
Abstract
Introduction
Lateral shelf acetabuloplasty is a well-recognised treatment modality for patients with Perthes’ disease, especially those over the age of 8 years at presentation. 1 Containment of the femoral head underneath the created shelf during the healing phase of Perthes’ disease has been reported to prevent further head deformity, likely by preventing lateral subluxation of the femoral head. 2 By creating a bony ‘shelf’, one can provide mechanical stability and spread the hip joint load over a wider area, which may help prevent the femoral head from collapse and discourage early degenerative changes. However, the outcome can be compromised by resorption of the shelf over time, especially in older children who have decreased potential for lateral acetabular growth. 3 Staheli believed that incorporation of autogenous bone graft was an essential step in creating a strong and well-developed acetabular shelf. 4 Similarly, Grzegorzewski et al. observed incidence of lateral graft resorption in their series of patients with Perthes’ disease treated with shelf acetabuloplasty without the use of calcium sulphate. 5
Various natural and artificial products including growth factors, bone morphogenetic proteins (BMPs), bone marrow, platelet-rich plasma (PRP), calcium phosphate and calcium sulphate have been used to enhance graft incorporation in different surgical indications.6,7 Osteoset® (Wright Medical Technology, Arlington, USA) is a surgical hemihydrate crystal of calcium sulphate product in pellet form designed to promote bone healing and subsequent bone remodelling.8,9 Calcium sulphate has many properties to allow it to be an ideal synthetic bone graft material: it is biodegradable, biocompatible and osteoconductive, facilitating ingrowth of both blood vessels and osteogenic cells. However, its relatively low mechanical strength and brittleness are still considered major obstacles in its use as a structural bone implant.10,11 Subsequent experimental and clinical trials have been conducted to explore and evaluate other clinical utilitites.12–15 Calcium sulphate proved its utility as a carrier in delivering antibiotics in the presence of bone infection and in filling bone defects in the treatment of benign bone lesions.16,17 However, ambiguous results were reported by other studies that evaluated its effect on bone graft incorporation.12,13
In the available literature we could find only a few reports that commented on usage of calcium sulphate in children. We did not find any study that assessed effectiveness of calcium sulphate to enhance bone graft incorporation into the pelvis. The aim of this study was to evaluate the effect of calcium sulphate (Osteoset pellets) on the rate and volume of bone graft incorporation after shelf acetabuloplasty for acetabular dysplasia secondary to Perthes’ disease, and on femoral head sphericity at skeletal maturity. We also examined whether Osteoset prevented early resorption of the shelf.
