
Abstract
Background
The treatment of dislocated hip hemiarthroplasty in low-demand elderly patients is controversial due to poor results with closed reduction, and significant complications with exchange arthroplasty. This case series demonstrates the use of a novel, simple surgical technique for hip hemiarthroplasty containment without resorting to exchange arthroplasty.
Methods
Eleven patients where screw-augmented cement shelf acetabuloplasty procedures were performed were retrospectively identified. All surgeries were performed by a single attending surgeon, at a level-one trauma center, from 2015 to 2022. Previous dislocations, interventions, co-morbidities, mobility level, and posterior wall deficiency were recorded from the patient's charts. The following outcome measures were recorded: operative time, blood loss, perioperative complications, early and late infections, shelf loosening, subsequent dislocations, and the need for additional procedures.
Results
The median duration between hip hemiarthroplasty and shelf procedure was 56 days. The mean duration of the surgical procedure was only 63 min, and the mean blood loss was only 250 mL. There was only one instance of loosening of the cement shelf. Two patients had surgical site infections leading to sepsis and death. In two patients, the femoral head was exchanged to improve stability. All patients were allowed immediate weight bearing after the procedure.
Conclusions
Shelf acetabuloplasty is a simple, inexpensive, and safe procedure to salvage recurrent hip hemiarthroplasty dislocation in low-demand patients. Shorter surgical duration, relatively lower blood loss, and immediate weight bearing render this an attractive procedure for this fragile population.
Keywords
Introduction
The incidence of hip fracture among the elderly, although declining, remains significant. Hip hemiarthroplasty (HA) is used to treat the majority of the fractures of the femoral neck in these patients. 1 The stability of hip HA is inherently greater than that of total HA (THA), chiefly owing to its higher head-to-neck ratio and, consequently, greater jump distance. 2 Nevertheless, dislocation is one of the most common complications of HA, with reported rates of dislocation ranging from 1% to 15%. 2 Closed reduction of a dislocated HA, although non-invasive, is often complicated by recurrent dislocations. 3 Patients with recurrent dislocations typically require either conversion to THA or excision arthroplasty. 4 Dislocation following a HA is also associated with significantly higher mortality in short-term and medium-term follow-up. 3
Various authors have examined risk factors associated with HA dislocation. Surgical approach, limb length discrepancy, type of prosthesis, method of capsular repair, and surgeon's arthroplasty volume are considered surgeon-modifiable factors for HA. 5 Patient-related factors, such as smaller center-edge angle, 6 posterior acetabular sector angle, and posterior wall angle, are associated with a shallow acetabulum and HA dislocation. With a few exceptions, most authors agree that dementia and cognitive dysfunction are associated with dislocation after hip arthroplasty.7,8 Importantly, defects of the posterosuperior acetabular wall have been identified in patients with recurrent hip dislocations. 9 These associated patient-related factors imply that adequate posterior wall stability and coverage help to prevent HA dislocations in patients.
The etiology of HA dislocations guides the treatment algorithm utilized to prevent further HA dislocations. 4 Deficient posterosuperior coverage can be due to a shallow acetabulum or deficient posterior wall, leading to HA instability. Patients with deficient posterosuperior coverage often require conversion to a THA with complex acetabular reconstructions, such as impaction grafting, 10 cages, augments, or allografts as implantation of a routine acetabular component may be difficult in the presence of acetabular defects. 11 Multiple authorities agree that acetabular reconstructive procedures are massive undertakings associated with significant complications like intensive care unit admission, death, and recurrent dislocations. These complications may be detrimental in fragile, elderly patients. 12 Results of acetabular reconstruction are unpredictable, with multiple studies citing a high failure rate of one or more of the above procedures. 13 Therefore, current pitfalls with acetabular reconstruction surgeries have led to a so-far unmet need for more straightforward procedures.
