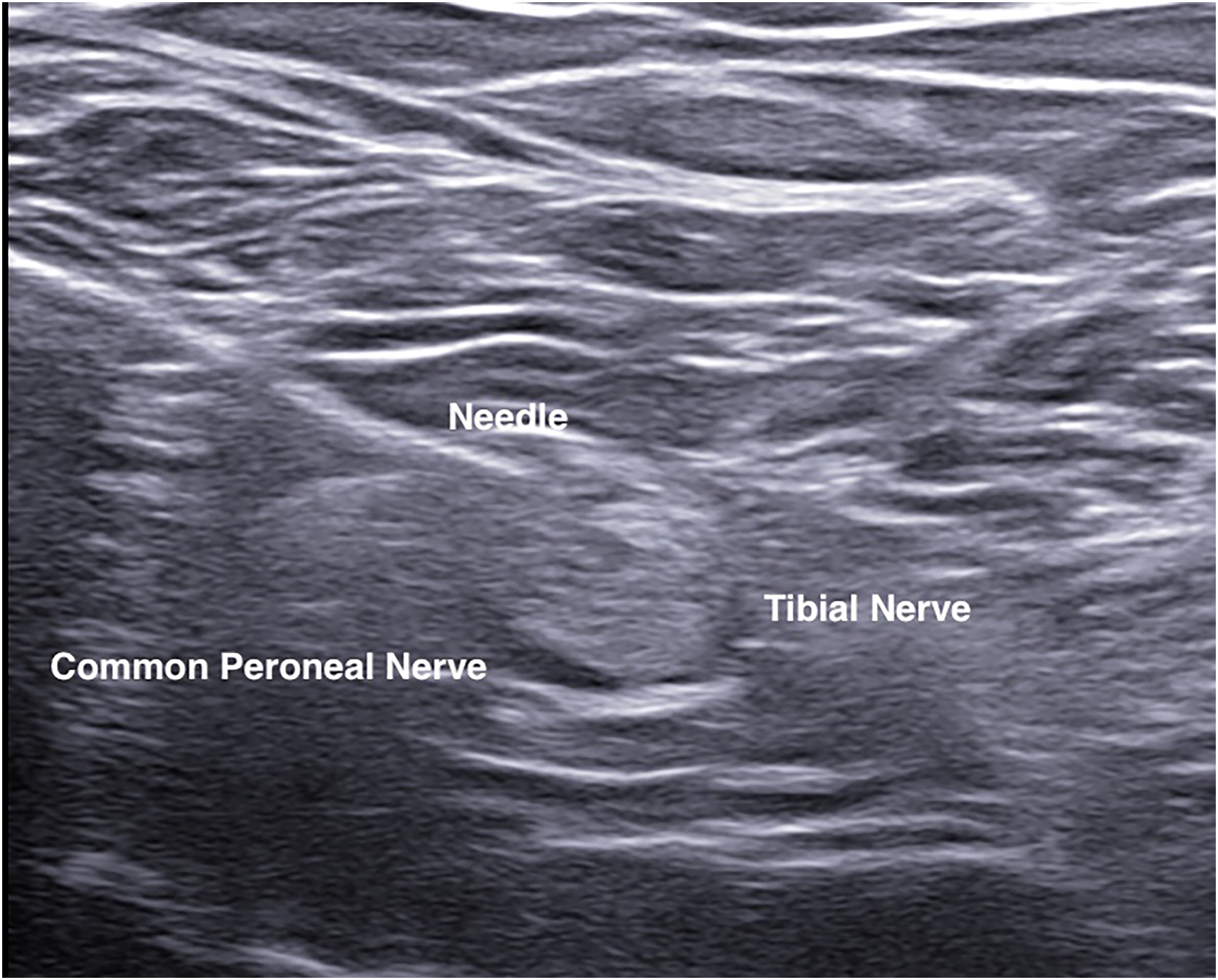
Needle placement at bifurcation of sciatic nerve into common peroneal and tibial nerves.