Methods
We retrospectively reviewed 32 children with Perthes’ disease managed by shelf acetabuloplasty. The study group comprised 15 children who had been managed by shelf acetabuloplasty using autogenous bone grafts from iliac bone and Osteoset. The control group consisted of 17 children managed by shelf acetabuloplasty using autogenous bone graft without Osteoset. Patients were included in the study if they had acetabular dysplasia or potential acetabular dysplasia secondary to lateral subluxation, and/or coxa magna which had been managed by shelf acetabuloplasty using autogenous bone graft, with or without Osteoset. Patients who had had previous surgical acetabular procedures or who had concomitant systemic or metabolic bone disease which might influence graft incorporation or healing were excluded. The decision to use Osteoset pellets was based on surgeon preference. Patients were included if they fulfilled the above inclusion criteria and had full radiological and clinical assessment until skeletal maturity. Skeletal maturity was evaluated on pelvis radiographs based on closure of triradiate cartilage and closure of the iliac apophysis (Risser sign 5). Patient selection process is presented in Figure 1.
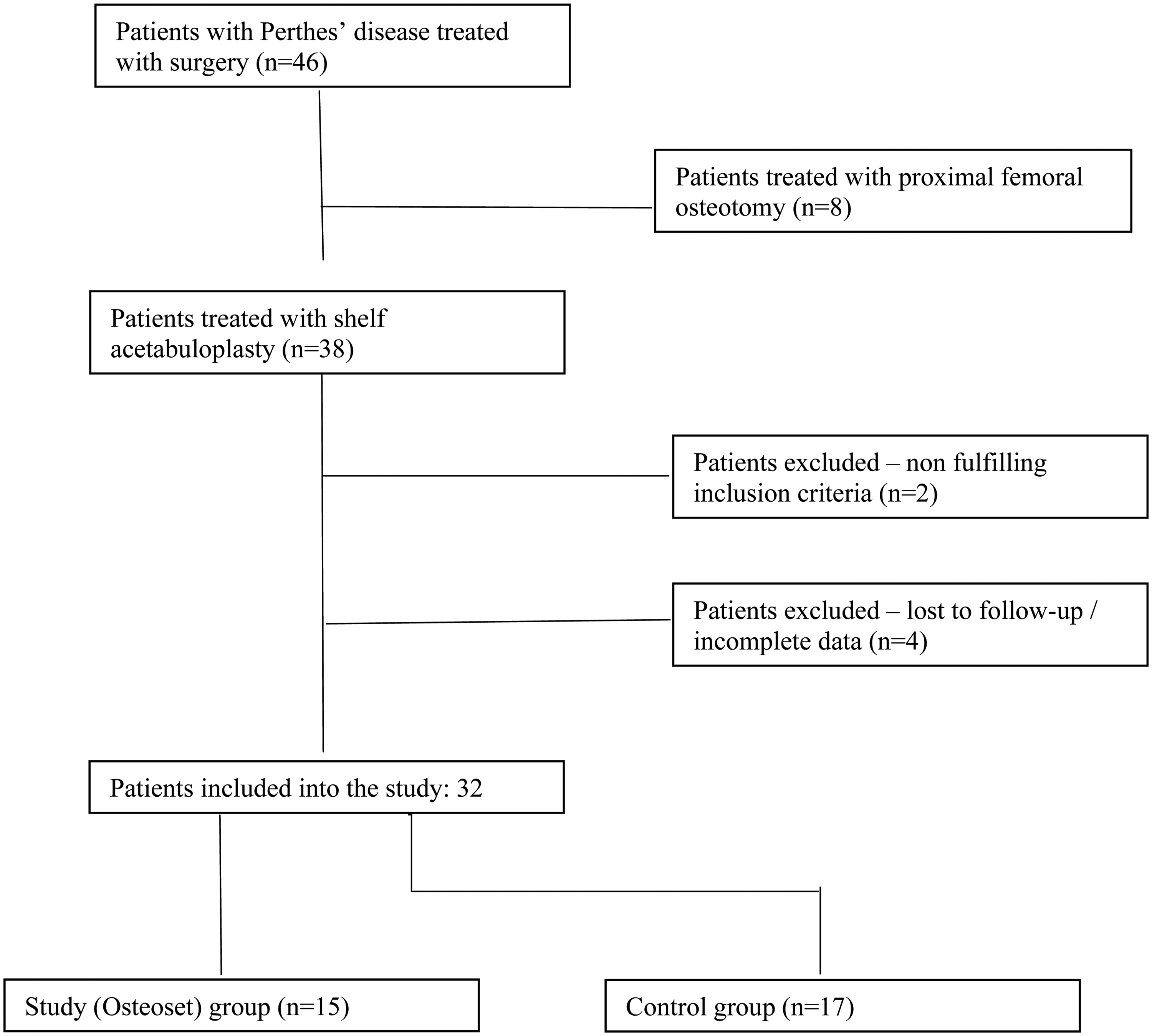
Flow chart of patient selection process.
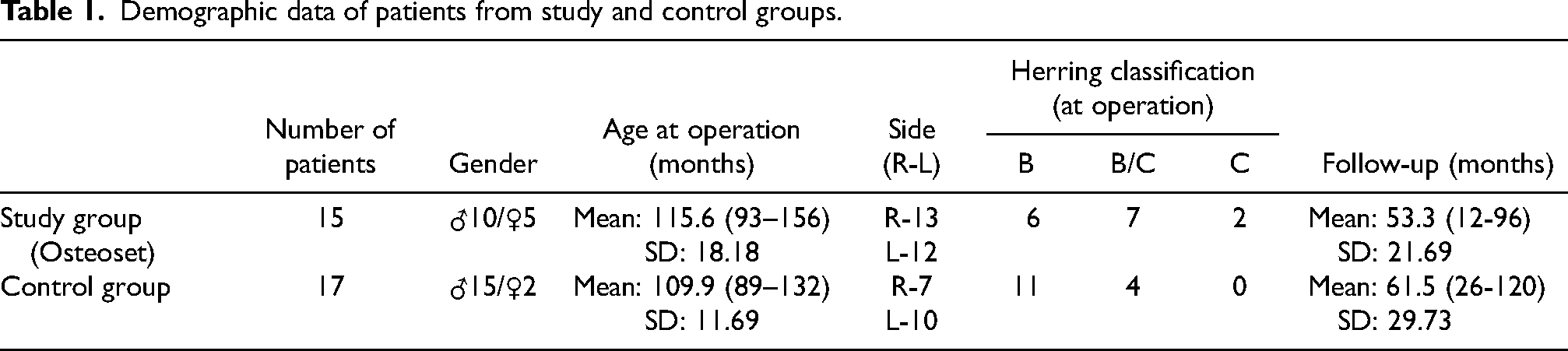
There were 25 boys and 7 girls. The mean age of diagnosis was 9 years and 1 month (from 7 years and 2 months to 12 years and 3 months). The mean age at operation was 9 years and 4 months (from 7 years 5 months to 12 years and 4 months). Patients in both groups were age-matched (p = 0.441) and had the same indications for surgery. Similarly, containment of the hip joint as assessed by percentage of acetabular cover also did not show any significant difference between the two groups (p = 0.061). Thirteen of 15 hips from the study group (88%) and all hips from the control group were graded as B or B/C according to Herring classification. 18 All patients were operated on at the early phase of the disease (necrosis or early fragmentation stages according to Waldenström classification). 19 All children were operated on less than 6 months from the onset of the disease and less than 6 weeks (mean 3.5 weeks; from 1 to 5 weeks) from the time of the diagnosis. The operations were performed at our institution between February 2003 and July 2008. Demographic, clinical and peri-operative details were retrieved from departmental databases, case notes and medical files. Patients’ demographic and clinical data is summarised in Table 1. The study was conducted in adherence to the Declaration of Helsinki and was approved by approved by the local NHS Research Ethic Board (REB) prior to recruiting patients for the study ((Registration Number 34/2011/REB).
Demographic data of patients from study and control groups.
