
Abstract
Introduction
Owing to their superficial nature, tibia fractures are considered one of the commonest long bone fractures, with an incidence of 8.1 to 37 per 100,000 patients; furthermore, these fractures are more susceptible to be open with further soft tissue and bone loss and subsequent infection, wound healing problems, and non-union which mostly necessitates further surgeries, especially in severe forms of open fractures such as Gustilo type III.1–4
Initial management of open tibial fractures includes early antibiotic therapy and temporary splinting followed by debridement to remove devitalised soft tissue or loose bony fragments and skeletal stabilisation, after which the actual soft tissue defect could be assessed.5,6 If primary wound closure was not applicable after debridement, delayed wound closure should be decided, besides the possibility of soft tissue reconstruction.6–8
With the introduction of negative-pressure wound therapy (NPWT) or vacuum-assisted closure (VAC), the results of wound management after open tibia fractures were favourable;9–12 this device helped in creating a closed environment that promoted granulation tissue formation; furthermore, it decreased the wound bacterial count till coverage is achieved.4,11,13
To the best of our knowledge, reports regarding the role of NPWT or VAC in managing severe open fracture wounds are rare in our area, so the primary objective of the current study was to investigate the early results by comparing the time needed till definitive soft tissue coverage between VAC versus conventional daily dressing in patients presented with open IIIB tibial fractures. The secondary objective was to determine the incidence of secondary surgical intervention before definitive coverage, the type of soft tissue reconstruction needed after each technique, and the success rate after the coverage procedure.
Patients and methods
After obtaining approval from our institution's ethical committee (IRB no.: 17100992), a prospective non-randomised clinical trial (NRCT) with a parallel design and allocation ratio of 1:1 was conducted per the TREND statement, 14 to compare outcomes of wound management of open tibia fracture after applying VAC compared to the conventional dressing at a level I trauma centre.
We selected cases from all patients admitted to our trauma unit who were diagnosed with open tibia fractures and treated surgically for two years starting in April 2019. We included skeletally mature patients (above 18 years old) who presented with acute (within three days) unilateral type IIIB open tibia fracture according to Gustilo classification.15,16 We excluded patients with a debilitated general condition or chronic medical comorbidities that could affect wound healing (such as chronic steroid therapy or peripheral vascular disease), pathological fractures, bone defect at the fracture site was more than 5 cm, if primary wound closure was achieved during surgery by tissue mobilisation or local flaps, delayed presentation (more than three days from the initial trauma), infected open fractures, and if the patient refused to participate in the study. This led to the eligibility of 45 patients to be included in the study.
Patients management
Initial assessment (for all patients)
On admission, an initial assessment was performed according to the ATLS protocol. After excluding other skeletal and non-skeletal injuries, attention was diverted to assessing and managing the open tibia fracture. Clinical evaluation of the wound and the distal neurovascular status of the limb was performed before sending the patient for radiological assessment. Radiographic evaluation (as a part of the ATLS secondary survey) included anteroposterior (AP) and lateral plain radiographs of the injured leg, including the ipsilateral knee and ankle. After confirming the diagnosis and assessing the fracture pattern in the radiographs, the patients’ tetanus vaccination status was assessed and dealt with accordingly; first generation cephalosporin was given immediately. The wound was inspected, and any gross contamination was removed, washed, and irrigated using normal saline, followed by applying a sterile dressing and a long leg temporary splint. The patient is then prepared for surgical debridement and initial fixation.
Before proceeding to surgical intervention, the patient's written informed consent was obtained regarding the intervention and approval for inclusion in the clinical trial, where all patients received the same initial surgical intervention protocol (per our trauma unit guidelines); however, they were assigned into two groups, Group A, where VAC was applied and Group B, where a conventional dressing (saline wet to moist non-adherent dressings) was used.