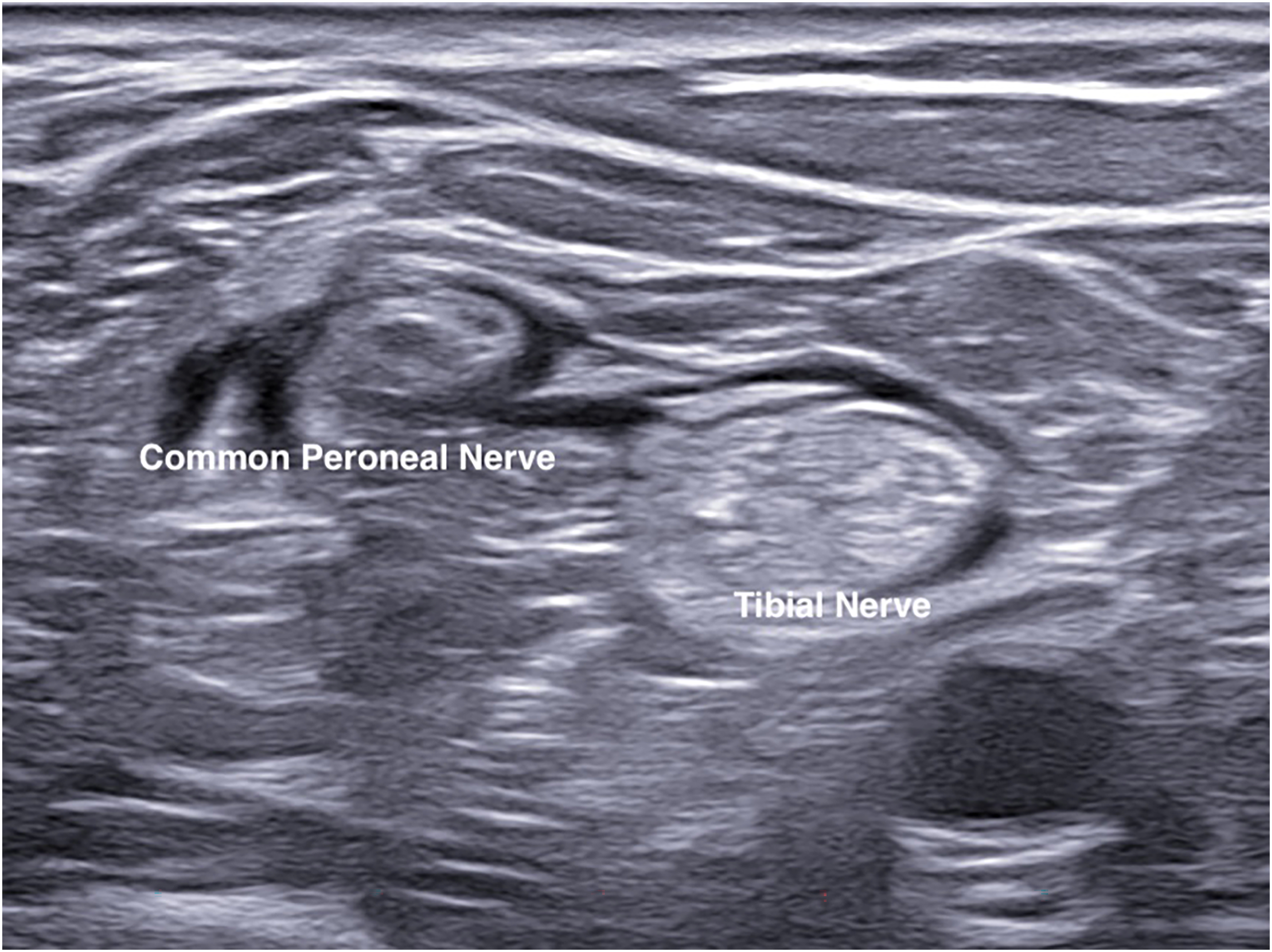
Common peroneal and tibial nerves surrounded by anesthetic agent.
Adductor canal block
The patient would then be put into supine position with the injured limb at slight abduction and external rotation to allow access to medial thigh (Figure 5). Ultrasound examination would be performed at mid-thigh level to identify the relevant anatomical structures of satorius, vastus medialis, femoral artery and vein, and saphenous nerve (Figure 6). Needle was placed in plane from lateral to medial direction through the satorius muscle. Needle tip was positioned just anterior to the femoral artery, between satorius and vastus medialis muscle and adjacent to saphenous nerve. Anesthetic mixture would then be infiltrated around the nerve under ultrasound guidance (Figure 7).

Patient positioning for adductor canal block.