Surgical technique
Acetabular augmentation was performed as described by Staheli. 4 The hip was exposed through a modified Smith–Petersen approach. Gluteus medius and the tensor fascia lata were elevated subperiosteally from the outer table of the ilium. The reflected head of rectus femoris was sectioned, elevated from its capsular attachment and retracted posteriorly. A slot was made by drilling holes at the margin of the acetabulum from the anterior edge of the ilium as far back as accessible. The slot was deepened with a curved osteotome to reach the inner cortex. Shallow cortico-cancellous bone strips were harvested from the lateral wall of the ilium and hammered into the slot, with the cortical surface towards the hip. The width of augmentation or extra-osseous length of the shelf was measured on preoperative anteroposterior (AP) radiographs of the hip as the length required to achieve a centre-edge angle (CEA) of approximately 35°. Cancellous bone, harvested from the exposed iliac wing, was then packed above the cancellous surface of the shelf strips. Where used, 10 ml Osteoset pellets were laid over the bone graft. The hip abductors were reattached to the iliac crest to secure the bone graft +/− Osteoset. A hip spica cast was used to immobilise 11 patients (three patients from the study group and eight patients from the control group) for 6 weeks post-operatively. Following removal of the spica cast, patients mobilised partial weight-bearing for a further 6 weeks. The remaining patients were mobilised partial weight-bearing immediately post-surgery for 6 weeks.
Radiographic measurements
Preoperative, immediate post-operative and serial follow-up AP radiographs of the pelvis were evaluated using Kodak Carestream PACS version 5.3.sp1.1. software. Standard magnification of the radiographs was 115%. We reviewed films taken immediately post-operatively, at 6 weeks, 3 months, 6 months, 12 months and then on a yearly basis. Patients were followed up until skeletal maturity. The following radiological parameters were assessed by 2 independent assessors who were blinded with regard to Osteoset usage (Osteoset was not visible except in the immediate post-operative film which could therefore not be blinded):
Shelf and bone graft area – this was assessed with the free hand tool in the PACS system by outlining the graft profile that was used as a proxy for bone graft volume. The Osteoset was not included in the graft profile in the study group (Figure 2). Length of the extra-osseous shelf in mm as measured by the PACS line measurement tool. Acetabular cover – defined as the percentage ratio of the width of the new acetabulum (anatomical acetabulum plus extra-osseous shelf length) divided by the diameter of the femoral head as described by Heyman and Herndon.
20
Measurement of the centre-edge angle (CEA). Graft incorporation as assessed by Avci et al. criteria.
21
The density of the graft was categorised as normal, sclerotic or porotic. Femoral head sphericity, according to Stulberg classification at the final x-ray, at skeletal maturity.
22
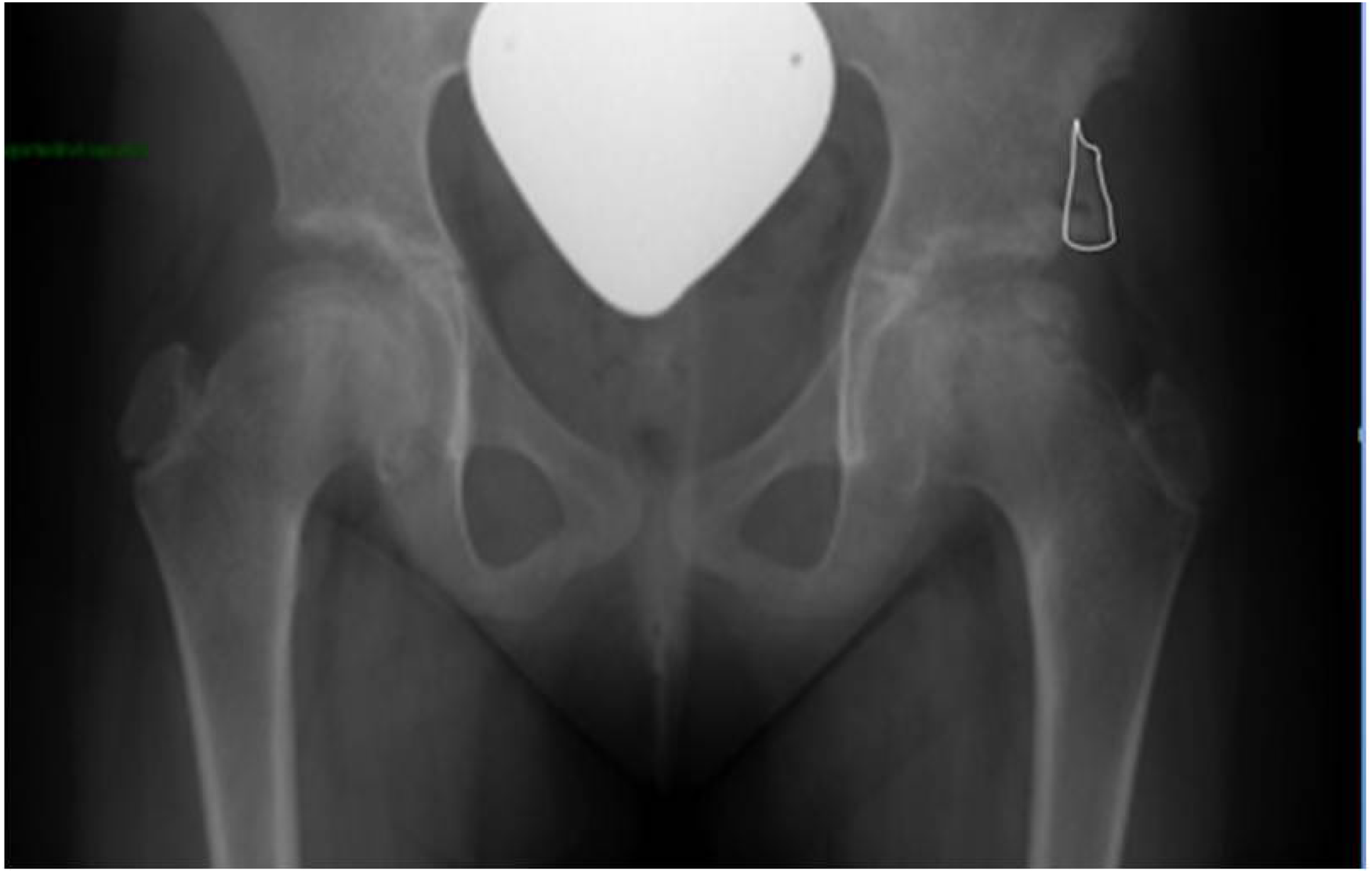
Ap pelvis x-ray after shelf acetabuloplasty of the left hip with shelf area marked in white.
