
Abstract
Introduction
Hinge fracture and cervical kyphosis are known complications of cervical laminoplasty. Prior literatures on hinge fracture focused mainly on laminoplasty performed using the open-door technique. In this study we aim to assess the effect of intraoperative hinge fracture on postoperative cervical spine alignment in cervical laminoplasty performed using the double door technique.
Methods
This study recruited patients who received double door cervical laminoplasty from January 2014 to December 2022. The diagnosis, demographic data, preoperation and postoperation cervical spine alignment of the patients with intraoperative hinge fracture were compared with patients withouintraoperative hinge fracture. Cervical spine alignment was measured using C2–7 Cobb's angle on neutral lateral cervical spine X ray.
Results
Nine patients with intraoperative hinge fracture and 51 patients without intraoperative hinge fracture were recruited into the study. There was no statistically significant difference in age, sex, diagnosis and preoperative cervical spine alignment between the patients with and without intraoperative hinge fracture. Significant difference was found in the postoperation cervical spine alignment (1.9 ± 15.5° vs 9.7 ± 13.6°, p = .044) and change in cervical spine alignment (−12.9 ± 12.1° vs −4.0 ± 10.0, p = .02) between patients with and without intraoperative hinge fracture.
Conclusions
In double door cervical laminoplasty, intraoperative hinge fracture is associated with development of postoperative cervical kyphosis.
Introduction
Cervical laminoplasty is an established surgical technique for the treatment of multilevel cervical spinal stenosis. Current techniques can be categorized into “open door laminoplasty” and “double door laminoplasty.” 1 Hinge fracture and cervical kyphosis are known complications associated with cervical laminoplasty. 2 Most of the literatures concerning the effect hinge fracture on the outcomes of laminoplasty are related to “open door laminoplasty.”3–8 There are some studies which assessed the relationship of preoperative cervical spine alignment and incidence of postoperative cervical kyphosis in double door laminoplasty.9,10 There is no literature about the effect of hinge fracture on postoperative cervical spine alignment in double door laminoplasty and our study aims to give an answer to this question.
Materials and methods
Study design and patient cohort
This was a retrospective cohort study conducted in a single institution. The study was approved by our institution's review board. Patients who received cervical laminoplasty from January 2014 to December 2022 were identified through electronic patient records. Only patients who had received laminoplasty from C3–C7 segments were included in the study. Exclusion criteria included the following items: (1) prior anterior spinal fusion or congenital block vertebra, (2) obvious ossification of posterior longitudinal ligament (OPLL) on lateral cervical spine X-ray, (3) C2–7 vertebral not fully visualized on lateral cervical spine X-ray, (4) No X-ray taken either before or after operation, (5) anatomical anomaly precluding placement of hydroxyapatite spacer block in the split spinous process, (6) post op wound infection required removal of hydroxyapatite spacer block. The cohort included 60 patients (46 male, 14 female) with a mean age of 65.2 ± 10.1 years (range: 42–85 years) at the time of operation. The diagnosis of the patients was either cervical myelopathy or central cord syndrome.
Surgical techniques
All patients received double door laminoplasty using Kurokawa's technique 11 from C3 to C7. Patient's head was stabilized with 3 kg's traction via a skull tong on a spinal table. A midline incision was made spanning from C3 to C7, and paraspinal muscles were dissected subperiosteally till the facets were exposed, with preservation of the facet joints capsule. Longitudinal grooves were made bilaterally at the lamina–facet junction by resecting the outer cortex and a part of cancellous bone using a 3.5 mm diamond burr. The interspinous ligaments and the tip of the spinous process of C3 to C7 were removed and the spinous process were split in the midline using a 2.5 mm high speed diamond burr under operating microscope magnification. Subsequently, the split laminas were opened in the midline and the constricting fibrous band above the dura mater and the hypertrophied yellow ligament were resected from C3 to C7 levels. Two millimeter sized holes were made at the split spinous process using a high-speed drill, and trapezoidal shaped hydroxyapatite spacer blocks were anchored to the split spinous process using ETHICON™ PDS® (polydioxanone) and ETHICON™ VICRYL® (polyglactin) sutures through the drill holes. Intra operative photographs are shown in Figure 1. A suction drain was put the subfascial layer before wound closure. The wound was closed with absorbable sutures. The drain was kept postoperatively until the daily output is less than 50 ml/24 h. All patients were given a rigid neck collar after the operation for six weeks. Patients were discharged from hospital if they could walk safely with a walking aid or transferred to a rehabilitation unit if further training is required.
