
Abstract
Introduction
The objective of this case series is to evaluate the clinical outcome of patients with tibial shaft fractures treated by suprapatellar nailing at a 2-year follow-up and to review available literature concerning this approach.
Method and material
This is a retrospective single-centre case series to evaluate patients' post-operative status at 2-year intervals. Fifteen (15) patients underwent intramedullary nailing with a supra-patella approach during the year 2019–2020 and consented to participate in this case series. Patients were regularly followed up in the outpatient clinic and evaluated in terms of range of movement, walking status and radiologically with RUST score and tibia alignment. Their functional outcome was assessed by a questionnaire including OKS, VAS, and Kujula scores.
Results
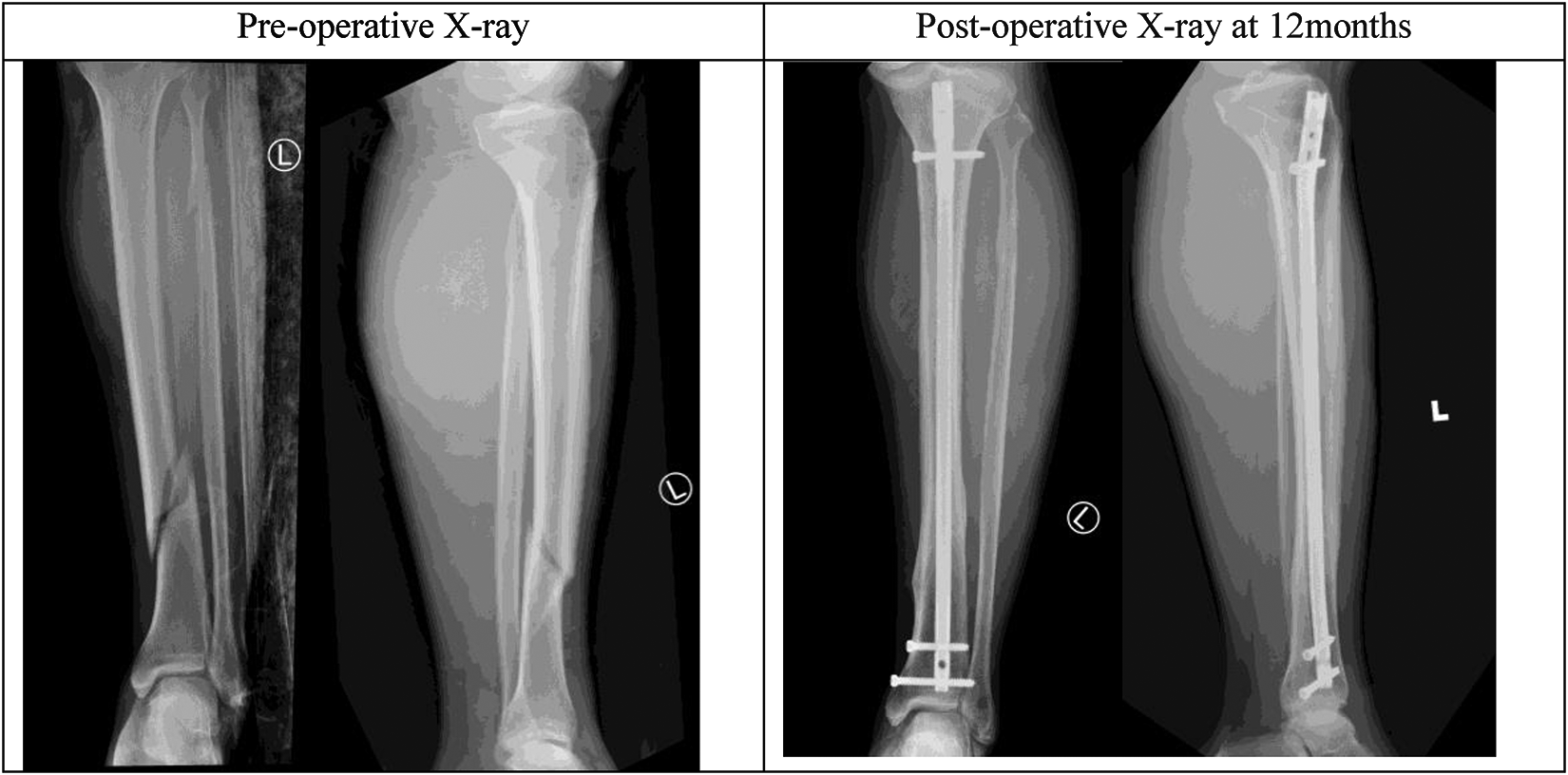
At post-op 2 years intervals, all patients had radiologically healed fractures as evidenced by RUST score and tibia alignment within five degrees in the coronal and sagittal plane, the functional outcome of the suprapatellar approach was satisfactory in the visual analogue scale and various knee scores. All patients achieved a full range of movement and could walk unaided.