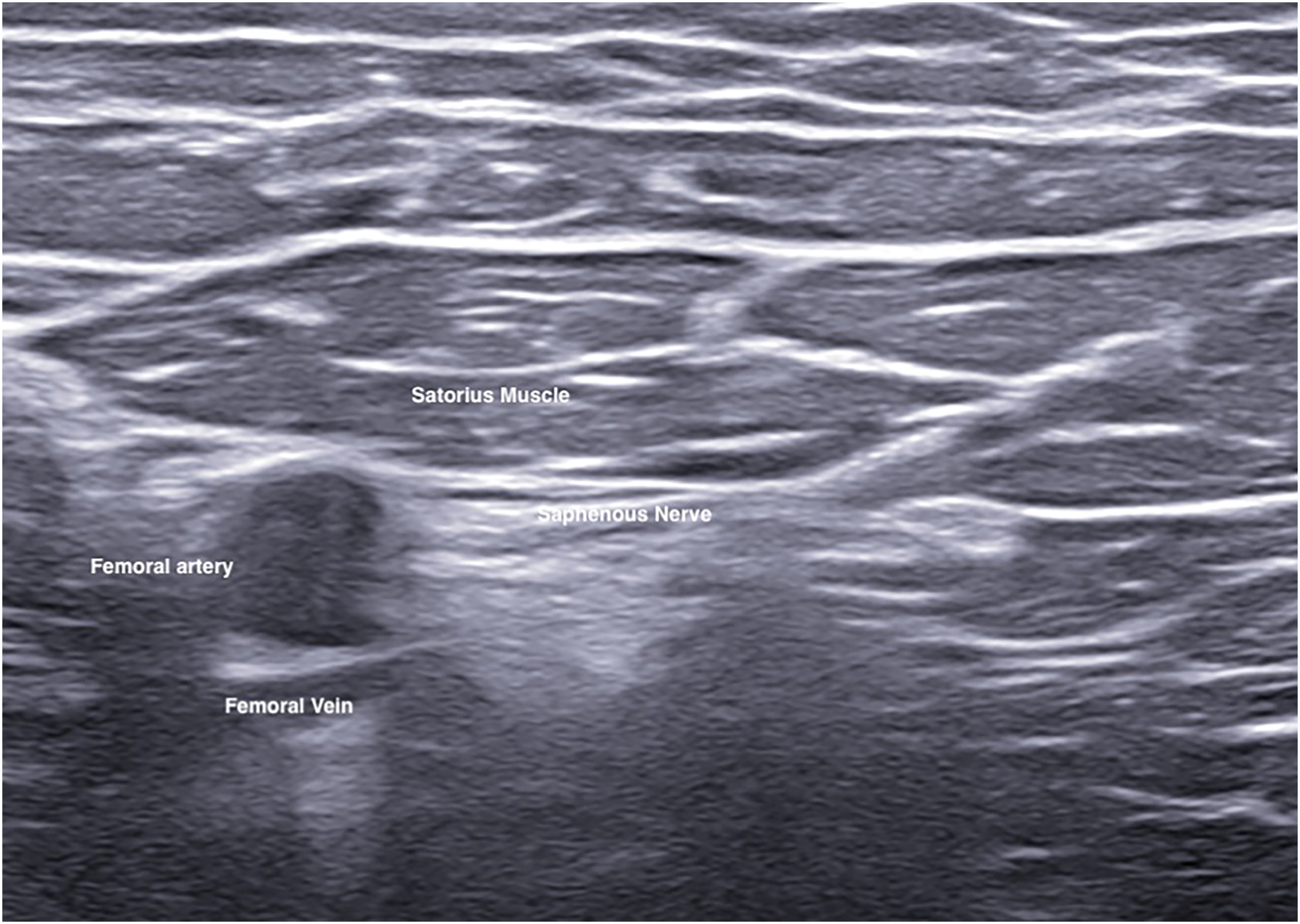
Needle advancement for saphenous nerve block under ultrasound guidance.