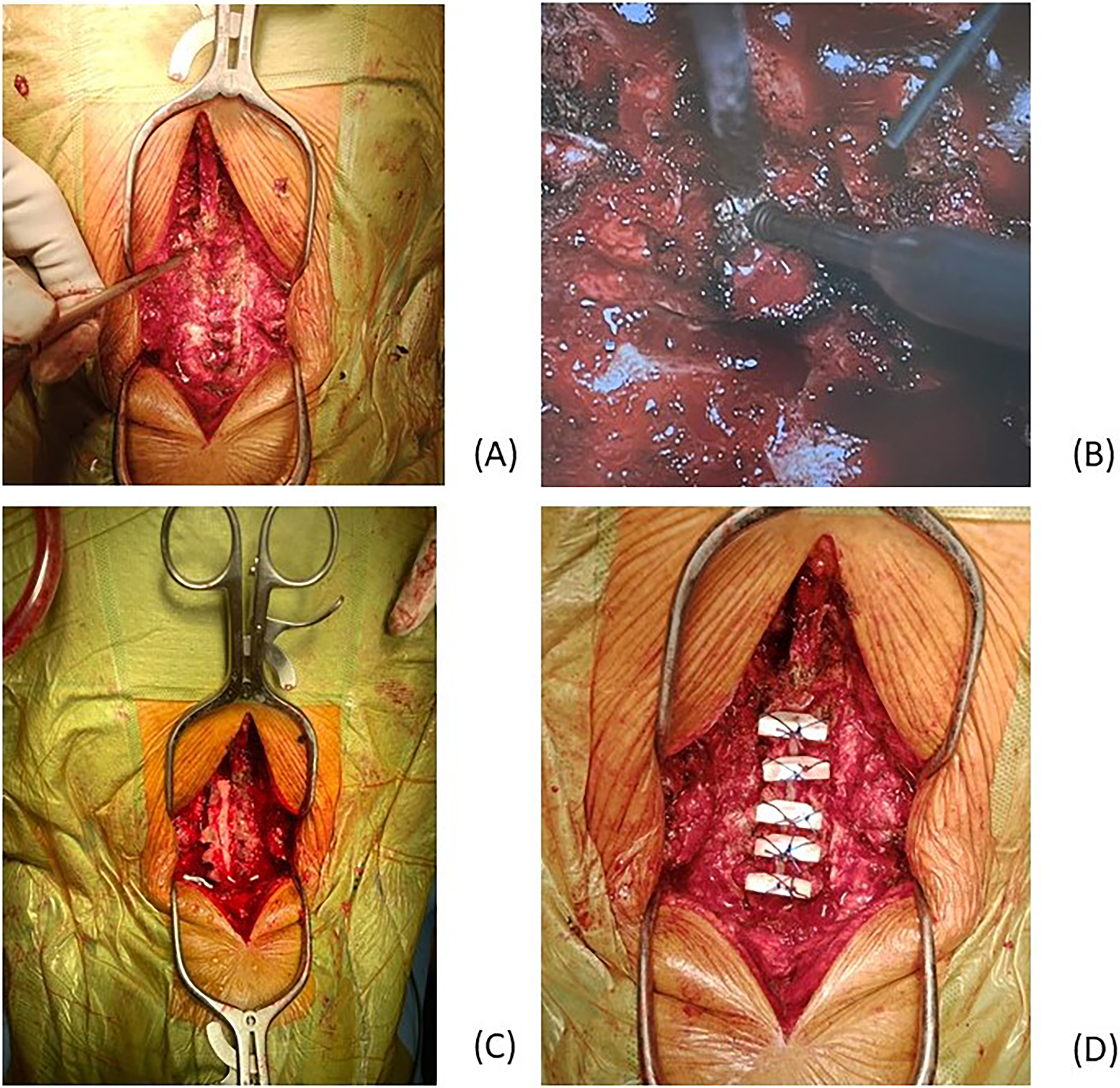
(a) Longitudinal groove created at junction of lamina and facet with high-speed burr. (b) Spinous process split in midline using high speed burr. (c) Split laminas opened. (d) Hydroxyapatite spacer blocks anchored to split spinous process with sutures.
Outcome measures
The lordosis between C2 and C7 was measured on lateral cervical spine X-ray taken in neutral position using the Cobb's method (from inferior endplate of C2 to inferior endplate of C7) (Figure 2). A positive value indicates lordosis while a negative value indicates kyphosis. The C2–7 lordosis were measured before operation and at the final follow up. The main outcome measures were the postoperative C2–7 lordosis and change in C2–7 lordosis defined as postoperative C2–7 lordosis—preoperative C2–7 lordosis.