Surgical technique
After proper anaesthesia, according to the patient's general status, a tourniquet was applied but not inflated, followed by surgical draping, and the wound was reassessed. Fellowship-trained surgeons performed all surgeries; proximal and distal extension of the wound was performed along fasciotomy incisions (if needed) and further irrigation using at least 6 L of normal saline. Excision of devitalised tissues and bony fragments without soft tissue attachment was performed. Initial fracture stabilisation with the length and alignment restoration was performed using a monolateral external fixation. Then, attention was directed towards obtaining haemostasis and covering vital structures (bone and tendons) through tension-free muscles and soft tissue mobilisation. By the end of the surgery, if primary closure was not possible, VAC was applied to the exposed area in Group A while it was covered using a sterile conventional dressing in Group B. Assigning patients to either group was based on the experience of the operating surgeon of applying VAC.
Postoperative care
All patients were given broad-spectrum IV antibiotics till definitive coverage. The dressing was changed daily in Group B, while in Group A, VAC was changed every four days. Wounds were evaluated by the attending orthopaedic consultant to determine if there was a need for further debridement or if they were ready for coverage. The final decision for wound coverage was made by a member of the orthopaedic microsurgery team, who also performed the definitive coverage (Figures 1 and 2).
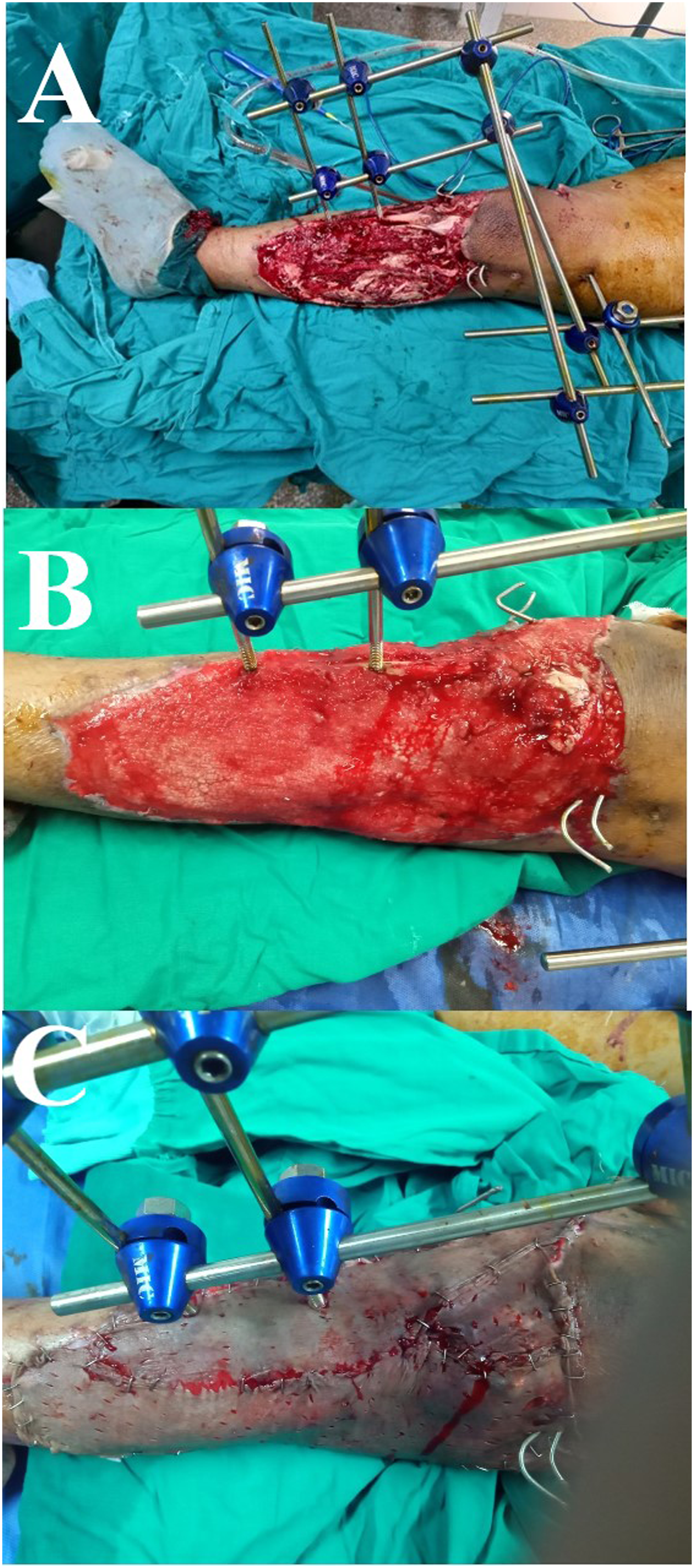
A female patient, 23 years old, presented 4 hours after a motor car accident with an open IIIB left tibial plateau fracture. (A) Intra-operative debridement and external fixation. (B) After two VAC dressings without further surgical debridement. (C) Definitive coverage using an STSG after 10 days from index trauma.