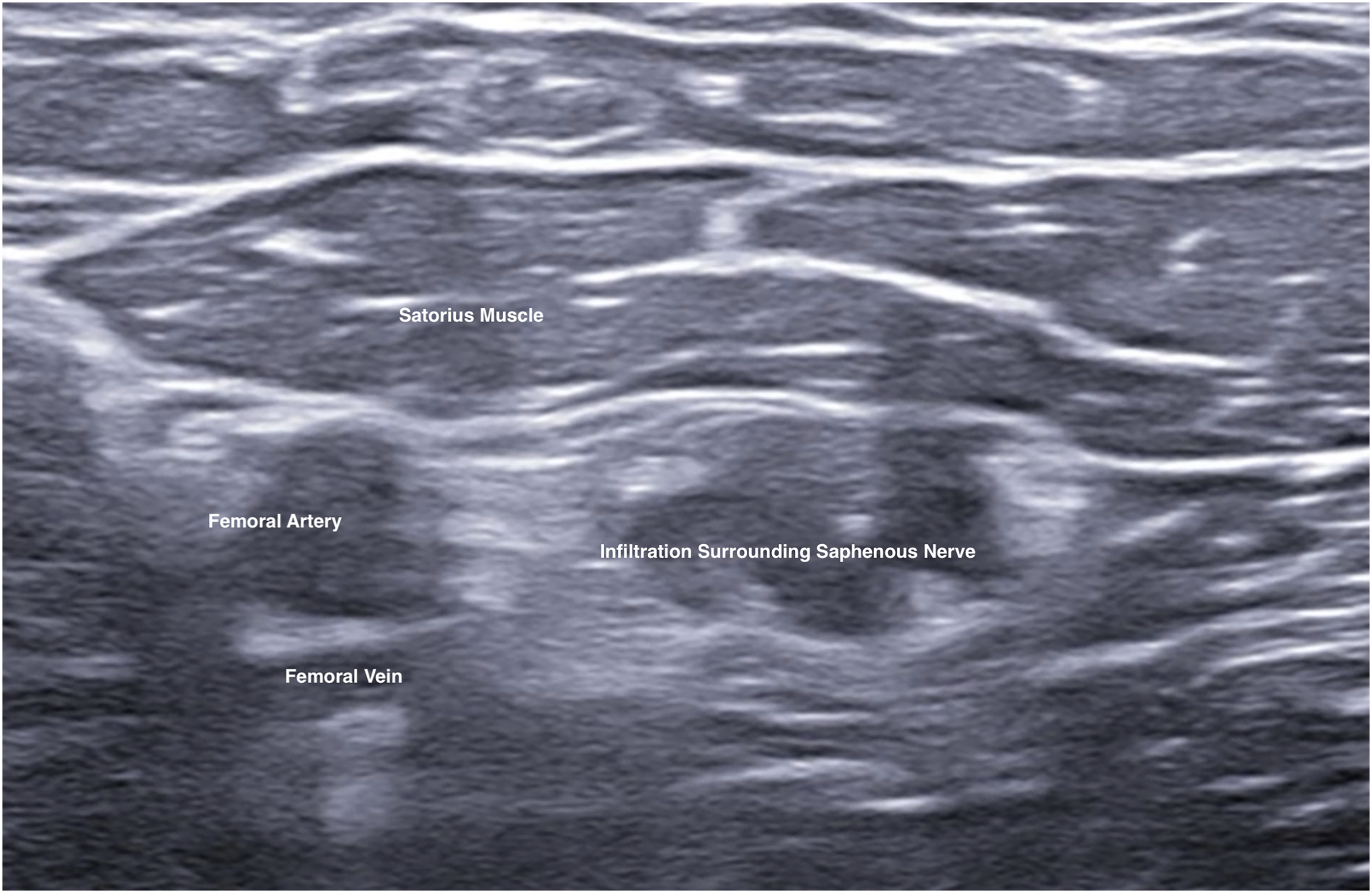
Infiltration of anesthetic agent around saphenous nerve.
Surgical technique
After confirmation of successful induction, the attending surgeon would then perform the surgical fixation. Operation would be performed with the patient put at floppy lateral position. Posterolateral approach was adopted for fixation of distal fibula fracture. Distal fibula fracture would be reduced and stabilized by Synthes 2.7/3.5 Distal Fibula Anatomical Locking Plate (Figure 8). Following distal fibula fixation, Volkmann fragment was exposed through the plane between peroneal muscle and Achilles tendon. Stabilization of Volkmann fragment was achieved with the use of 4.0 mm cannulated screw or one-third tubular plate depending on the fragment size. Medial malleolar fragment would be exposed and reduced through a mini-open incision at the medial malleolus and subsequently stabilized with two parallel 4.0 mm cannulated screws (Figure 9).