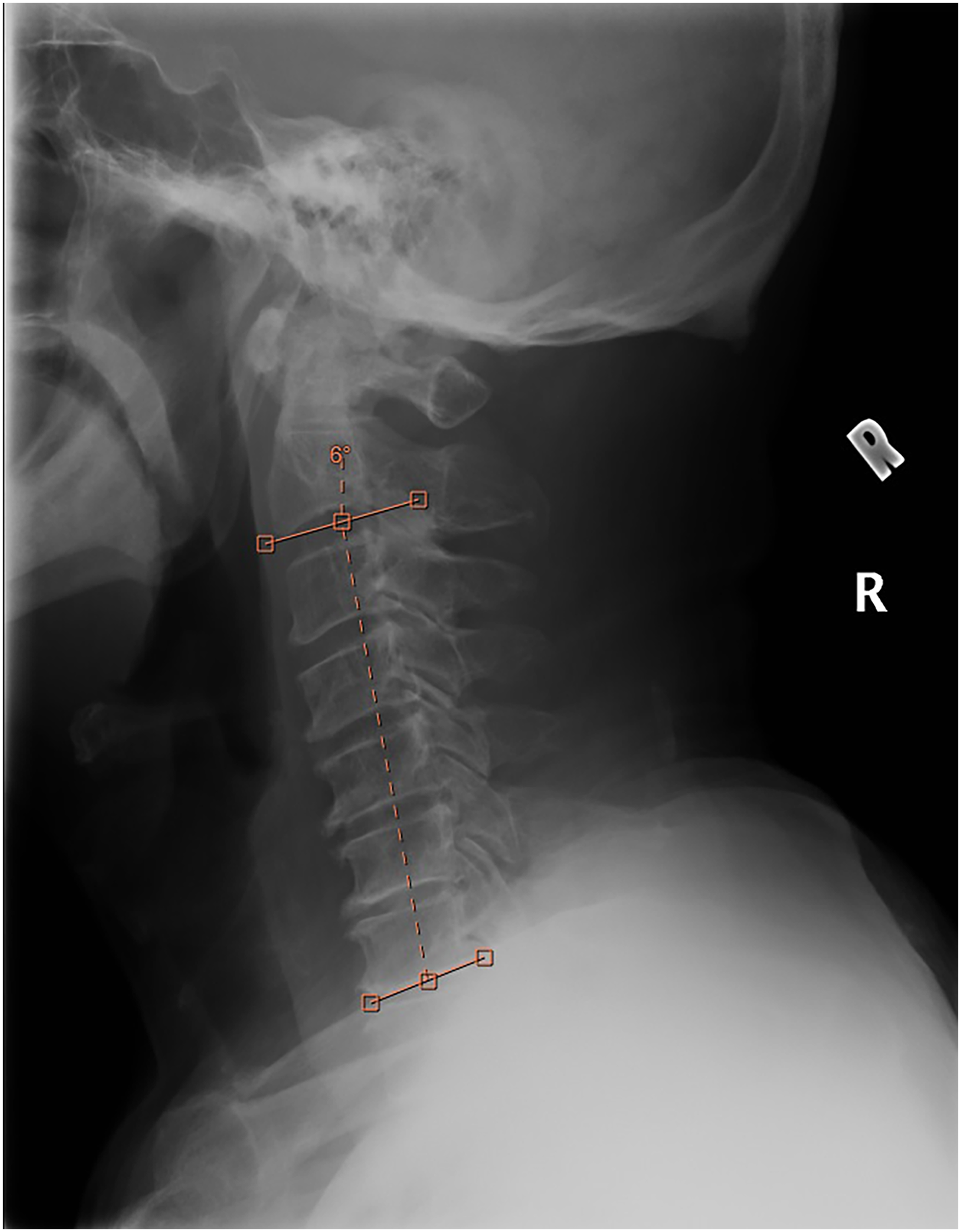
The lordosis between C2 and C7 measured on lateral cervical spine X-ray taken in neutral position using the cobb's method (from inferior endplate of C2 to inferior endplate of C7). A positive value indicates lordosis while a negative value indicates kyphosis.
Study design and statistical analysis
We compared the baseline demographic, diagnosis and preoperative C2–7 lordosis between the patients with an intraoperative hinge fracture and without intraoperative hinge fracture. We also compared postoperative C2–7 lordosis as well as the change in C2–7 lordosis between these two patient groups. Figure 3 shows the flowchart in patients’ selection.
