
Abstract
Study Design:
A retrospective multicenter study.
Objective:
Routine cervical spine surgeries are typically associated with low complication rates, but serious complications can occur. Intraoperative death is a very rare complication and there is no literature on its incidence. The purpose of this study was to determine the intraoperative mortality rates and associated risk factors in patients undergoing cervical spine surgery.
Methods:
Twenty-one surgical centers from the AOSpine North America Clinical Research Network participated in the study. Medical records of patients who received cervical spine surgery from January 1, 2005, to December 31, 2011, were reviewed to identify occurrence of intraoperative death.
Results:
A total of 258 patients across 21 centers met the inclusion criteria. Most of the surgeries were done using the anterior approach (53.9%), followed by posterior (39.1%) and circumferential (7%). Average patient age was 57.1 ± 13.2 years, and there were more male patients (54.7% male and 45.3% female). There was no case of intraoperative death.
Conclusions:
Death during cervical spine surgery is a very rare complication. In our multicenter study, there was a 0% mortality rate. Using an adequate surgical approach for patient diagnosis and comorbidities may be the reason how the occurrence of this catastrophic adverse event was prevented in our patient population.
Introduction
Low back and neck problems are among the top 5 surgically treated conditions in the United States. Due to its intricate structure, the cervical spine is exposed to increased stress and loads that can lead to various conditions such as degenerative or herniated discs, stenosis, and osteoarthritis. Depending on the disease severity, patients can be treated conservatively or surgically. 1 For most of the patients the first line of treatment is usually the nonoperative management including oral medication, physical therapy, bracing, and changes in the activity. 1 It has been shown that in the 70% to 80% of the patients with cervical radiculopathy, nonsurgical treatments were successful. 2 On the other hand, trauma or chronic conditions can require surgical intervention. 1,2 Common primary goals of cervical spine surgery are to decompress spinal cord and nerves and stabilize the spine when needed.
Although the clinical success of cervical procedures is very high, several complications have been reported. It has been show that the type of surgical approach can contribute to the complication onset. Fager reported that patients who were treated anteriorly for cervical degenerative conditions with myelopathy had a 10% higher chance for developing neurological complications. 3 Intraoperative complications associated with both anterior and posterior approaches include esophageal and tracheal perforation; injury of main arteries; hematoma, wound infections; spinal cord and nerve injury; dura leak; and improper positioning of instrumentation and graft. 4,5 Some of the primary complications can lead to death. A 5-year report done by the Cervical Spine Research Society (1982 to 1987) on the death incidence after cervical spinal surgery demonstrated low mortality rates, ranging from 0.34% to 0.96%, with 1982/1983 and 1985/1986 having the highest rates (0.95% and 0.96%, respectively). 4 They further reported that the cord-related complications were more prevalent with the posterior approach and nerve root with the anterior approach. 4 Even though death is a secondary adverse event there are several variables that can influence the mortality rates. First, the incidence magnitude differs between elective and emergency room procedures. 6 Second, there are reports that demographic factors (age and race) play an important role. 7,8 Skolasky and coworkers have shown an overall 0.42% mortality rate and found that African Americans had 59% higher odds of dying after cervical spine surgery compared to Caucasian patients. 7 In addition, Alosh et al found that African Americans had 57% higher odds of death as a terminal complication after anterior cervical spine surgery. 8 Last, an overall mortality incidence will be directly linked to the patient’s medical condition.
Although there is literature on the death incidence with spine surgeries, most of the studies focused on the postoperative mortality rates or on the complications leading to death. The purpose of our multicenter study was to determine the incidence of intraoperative death in patients undergoing cervical spine surgery. We also sought to address the correlation between patient demographics, surgical approach, and intraoperative death rates.
Material and Methods
We have conducted a retrospective multicenter case series study involving 21 high-volume surgical centers from the AOSpine North America Clinical Research Network, selected for their excellence in spine care and clinical research infrastructure and experience. All the centers were academic, teaching hospitals. Medical records for 17 625 patients who received cervical spine surgery between January 1, 2005, and December 31, 2011, inclusive, were reviewed to identify occurrence of 21 predefined treatment complications. The complications included reintubation requiring evacuation, esophageal perforation, epidural hematoma, C5 palsy, recurrent laryngeal nerve palsy, superior laryngeal nerve palsy, hypoglossal or glossopharyngeal nerve palsy, dural tear, brachial plexopathy, blindness, graft extrusion, misplaced screws requiring reoperation, anterior cervical infection, carotid artery injury or cerebrovascular accident, vertebral artery injuries, Horner’s syndrome, thoracic duct injury, quadriplegia, intraoperative death, revision of arthroplasty, and pseudomeningocele. Trained research staff at each site abstracted the data from medical records, surgical charts, radiology imaging, narratives, and other source documents for the patients who experienced one or more of the complications from the aforementioned list. Patient demographics were collected at the time of surgery. Data was transcribed into study-specific paper case report forms. Copies of case report forms were transferred to the AOSpine North America Clinical Research Network Methodological Core for processing, cleaning, and data entry.