Discussion
Technical tricks and tips for the suprapatellar approach are discussed. Literature review showed satisfactory outcomes for intramedullary nailing for tibial shaft fracture in different parts of the world. Compared with the infra-patellar approach, the suprapatellar approach is superior in fracture alignment but has no significant difference in terms of pain, disability and range of movement. Potential risk of suprapatellar approach is discussed including possible cartilage damage and intra-articular sepsis.
Conclusion
There is a good clinical outcome of the suprapatellar approach to tibial nail radiologically and functionally. Results are in line with the literature review, which also showed that compared with the infra-patellar approach, the suprapatellar approach is associated with better alignment and less knee pain but no significant difference in range of movement and disability.
Introduction
Intramedullary (IM) nail fixation is the treatment of choice for unstable, displaced tibial shaft fracture. The goal of treatment is to restore the length, alignment, and rotation of the tibia. IM nailing allows fixation with minimal surgical dissection and immediate mobilization with full weight bearing as the nail acts as a load-sharing device.
There are two main approaches to tibial nailing depending on knee positioning, Infra-patella approach with knee flexing at least 90 degrees has been the standard procedure, however, a high incidence of anterior knee pain of 31% to 86% 1 has been reported. The suprapatellar approach with a knee in a semi-extended position was developed to reduce anterior knee pain and other disadvantages related to the infra-patellar approach such as difficulty in intra-operative X-ray, difficulty in maintaining reduction, increased need for poller screws and pins, etc. In 2019, a multicentre clinical trial conducted in the United Kingdom showed the suprapatellar approach being associated with less anterior knee pain as compared with the infra-patellar approach. 2
A similar case series in Italy 3 illustrated a full range of movement and good functional outcomes with complete healing in all cases. This case series analysed Hong Kong's local data to evaluate the outcome of the suprapatellar approach for tibial fracture nailing.
The objective of this case series is to evaluate the clinical outcome of a patient with tibial shaft fracture treated by suprapatellar nailing evaluated in terms of a range of movement, walking status and radiological RUST score at 2 years follow-up. A review of available literature about suprapatellar tibial nailing was undertaken.
Method and material
This is a retrospective single-centre case series to evaluate the patient's post-operative status 2 years after the index operation. Inclusion criteria were: adult patients between 18 and 70 years of age, closed fracture of tibial shaft. Exclusion criteria were severe knee osteoarthritis, history of previous surgeries on the same limb, history of septic arthritis over the same limb, underlying neurological disease, and open fracture.
The operation was performed with a supra-patella approach; details of the operation and technical tips will be discussed in “Discussion”
Post-operatively, patients started with full weight-bear walking exercises under the supervision of a physiotherapist with adequate analgesics. Patients were regularly followed up with an examination of the wound, functional outcome, and radiological healing of the fracture.