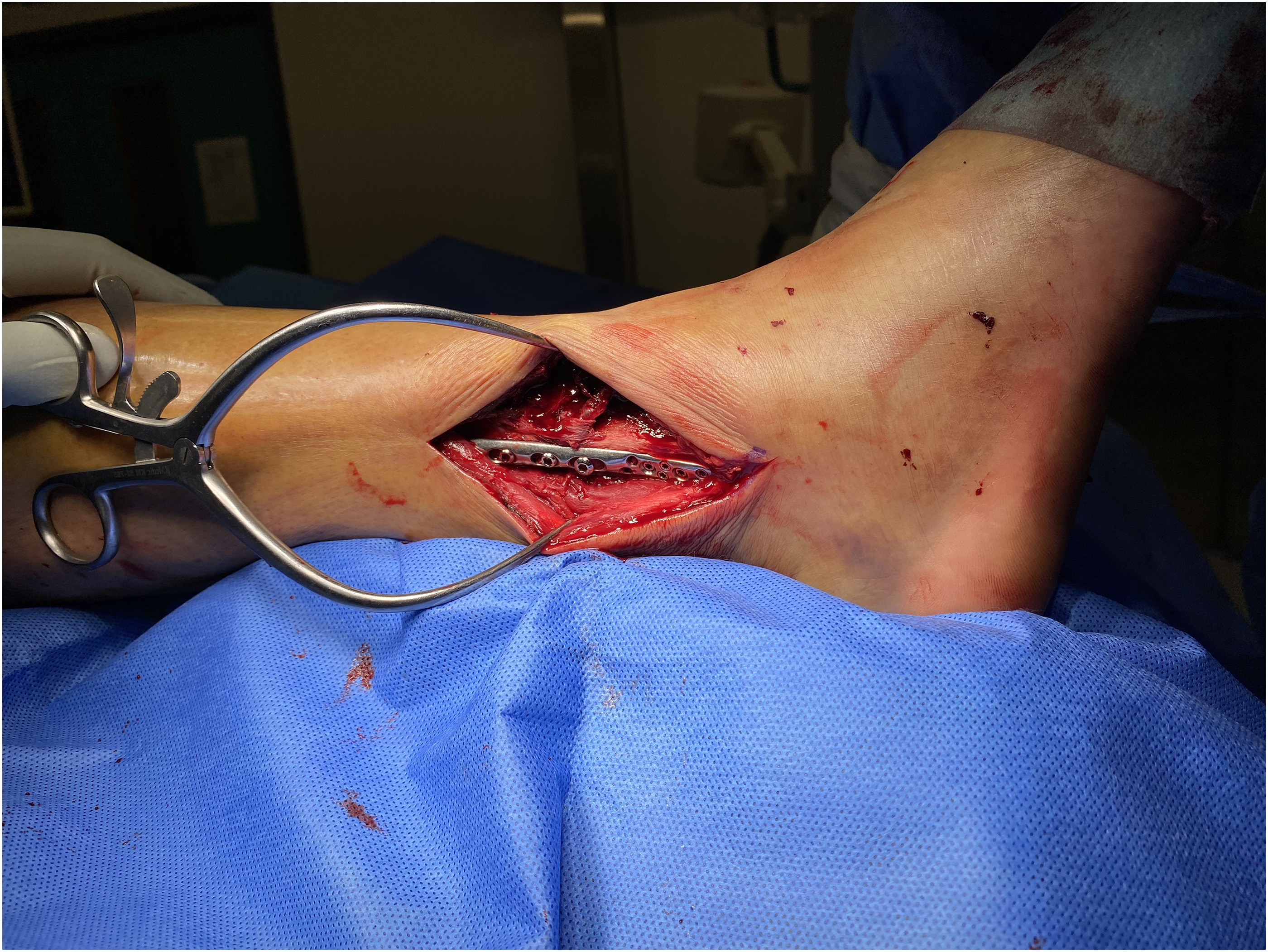
Fixation of distal fibula fracture.

Fixation of medial malleolar fracture.
Follow-up
All patients were monitored continuously throughout the operation. Pain control, degree of motor blockage and vital signs were assessed and recorded. Pain control during operation and at 6 h postoperatively were documented. Panadol and tramadol in oral form were used as standard analgesics upon patients’ request if the pain was regarded as intolerable.
Result
There were six men and seven women included in this study. The average age of patients included was 57.8. All of them suffered from ankle fracture which would be classified according to AO classification. Eleven patients suffered from 44-B3 type injury, 1 patient suffered from 44-C2 and 44-C3.3 injury respectively. Average hospital stay from injury to operation was 13.9 days. All patients experienced complete anesthesia with VAS 0 and complete motor blockage throughout the operation. Average operative time was 179 min with an average blood loss of 24.6 mL. Postoperative pain control was satisfactory with all patients experienced pain with VAS less than 2 at 6 h after operation. Average postoperative hospital length of stay was seven days. There was no anesthetic related complication reported. Postoperative X-ray of all patients showed anatomical reduction with satisfactory alignment (Figures 10 and 11). Patients’ characteristic and results were summarized in Table 1.
