
Abstract
Introduction
Ultrasound-guided popliteal sciatic nerve block has been described as a safe and consistent form of regional anesthesia for foot and ankle surgery. Little studies have been performed to prove the effectiveness of surgeon self-administered regional anesthesia for foot and ankle injury requiring an operation. This study aimed to assess the applicability and safety in surgeon-administered ultrasound-guided popliteal sciatic nerve block in providing anesthesia for foot and ankle fracture.
Material and Methods
Patients with foot and ankle injury who underwent operation under surgeon-administered ultrasound-guided popliteal sciatic nerve block were evaluated in this retrospective study. A total of 7 patients (3 females and 4 males) with a mean age of 46) were evaluated by the diagnosis, side of injury, comorbidities in American Society of Anesthesiologists Classification (ASA), duration of operation, blood loss, pain control in visual analog scale (VAS) intra-operatively, degree of motor blockage, post-operative pain control and hospital length of stay.
Result
Average age of the study population was 46. Of all the patients, two of them were of ASA I four of them were of ASA II and one of them was of ASA III. Complete sensory and motor blockages were achieved for all patients. Average operative time was 117 min. Average blood loss was 16.4 mL. Average post-operative inpatient stay was 3.57 days. There was no regional anesthesia-related complication arising from the procedure.
Conclusion
Surgeon-administered popliteal sciatic nerve block is a safe procedure and can provide excellent pain control throughout the operation according to our experience. Foot and ankle fracture fixation can be performed by orthopedic surgeons under this technique.
Keywords
Ultrasound-guided popliteal sciatic nerve block has been described as a safe mode of anesthesia with good consistency and efficacy for foot and ankle conditions. 1 It allows pain control and anesthesia over the territories under innervation of the common peroneal and tibial nerve. 2 Regional anesthesia is a domain and procedure routinely performed by anesthetists. However, because of the shortage of anesthetist manpower, our center started the practice of surgeon-administered ultrasound-guided regional anesthesia for various traumatic conditions. The popliteal sciatic nerve block was performed by trained orthopedic surgeons in our center under ultrasonic guidance and the very same attending surgeon would subsequently perform the operation himself after confirming successful nerve blockage.
To our knowledge, it is the first-ever article describing a series of patients with operations performed under a surgeon self-administered ultrasound-guided popliteal sciatic nerve block in Hong Kong. Limited studies have been performed to share the experience and to prove the efficacy of a surgeon-administered popliteal block. The aim of this study was to investigate the effectiveness of surgeon-administered regional anesthesia, particularly ultrasound-guided popliteal sciatic nerve block for foot and ankle fractures.
Patient and method
Study design and objective
This retrospective study was conducted with 6 patients who underwent an operation on their foot and ankle injury under surgeon-administered ultrasound-guided popliteal sciatic nerve block from August 2023 to February 2024.
Inclusion and exclusion criteria
The inclusion criteria were patients suffering from foot and ankle injury whose operation was indicated and whose area of involvement was covered by the sciatic nerve. Patients with their operation performed under surgeon-administered popliteal sciatic nerve block were included. Patients with injuries who required another supplementary nerve blockage, for example, adductor canal blockage or saphenous nerve block, were excluded from this study.
Other exclusion criteria for operation under regional anesthesia in our program were as follows: uncooperative pediatric patients, uncooperative psychiatric or demented patients, patients with uncontrolled bleeding tendency, patients with poor soft tissue condition at the site of anesthesia injection and surgeries performed under general anesthesia or regional anesthesia by anesthetists
Data collection
Patient's demographic factors and injury details such as age, sex, medical comorbidities (classified according to ASA classification), diagnosis, and side of injury were referred by the medical record. The type of operation, operative time, and blood loss were extracted from the operative records. Post-operative length of stay was referred by the discharge summary of the patient. Patient's pain control, and motor blockage intraoperatively and 6 h post-operatively were recorded.