Statistical analysis
Data were analysed using IBM SPSS Statistics software, version 27, 2019. Histogram analysis showed that all the data were normally distributed. The unpaired two-tailed t test was used to compare the radiological measurements between the groups and a p-value of < 0.05 was considered to be significant. Pearson's correlation coefficient was used to define pairwise agreement between two observers (inter-observer reliability) regarding measurements of respective radiological parameters.
Results
The mean follow-up period in the study group was 53.3 months (range: 12–96; SD: 21.6), and 61.5 months (range: 26–120, SD: 29.73) in the control group, at which point all patients had reached skeletal maturity as assessed on pelvic radiographs. We did not observe any intraoperative or early post-operative complications. The only ‘complication’ observed during the follow-up period on radiographs was heterotopic calcification at the lateral edge of the shelf in 3 patients (2 boys, 1 girl) from the study group. Heterotopic calcification did not have any clinical implications (pain, limited range of hip abduction). One patient had delayed graft incorporation till 3 months post-operatively while the other 2 were fully incorporated by 6 weeks. By the end of follow-up, the heterotopic calcification has resorbed in all cases. The results of the examined radiological parameters are as follows:
Shelf and bone graft area (Figure 3)
Immediately post-operatively shelf area was similar in both groups: (358.1 cm2 and 353.2 cm2 in the study and control group, respectively). From 6 weeks post-operatively and thereafter, shelf area was significantly greater (p = 0.034) throughout the follow-up period in patients who had Osteoset pellets. Patients from the control group showed steady decline in graft area throughout the follow-up period. The inter-observer reliability for shelf area was 0.851 (Figure 3).
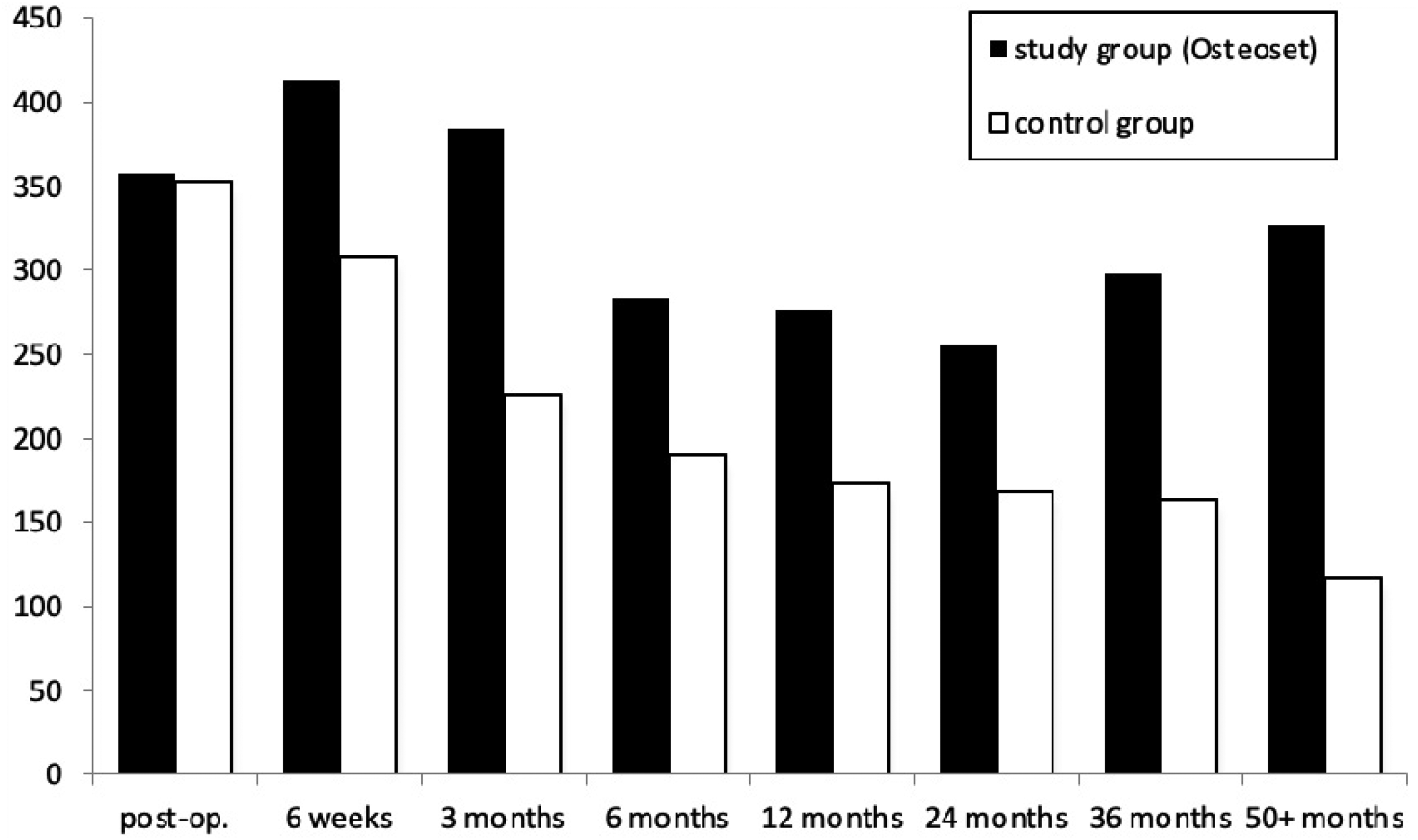
Total shelf and bone graft area [mm2].
