
Abstract
Introduction
The rehabilitation of patients after flexor tendon repair has been debated for more than half a century. Initially it was suggested that one should adopt immobilization during the exudative phase of wound healing. 1 The emergence of the Kleinert regimens was a breakthrough, promoting early movement of the affected digits by the aids of a rubber band. 2 The efficiency of the Kleinert protocol has been verified by numerous studies in the past.3–5 Due to the well proven results of the Kleinert protocol, most of our local institutes utilized the Kleinert splintage as the standard rehabilitation protocol.
Starting in the 1980s, the pendulum has shifted toward early active motion with multiple bench studies supporting the benefits of it.6,7 Thus, researchers have tried to further optimize the ideal mobilization strategy. Several studies suggested that wrist extension is effective in minimizing the work of finger flexion when adopting an active mobilization regimen.8–10 This led to the incorporation of wrist motion in flexors rehabilitation by Pecker in 2014, 11 which demonstrated encouraging results.
Later on, the Saint John Protocol was proposed by Higgins and Lalonde in 2016. 12 This protocol allows the patient to perform active finger flexion within a forearm-based splint that places the wrist in extension for the first 2 weeks. They found that with the wrist extended and the metacarpophalangeal (MCP) joint flexed, there is the least tension in the flexor tendon. After 2 weeks, a short Manchester splint is used and this facilitates the synergistic motion of wrist extension and finger flexion to further promote tendon excursions. Despite the existence of this protocol for some time, there is limited evidence supporting its effectiveness. Moreover, according to our recent literature review, no studies have directly compared the Saint John protocol with other traditional protocols, such as the Kleinert rehabilitation protocol.
This retrospective study aims to compare the outcomes of primary flexor tendon repair (zones 1 and 2) using the Saint John protocol, compared with a historical cohort treated with the Kleinert protocol.
The objective of this study is to provide local high-level evidence on the outcomes of the Saint John protocol in patients with acute flexor tendon injuries in zones I and II. This information can then be used to incorporate the protocol into our daily routine and improve patient management.
Materials and methods
All patients with primary zone I/II flexor tendon injuries, admitted to our unit from 2021 to 2023, treated with the Saint John rehabilitation protocol were recruited. The exclusion criteria include: age under 18 years old, associated fracture in the same digit, delayed presentation, patients who failed to comply with the rehabilitation regime, and patients who defaulted follow-up before postoperative 12 weeks. A historical control cohort of patients with primary zone I/II flexor tendon injuries using a Kleinert protocol, admitted from 2015 to 2021, were recruited for comparison.
Surgical technique
All the operations were performed within 72 h after admission. For all the cases in the two groups, they were performed in emergency setting by on-call colleagues, which were orthopedic specialists or orthopedic trainees under specialist supervision. The flexors repair utilized the same repair regime. Flexor digitorum profundus and flexor digitorum superficialis tendons were repaired with modified Kessler four-strand repair. 3/0 nonabsorbable sutures were used for the core suture and 5/0 or 6/0 nonabsorbable sutures were used for the epitendinous suture. Smooth gliding of the repairs through the pulley system was ensured at the end of each operation. Venting of pulleys was performed in order to allow adequate free gliding of the repaired tendon, while preserving the pulleys as much as possible. Postoperatively, the affected fingers were protected in a plaster of Paris dorsal blocking slab until the custom-made splints were fitted for the patients.