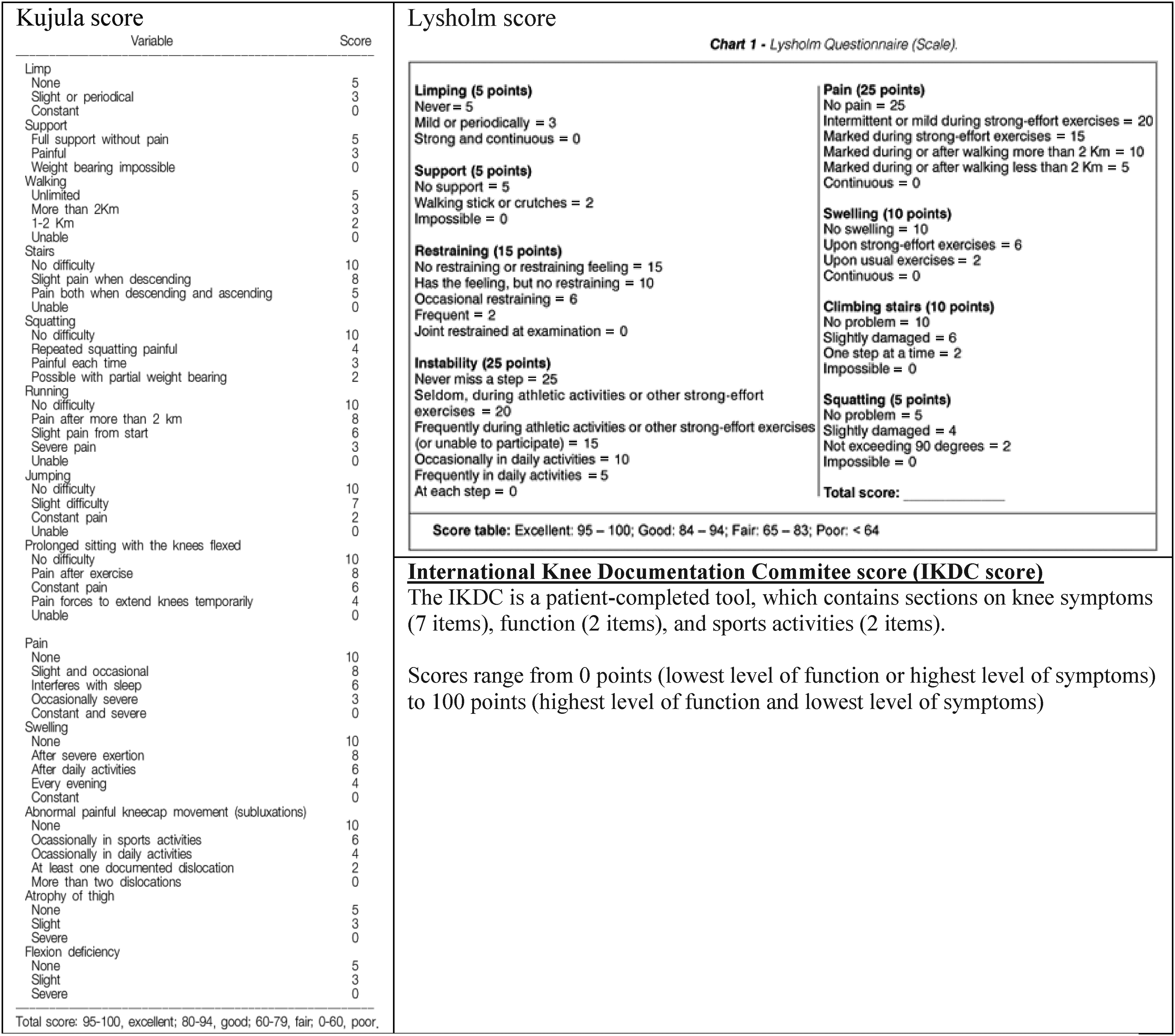
At 2 years post-op interval, patients were reviewed in an outpatient clinic during their follow-up, and 15 patients consented to participate in this retrospective case series. They were evaluated in terms of range of movement, walking status and radiologically with RUST score 4 and alignment of healed fracture. Alignment of the tibia was assessed by two individual surgeons, defined as well aligned if <5 degrees, both coronal and sagittal planes were assessed. Their functional outcome was assessed by a questionnaire including Oxford knee score, 5 Visual Analogue Scale, Kujula score, 6 Lysholm score and International Knee Documentation Committee score.