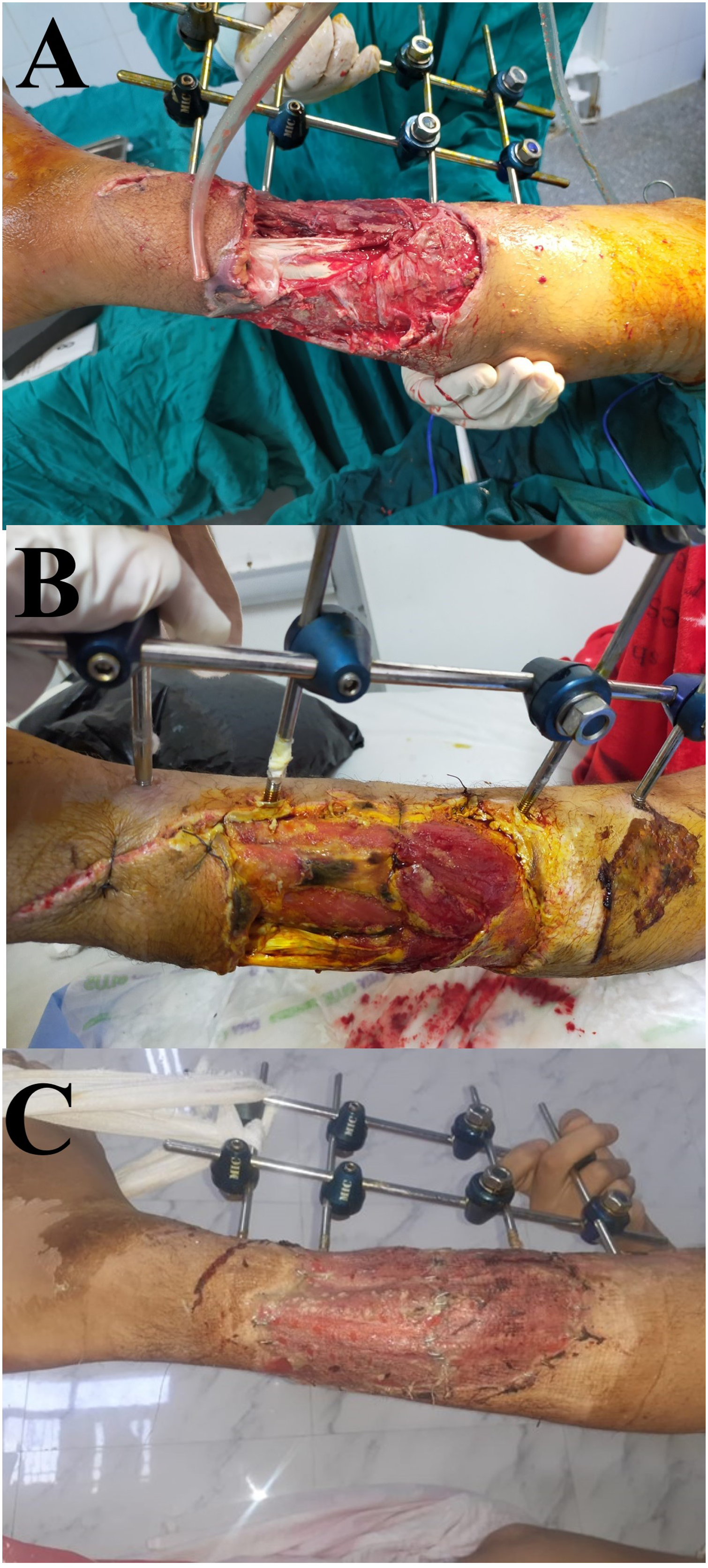
A male patient, 34 years old, presented 10 hours after a motorbike accident with an open IIIB tibial fractures. (A) Intra-operative debridement and external fixator were done. (B) The patient had daily conventional dressing; however, he needed two other sessions of surgical debridement. (C) Definitive coverage using an STSG after 16 days from index trauma.