Kleinert protocol
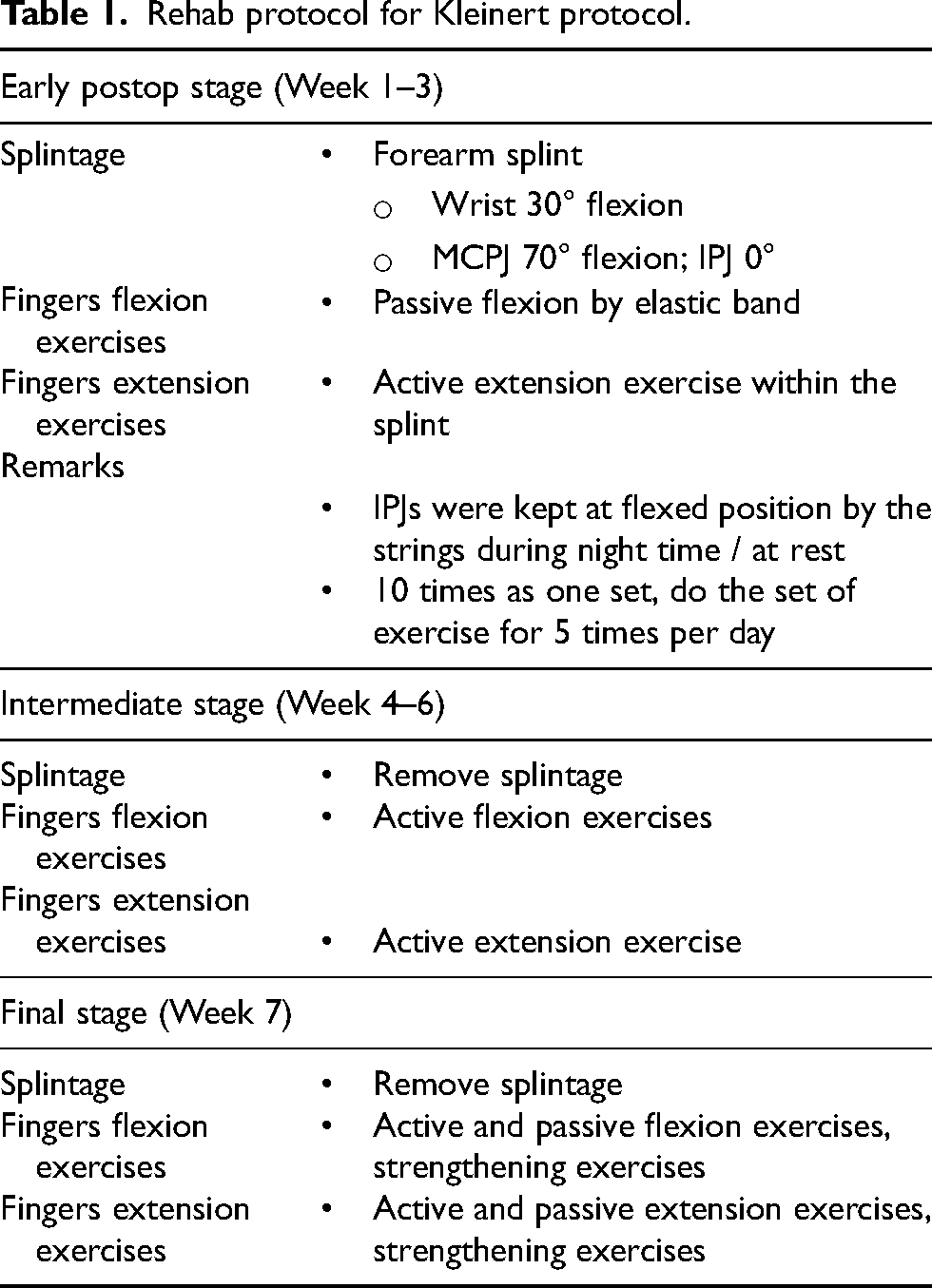
Following surgery, patients were given a temporary immobilization dorsal blocking slab made of plaster of Paris. The next day, rehabilitation began according to the protocol outlined in Table 1, using the Kleinert splint (Figure 1). Patients in the Kleinert protocol would be instructed to use the splint for 3 weeks. Within this period of time, they would perform digital flexion and extension exercises within the Kleinert splintage, in which active extension and passive flexion were carried out. And beginning from the fourth week after repair, patients would remove the Kleinert splintage and perform active finger flexion and extension exercises. Strengthening and passive exercise would then commence in the seventh week.

Kleinert splint. The splint consists of a dorsal slab, volar strips, and an elastic band system. The dorsal slab is contoured to the wrist, flexed at 30 with the metacarpophalangeal joints in 70° of flexion and extending to tip of finger to prevent any hyperextension of the finger. The volar strips consist of a forearm and a palmar component. The elastic band system connects the injured finger via a false nail, and is attached to the spring wire unit in the upper forearm after running under a palmar pulley.
Rehab protocol for Kleinert protocol.