Anesthesia technique
Trained specialist orthopedic surgeons would be responsible for the administration of the regional anesthesia. The same attending surgeon would also be responsible for carrying out the following operation. The popliteal sciatic nerve block was carried out with the patient in the lateral position, putting the knee slightly flexed. An ultrasound probe was placed at the popliteal fossa (Figures 1 to 3).
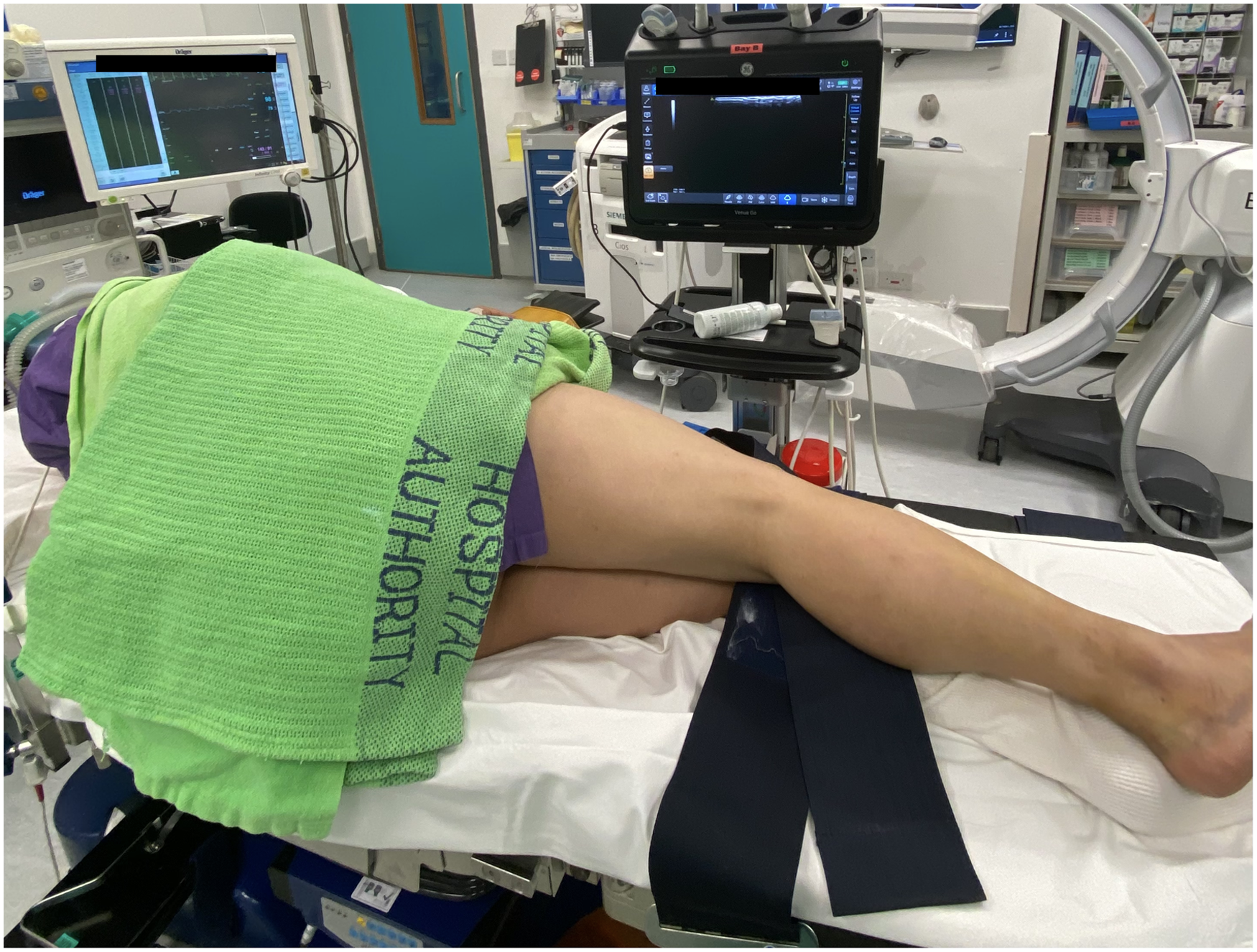
Positioning of a patient for popliteal sciatic nerve block.