Results
From the initial 17 625 patients, 258 patients met the inclusion/exclusion criteria and were used in the study. There were 141 male (54.7%) and 117 female (45.3%) patients (Table 1). The average age was 57.1 ± 13.2 years, and the mean body mass index was 28.8 ± 6.5. Fifty-two patients were current smokers, 69 were previous smokers and 111 never smoked (Table 1).
Patient Demographics.
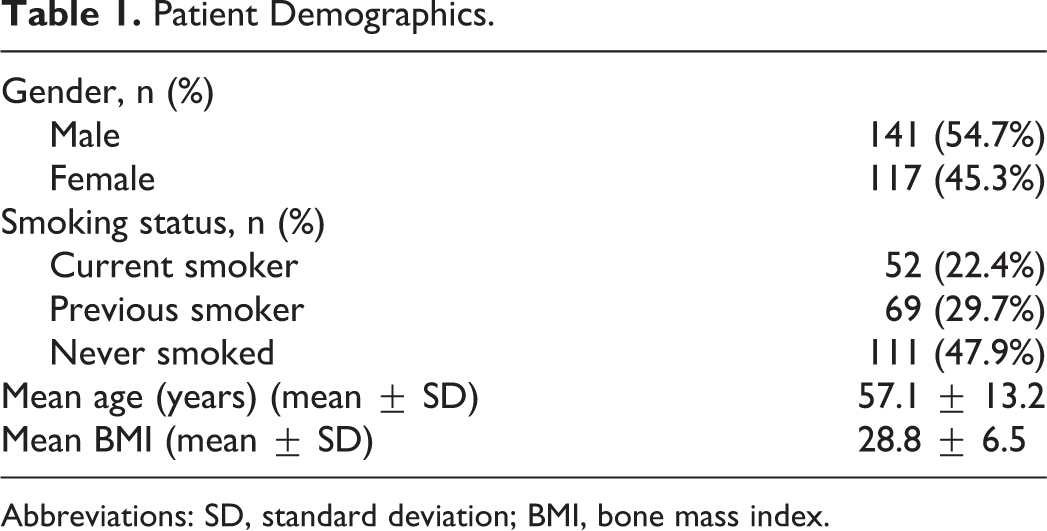
Abbreviations: SD, standard deviation; BMI, bone mass index.
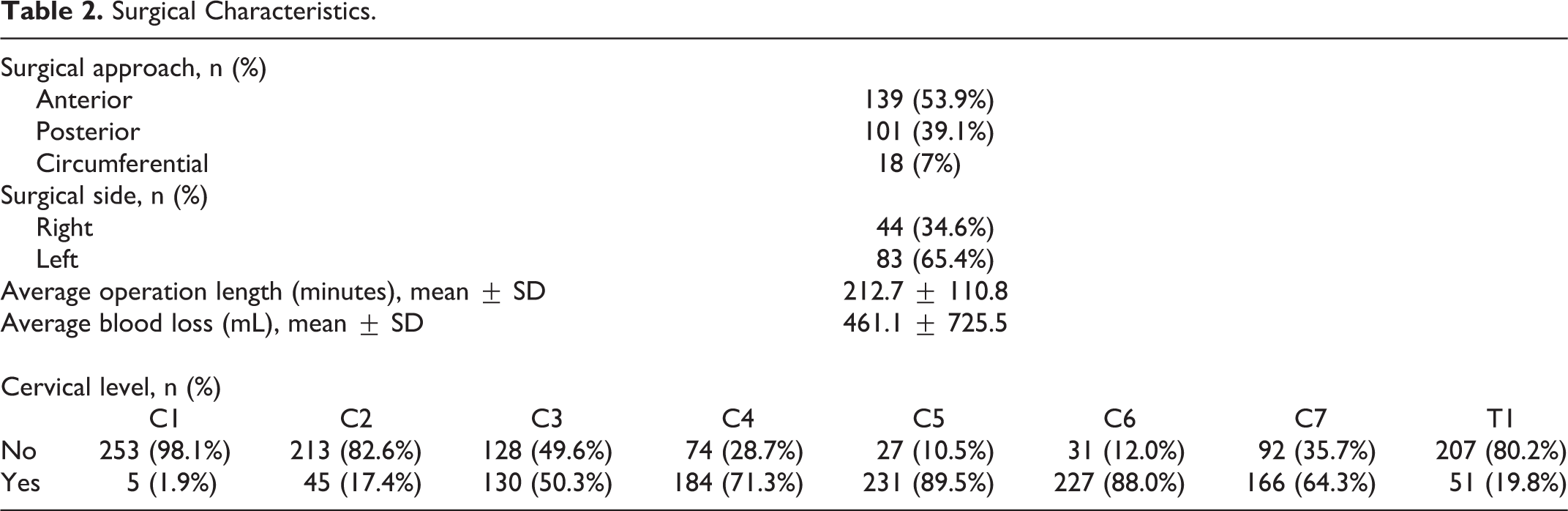