Saint John protocol
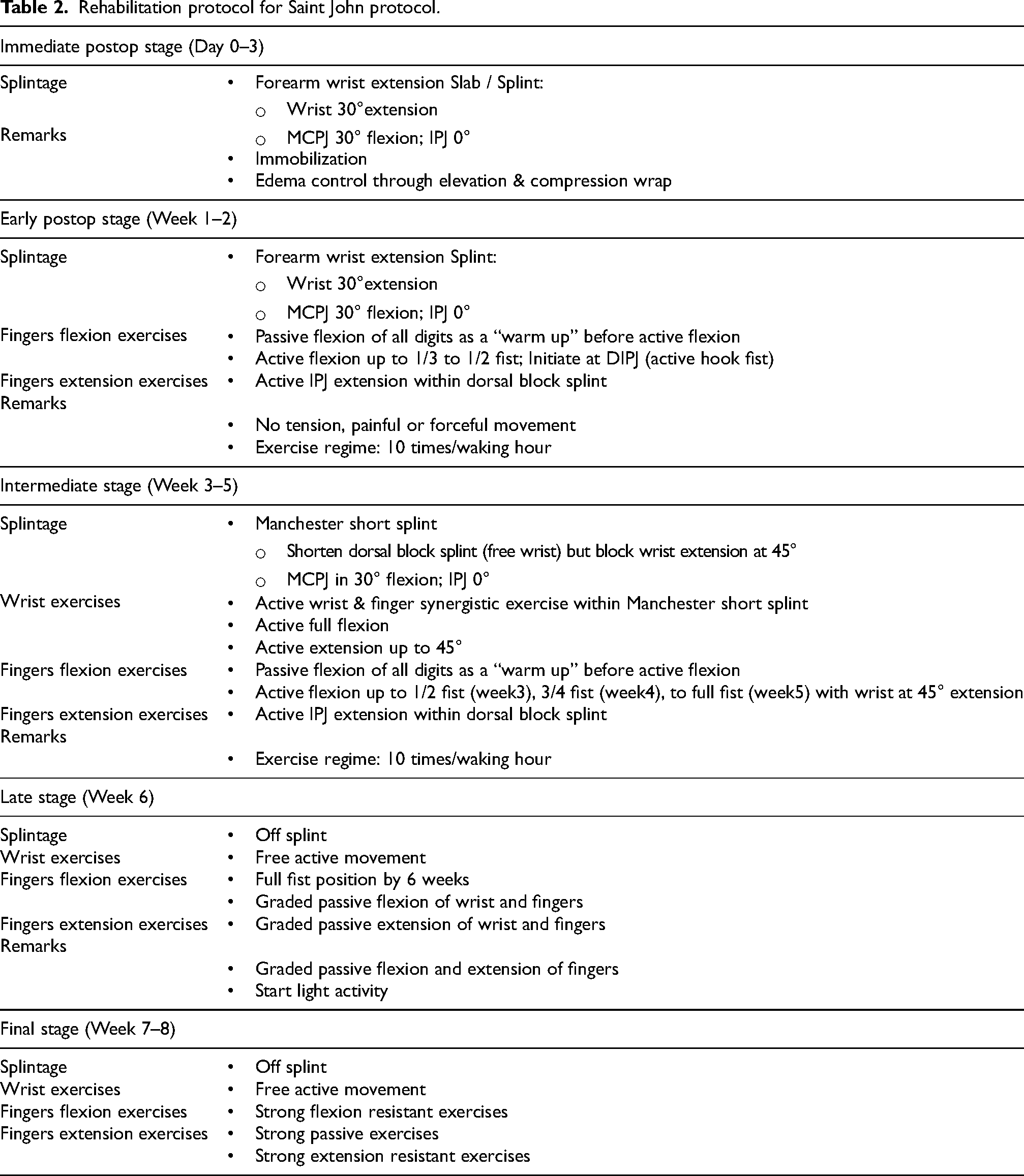
Similar to the Kleinert protocol, patients received a temporary immobilization dorsal blocking slab made of plaster of Paris immediately after surgery. The next day, they underwent a more advanced rehabilitation protocol outlined in Table 2, utilizing two different types of splints: a forearm extension splint (Figure 2) and a Manchester short splint (Figure 3). In the first one to two weeks after surgery, they were fitted with the forearm extension splint that allowed for active finger flexion up to 1/3 to 1/2 of full fist movement, and active IP joint extension within the dorsal block splint. Wrist movement is prohibited in this stage. Starting from the third week, patients were switched to the Manchester short splint, which allowed for active digital flexion exercises with the wrist extended to 45°. Next at sixth week time , splintage was removed for the patients, meanwhile free active wrist/finger flexion and extension, as well as graded passive extension of wrist and fingers were permitted. Finally at the seventh week after the repair, strong passive extension exercises of the fingers were allowed.

Forearm wrist extension splint. The splint consists of a thermoplastic dorsal slab that extends up to the mid forearm, and pieces of volar strips. This splint keeps the wrist at 30° of extension, and MCP joint in 30° of flexion and 0° of IP joint extension. The strips are used to secure the forearm and fingers to the slab.

Manchester short splint. The splint is a thermoplastic dorsal slab that extends just proximal to wrist joint. There are only palmar and finger strips and no wrist strips, as the absence of wrist strips allow for controlled wrist movement. This splint permits maximal wrist flexion and up to 45° of wrist extension, and keeps MCP joint in 30° of flexion and 0° of IP joint extension.
Rehabilitation protocol for Saint John protocol.