Literature on clinical outcomes, potential risks of the suprapatellar approach and comparison between infra-patellar and suprapatellar approaches were reviewed and included for discussion.
Results
Fifteen patients’ data were analysed. Patient demographics include three female and 12 male patients. Their age ranged from 23 to 61 years old. All patients walked unaided before the index fractures. Fractures 23 mm to 243 mm above the tibial plafond. Fifty-three per cent of them were in the middle one-third of the tibia and 47% in the distal one-third of the tibia, 13.3% of them were segmental fractures.
At post-op 2-year intervals, patients were evaluated in terms of range of motion, walking ability, radiological healing, alignment of tibia and functional knee scores.
Hundred per cent of the patients achieved a full range of movement, 14 (94%) patients walked unaided and one (6%) walked with a stick. Hundred per cent of the patients had radiologically healed fractures evidenced by a RUST score of 16. All tibial alignments were within five degrees of both coronal and sagittal planes, as reviewed by two independent viewers. The functional outcome of the suprapatellar approach was satisfactory, with an average visual analogue scale of 2, an average Oxford knee score of 46, an average Kujula score of 96, an average Lysholm score of 94 and an average International Knee Documentation Committee score of 81 (Table 1).
Result.
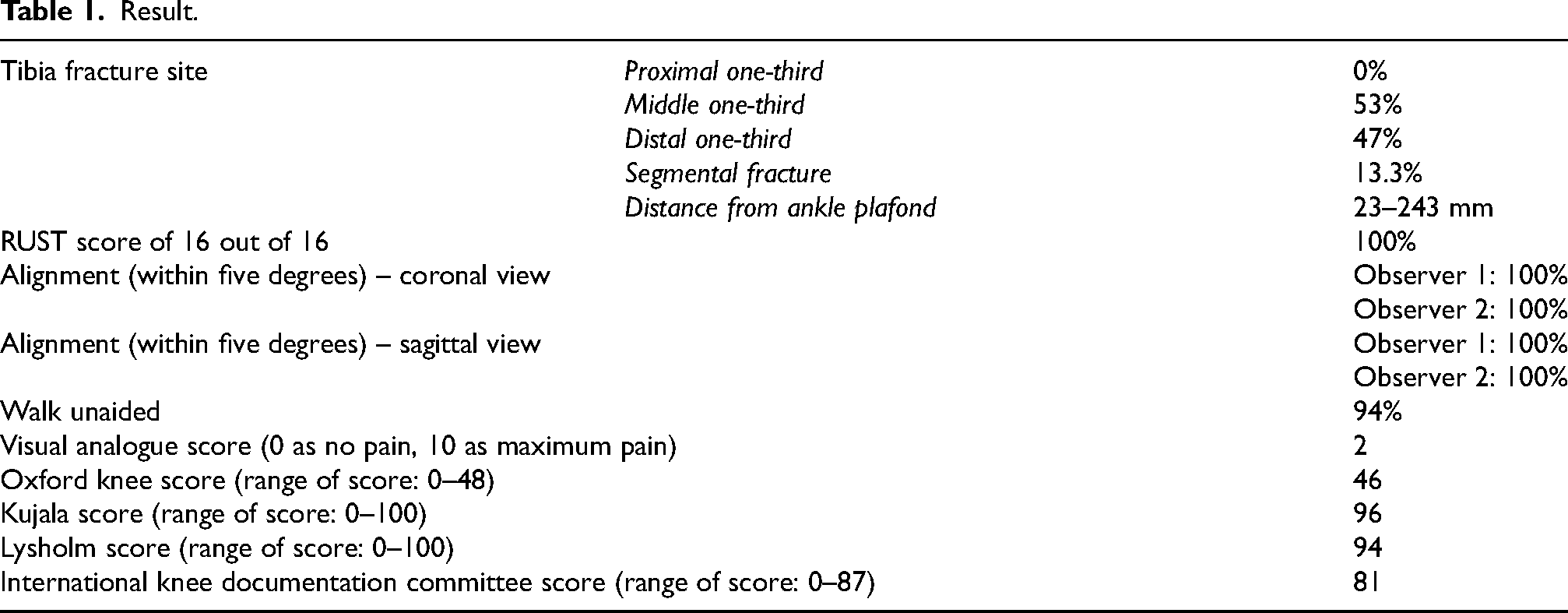
Forty-seven per cent of tibia fractures were within distal one-third of the tibia with the shortest distance to ankle plafond down to 23 mm. Fifty-three per cent of tibia fractures were at the middle one-third of the tibia. Two patients had segmental tibial fractures over the middle to distal one-third of the tibia. Poller screws or pins had not been used in any of the operations.