Um et al. 14 and Rogers et al. 15 used an antibiotic-loaded cement shelf to prevent the dislocation of cement spacers used for two-stage exchange arthroplasty for septic revisions. Mussa et al. 16 used a novel two-stage screw with cement technique to address large uncontained defects in low-demand elderly patients. Since pain relief and restoration of function are the main objectives of revision hip arthroplasty in the elderly, we used this technique to salvage unstable bipolar HAs with instability due to deficient posterosuperior acetabular walls. This study aimed to evaluate the safety and efficacy of augmented cementoplasty for treating recurrent hip dislocations following HA in patients with deficient posterosuperior acetabular coverage.
Material and methods
A single attending surgeon (TL) performed augmented cementoplasty for the treatment of recurrent hip dislocations following HA in low-demand patients with deficient posterosuperior acetabular coverage. Acetabular revision surgeries performed by the surgeon at a level-one trauma center from 2015 to 2022 were obtained. The surgeries were performed at an urban academic center in Ohio. The inclusion criteria included patients with hip hemiarthroplasty with a history of hip dislocations (at least one). As required in any hip revision surgery, exclusion of infection was necessary. Detailed clinical examination and lab investigations were carried out to assess limb length and function and to exclude infection. Imaging includes routine radiographs, while computed tomography (CT) scans were obtained in patients with more than two dislocations to help assess the preoperative acetabular morphology and presence of deficiency.