For convenience, we excluded the first five patients from Group A, as these were the first cases where VAC was applied and were considered initial training on the new technique. The final analysis included 20 patients in each group.
Besides collecting patients’ basic demographic and injury-related data, the time needed till definitive coverage, type of coverage, failures, and the need for secondary surgery were collected. Furthermore, we stratified the coverage procedures into either using skin grafts or performing different kinds of flaps.17,18
Statistical analysis
Data was collected and analysed using SPSS (Statistical Package for the Social Sciences, version 20, IBM, and Armonk, New York). Continuous data was expressed as mean ± SD, while nominal data was expressed as frequency (percentage). Chi2-test was used to compare the nominal data of different groups in the study, while the Student’s t-test was used to compare mean of different two groups. A P-value <0.05 indicated a significant difference. For the sample size, we included all eligible patients for a total coverage of two years.
Results
Both groups had no differences in the basic demographic, comorbidities, injury mechanism and associated injuries (Table 1). The need for secondary debridement surgeries before definitive coverage was significantly lower in Group A compared to Group B, 1 ± 0.50 versus 2.50 ± 0.85, respectively (P < 0.001). The time till definitive coverage was significantly lower in Group A than in Group B, 12.22 ± 2.90 versus 23.56 ± 8.68 (days); P < 0.001. Furthermore, the type of coverage needed significantly differed between groups, where simpler coverage procedures (mainly skin grafts) were used in Group A compared to Group B (Table 2). All coverage procedures succeeded in Group A, while four (20%) failed in Group B, P = 0.04. Regarding infection rates, these were significantly higher in Group B, where infection was reported in six (30%) patients (including the four failed coverage cases) compared to only one (5%) in Group A, P = 0.01.
Baseline data of studied both groups.
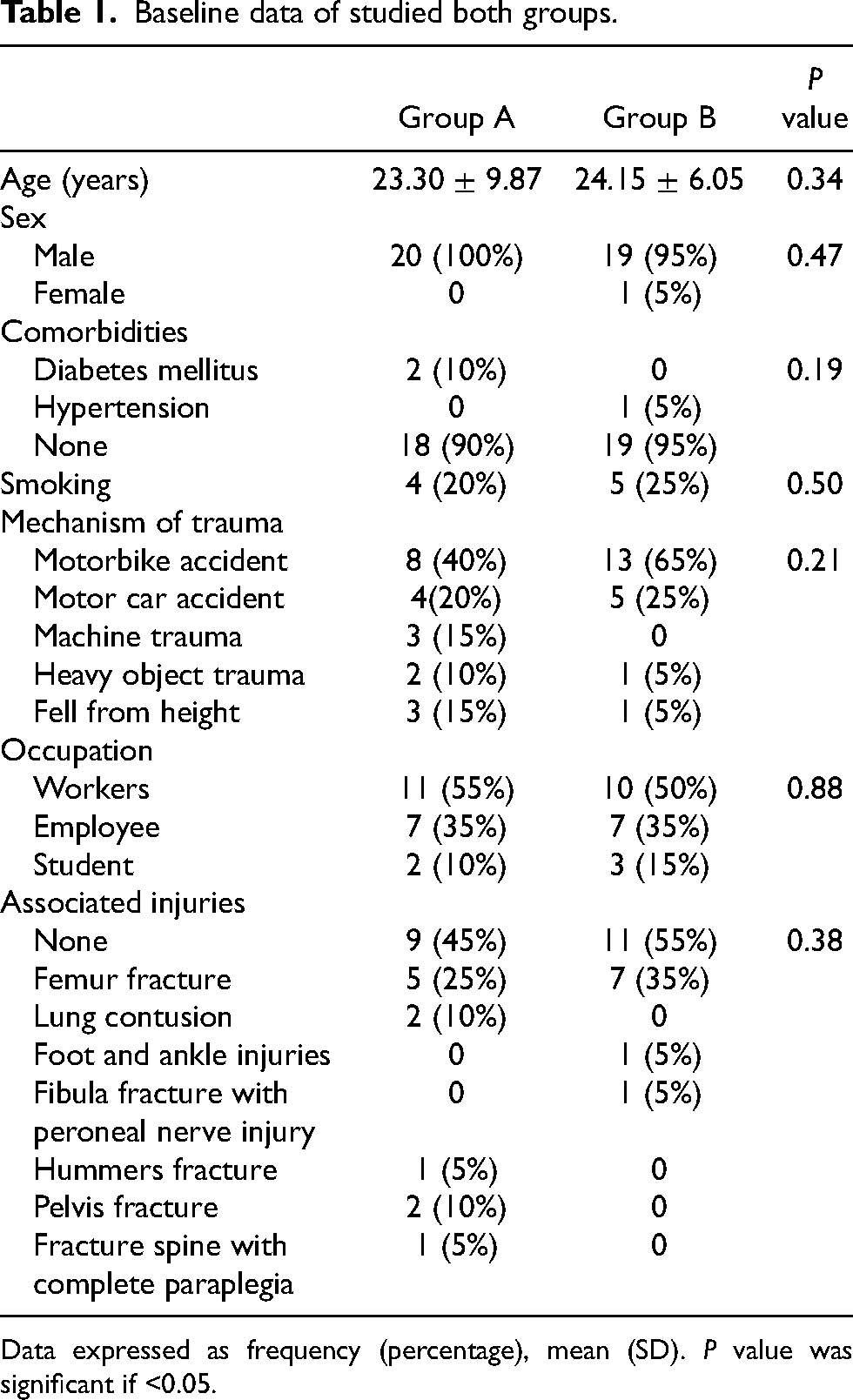
Data expressed as frequency (percentage), mean (SD). P value was significant if <0.05.
Surgical management and wound coverage details.
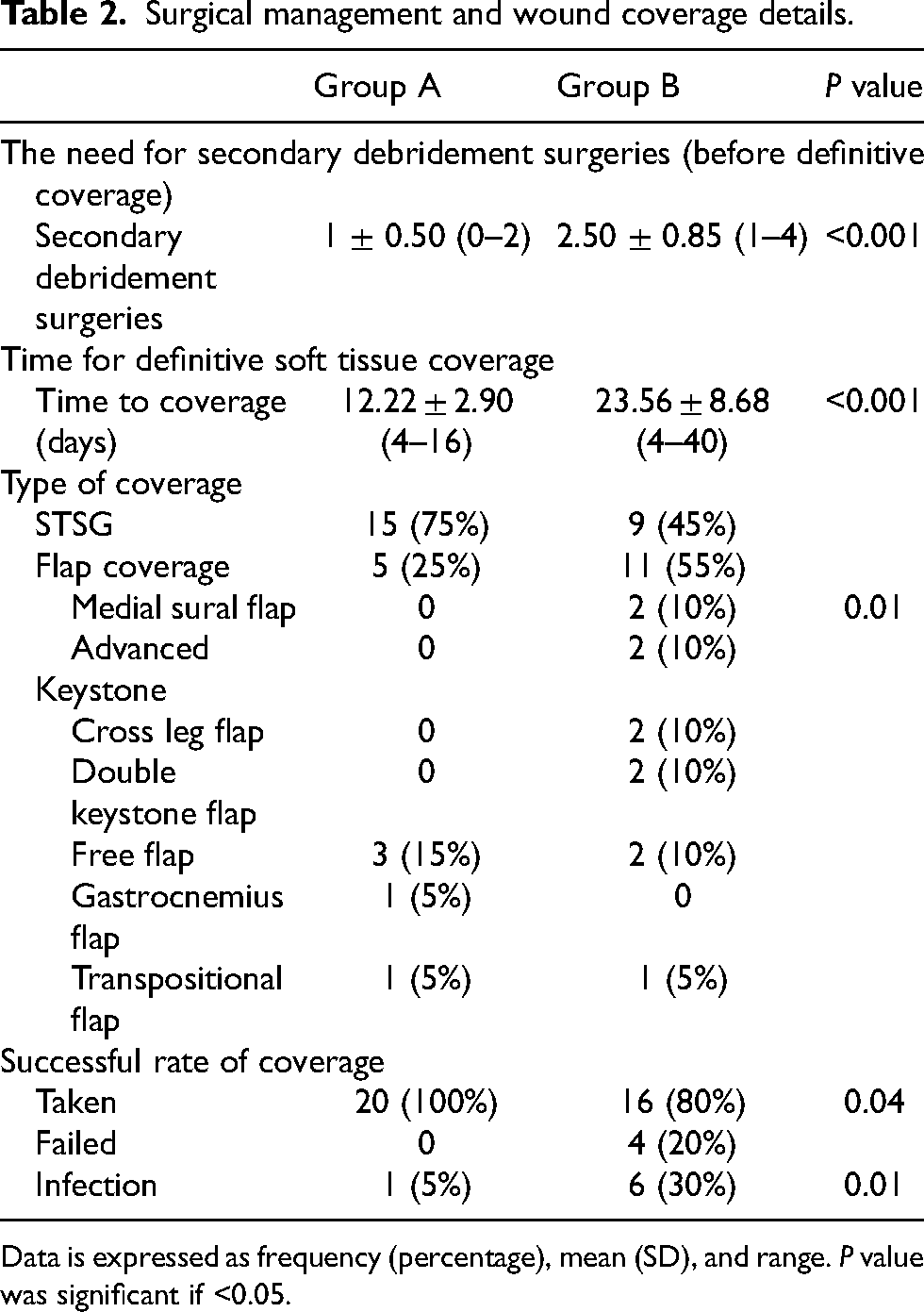
Data is expressed as frequency (percentage), mean (SD), and range. P value was significant if <0.05.
Discussion
The usefulness of NPWT or VAC in managing complex lower limb wounds, especially those associated with severe forms of open fractures, was proved in the literature,4,19–21 leading to an increasing trend of its use over the past decade. 12
Although we recently introduced VAC in our centre, the early results obtained from the current studies are promising. They showed lower infection rates and less need for complex coverage procedures such as different forms of flaps.
In the current study, infection rates were significantly higher in the group treated with conventional dressing; the same results were reported in various literature. A systematic review by Liu et al. included 14 studies constituting 909 patients diagnosed with open fractures (over 60% of them were grade III) aiming at comparing the results of using NPWT with conventional dressing in managing wounds associated with these open fractures. Their results showed that NPWT significantly reduced the infection rates, wound healing time, wound coverage time, amputation rates and length of hospital stay; however, the difference was insignificant regarding fracture union. 4
In a retrospective cohort study by Blum et al., 22 evaluating the role of NPWT on deep infection rates after managing open tibial fractures, 166 (72%) fractures were treated using the NPWT, while 63 (28%) were managed by conventional dressing. The percentage of open fractures grade III fractures was significantly higher in the NPWT group than in the conventional dressing group, 123 (74%) versus 36 (57%), respectively, P = 0.01. They reported significantly lower infection rates with the NPWT than conventional dressing, 8.4% versus 20.6%, respectively, P = 0.01; furthermore, after controlling other factors using a multivariate analysis model, using NPWT reduced the risk of deep infection by about 80% (OR: 0.22 (95% CI: 0.09–0.55); P = 0.001).