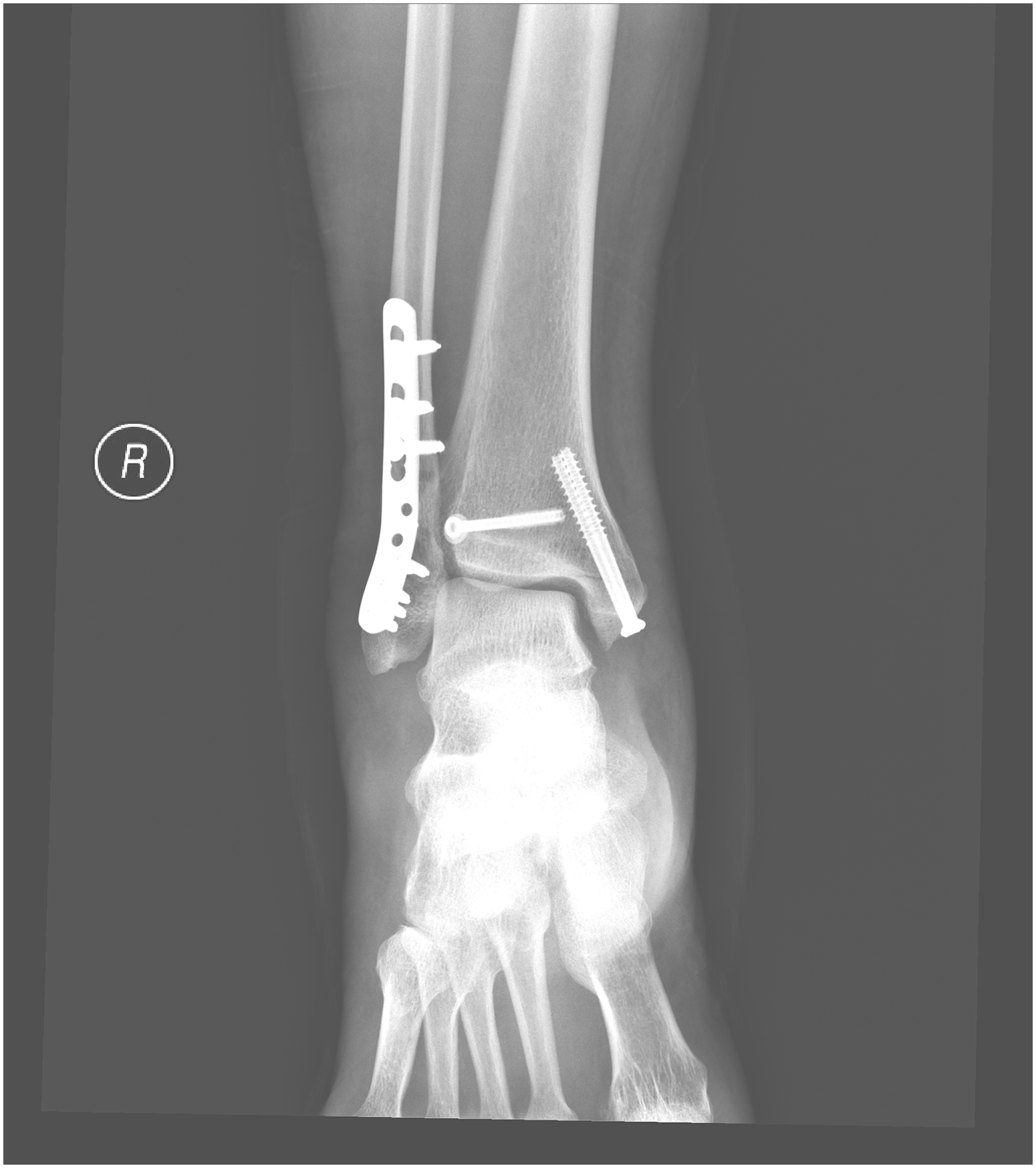
Postoperative X-ray in AP view.