Extra-osseous shelf length (Figure 4)
Immediately post-operatively the extra-osseous shelf length was similar in study and control groups (17.6 mm and 18.5 mm, respectively). From 6 weeks post-operatively and thereafter extra-osseous shelf length was significantly greater in the study group than in the control group (p = 0.046). Extra-osseous shelf length till 1 year post-operatively again was significantly greater in the study group than in the control group (p = 0.03). Thereafter, there was no statistical difference in extra-osseous shelf length between the two groups till the end of the follow-up period. For shelf length Pearson's correlation coefficient for inter-observer reliability was 0.938.
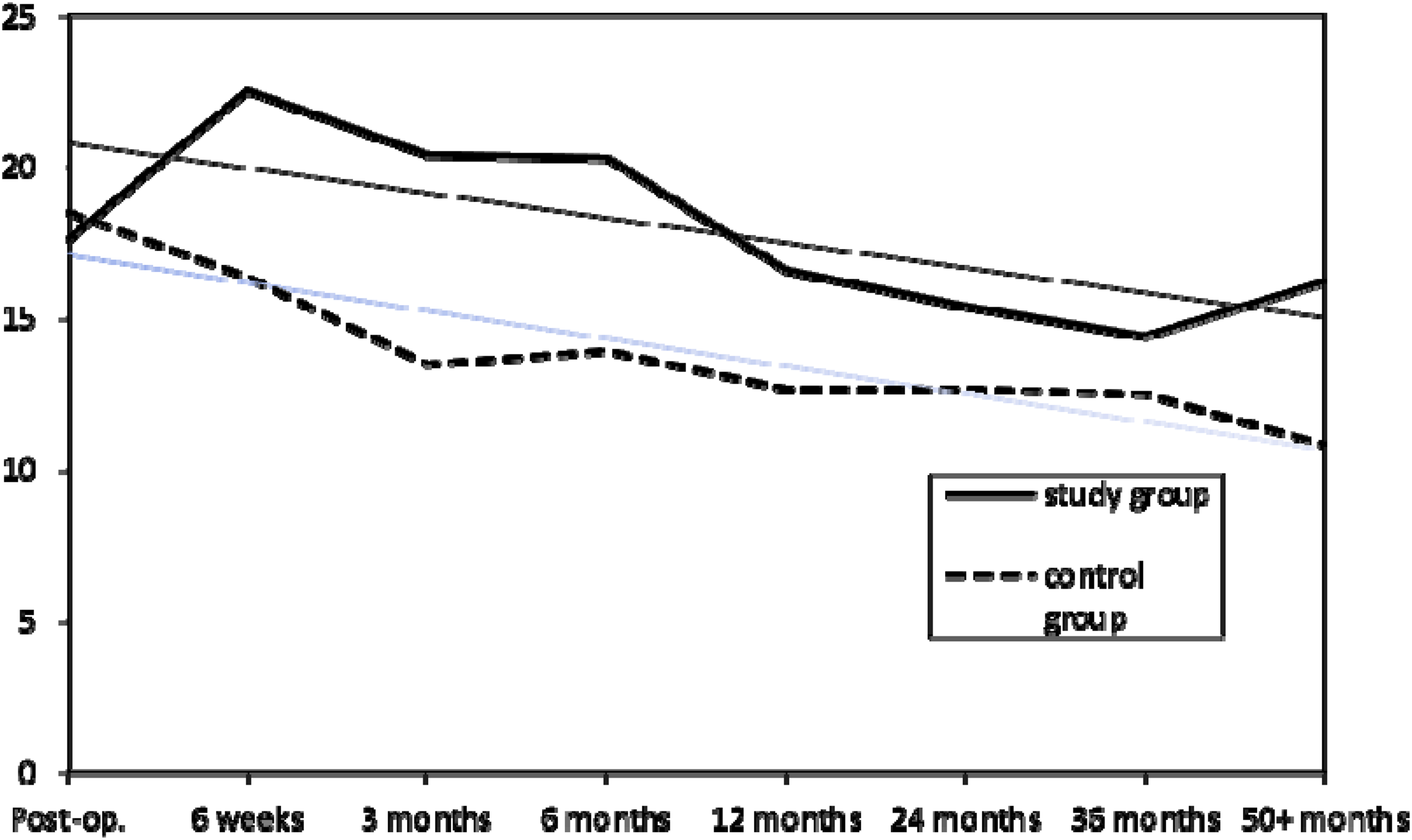
The length of the external portion of the shelf [mm].
Percentage acetabular cover (Figure 5)
Acetabular cover decreased throughout follow-up for both groups. However, decrease in acetabular cover in the control group was more pronounced in the control group (from 87% to 75%) than in the study group (75% to 70%). The difference was not statistically significant (p = 0.095 at the end of the follow-up). Inter-observer reliability was 0.883.