Patients with nerve injury
For patients with additional digital nerve injuries on top of flexor tendon injuries, they would undergo the identical rehabilitation protocol with the same splints in both protocols without any additional flexion block.
Evaluation
Demographic information and intraoperative findings were obtained from case notes. Following the surgery, patients were fitted with the appropriate splint and educated on rehabilitation. Patients were assessed at 6 and 12 weeks postoperatively. Pain scores were recorded using a visual analog scale (VAS) ranging from 0 to 10. Range of movement (ROM) was measured using a goniometer for active and passive flexion and extension of the affected fingers at the MCP joint, proximal interphalangeal (PIP) joint, and distal interphalangeal (DIP) joint. Grip strength was measured using a dynamometer. Complications such as infection, adhesion formation, and tendon rerupture were recorded.
Statistical analysis
Statistical analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Continuous variables were analyzed using the independent samples t-test or Mann–Whitney U test, depending on the data distribution. Categorical variables were analyzed using the chi-square test or Fisher's exact test. A P-value of less than 0.05 was considered statistically significant.
Results
Demographics
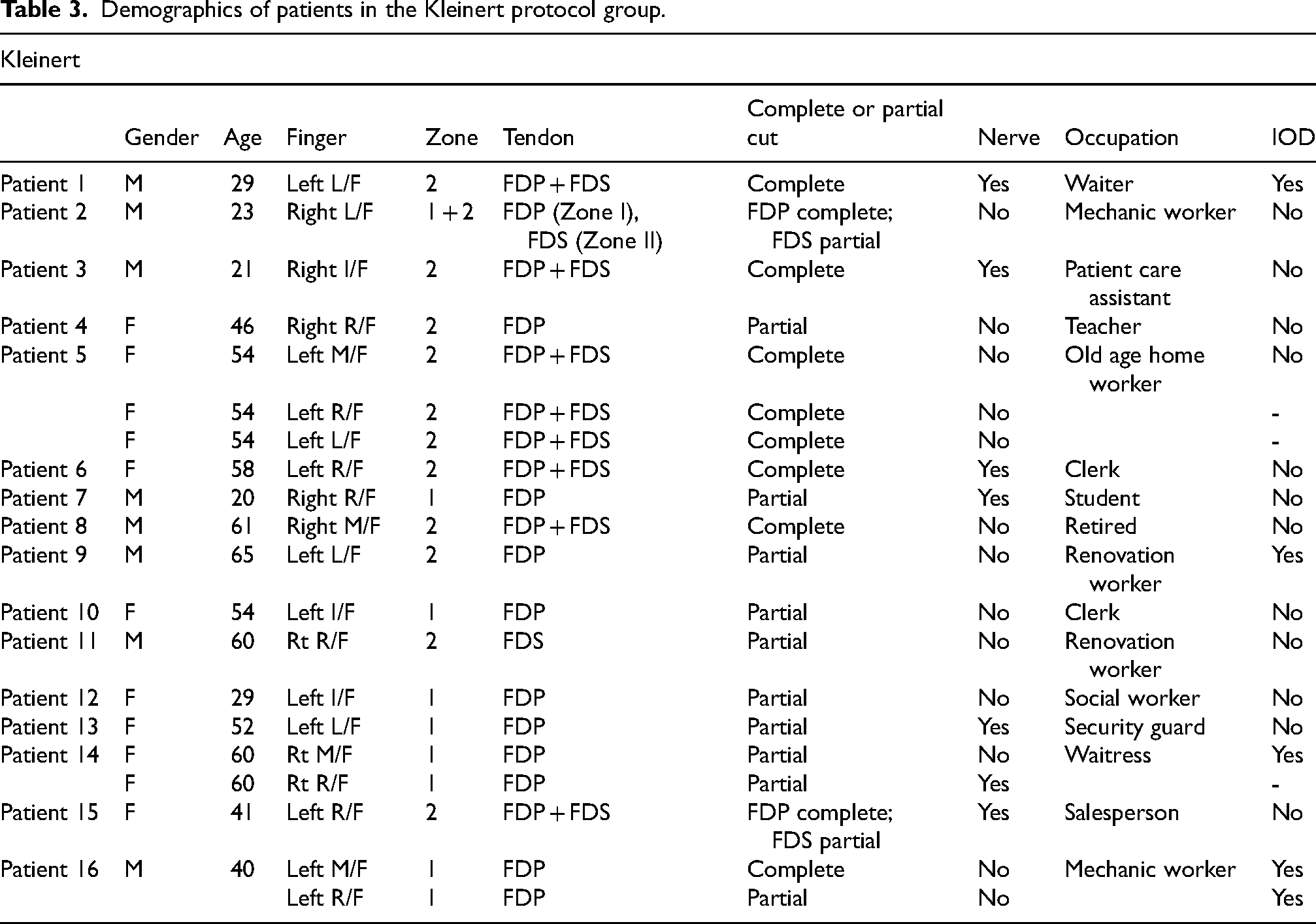
From January 2015 to June 2021, a total of 16 patients with flexor zone I/II repaired were put on the Kleinert protocol as it was the sole rehabilitation protocol at our department. The patients comprised of eight males and eight females. The average age was 46.1. There were 20 fingers involved in this group. 9 fingers belonged to Zone I injury and 11 fingers belonged to Zone II injury. Complete and partial rupture of the flexors each comprised half of all fingers involved. 7 finger injuries were associated with nerve injuries and 13 were isolated tendon injuries. Five patients were alleged to have sustained the injury while on duty (Table 3).