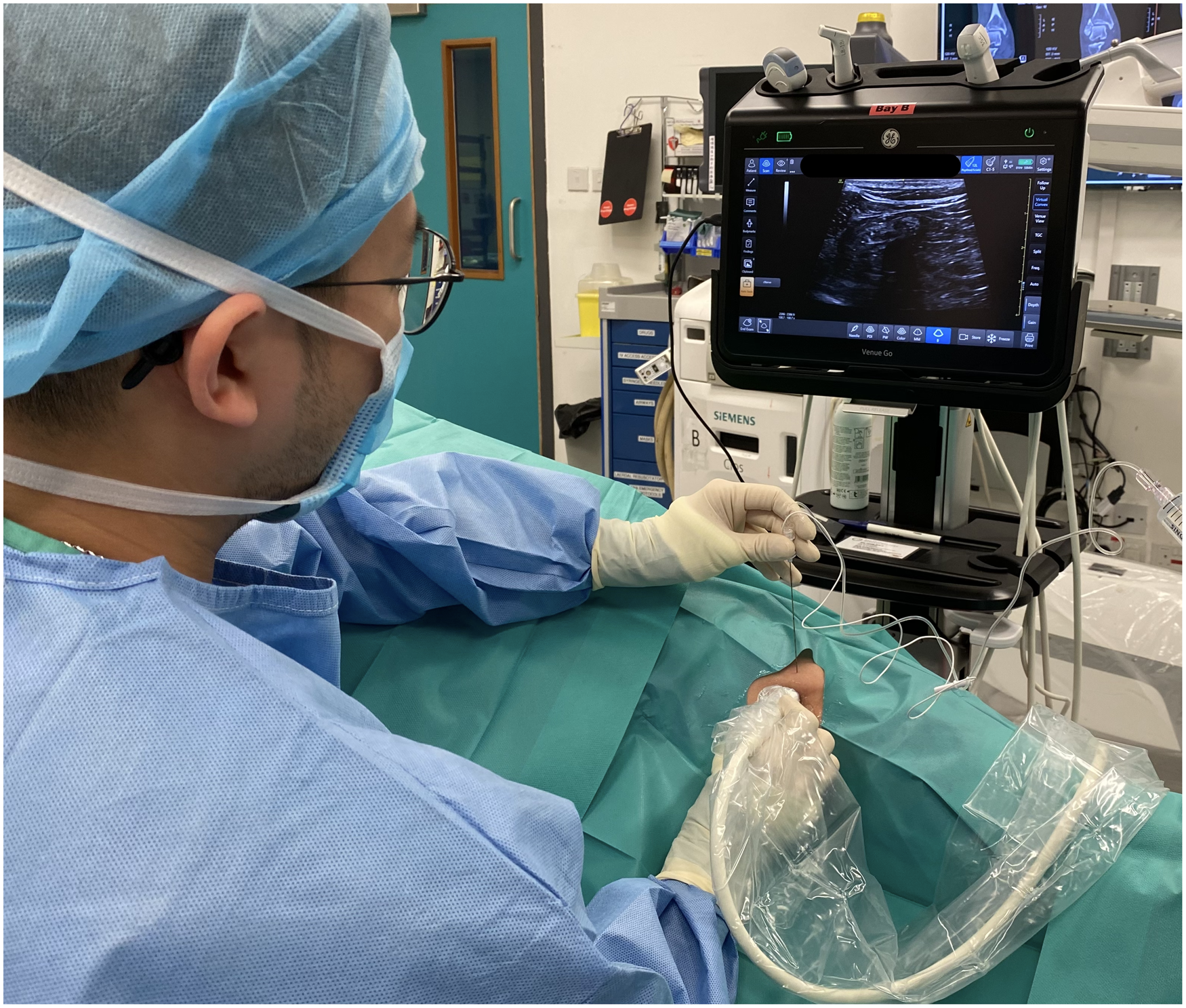
Application of popliteal sciatic nerve block under ultrasonic guidance.