The most common procedure was the anterior approach 139 (53.9%), followed by posterior 101 (39.1%) and circumferential 18 (7%) approaches; and for most of the cases surgery was done on the left side (65.4%; Table 2). Average length of surgery was 212.7 ± 110.8 minutes, and the average blood loss was 461.1 ± 725.5 (Table 2).
Surgical Characteristics.
There was no intra-operative death in our study, and the total incidence of other rare complications was low (Table 3).
Rare Complications.
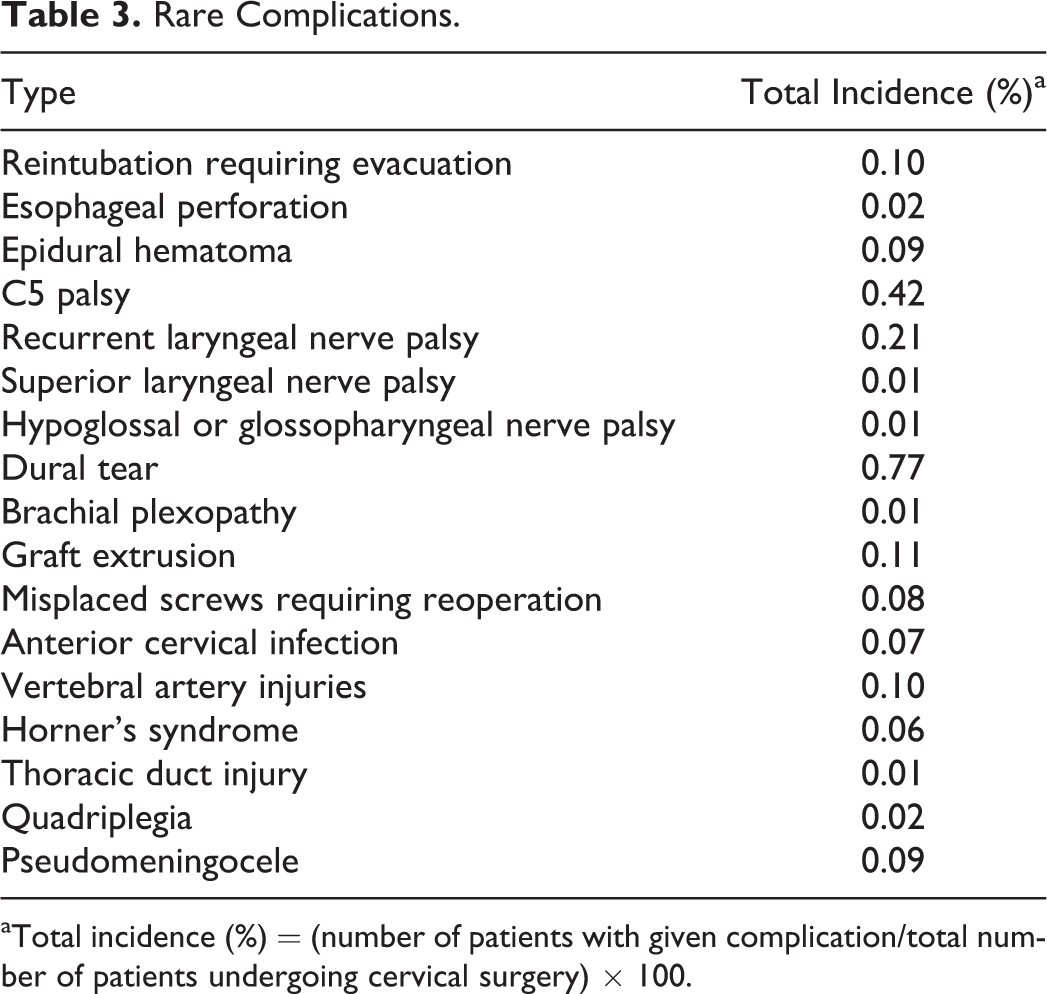
aTotal incidence (%) = (number of patients with given complication/total number of patients undergoing cervical surgery) × 100.