Demographics of patients in the Kleinert protocol group.
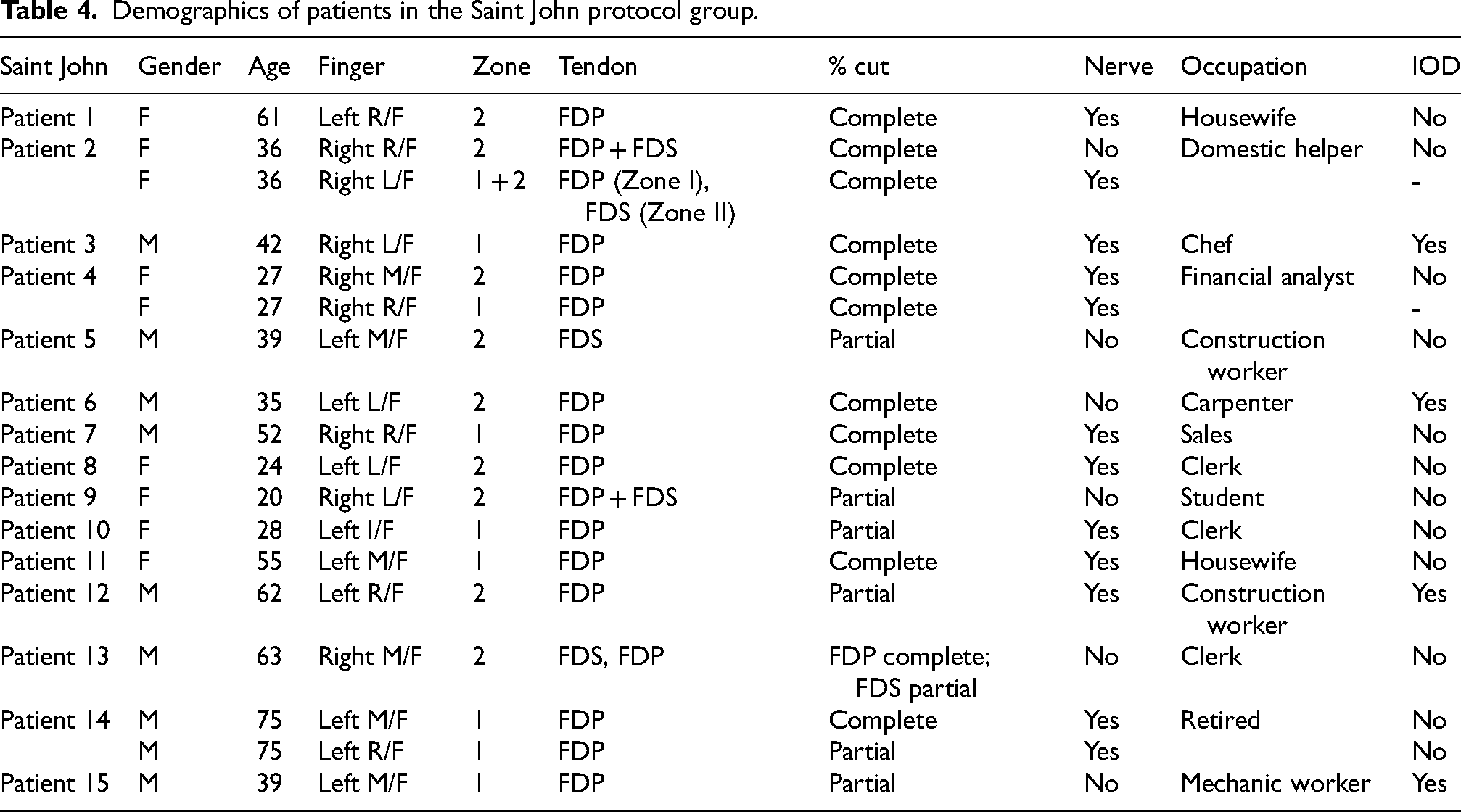
From November 2021 to August 2023, 15 patients with flexor Zone I/II repaired underwent rehabilitation using the Saint John protocol. The patients comprised of eight males and seven females. The average age was 44.2. There were 18 fingers involved in this group. 9 fingers belong to Zone I injury and 9 fingers belong to Zone II injury. Complete rupture of the flexors comprised one-third of all fingers (6 fingers) involved and partial rupture comprised the other two-third (12 fingers). 12 finger injuries were associated with nerve injuries and 6 were isolated tendon injuries. Four patients claimed to have sustained the injury while on duty (Table 4).