Surgical technique
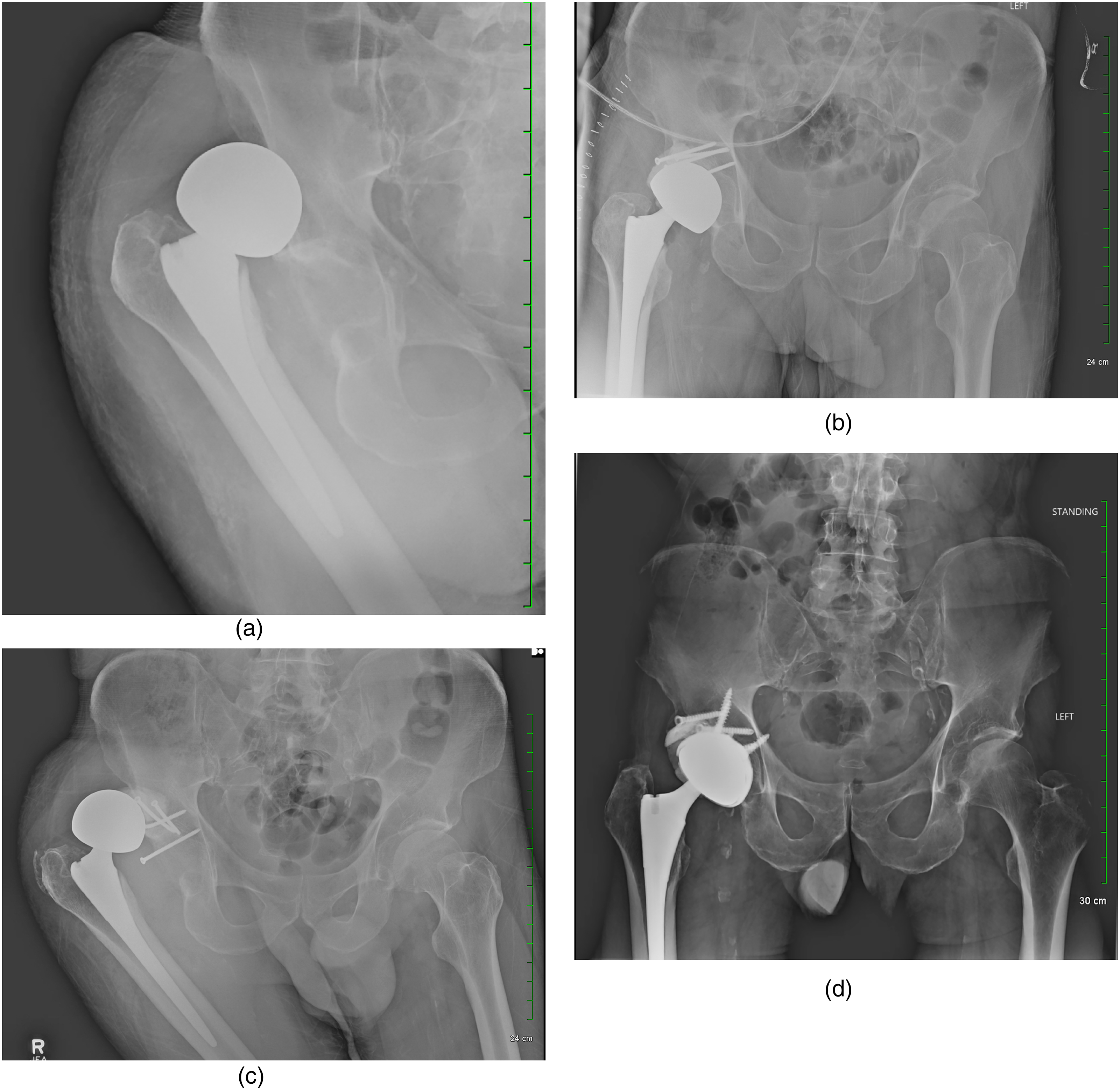
Patients were placed in the lateral decubitus position, and routine preoperative preparation was carried out. Utilizing the posterior approach, the hip joint fluid sample was obtained. Subsequently, the acetabulum was exposed after dislocating the femoral head. Tissue for biopsy was obtained. The femoral stem was assessed for loosening and anteversion of the femoral neck. The acetabular defect was carefully assessed. Four to seven screws were inserted in and around the defect. In one case, a one-third tubular plate was fixed superficial to the cement shelf, with screws on either side of the shelf (Figure 1A to D). The screw heads were protected with bone wax to avoid bone cement blocking the access to the screw heads. Subsequently, bone cement was applied to the defect. During the period of cement consolidation, the bipolar head was continuously rotated to avoid adhesion of the cement to the surface of the head. Once the cement was set, the hip joint was taken through the range of motion to assess stability and screen for impingement. Additional soft tissue release in the form of an iliopsoas tenotomy was performed in one patient with a neglected dislocation. This was followed by the closure of the hip capsule and routine, layered closure of the surgical site. Abduction braces were used in all patients. Postoperative weight bearing was allowed as tolerated.
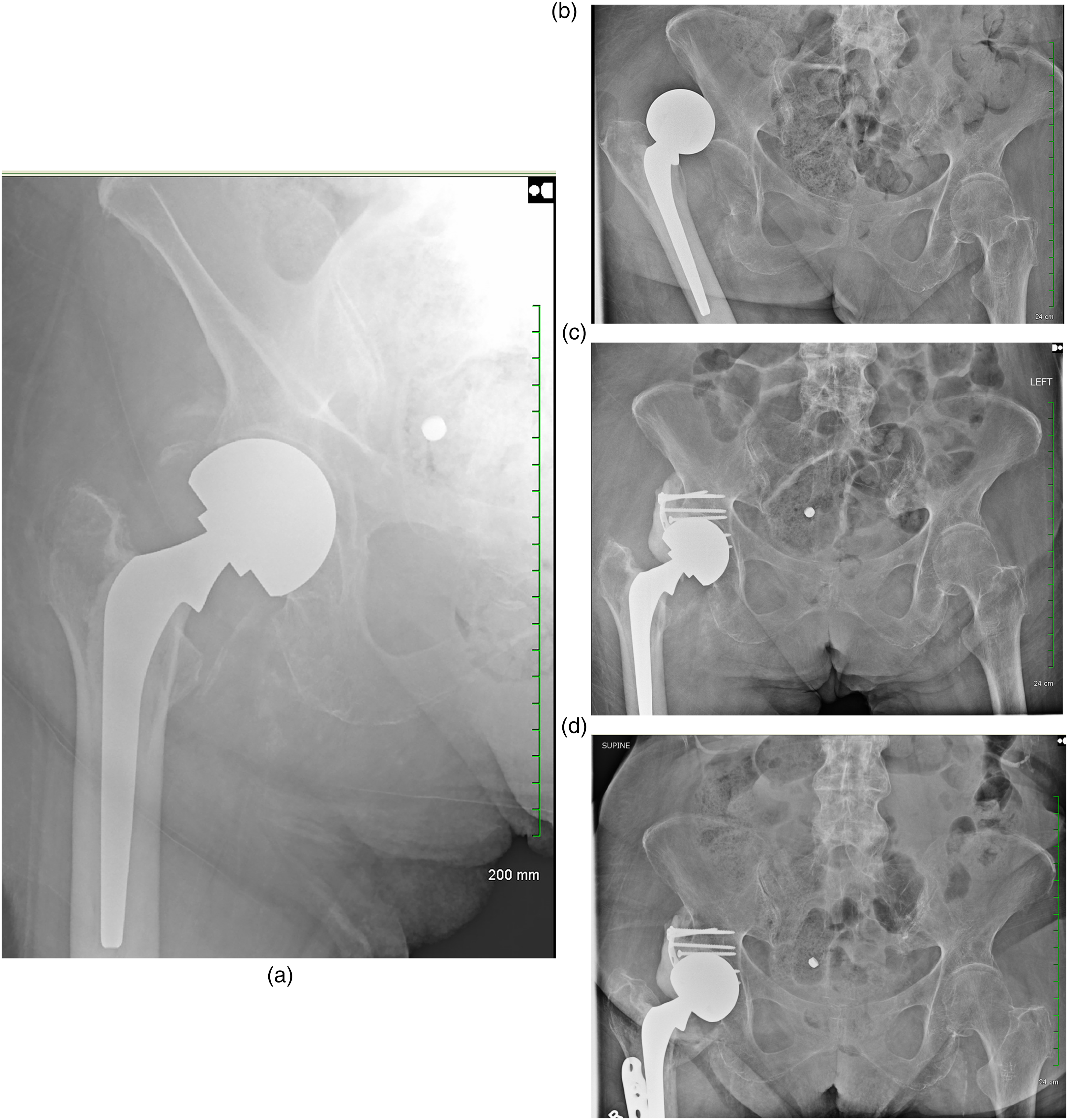