Our result showed that there was no problem in fracture healing, alignment, and fixation for tibia fractures regardless of the location of the fracture within the lower two-thirds of the tibia. The functional outcome of the suprapatellar approach was also satisfactory, as patients were restored to premorbid function with minimal knee pain.
There was no case of infection. One patient had reoperation for the removal of a prominent locking screw under local anaesthesia.
Discussion and literature review
Technical tips for suprapatellar approach for tibial nail insertion
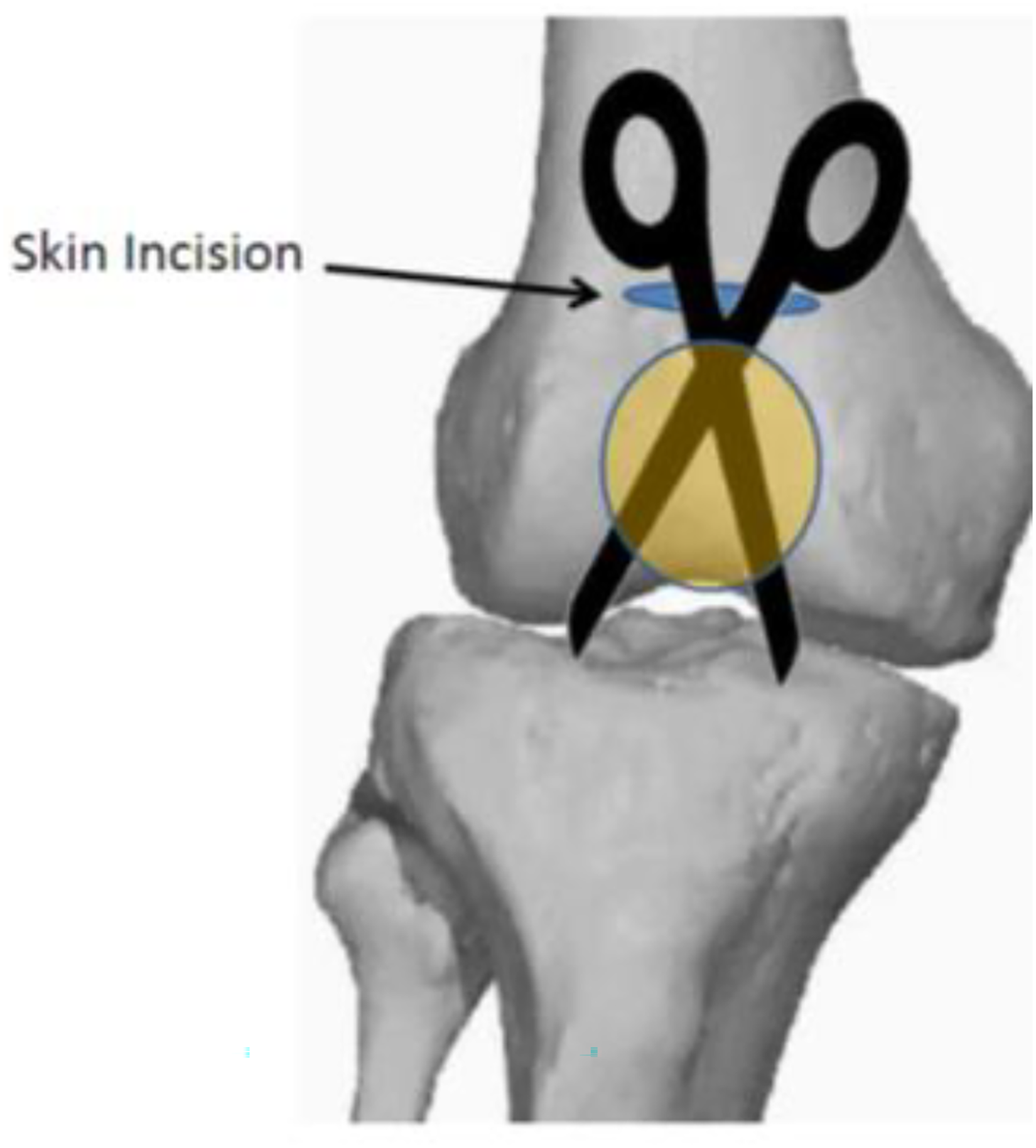
A surgeon should liaise with an anaesthetist to provide full muscle relaxation to allow easier access via the patellofemoral joint space. We suggest starting with a knee in 20 to 30 degrees