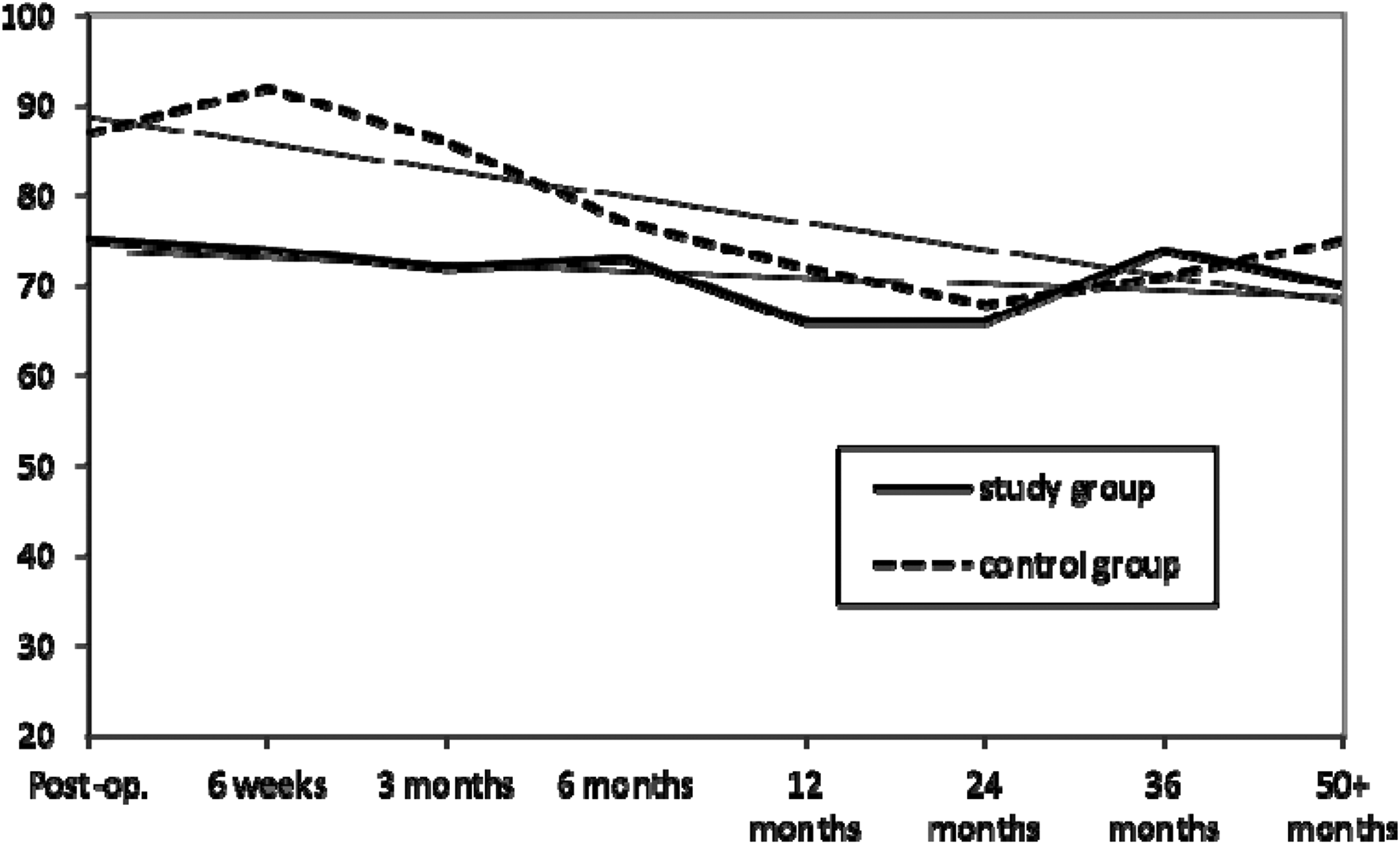
The average acetabular coverage (%).
Centre-edge angle (Figure 6)
Similar observations were observed with regards to CEA. Again, CEA decreased slightly throughout follow-up in both groups, but again significantly less in the Osteoset group.