(A) Patient 1 – postoperative radiograph after cemented bipolar hemiarthroplasty. (B) Patient 1 – dislocation nearly two months after hemiarthroplasty. (C) Patient 1 – Immediate post-operative radiograph after cement shelf acetabuloplasty. (D) Patient 1 – two years after shelf acetabuloplasty.
Eleven consecutive patients were retrospectively identified by chart review. All procedures were performed by the senior author. Patients who had undergone HA instability treated with a cement shelf procedure were included. Variables recorded included demographic details, mobility status, number of episodes of dislocation, chronology of dislocation episodes, acetabular defect (if present), co-morbidities (including, but not limited to, neuromuscular weakness), postoperative infection, and mortality (if applicable). The eventual fate of the cement shelf was also followed for loosening, displacement, and further dislocations, if any, were identified. Patients who were eventually converted into total hip arthroplasty were also identified. Descriptive statistical methods used included the measures of central tendency.
Results
The preoperative characteristics of the patients are detailed in Tables 1 and 2.
Pre-operative and demographic features of the patients.
HA: hemiarthroplasty; ASA: the American Society of Anesthesiologists; CCI: Charlson comorbidity index.
This patient had a neglected dislocation with the formation of a false acetabulum.
Summary of demographic and pre-operative details of the patients.
HA: hemiarthroplasty; ASA: the American Society of Anesthesiologists; CCI: Charlson comorbidity index.