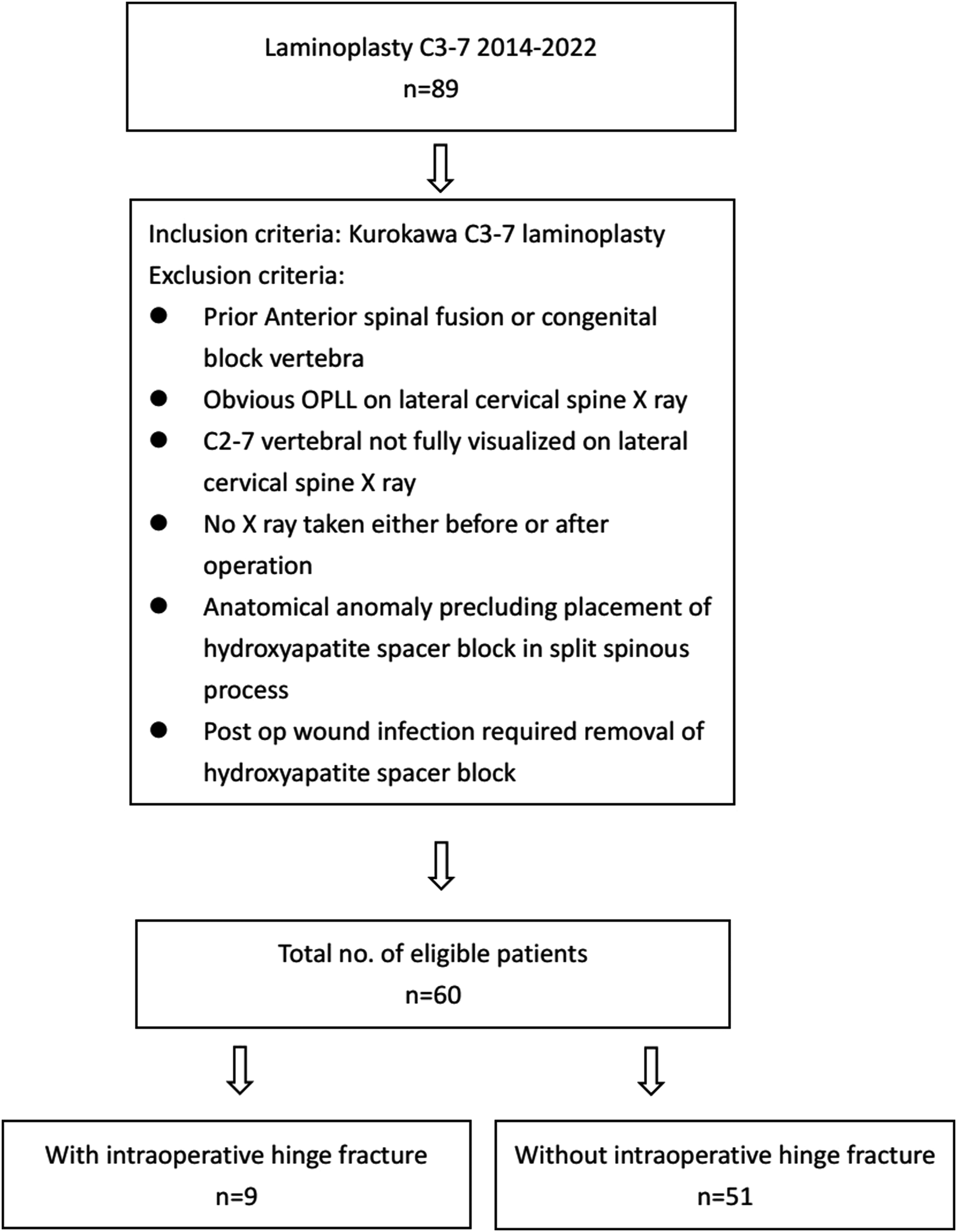
Flowchart showing the procedures in patients’ selection.
Patient's demographics (age, sex) and diagnosis were compared using the Mann–Whitney U test (age) and chi-square test (sex and diagnosis). Pre-op and post-op C2–7 lordosis, change in C2–7 lordosis and follow-up duration (months) were compared using Mann–Whitney U test. Data analyses were carried out using IBM SPSS 28 (Armonk, NY: IBM Corp). A two-sided p-value of ≤.05 was considered statistically significant.
Results
Patient's characteristics
Of the 60 patients eligible to be recruited, nine patients (15%) were found to have an intraoperative hinge fracture. Table 1 shows the baseline characteristics of the patients. The mean age was similar in the two groups (“With hinge fracture” group = 68.8, and “Without hinge fracture” group = 64.5). Percentages of male and female patients in both groups were similar also (88.9% and 74.5% were male patients respectively). Cervical myelopathy was found in 66.7% of patients who suffered from hinge fracture, and in 76.5% of patients without hinge fracture. Follow-up duration of patients without hinge fracture was significantly longer than patients with hinge fracture (18.9 months vs 40.3 months; p = .030). No statistical significance in preoperation C2–7 lordosis between the two groups was found.