Application of popliteal sciatic nerve block under ultrasonic guidance.
Ultrasound examination was performed with identification of underlying structures including common peroneal nerve, tibial nerve, popliteal vessel, and bicep femoris. Ultrasound probe would then be moved from caudal to cranial direction to identify the level where the sciatic nerve just diverged into common peroneal and tibial nerves. (Figures 4 and 5). Anesthetic agent, prepared with 10 mL 2% lignocaine with 1:200000 adrenaline and 10 mL 0.5% levobupivacaine, was prepared with reference to the patient's body weight. A 100-mm 21 gauge insulated stimulating needle was inserted in an in-plane manner from lateral to medial through the common paraneural sheath surrounding the common peroneal and tibial nerves. Successful infiltration was confirmed by the separation of common peroneal and tibial nerves by the anesthetic agent after injection (Figures 6 and 7).

Ultrasound image of common peroneal and tibial nerves, two nerves were separated with the probe at the caudal side of popliteal fossa.

Sciatic nerve just diverged into common peroneal and tibial nerves as probe moves from caudal to cranial direction.
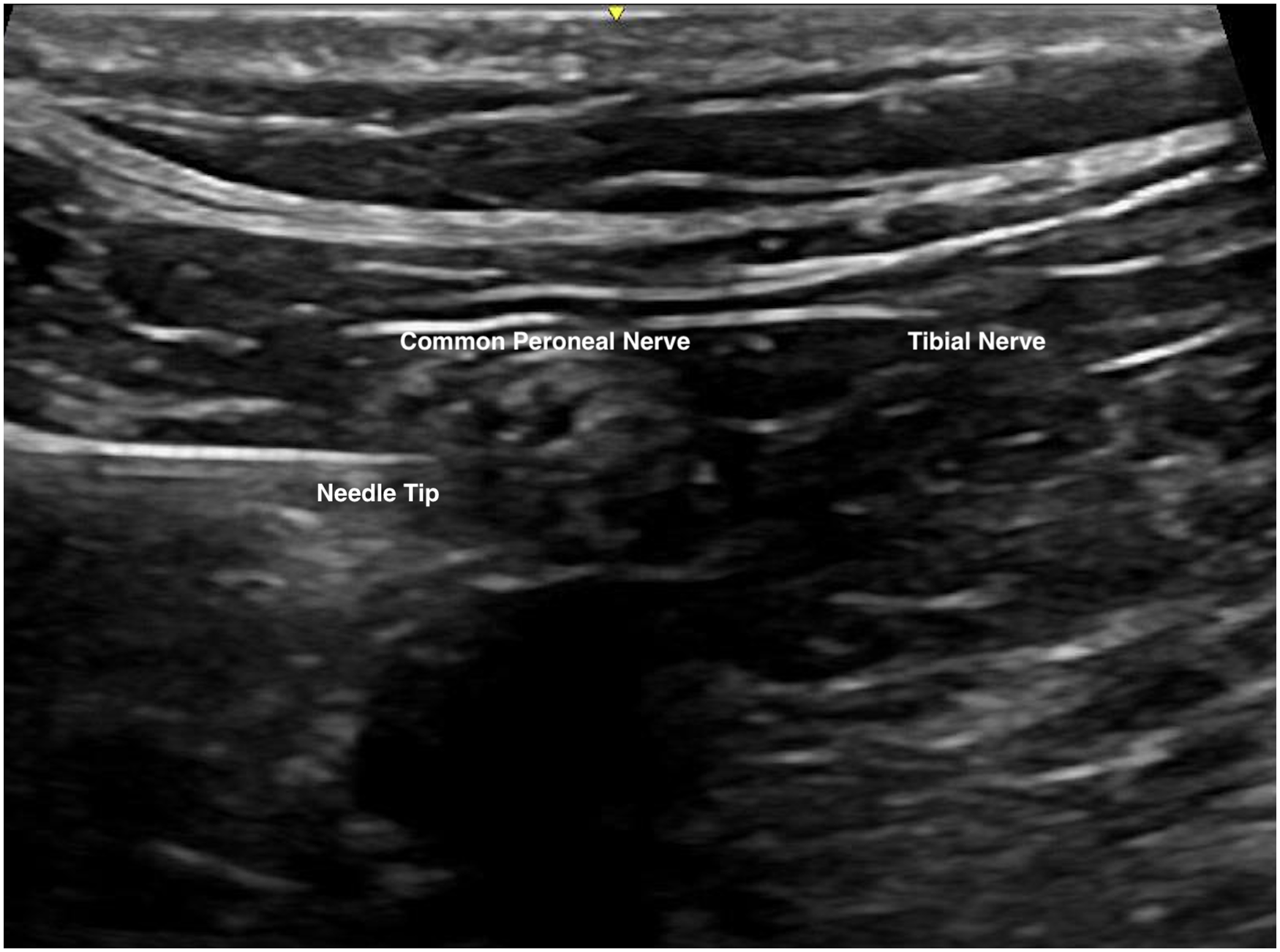
Needle advancement under ultrasonic guidance.
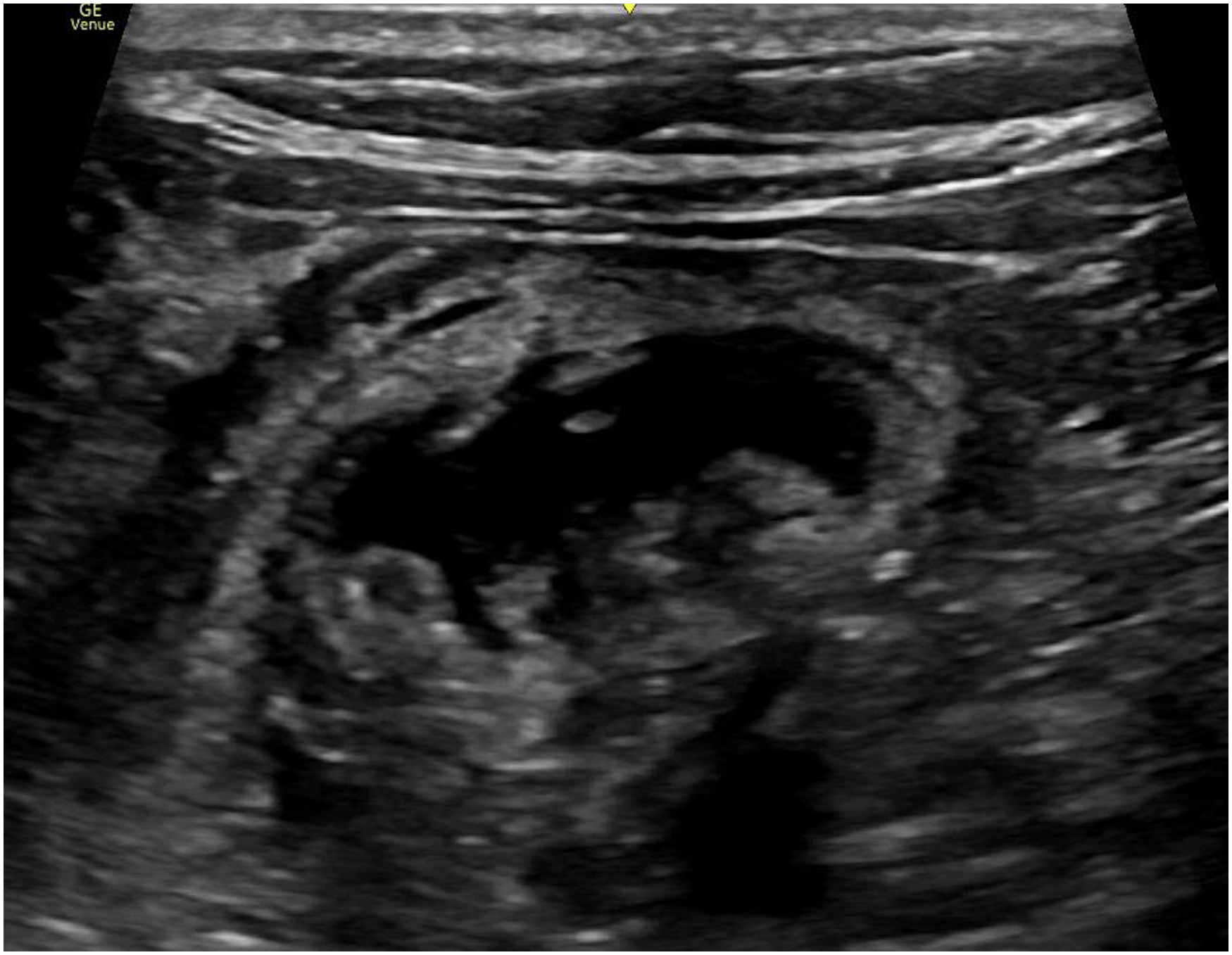
Separation of common peroneal and tibial nerve by anesthetic agent after injection.