Demographics of patients in the Saint John protocol group.
There were no statistical differences between the two groups in terms of the following: age (P = 0.728); gender (P = 0.758); zone of involvement (P = 0.758); degree of flexor rupture (P = 0.299); association nerve injuries (P = 0.051); and injury on duty (P = 0.206).
Range of movement
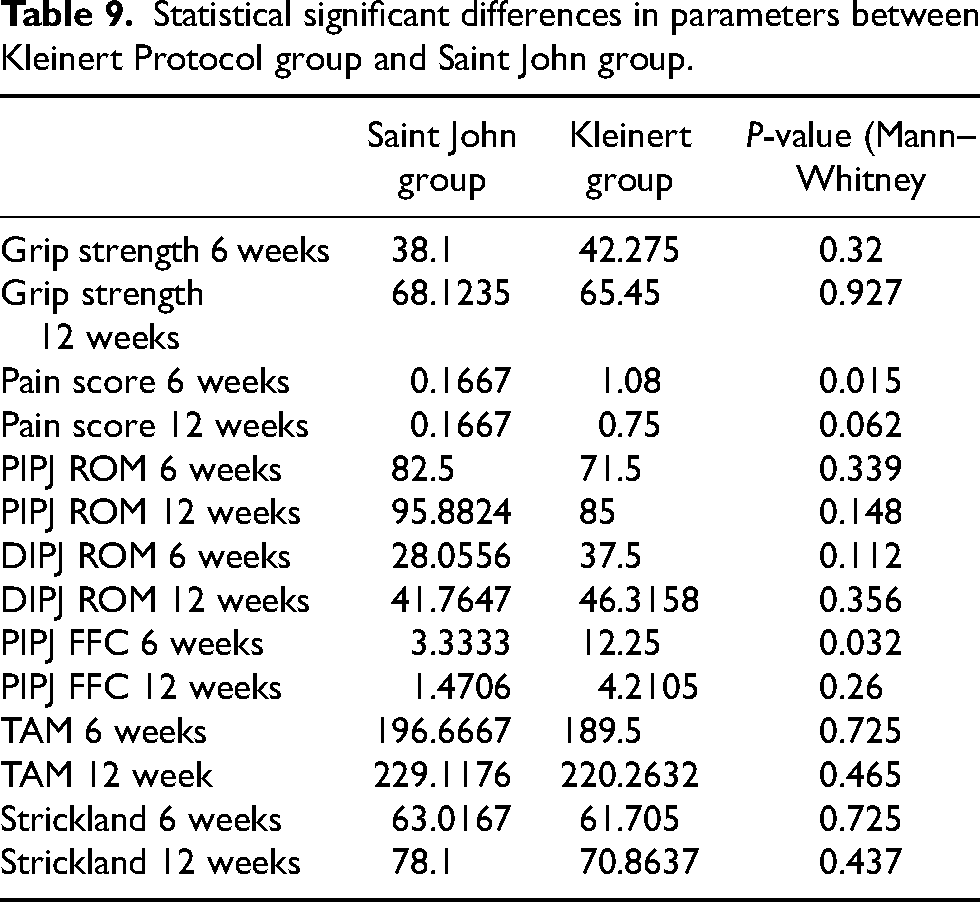
At 6 weeks after surgery, the patients who were managed in the Saint John protocol demonstrated a better ROM of the PIP joint, but it was not statistically significant (82.5 vs 71.5, P = 0.339). There was a statistically significant less severe PIPJ flexion contracture (3.33 vs 12.25, P = 0.032) than patients who used the Kleinert protocol.
At the same time interval, patients in the Saint John group showed better total active movement (196.7 vs 189.5, P = 0.725) and Strickland hand score (63.0 vs 61.7, P = 0.725), although the differences were not statistically significant.
At 12 weeks postoperatively, patients in Saint John protocol showed a better ROM in the PIP joint (95.9 vs 85, P = 0.148), but such difference was not statistically significant. Although the difference was not statistically significant, it was noticed that there was less flexion contracture over the PIPJ (1.47 vs 4.21, P = 0.26) compared with those managed with the conventional Kleinert protocol.