In a prospective randomised study by Stannard et al., 23 the authors compared the results of using NPWT to conventional dressings while dealing with 62 severe open fractures (92% were open type III), which included both upper and lower limb fractures (42% were tibial fractures), 25 fractures were treated with conventional dressing while 37 had NPWT, patients were followed for an average of 28 months. Infection rates were significantly higher in the conventional dressing group, 28% versus 5.4% for the NPWT group, P = 0.024. Furthermore, the authors evaluated tibial fractures separately; they reported the same trend of increased infection rates in patients who received conventional dressing.
On the contrary, in a larger study (The WOLLF Randomised Clinical Trial) by Costa et al., the authors investigated the difference between standard dressing compared to NPWT while managing wounds related to severe lower limb open fractures, they reported that the rate of deep surgical site infection was lower in the NPWT group compared to standard dressing group at 30 days postoperatively (7.1% vs. 8.1%, respectively), however, the difference did not reach statistical significance (P = 0.64). 24
We found a significant difference regarding the complexity of secondary wound coverage in the selected open grade IIIB tibial fractures, where in the VAC group, 75% of the wound required coverage using a simple STSG, while in the convention dressing group, 55% needed some sort of graft. Contrary to our results, Blum et al. reported that the group treated with NPWT required more free flaps to cover the soft tissue defects compared to patients managed with the conventional dressing, 47 (28%) versus 9 (14%); respectively, P = 0.03. 22 Furthermore, in the study by Stannard et al., 23 the authors reported that delayed primary wound closure was possible in 63% of their patients; however, the study included all types of fractures (tibial fracture represented 42%), and various grades of open injuries.
Although we did not perform a cost-effectiveness analysis, this issue should be considered before the wide adoption of the NPWT or VAC technique in wound management, as there were some concerns regarding this particular issue in the literature. In a Cochrane review by Iheozor-Ejiofor et al., after evaluating seven RCTs including 1381 participants, reported that the evidence was of moderate certainty regarding whether NPWT could improve the number of wounds healed after open fractures compared to the conventional dressings, which led to the conclusion that NPWT could not be considered as a cost-effective treatment (at least in a UK setting). 25 Furthermore, results from a more recent RCT (the WOLLF trial) found that NPWT is unlikely to be considered a cost-effective management option for wounds associated with severe lower limb open fractures. 26
We admit the limitations of the current study. First, although this was a prospective clinical trial, there was no randomisation, which could create a source of bias. Second, we only reported the in-hospital experience, and the fate of each patient in both groups should be followed up and reported. Third, no cost-effectiveness analysis was carried out. Last, the relatively small number of included patients could be attributed to including only one type of fracture of a specific degree.
Conclusion
Although the role of VAC in wound management is well established in the literature, reports regarding its role in managing severe open fracture wounds are rare in our area. We found that the initial results are encouraging, leading to lower infection rates and less cumbersome reconstruction procedures; however, further evaluation of the patient's final outcomes is mandatory, along with an evaluation of the cost-effectiveness of the procedure.
Footnotes
Acknowledgment
The authors would like to thank all the team members of our centre's trauma and microsurgery units.
Authors’ contribution
O.F. and K.A.E. conceived and designed the study. H.A. and A.M.H. carried out data acquisition and assessment. A.A.K. and H.A. analysed and interpreted data, drafted the manuscript and designed the figures and tables. O.F. and K.A.E. did the critical revision. All authors discussed the results and commented on the manuscript. All authors read and approved the final manuscript. The first and the second authors contributed equally to the manuscript.
Availability of data and material
All the data related to the study are mentioned within the manuscript; however, the raw data are available with the corresponding author and will be provided upon a written request.
Consent to participate
Informed consent was obtained from all participants included in the study.
Consent for publication
Patients signed informed consent regarding publishing their data and photographs.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This article does not contain any experimental studies with human participants or animals performed by any of the authors, and the ethical committee of our institution approved it: Faculty of Medicine, Assiut University, Egypt (IRB no.: 17100992) (Telephone, Fax.+20882332278, ethics-committee12@yahoo.com, IRB-Asyut@aun.Edu.eg, http://afm.edu.eg), Study setting: Trauma unit, Orthopaedic department, Assiut University Hospital, Assiut, Egypt. Clinical Trial Registration: (NCT04063111).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.