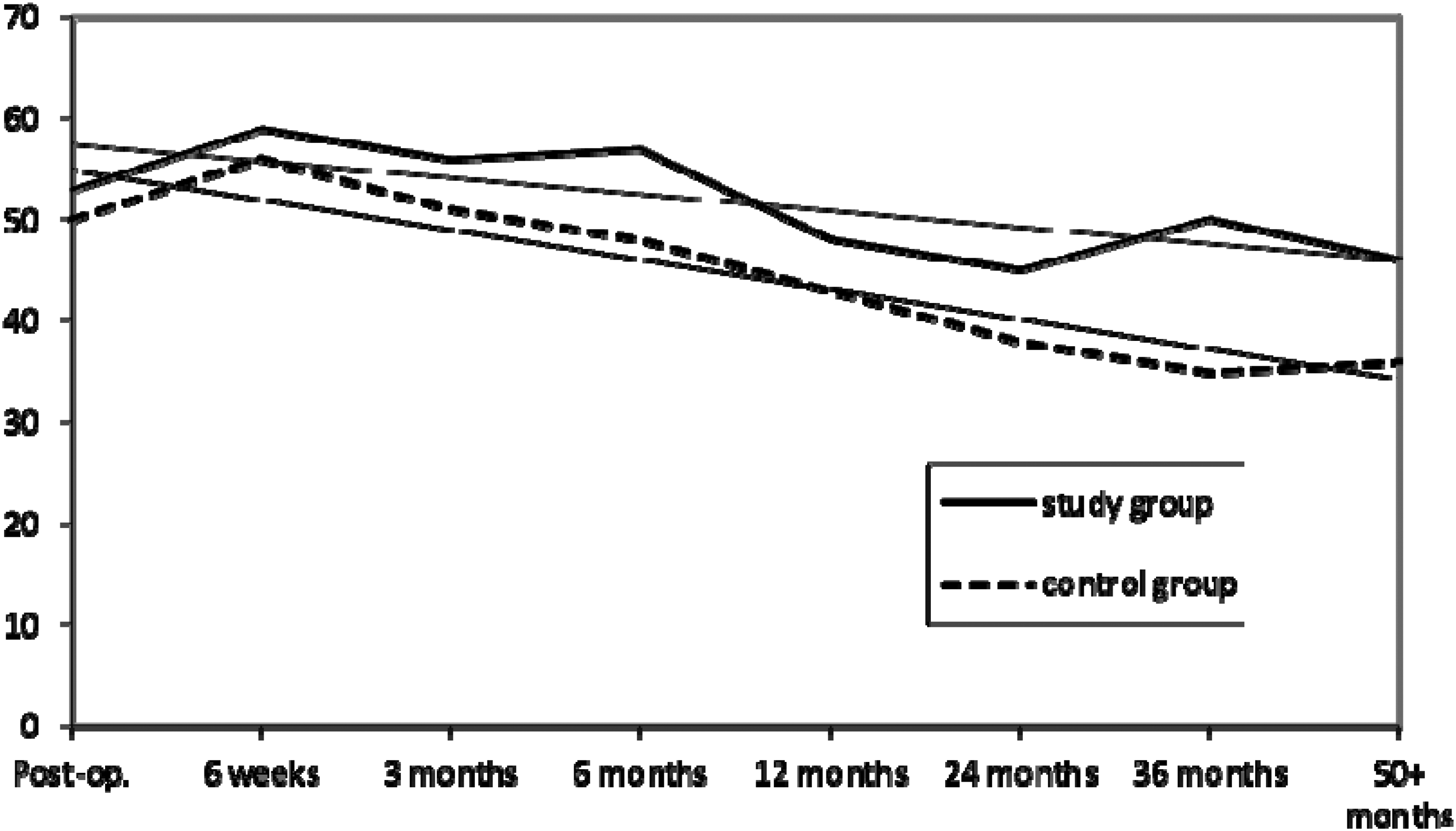
Centre-edge angle (°) in the study and control groups.
Graft incorporation
Using the Avci criteria for evaluation of graft incorporation, we found 6 patients (43%) in the study group whose graft had not incorporated 6 weeks post-operatively, comprising 3 partially porotic and 3 sclerotic grafts. By 3 months only 1 patient remained partially porotic. All grafts were fully incorporated by 6 months. In the control group, where Osteoset was not used, 10 patients (58%) showed incomplete bone graft incorporation at 6 weeks. In 9 cases bone grafts were classified as porotic and in 1 case as sclerotic, and the remaining cases bone grafts were assessed as normal. By 3 months in 2 cases bone grafts remained still osteoporotic, but by 1 year all grafts were fully incorporated.
Eleven patients who had been immobilised in plaster post-operatively demonstrated no significant difference in shelf area, shelf length and femoral head sphericity at the end of the follow-up period from the remaining patients who were not immobilised.
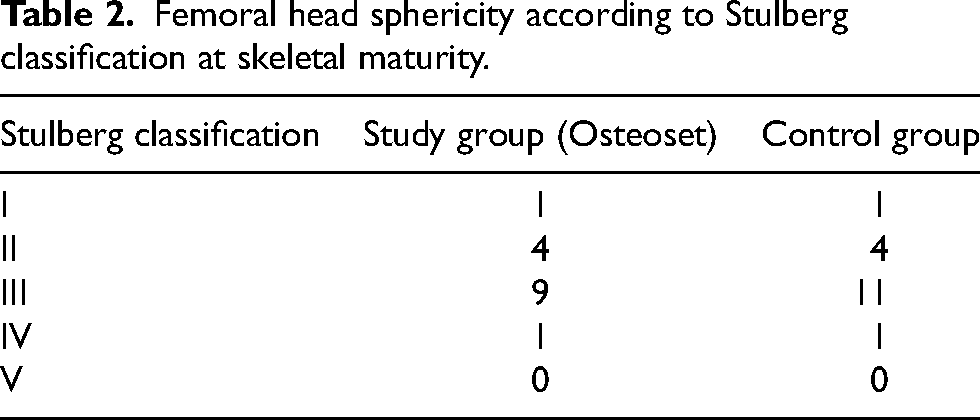
Final femoral head sphericity
There was only 1 hip in each group classified as Stulberg type IV and no hips type V (Table 2). We found no significant difference between groups in femoral head sphericity at skeletal maturity. We did not observe relationship between initial Herring classification and the final femoral head sphericity assessed by Stulberg classification. The number of children in each subgroup of Herring classification was small and there was no correlation between initial Herring classification and final femoral head sphericity. However, patients from the study group had higher number of hips classified as Herring grade B/C and C (7 and 2 for B/C and C, respectively). In comparison, in the control group, there were only 4 B/C hips and no C hips.
Femoral head sphericity according to Stulberg classification at skeletal maturity.