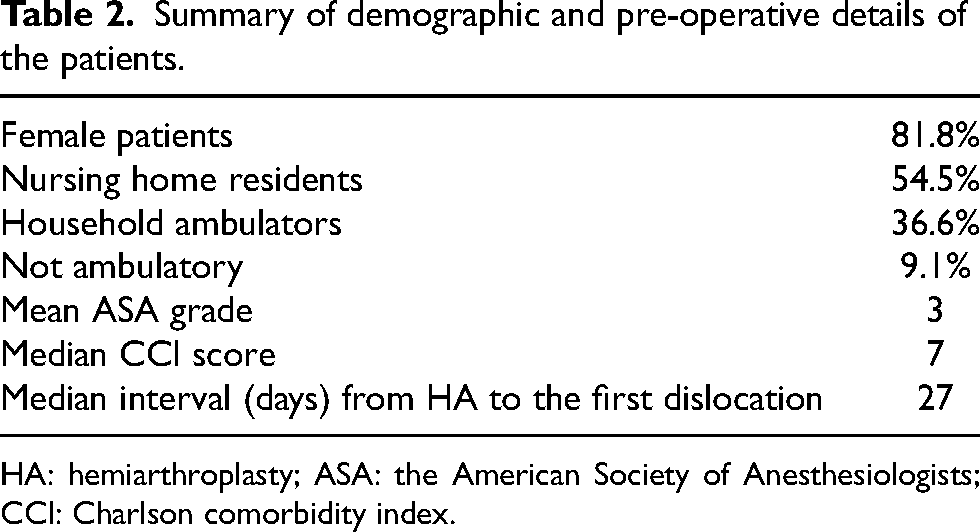
There were nine females and two males with a median age of 88 years. More than half of the patients were nursing home residents and needed continuous help with mobilization. The median ASA was 3 (ASA 3, n = 9; ASA 4, n = 2). Five patients had posterosuperior wall defects, while one patient (case #4) had a chronic dislocation, resulting in the formation of a false acetabulum (Figure 2A to E). None of the patients had loose femoral stems. The mean number of dislocations was 2.4. After HA, the first dislocation occurred at a median of 27 (range 5–960) days.
(A) Patient 4 – neglected posterior dislocation with pseudoacetabulum formation. (B) Patient 4 – axial CT scan demonstrating neglected posterior dislocation with pseudo acetabulum formation. (C) Patient 4 – six months after cement shelf acetabuloplasty. (D) Patient 4 – distal femoral fracture 6.5 months after cement shelf acetabuloplasty. (E) Patient 4 – one year after shelf acetabuloplasty and 5.5 months after distal femoral fracture. The shelf is intact, and there has been no dislocation.
The median gap between HA and shelf procedure was 56 days. The mean duration of the surgical procedure was 63 min, and the mean blood loss was 250 mL. A median of five screws were used. The median follow-up among seven patients alive at the time of writing this manuscript was 76 weeks. Four patients died in the follow-up period, two of which were due to causes unrelated to their hip surgery (Patient #1 and Patient #8). Two patients suffered postoperative surgical site infection and resultant multi-organ dysfunction and death (Patient #5 and Patient #10). Two other patients had postoperative surgical site infections, which could be managed by antibiotic treatment in one (Patient #2) and debridement and lavage in another (Patient #4). In one patient (Patient #10), an explanation of the prosthesis was considered in view of deep infection. However, the family refused operative debridement and lavage, and antibiotics, according to the sensitivity of the cultured organism, were started. In two patients (Patient #3 and Patient #11), a femoral head exchange was performed to optimize stability. There was only one instance of loosening of the cement shelf (Patient #6) that had to be revised to THA (Figure 3A to D). The procedure involved the excision of the loose portion of the cement mantle, conversion of the bipolar head to a 32-mm modular head, and placement of an uncemented acetabular liner. The stem was well fixed, with an appropriate version, horizontal and vertical offset, and was thereby retained. All patients were allowed immediate weight bearing after the procedure. Intraoperative characteristics and postoperative course of the patients are detailed in Table 3.
(A) Patient 6 – first dislocation after hemiarthroplasty. (B) Patient 6 – immediate post-operative radiograph after shelf acetabuloplasty. (C) Patient 6 – dislocation, six weeks after shelf acetabuloplasty. (D) Patient 6 – nine months after conversion to total hip hemiarthroplasty (THA).
Intra-operative details and the post-operative course of the patients.