Discussion
In the past decades, there has been immense progress in understanding the link between pathophysiological changes and spine biomechanics, leading to defined cervical surgical approaches. The risk of complications is inevitable but it can be reduced with the proper surgical indications that are appropriate for the pathology present.
Our data shows that among 21 centers, there was no case of intraoperative deaths in elective cervical spine surgeries. We did not measure the mortality rate of postoperative deaths in our series of patients. The low risk of postoperative death has been previously reported. Goz and coworkers indicated that the mortality rates after spine surgery remained constant over a 10-year period. 9 Thoracic spine surgery had the highest death incidence (1.2%), followed by cervical (0.46%) and lumbar (0.14%). A similar pattern was observed in another database study, with the mortality incidence being 0.57%, 0.13%, and 0.11% for the thoracic, cervical, and lumbar regions, respectively. 10 Both studies found that older age (>65 years), male patients, and various comorbidities (congestive heart failure, chronic pulmonary disease, neurological disorders, metastatic cancer, renal failure, weight loss) strongly correlated with the risk of in-hospital death. In our study, the mean patient age was 54 years, and 54.7% were male patients.
One of the key factors that can lead to an increase in death incidence is the nature of the surgery, whether it is emergent or elective. A prospective study on spinal surgery with 471 patients receiving elective surgery and 471 patients receiving emergency surgery reported an overall 2.1% mortality rate. 6 In the study by Street et al, 6 there was only one death in the elective surgery group, and 19 in the emergency group, mainly in patients with trauma or spinal tumors. In our retrospective study, all the surgeries were elective and no intraoperative death was observed. Furthermore, a retrospective database study reported 0% postoperative mortality rates after ambulatory cervical surgeries over a 5-year time period. 11 The majority of these cases (68%) were done using the anterior cervical discectomy and fusion, similar to our study where 53.9% of the patients underwent an anterior approach.
The impact of teaching and nonteaching hospitals on the death incidence rates after spine surgery has been an extensive ongoing debate. Numerous studies have shown that teaching hospitals in general perform better when it comes to the more complex surgeries and that mortality rates are lower or similar to nonteaching hospitals. 12 -14 However, Fineberg et al found a significant difference in mortality rates between teaching and nonteaching hospitals (1.2 vs 0.6 per 1000). 15 Some of the predictors for this high incidence were patient age, weight loss, neurological, pulmonary, and cardiac comorbidities and complications. Another contributing factor in this study was the surgery complexity, which was higher at the teaching hospitals. 15 Our data is in agreement with these reports; all the centers in our study were teaching institutions and the complication rates were low.
One of the most common complications after cervical surgery occurs in the region of the esophagus. Patients with anterior cervical discectomy and fusion procedures in particular are at a higher risk of dysphagia, laryngeal nerve injury, and pharynx wall swelling. Those complications can lead to aspiration pneumonia, which can be fatal. Fineberg et al looked at the influence of aspiration on the death incidence after anterior fusion, posterior fusions, or posterior decompression. 16 The aspiration incidence was 5.3 per 1000, and it was more common in older patients and male patients. Mortality rates were significantly higher in patients with aspiration compared to those without (34.4 vs 0.7 per 1000). The highest mortality rates were observed in multilevel surgeries (3 or more levels) and in posterior cervical fusions. The aspiration and mortality rates were strongly correlated with older age and male gender. In our study, the incidence of esophageal perforation was very low (0.02%), and most of the cases were done using the anterior approach. Another study looking at the trends of cervical surgery with and without human recombinant bone morphogenetic protein 2 (rhBMP2) found that posterior cervical fusion had the highest mortality rate of 12.6 per 1000 compared to 2.9 per 1000 for anterior cervical fusion and 3.2 per 1000 for posterior cervical decompression. 17
Injury of the vertebral artery during anterior cervical fusion can lead to a fatal outcome. A systematic review done by Park and Jho 18 found that among 39 cases (17 studies) that underwent anterior cervical approach only one case ended up fatally due to excessive bleeding and 45% of the patients had delayed vascular complications.