flexion. A transverse skin incision over the suprapatellar area heals well with minimal scar. The quadriceps tendon was incised longitudinally for 5 cm proximal to the patella.
The suprapatellar pouch was popped by inserting a pair of blunt scissors into a patellofemoral joint (PFJ), all the way to the tibial tuberosity under the patella tendon, and then pulled upwards with the jaws wide open.
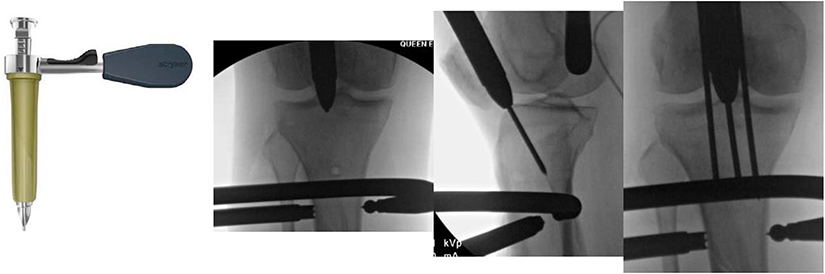
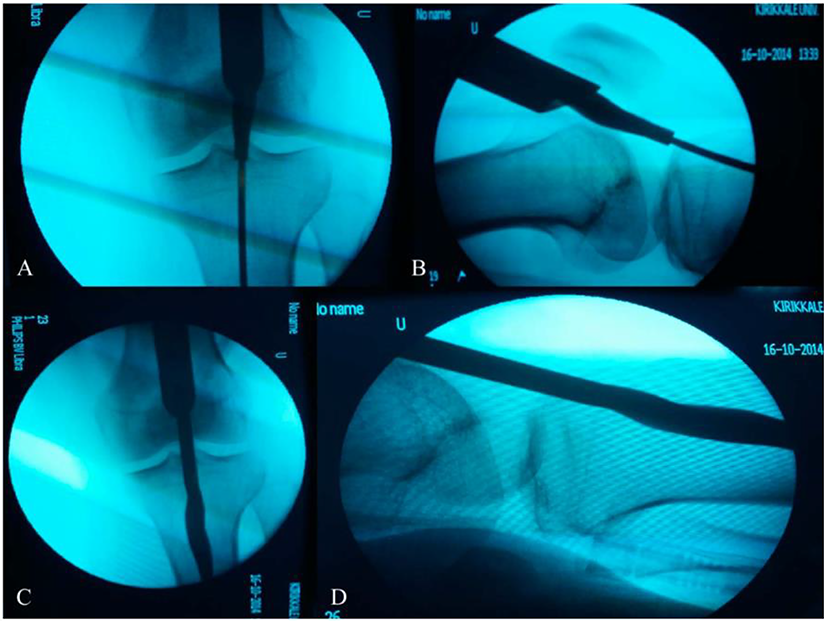
A silicon sleeve with a metal trocar was introduced for creating a retro-patella portal while protecting the patella-femoral articular surfaces from reamers and the tibial nail. If the patellofemoral space was too tight, arthrotomy was extended medially to partially sublux the patella. The entry site was confirmed with an X-ray.