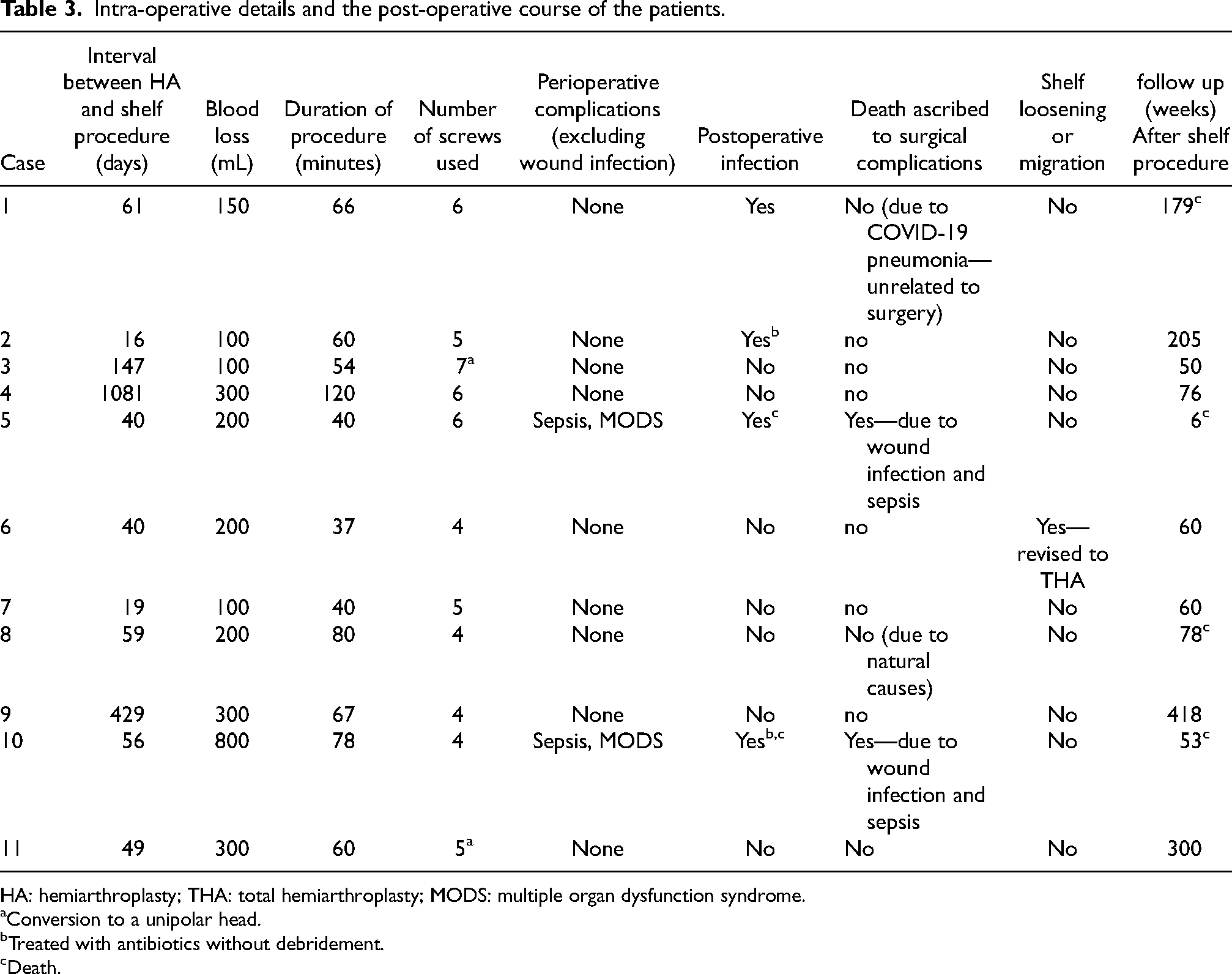
HA: hemiarthroplasty; THA: total hemiarthroplasty; MODS: multiple organ dysfunction syndrome.
Conversion to a unipolar head.
Treated with antibiotics without debridement.
Death.
Discussion
The most important finding of our study is that the cement shelf procedure is a simple and effective procedure to treat instability after Hip hemiarthroplasty. Conversion of HA to THA carries a substantial risk of complications, with multiple studies highlighting significant rates of prosthesis loosening and dislocations. 17 Multiple authors have regarded conversion THA to present challenges similar to revision THA rather than a primary THA.18,19 Defects of the bony acetabulum often necessitate complex acetabular reconstructions requiring allograft, augments, or special implants. They are best treated by a dedicated hip surgeon in a unit with expertise in revision arthroplasty. 17 Owing to poor bone stock and precarious fixation, weight bearing is deferred in these patients for 6–12 weeks. 20 Large case series have demonstrated increased complications with delayed weight bearing in the geriatric population. 21 Considering all these factors, the need for more straightforward procedures, allowing immediate weight bearing has been felt by many authors.