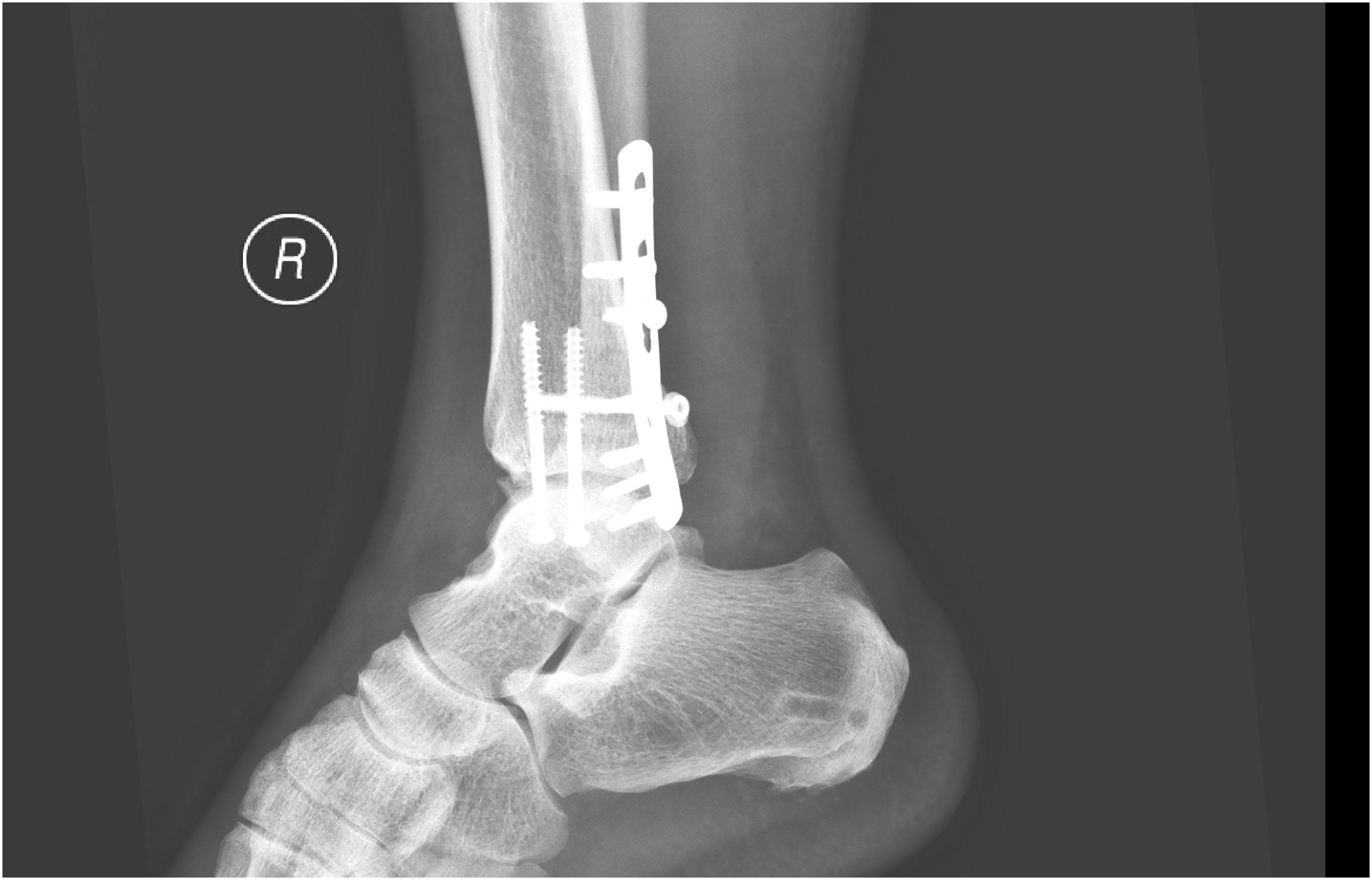
Postoperative X-ray in lateral view.
Table summarizing patients’ characteristic and result.
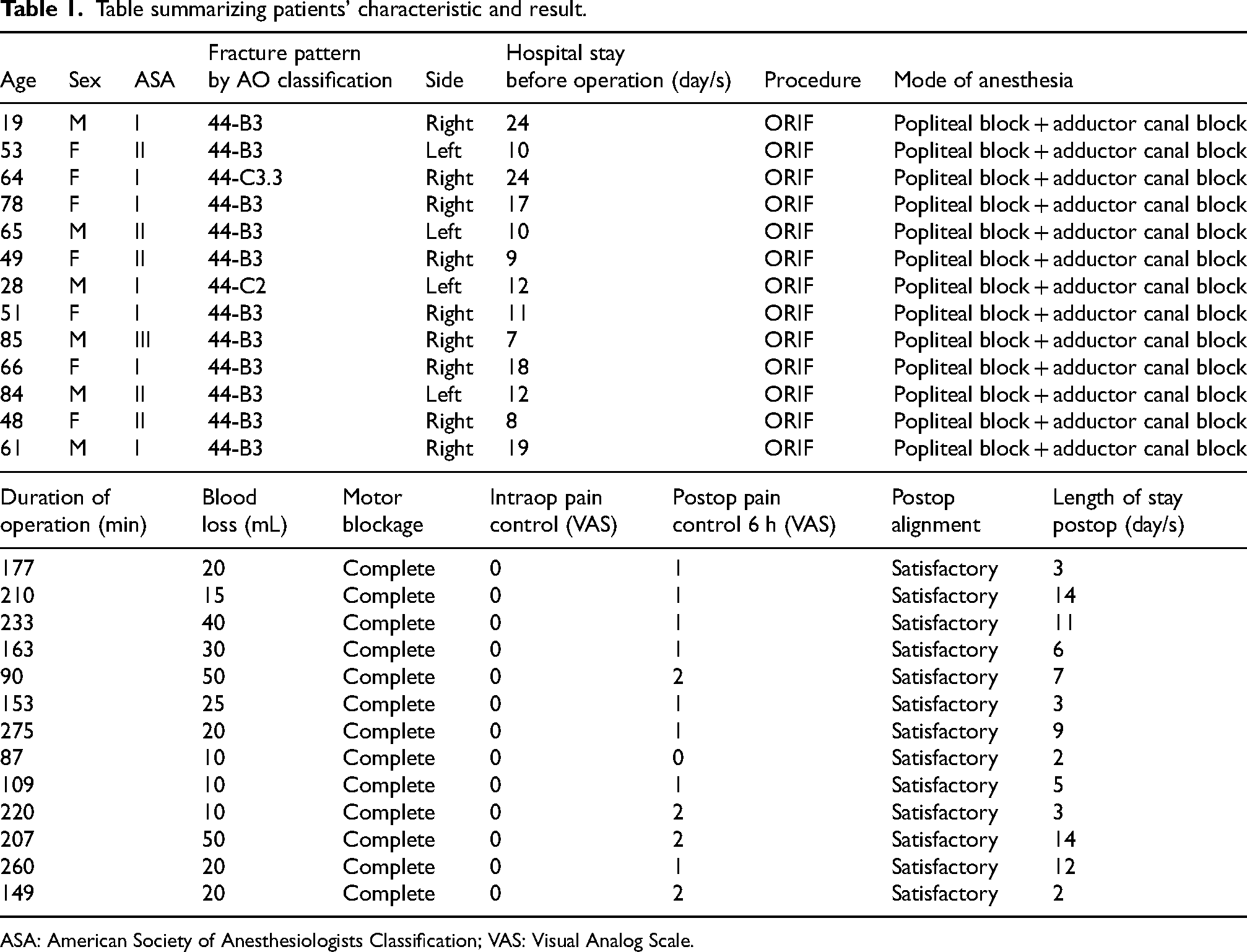
ASA: American Society of Anesthesiologists Classification; VAS: Visual Analog Scale.
Discussion
Saphenous nerve is the terminal branch of the femoral nerve providing sensory innervation to medial aspect of leg, ankle and foot. 5 While a well-performed popliteal sciatic nerve block provides excellent anesthesia to the entire distal two-third of the lower limb except the medial aspect, saphenous nerve block provides great supplement to allow anesthetic coverage over the residual part. 6
We adopted the adductor canal subsatorial blockage of saphenous nerve with saphenous nerve identified at level of mid-thigh under ultrasound guidance. Different approaches had been described concerning saphenous nerve blockage from inguinal area to ankle region, including perifemoral block, femoral triangle block, infrapatellar saphenous nerve block and supramalleolar nerve blockage.7–9 Adductor canal saphenous nerve block is intended for blockage of sensation, theoretically the anesthetic agent injected may spread along the subsatorial region affecting motor function of vastus medialis through partial motor blockage of its supplying nerve. 10 The occurrence of quadricep weakness from unintended vastus medialis nerve block is controversial, with several studies reported its effect on quadricep muscle power as minimal.11–13