Demographic characteristics of the 60 patients.
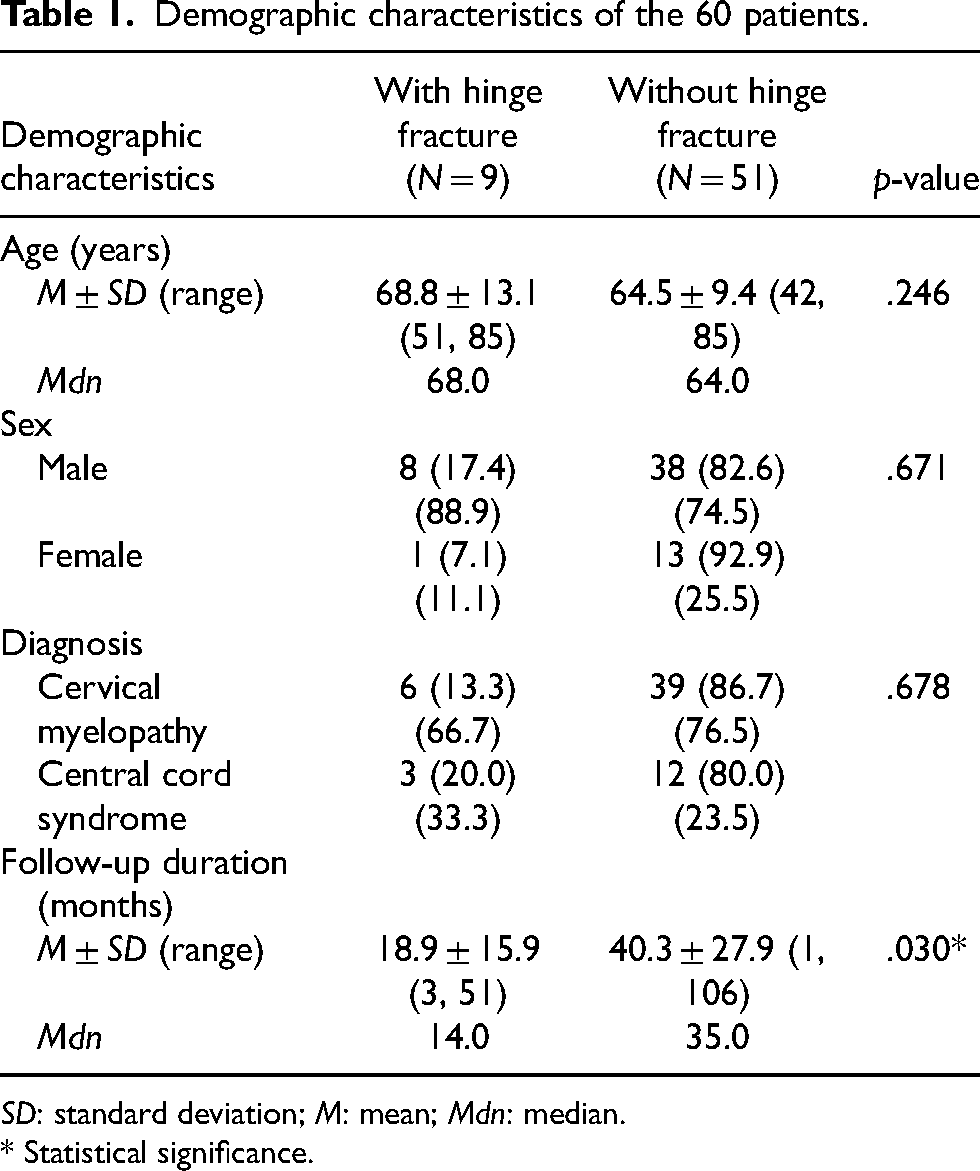
SD: standard deviation; M: mean; Mdn: median.
* Statistical significance.
Table 2 shows the numbers and levels of intraoperative hinge fracture of these nine patients as well as the rescue procedures. Seven patients who sustained an intraoperative hinge fracture at a single level in a unilateral side required removal of the fractured lamina. One patient suffered from a bilateral hinge fracture at C5 level but the broken laminas were successfully retained due to its attachment to the ligamentum flavum and an hydroxyapatite spacer block could still be sutured through the broken split laminas. Another patient suffered from a unilateral hinge fracture at a single level but the broken lamina could still be retained and sutured to the adjacent facet joint capsule.