Apart from the use of ultrasound guidance, we also made use of the tactile feedback of loss of resistance after passing through the paraneural sheath for locating the site of needle placement. Before injection of anesthetic agent, aspiration was performed to confirm needle placement without puncture of vascular structure. Excessive resistance was avoided during injection to avoid intraneural anesthetic agent injection.
Follow-up
All patients were continuously assessed throughout the operation with the level of pain control and motor blockage as well as vital signs being monitored. Pain control during operation and 6 h post-operatively were recorded on postop day 0. Oral Panadol and tramadol were used as standard pain control regimens upon patients’ request if the pain was deemed intolerable at 6 h post-operatively.
Result
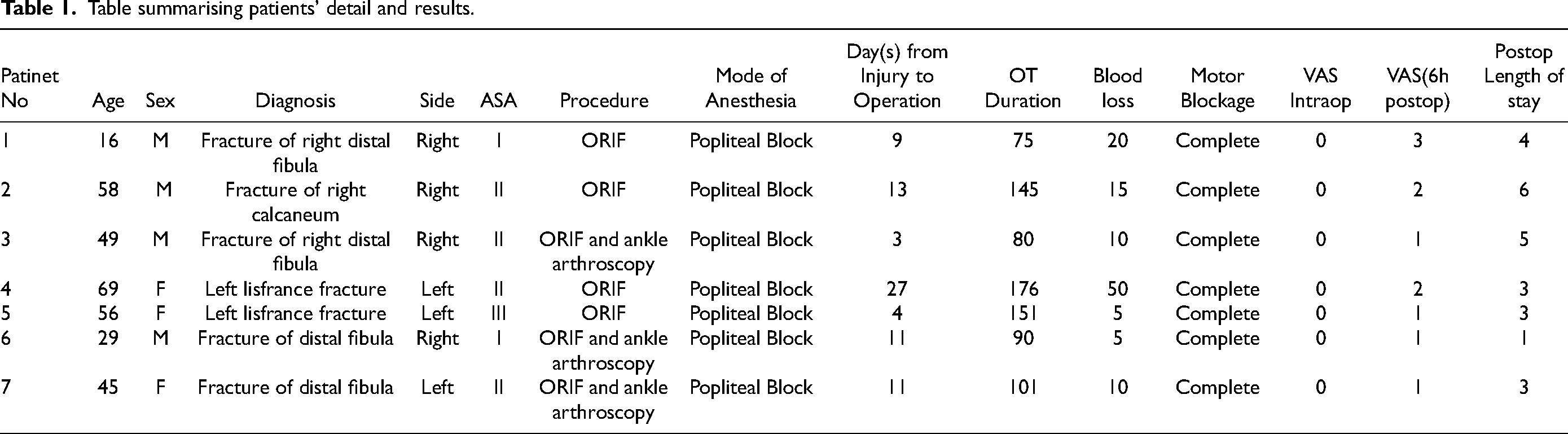
In total 7 patients with an average age of 46 were included in this study. The patient's comorbidities were classified according to the American Society of Anesthesiologists Classification (ASA). Four of them were of ASA II, two of them were of ASA I while one of them was of ASA III. Four patients suffered from distal fibula fracture, two patients suffered from Lisfranc fracture of foot and one patient suffered from calcaneal fracture. The average time from injury to operation was 12.6 days. The average operative time was 117 min. The average blood loss was 16.4 mL. We achieved complete motor blockage in all patients. Complete pain control during the operation was achieved with all patients who experienced painless operation, i.e., VAS =0. Tourniquet usage was avoided in all cases. Early post-operative pain control was satisfactory at 6 h after the operation, with all patients experiencing pain less than VAS 3 (VAS 1: 4 patients; VAS 2: 2 patients; VAS 3: 1 patient). The average post-operative in-patient length of stay was 3.57 days. There was no complication arising from the application of anesthesia. Results are summarized in Table 1 [Figures 8 to 10].