Discussion
The aim of shelf acetabuloplasty is to provide a satisfactory cover of the femoral head, which is essential for normal loading and development of the hip. In Perthes’ disease in older children, acetabular augmentation seems to prevent further femoral head deformity as the femoral head progresses through fragmentation, and furthermore corrects the lack of remodelling which results in acetabular dysplasia as the femoral head enlarges during the healing phase. 1 Our final results measured by femoral head sphericity (Stulberg classification) are not fully satisfactory. However, the mean age of the patients from our study at the time of the diagnosis and surgery was above average for children with Perthes’ disease and the majority of them have had a significant femoral head involvement (measured according to Herring classification). These are both known as risk factors for a poor outcome regardless treatment modality and may explain unsatisfactory results in our study.
However, there are concerns that the shelf may resorb, especially if placed too high, which compromises the outcome. Indeed, in this study, we observed steady decreases of shelf area and shelf length. This phenomenon was observed both during the early post-operative period, when resorption was the fastest, and during the entire follow-up period. However, this decrease was statistically slower in patients from a study group, where Osteoset was used. Decreased graft resorption resulted in a better femoral head coverage, as measured by percentage of acetabular cover. Similarly, Grzegorzewski et al. observed incidence of lateral graft resorption in their series of patients with Perthes’ disease treated with shelf acetabuloplasty without the use of Osteoset. 5 In this study, improvement in bone graft incorporation and preservation in femoral head coverage as measured by extra-osseus shelf length and percentage acetabular cover did not translate into better femoral head sphericity measured at skeletal maturity. Perhaps other factors not fully understood yet are also responsible in a healing process and final femoral head remodelling in Perthes’ disease.
Another argument for the osteoconductive property of Osteoset was faster bone graft incorporation observed in patients from the study group. There was a 17% difference in percentage of cases where bone grafts were fully incorporated with ilium at 6 weeks after operation. Chang et al. used Osteoset with bone grafts in spinal surgery. 23 He noticed that adding Osteoset to local autologous bone grafts improved fusion rate in posterolateral spinal fusion. Kim et al. 24 demonstrated the osteoconductive properties of calcium sulphate in distraction osteosynthesis. It improved early consolidation of bone regenerate in distraction osteogenesis for craniofacial microsomia in adults.
In a prospective study, Kumar et al. 25 used calcium sulphate to fill bone lesions in 15 patients with a variety of orthopaedic conditions such as benign bone lesions and osteomyelitis. Thirteen cases out of 15 showed calcium sulphate resorption and new bone incorporation. Calcium sulphate resorption occurred at an average of 14.5 weeks. New bone incorporation occurred at an average of 6 months. A similar study was carried out by Andreacchio et al. 26 The authors used calcium sulphate grafts to treat non-ossifying fibromas in 9 children and adolescents. At the last follow-up at 2 years calcium sulphate grafts were fully incorporated. Injectable calcium sulphate was found to be as effective as a mix of autogenous and allogenous bone grafts in filling the defects and incorporation to the humerus in unicameral bone cysts (UBCs) treatment in the study of Li et al. 27 Osteoset was also used to treat pathological fractures in the presence of UBCs in the proximal femur in 7 patients in the study of Vigler et al. 13 At average follow-up of nearly 5 years, all fractures had healed uneventfully. The cyst was fully obliterated in 5 patients and partially obliterated in 2 patients.
On the contrary, Petruskevicius et al. 12 did not find Osteoset to have a stimulating role in bone healing. In a prospective randomised study, the tibial defect created during anterior cruciate ligament (ACL) reconstruction procedure was filled with Osteoset pellets or left empty. Authors did not observe enhanced filling of the defect in the Osteoset group at 3 and 6 months post-operatively.
Calcium sulphate was found to be a safe, efficient bone graft substitute in the treatment of osseous defects. In our series we did not observe inflammatory allergic reactions reported by other researchers, and there were no cases of post-operative infection. Interestingly, Lee et al. observed a relatively high (13.8–19.0%) incidence of sterile inflammatory adverse reaction to Osteoset used to fill benign bone lesions. 28 This reaction was essentially self-limiting and fairly benign, requiring only anti-inflammatories and observation. Presumably the young age of patients might be responsible for better tolerance of Osteoset in our series.
This study has several limitations. Although patients from both groups were age- and sex-matched, had the same indications for surgery, and surgical technique were identical and had similar femoral head involvement assessed retrospectively according to Herring classification, they were not randomised into both treatment modalities.
The number of patients in both groups was relatively small, but similar to the number of patients from the other comparable studies. Another technical limitation of the study is that no marker for absolute size was used to calibrate radiographs and film magnification was not known. Therefore, there may be some uncertainty regarding the variability of measurements between films for the same patient and between patients. All radiographs were taken in the same radiology department using the same protocol and technical specification and magnification. We therefore conclude that the lack of additional precise calibration does not have a significant effect on the accuracy of our measurements.
In summary, this study proved that calcium sulphate can be safely used in the paediatric population when there is desire to enhance bone graft incorporation and reduce graft resorption. Our findings can support its use when there is not enough autogenous bone stock available in various surgical procedures or when increased bone graft resorption is a concern. In case of shelf acetabuloplasty for Perthes’ disease it may have a role in cases where, intraoperatively, the initial extra-osseous length or volume of the shelf is not sufficient. When surgery is performed correctly, augmentation with Osteoset did not result in improvement of femoral head sphericity. Further randomised studies are needed to confirm its usefulness in other orthopaedic procedures, both in adults and in children.
Footnotes
Acknowledgements
This paper and the research behind it would not have been possible without the exceptional support from Mr David Sherlock, Consultant Orthopaedic Surgeon. His hard work and wealthy knowledge have been an inspiration and always kept this work on track.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.