Two-stage revision arthroplasty is frequently complicated by the dislocation of the cement spacer, resulting in significantly poorer outcomes. 20 To address this problem, Jin et al. 22 used a screw-augmented supra-acetabular cement shelf in infected hip arthroplasties. They reported a marked reduction in dislocation rates and dislodgement of cement spacers. Um et al. 14 also reported significantly superior outcomes in two-stage exchange arthroplasty with the use of screw augmented supra-acetabular cement spacer. To our knowledge, a similar technique has not been reported for treating instability of bipolar hemiarthroplasty.
In our study, one patient (#6, n = 1, 9.1%) experienced dislocation, which is comparable with other methods of treating instability with bipolar hemiarthroplasty. Various procedures to address the instability have included femoral stem repositioning, 23 using constrained acetabular components, increasing neck offset, 24 soft tissue repair, and trochanteric advancement. 25 Unfortunately, the containment rate with these procedures remains a dismal 60%–80%.23–25 Recently, the use of dual mobility acetabular components has been associated with zero recurrent dislocation. 26 We are not aware of any case series where bipolar HA was revised to a dual mobility acetabular component. Excision arthroplasty (EA) has been advised by some authors to treat failed HA or THA. However, EA is associated with pain, disability, and poor quality of life, leading to further functional deterioration and loss of independence. 27 Due to these reasons, we chose not to resort to EA in our patients.
The mean blood loss in our study was 250 mL. This significantly contrasts with conversion arthroplasty, where blood loss has ranged from 500 to 700 mL.28,29 Conversion arthroplasty is also associated with significant increases in transfusion requirements. 28 Another consideration is prolonged operative times with conversion arthroplasty. The reported average operative time for a conversion arthroplasty is 95 (± 32.8) minutes, 29 while the median operative time in our series was 60 (± 23.7) minutes. A 30-minute increase in operative times has been shown to increase the odds of mortality by 17%. 30 Further, it is now well established that conversion arthroplasty is closer to revision hip arthroplasty than primary THA in terms of surgical complexity, resource utilization, and complication rates. 19
Despite these advantages, the risk of surgical site infection (SSI) remains high. However, SSI is also seen with revision surgery and with conversion arthroplasty. de Jong et al. 31 demonstrated a 15-fold increase in infection risk in conversion hip arthroplasty. Other authors have also demonstrated an increased risk of infection in previously operated patients.. 32 While we performed the serologic testing before surgery and cultured deep tissue from the operative specimen, four patients still developed SSI despite no indication of occult infection. We wish to highlight the high median Charlson comorbidity index (CCI) of seven in our case series, which is significantly higher than previously published research. 17
Our study has several limitations. It is a single institution, a single surgeon case series. A few patients have had short follow-ups until the time of writing this article, and these patients may experience dislocation(s) or failure of the cement shelf. We also do not know the effect of the generation of polymethylmethacrylate debris from the articulation between the cement shelf and bipolar head. We did not grade the defect in the posterosuperior acetabular wall. However, given the limited life expectancy and limited mobility of most patients in our cohort, we do not expect conversion arthroplasty in most of our patients. Additionally, we did not grade the defect in the posterosuperior acetabular wall, but a change in the therapeutic decision may be unlikely based on the size of the defect. Finally, in some patients, cement acetabuloplasty was performed without obvious radiological defects. This decision is to deepen the acetabular cavity and protect against posterosuperior dislocation without resorting to conversion arthroplasty.
Conclusions
Shelf acetabuloplasty is a safe and reasonable procedure to salvage recurrent dislocation of HA in low-demand patients without resorting to total hip arthroplasty. Shorter surgical duration, relatively lower blood loss, and immediate weight bearing render this an attractive option in this fragile population. We recommend a prospective multicenter study to evaluate the merits of this procedure in a larger cohort of patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.