The next step is to insert the metal trocar and silicon protection sleeve to touch the tibia, these could be lubricated by the application of liquid paraffin outside the silicon sleeve, and between the metal and silicon sleeves. If a patellofemoral joint is still tight, consider retinacula extension.
The entry point should be in line with the tibial shaft and equidistant from the medial and lateral articular surface on the anterosuperior corner of the tibia. 7
Protection sleeves were advanced until they touched the proximal tibia in order to minimize the escape of reamed bone into the joint. Reaming was undertaken after protection sleeves were anchored with pins. Though anchored, the operating team still needs to look out for the unlikely event of dislodgement of the protection sleeves during reaming, as this could cause serious irreversible damage to the patella-femoral joint (PFJ).
 This is a fluoroscopy picture published in the Journal of Orthopaedic Trauma, in January 2019 which showed the potential danger for PFJ.
This is a fluoroscopy picture published in the Journal of Orthopaedic Trauma, in January 2019 which showed the potential danger for PFJ.
Remove the anchoring pins and the metal sleeve but keep the silicon sleeve before insertion of the nail. A nail of appropriate size was inserted after reaming, with the soft silicon protection sleeve in place to protect the PFJ. After nail insertion, knee joint irrigation was carried out with the soft sleeve in place to facilitate the egress of wash fluids. Closure of soft tissue and skin was only undertaken after copious irrigation of the knee joint to remove all reamed bone from within the joint cavity. Ensure there is no retained reamed bone with a lateral view X-ray before skin closure.
Clinical outcome of suprapatellar approach
Our results showed satisfactory outcomes clinically, radiologically and functionally. In the literature review, the case series from Italy also showed good clinical outcomes with no wound complication, no post-operative infection and a good functional outcome score. All 25 patients in the series showed a full range of movement and full RUST score. 3 Another prospective case series reviewing the 1-year result of suprapatellar intramedullary nailing showed good tibial alignment, union and full range of movement. Immediate post-operative arthroscopy, 1 year MRI and clinical presentation showed no adverse sequelae in the patellofemoral joint. 8
Comparing suprapatellar and infra-patellar approaches
Infra-patella and suprapatellar approaches are compared in terms of different parameters in various articles. In the latest meta-analysis in 2021 JOSR, a systemic review and meta-analysis which included 12 studies showed suprapatellar approach has less post-operative pain and better functional outcomes. Another meta-analysis in 2018 IJS 9 which included eight studies showed suprapatellar approach has SHORTER fluoroscopy time, lower VAS pain score, better sagittal plane alignment and lower incidence of angular malalignment; however, there is no significant difference in operation time, coronal plane alignment, incidence of post-operative deep infection, non-union and secondary operation. Another cohort study published in the Journal of Orthopaedic Trauma also showed suprapatellar technique results in a significantly lower rate of malalignment compared with the infra-patellar IMN technique. 10
Reviewing randomized controlled trials and case series, the suprapatellar approach results in less anterior knee pain, 2 lower radiation exposure, 11 and lower risk of malunion but there is no significant difference in functional level. 12
Potential risks of the suprapatellar approach
Compared with the infra-patella approach, surgeons may have worries concerning cartilage damage and the risk of joint sepsis due to the surgical invasion of the joint space. Upon literature review, post-procedural macroscopic and arthroscopic assessment of the articular surfaces for chondral damage has shown no evidence of injury in cadavers.13, 14
Another cadaveric study in 2016 15 also showed a similar rate of knee structure damage comparing the infra- and supra-patella approach.