Myelopathy is possibly the comorbidity with the highest influence on morbidity rates associated with cervical surgery. Patients who had myelopathy and an anterior cervical procedure had a higher mortality rate compared to nonmyelopathy patients (0.52% vs 0.05%). The posterior approach was not strikingly different, but the mortality rates were higher overall in myelopathy patients (0.67% vs 0.36% respectively). 19 One of the most probable explanations is that myelopathy can lead to a sequel of perioperative complications obstructing vital functions. Similar findings with a 0.8% mortality were reported by other investigators. 20 Wang and coauthors further found that patients over 75 years of age and with myelopathy had a 19 times higher chance of dying after cervical spine surgery, posterior or circumferential. 21
Even though there is data on death after cervical spine surgery, several reports have shown that those trends are stable or declining. Patil et al have shown that despite the 2-fold increase in the number of cervical procedures over a decade, the average mortality and length of stay decreased, suggesting improvement in surgical approach and patient care. 22
There are several limitations to our study, including that it was retrospective. The major limitation was the study size, as only 258 patients met the inclusion criteria. Within each center, cases originated from a single surgeon potentially introducing bias due to the highly defined surgical setting. Furthermore, other demographic data known to affect mortality rates such as ethnicity or previous conditions was not collected. Despite those limitations and no death cases, our study suggests that using an adequate surgical approach for patient diagnosis and comorbidities may prevent the occurrence of this intraoperative death.
Conclusions
Death after cervical spine surgery is a very rare complication. In our multicenter study, there was no incidence of intraoperative death. Our findings further strengthen the notion that low complication rates and proper surgical skills can diminish the circumstances that could lead to intraoperative death.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jeffrey C. Wang reports royalties (Aesculap, Biomet, Amedica, Seaspine, Synthes), stock ownership (Fziomed), private investments (Promethean Spine, Paradigm spine, Benevenue, NexGen, Vertiflex, electrocore, surgitech, corespine, expanding orthopaedics, osprey, bone biologics, curative biosciences, pearldiver), Board of Directors (North American Spine Society [nonfinancial, reimbursement for travel for board meetings, courses, etc.], North American Spine Foundation [nonfinancial], Cervical Spine Research Society [nonfinancial, reimbursement for travel for board meetings], AOSpine/AO Foundation [honorariums for board position], fellowship support (AO Foundation [spine fellowship funding paid to institution]; Zorica Buser reports Xenco Medical (consultancy), AOSpine (consultancy, past) Zorica Buser reports grants from AOSpine North America during the conduct of the study; David Fish reports grants from AOSpine North America during the conduct of the study; Elizabeth L. Lord reports grants from AOSpine North America during the conduct of the study; Allison Roe reports grants from AOSpine North America during the conduct of the study; Dhananjay Chatterjee reports grants from AOSpine North America during the conduct of the study; Erica Gee reports grants from AOSpine North America during the conduct of the study; Erik Mayer reports grants from AOSpine North America, during the conduct of the study; Marisa Yanez reports grants from AOSpine North America during the conduct of the study; Owen McBride reports grants from AOSpine North America during the conduct of the study; Peter Cha reports grants from AOSpine North America during the conduct of the study; Paul Arnold reports grants from AOSpine North America during the conduct of the study; other from Z-Plasty, other from Medtronic Sofamore Danek, other from Stryker Spine, other from FzioMed, other from AOSpine North America, other from Life Spine, other from Integra Life, other from Spine Wave, other from MIEMS, other from Cerapedics, other from AOSpine North America, outside the submitted work; Michael G. Fehlings reports grants from AOSpine North America during the conduct of the study; Thomas E. Mroz reports other from AO Spine, grants from AOSpine North America during the conduct of the study; personal fees from Stryker, personal fees from Ceramtec, other from Pearl Diver, outside the submitted work; K. Daniel Riew reports personal fees from AOSpine International, other from Global Spine Journal, other from Spine Journal, other from Neurosurgery, personal fees from Multiple Entities for defense, plantiff, grants from AOSpine, grants from Cerapedics, grants from Medtronic, personal fees from AOSpine, personal fees from NASS, personal fees from Biomet, personal fees from Medtronic, nonfinancial support from Broadwater, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by AOSpine North America Inc, a 501(c)3 nonprofit corporation.