Details of patients with intraoperative hinge fracture.
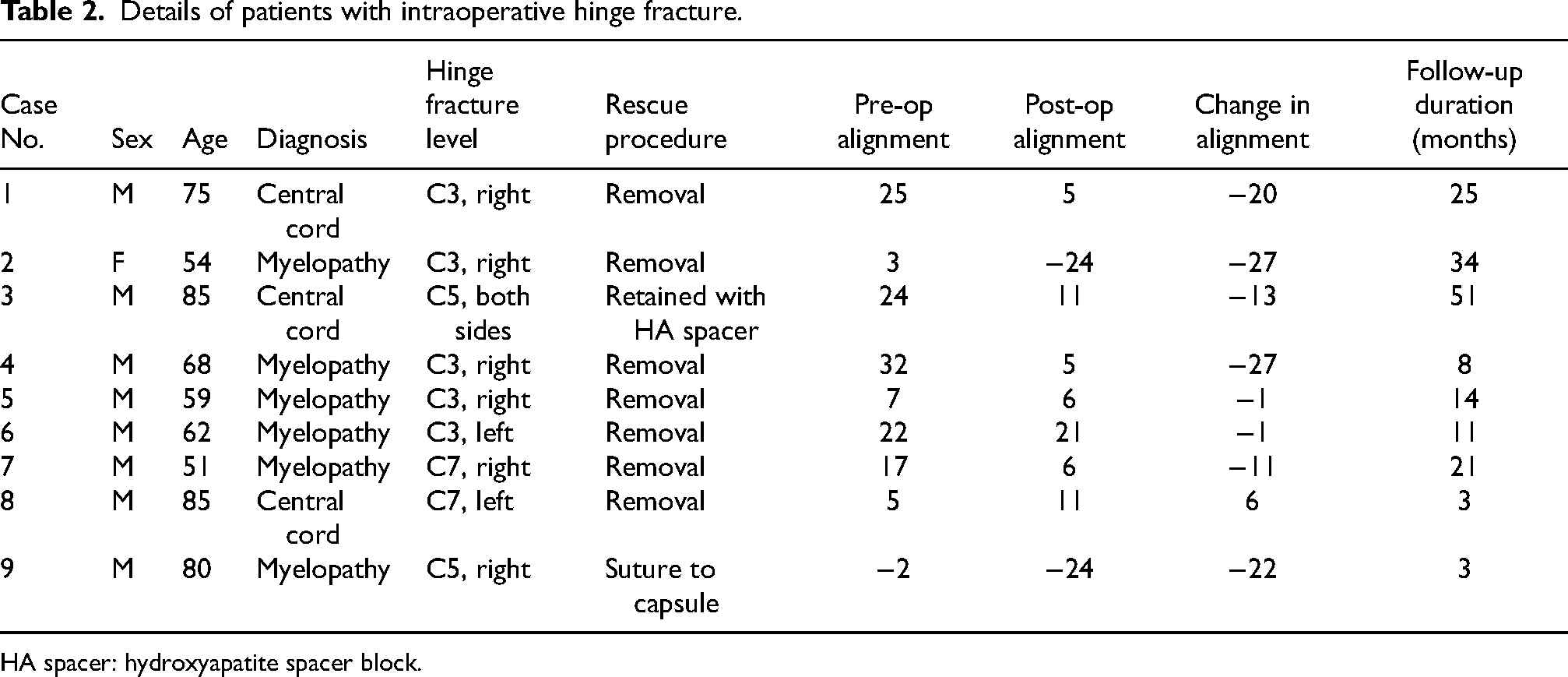
HA spacer: hydroxyapatite spacer block.
Comparison of postoperation C2–7 lordosis and change in C2–7 lordosis
Significant difference was found in postoperation C2–7 lordosis (mean C2–7 lordosis “with hinge fracture” group vs “without hinge fracture” group = 1.89 vs 9.67; p = .044). Median post-op C2–7 lordosis was 6.00 and 10.00 respectively. Change in C2–7 lordosis also showed statistical difference between these two groups (mean change in lordosis = −12.89 vs −3.98; p = .020). The median of change in Cobb's angles were −13.00 and −4.00 respectively. Table 3 summarize the results.
Comparing the pre-op and post-op C2–7 Cobb's angle, and change in Cobb's angle between “within hinge fracture” group and “without hinge fracture” group.