There is also no increased risk of intra-articular infection compared with the infra-patella approach in a study in 2017 comparing post-operative knee sepsis. 16
Achieving good tibial alignment
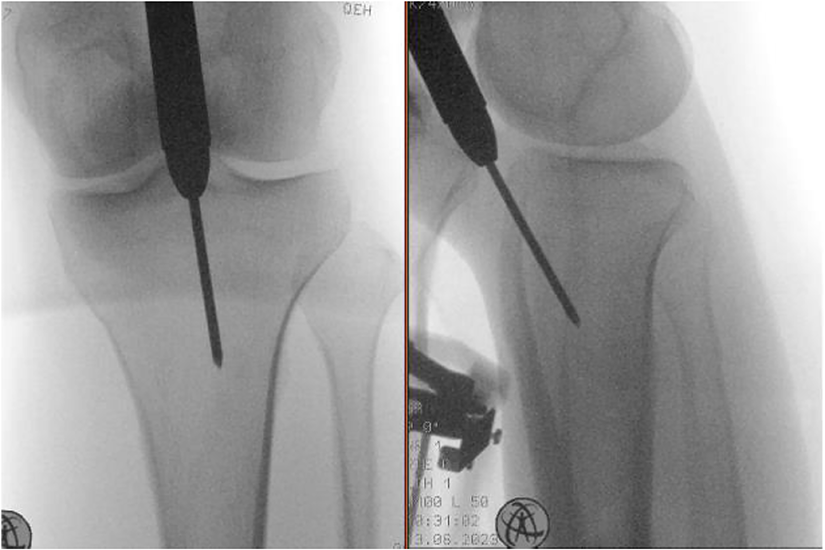
In the literature review, 37% 17 of tibial fractures require percutaneous or open reduction. With the position of 30 degrees knee flexion in suprapatellar approach, reduction of fracture and entry of nail is technically easier, as borne out in previous cohort study. 10 In our series, all reduction can be achieved by closed reduction. Poller screw or poller pin had been avoided even in the very distal fractures. It could reduce the risk of iatrogenic fracture caused by inserting a poller screw or poller pin.
From our results, distal one-third of tibia fractures were well reduced with satisfactory results. The most distal fracture was just 23 mm from the ankle plafond. Indication of tibial nailing can be extended to very distal tibia fracture by suprapatellar approach for tibial nails. Positioning the knee at a semi-extension position will be easier for X-ray and maintenance of reduction. With an infra-patellar approach, we need to flex the knee to 90 degrees or more. It is more difficult to manipulate the limb and the C-arm to visualize consistent anteroposterior and lateral views. Hence, reduction may be lost during a change of position.
Limitations and strengths of this study
This study is a case series hence there is no control group for comparison. Moreover, this is a single-centre study and thus of a limited sample size. Although we endeavour to apply the SPI approach for nailing proximal shaft fractures, we did not encounter proximal shaft fractures during this study period.
However, the strength of this study includes a 2-year interval of follow-up. It is the first Asian case series about supra-patella approach clinical outcomes. As the Southeast Asian population generally has a smaller body build as compared with the non-Asian population reported in the literature, this series verified that the SPI approach is equally applicable despite a smaller body build. We also made use of multiple functional scores for evaluation. Technical tips and tricks were presented for each step of operation.
Conclusion
To conclude, this case series showed good clinical outcomes of the suprapatellar approach tibial nail radiologically and functionally. Our results are in line with literature reviews. Compared with the infra-patellar approach, the suprapatellar approach results in better alignment and less knee pain, but no significant difference in terms of range of movement and disability. Though there are potential risks, current evidence showed no increased risk of intra-articular sepsis, and no cartilage damage of the patella-femoral joint as evidenced by imaging, clinical examination, and knee arthroscopy.
To imply in clinical practice, we suggest an increase in the application of the suprapatellar approach for tibial nailing for tibial shaft fracture. We aim to decrease the incidence of knee pain while maintaining good alignment and functional scores. We also include technical tips for the operation, with readily available implants and the tips we included, we believe the learning curve of this approach is not steep.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.