Sciatic nerve is surrounded by the fascial paraneurium. We utilized the virtual space between paraneurium, common peroneal nerve and tibial nerve at level of its bifurcation for application of anesthetic agent. Anesthetic mixture injected would subsequently spread to surround the two nerves distally. Accurate needle placement at the intended level was confirmed by injection test in which circular expansion of paraneural sheath was observed after trial with small volume injection. 14
Nerve injury is uncommon but has been reported following popliteal and adductor canal blocks. 15 The chance of neurological injury was reported to be less than 10%. 16 Mechanisms of injury can be due to physical injury during needle placement, chemical injury related to anesthetic agent and ischemic injury following injection into a relatively confined compartment. There is study suggested a neurotoxic component of neurological injury due to intrafascicular injection of anesthetic agent. 17 There are discussions about the advantage of ultrasound guided nerve block compared to traditional landmark technique with aid of nerve stimulation. Randomized control trial by Sagherian et al. showed similar block performance between two techniques except induction time. 18
Conclusion
According to our experience, combined popliteal sciatic nerve and adductor canal block can be safely performed by orthopedic surgeons. It allows satisfactory anesthetic performance for trimalleolar ankle fracture fixation.
The same principle may be applied to other orthopedic conditions involving foot and ankle region. However, further studies need to be continued to allow adequate power for formal analysis of its feasibility.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.