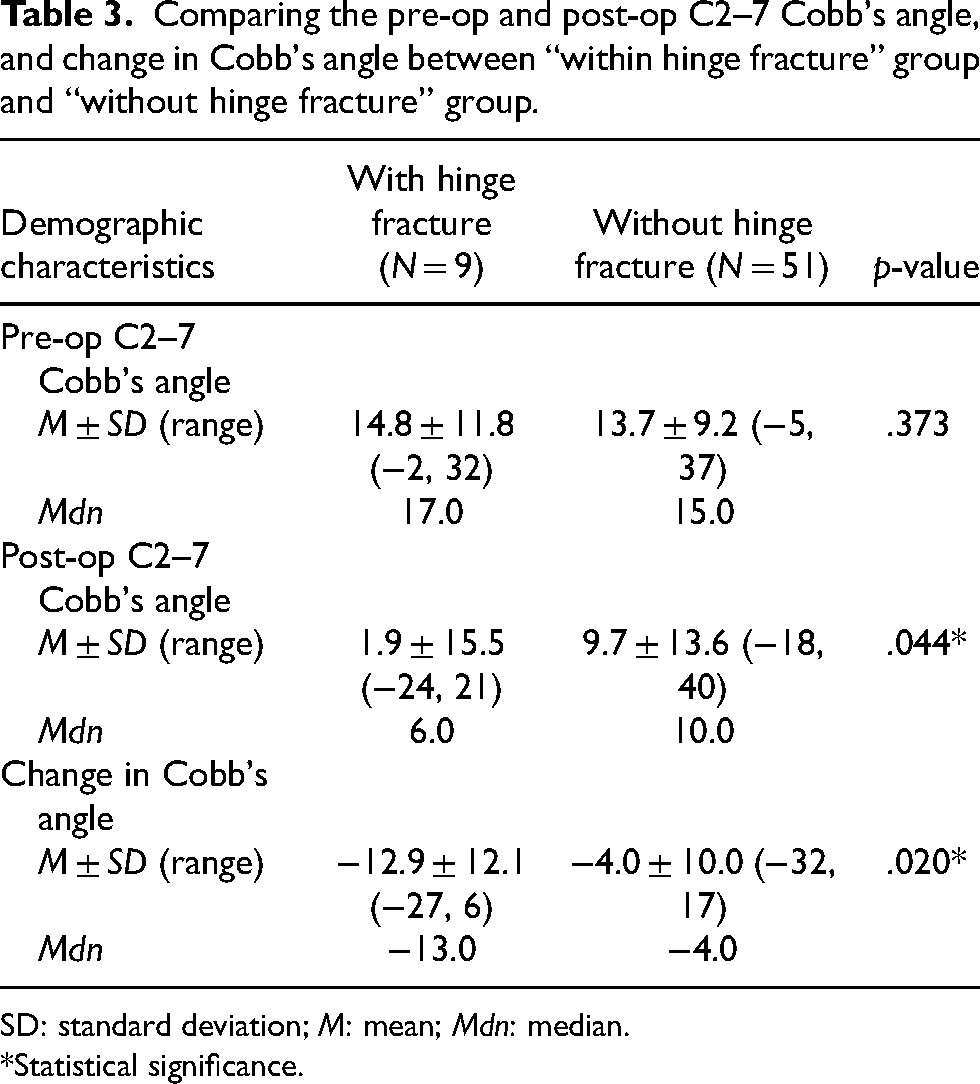
SD: standard deviation; M: mean; Mdn: median.
*Statistical significance.
Discussion
Cervical kyphosis is a known complication of cervical laminoplasty. Several studies have assessed the risk factors associated with development of postlaminoplasty kyphosis in double door laminoplasty. Machino et al. 9 suggested that a preoperative C2–7 lordotic angle of 7° is predictive of postlaminoplasty kyphosis. Kim et al. 12 suggested that a high preoperative T1 slope is associated with increased odds ratio for postoperative kyphosis. Sakai et al. 10 suggested that a center of gravity of the head—C7 SVA (sagittal vertical axis) of 42 mm and age of 75 years old were predictive of postlaminoplasty kyphosis. In the multivariate analysis by Cao et al., 13 cephalad vertebral level undergoing laminoplasty, C2-7 SVA and destroyed facet joints are associated with post laminoplasty kyphosis in his patient cohorts who received unilateral expansive open door cervical laminoplasty.