Table summarising patients’ detail and results.

Open reduction and internal fixation with plate for calcaneal fracture.

Open reduction and internal fixation with plate for lisfranc fracture dislocation.

Open reduction and internal fixation with plate for distal fibula fracture dislocation.
Discussion
The sciatic nerve is surrounded by paraneurium, a fascial structure. Popliteal sciatic nerve block makes use of the virtual space between paraneurim, 3 common peroneal and tibial nerves to allow a safe zone for needle placement and spreading of anesthetic agent surrounding the two nerves. 4 Local anesthetic injection right at the bifurcation of the sciatic nerve is associated with a high successful rate with a short onset time. 5 Identifying the exact point of needle placement is technically demanding, Tran et al. suggested confirmation of needle tip position inside the paraneurium through injection test. A small volume of local anesthetic was injected and the presence of a circular expansion of the sheath confirmed the correct site of needle placement. Though they also found out that injection of local anesthetic proximal to the bifurcation can also provide comparable efficacy, 6 we still suggest the use of the bifurcation as a reference since it provides a consistent landmark for nerve block administrators.
Some authors also suggested the confirmation of the bifurcation by eliciting the “seesaw sign.” 7 The “seesaw sign” involves the change in the relative position of common peroneal and tibial nerves with respect to ankle position. During ankle dorsiflexion, the tibial nerve moves to the posterior side while the common peroneal nerve moves to the posterior side during ankle plantarflexion. We did not apply this technique in view of the possible discomfort brought to patients during ankle movement at the injured limb.
There have been different techniques described in an attempt to shorten onset time and improve the efficacy of regional anesthesia, namely single and double injection techniques. 8 In the double injection technique, with the use of a nerve stimulator local anesthetic would be injected after confirming nerve stimulation of the two branches of the sciatic nerve. It was suggested that the onset time of the superficial peroneal block may be shorter and the success rate of the deep peroneal block may increase with the use of the double injection technique. The overall onset time and the overall success rate were similar between the two techniques. 9
Regional anesthesia with the use of ultrasound guidance has been proven to be a safe and effective means to provide nerve blockage for operation. 10 Benefits of the use of ultrasound include accurate localization of anatomical structures and infiltration of anesthetic agent. When compared to the traditional method of nerve stimulation guidance, there has been controversy about whether the success rate of sciatic nerve block can be improved by ultrasound guidance. 11 Ultrasound guidance is still currently deemed to be the gold standard for single-shot regional anesthesia. 12 In a meta-analysis by Cao et al., it was found that the success rate of block and the risk of vascular puncture can be improved with the use of ultrasound guidance. 13
Conclusion
According to our experience, orthopedic surgeon-administered regional anesthesia could allow satisfactory pain control for the fixation of foot and ankle fractures.
We may be able to apply the sample principle to orthopedic conditions both elective or traumatic in nature. However, further studies need to be continued for adequate power for formal analysis of feasibility.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.