There are many studies about hinge fracture in open door laminoplasty3–8 with correlations to clinical outcomes such as axial neck pain and JOA score or healing status on computer tomography (CT) scan. However, no study has reported the relationship between hinge fracture and postoperative cervical spine alignment. To the best of our knowledge, this is the first study which assessed the effect of intraoperative hinge fracture in a cohort of patients who received double door laminoplasty. The results of our study are specific as it represents the surgical results of a single procedure carried out by a single surgical team. In the study by Sakaura et al. 14 which compared the differences in postoperative cervical spinal alignment after cervical laminoplasty between patients with cervical spondylotic myelopathy and OPLL, there was a significant higher loss of cervical lordosis in patients with OPLL than cervical spondylotic myelopathy. To make our results more specific we exclude patients with OPLL in the analysis. One may criticize some of the patients in our study had a short follow up duration of one to three months after operation. Choi et al. 15 reported that the change in cervical lordotic angle after laminoplasty peaked in the first month and reached a plateau after six months and was maintained for three years and we believe cases with a follow up duration of one to a few months should be included in the study. Our cases with hinge fracture had a significantly shorter postoperative follow up duration compared with cases without hinge fracture (18.9 months vs 40.3 months). This could be accounted by the recruitment of junior spine surgeons in our unit in the later half of the study, with more intraoperative hinge fracture experienced in the second half of the cases.
Our results suggest that the C3 lamina is more prone to intraoperative hinge fracture. This could be explained by the small size of the C3 spinous process and thin lamina making it more susceptible to fracture. The importance of C2 extensor muscle attachment in the post operative cervical spinal alignment in laminoplasty have been demonstrated by several studies.16,17 We believe the attachment of ligamentum flavum to C2 also plays a role in the maintenance of cervical spinal alignment and hinge fracture at C3 level will cause disruption of the ligamentum flavum attachment to C2, causing postoperative loss of cervical lordosis.
One may question the clinical significance of this study. Several studies had demonstrated that patients with postoperative cervical kyphosis is associated with worse clinical outcome after cervical laminoplasty. In the study by Sakaura et al., 14 the recovery rate of the JOA score was significantly lower in the postoperative kyphosis subgroup than the postoperative lordosis subgroup in patients with cervical spondylotic myelopathy but not for patients with OPLL. In another study by Yang et al., 18 postoperative arm pain improved significantly in patients without postoperative cervical kyphosis but not for patients with postoperative cervical kyphosis. Our results demonstrated that intraoperative hinge fracture is associated with loss of cervical lordosis to a mean C2–7 Cobb's angle of 1.9° of lordosis only, and this could be associated with worse clinical outcome.
There are several limitations to our study. First, our study used the C2–7 lordosis as the only outcome measure. Clinical outcome (e.g., JOA score) was not included as outcome measure. This was because 15 out of 60 patients (25%) suffered from central cord syndrome in which most of whom did not have preexisting cervical myelopathy symptoms and thus they did not have a preoperative JOA score. For the radiological outcome measures, we did not include T1 slope or C2–7/center of gravity of the head (CGH)-C7 sagittal vertical axis (SVA). In many of our patients the T1 vertebra was obscured by the shoulder and inclusion of T1 slope in analysis will further reduce the sample size. Measurement of SVA on plain cervical spine X-ray may be associated with magnification errors. As pointed out by Morimoto et al., 19 cervical radiographs taken using setups that involve different distances between the X-ray tube and film can diminishes reproducibility because the CGH-C7 SVA is affected by magnification error. Instead, he suggested that the CGH-C7 angle is a more objective parameter because it does not vary with the distance between the patient and the X-ray tube. Second, the presence of hinge fracture was based on the intraoperative assessment by the surgeons only. In previous literatures on hinge fracture in open door laminoplasty,3–8 CT scans were used in the assessment of the hinges with many of the hinge fracture cases picked up on postoperative CT scan. Our results may underestimate the true incidence of hinge fracture as some of the hinges might have fractured rather than exhibiting a plastic deformation. Third, the case number in our study is limited because of the strict inclusion and exclusion criteria. We limit our study to cases who received double door laminoplasty at C3–7 segments to give a more specific result. A larger study with more case number is mandatory to give a more conclusive result.
Conclusions
Our results suggest that in patients undergoing double door cervical laminoplasty, intra-operative hinge fracture is associated with development of postoperative kyphosis in the cervical spine.
Footnotes
Author contribution:
Concept or design: Yu Chung Wong; acquisition of data: Yu Chung Wong; and analysis or interpretation of data: Wai Wang Chau; drafting of the manuscript: Yu Chung Wong; critical revision for important intellectual content: Kin On Kwok and Sheung Wai Law. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the ethics review board of the Joint New Territories East Cluster/Chinese University of Hong Kong Ethics Committee (Ref No. 2023.319).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
This study is a retrospective cohort study. Our institution did not require informed consent for retrospective studies.