Similarly, patients in the Saint John group continued to demonstrate better results in terms of the total active movement (229 vs 220, P = 0.465) and Strickland hand score (78.1 vs 70.9, P = 0.437), with the differences being not statistically significant.
As for the DIP joint, Saint John group demonstrated inferior results in terms of ROM in both 6 week (28.1 vs 37.5, P = 0.112) and 12 week time (41.8 vs 46.3, P = 0.356) postoperatively, but the results were not statistically significant.
Pain
The pain score at 6 weeks (0.167 vs 1.08) and 12 weeks (0.167 vs 0.75) showed a better result in Saint John Protocol, with the difference in 6 week time being statistically significant (P = 0.032).
Grip strength
Regarding the grip strength of patients after undergoing rehabilitation for 12 weeks, Saint John group demonstrated superior grip strength in comparison with the unaffected side, but the difference was not statistically significant (Saint John: 68.1% of the contralateral side; Kleinert: 65.5% of contralateral side; P = 0.628).
Re-rupture
There was one rupture in the Saint John group and one rupture in the Kleinert group and there were no significant differences between the groups. The ruptures for the patient in the Saint John group occurred at week 6. In the Kleinert group, the patient had the re-rupture at 7 week time. No identifiable cause was found for both of the cases.
Functional outcomes
To assess the functional outcome of the patient, the time required for each group of patient to return to work was documented. For the Kleinert group, 25% of the patients were manual worker, while in the Saint John group, 20% of the patients were manual worker. The proportion of manual workers in each group were comparable. Students and retired individuals were excluded in both groups for the comparison.
It was found that patients in the Saint John group were able to work earlier compared with the counterparts in the Kleinert group (51 vs 115 days, P = 0.03357), and the difference was statistically significant. Two patients in the Kleinert group were not able to return to work after the injury, and all injuries workers in the Saint John group were able to return to duty.
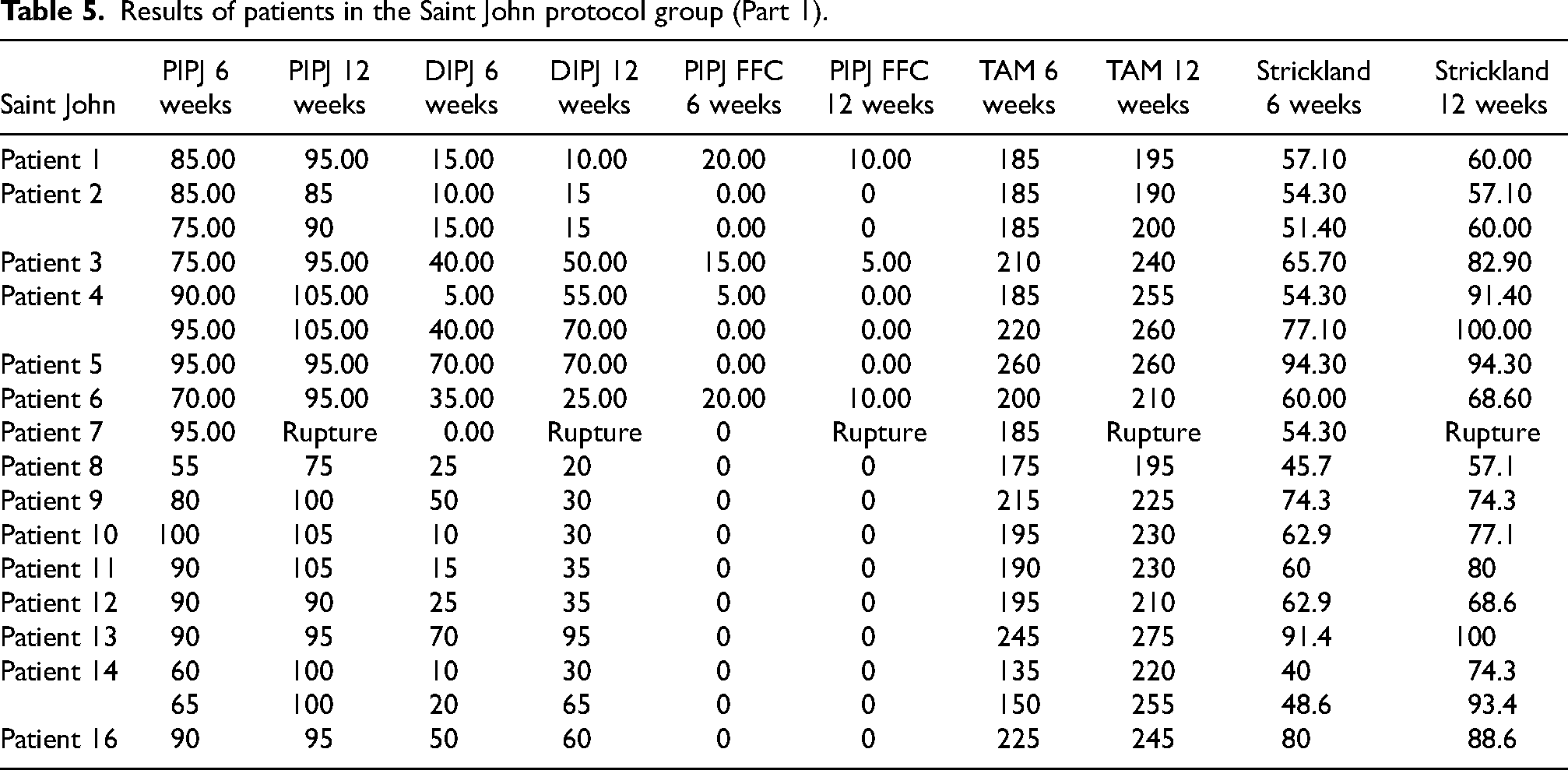
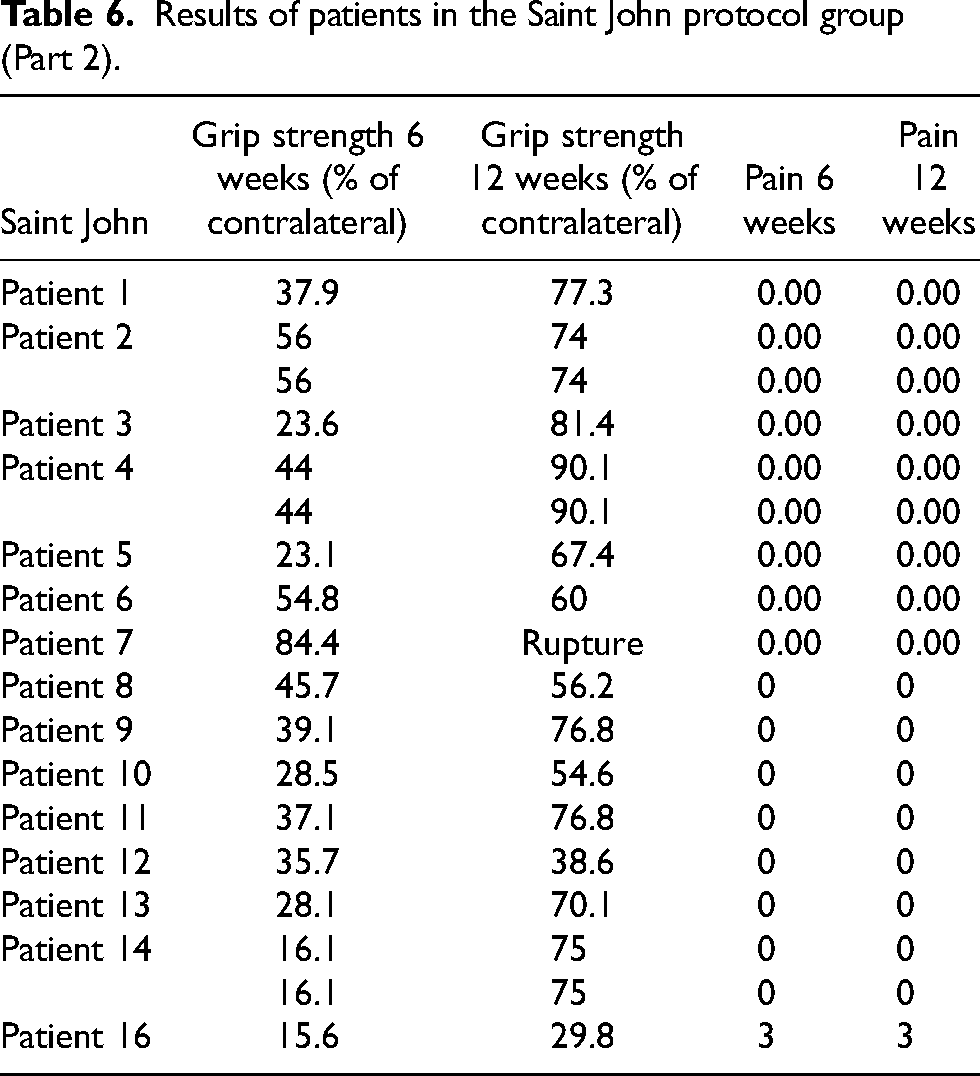
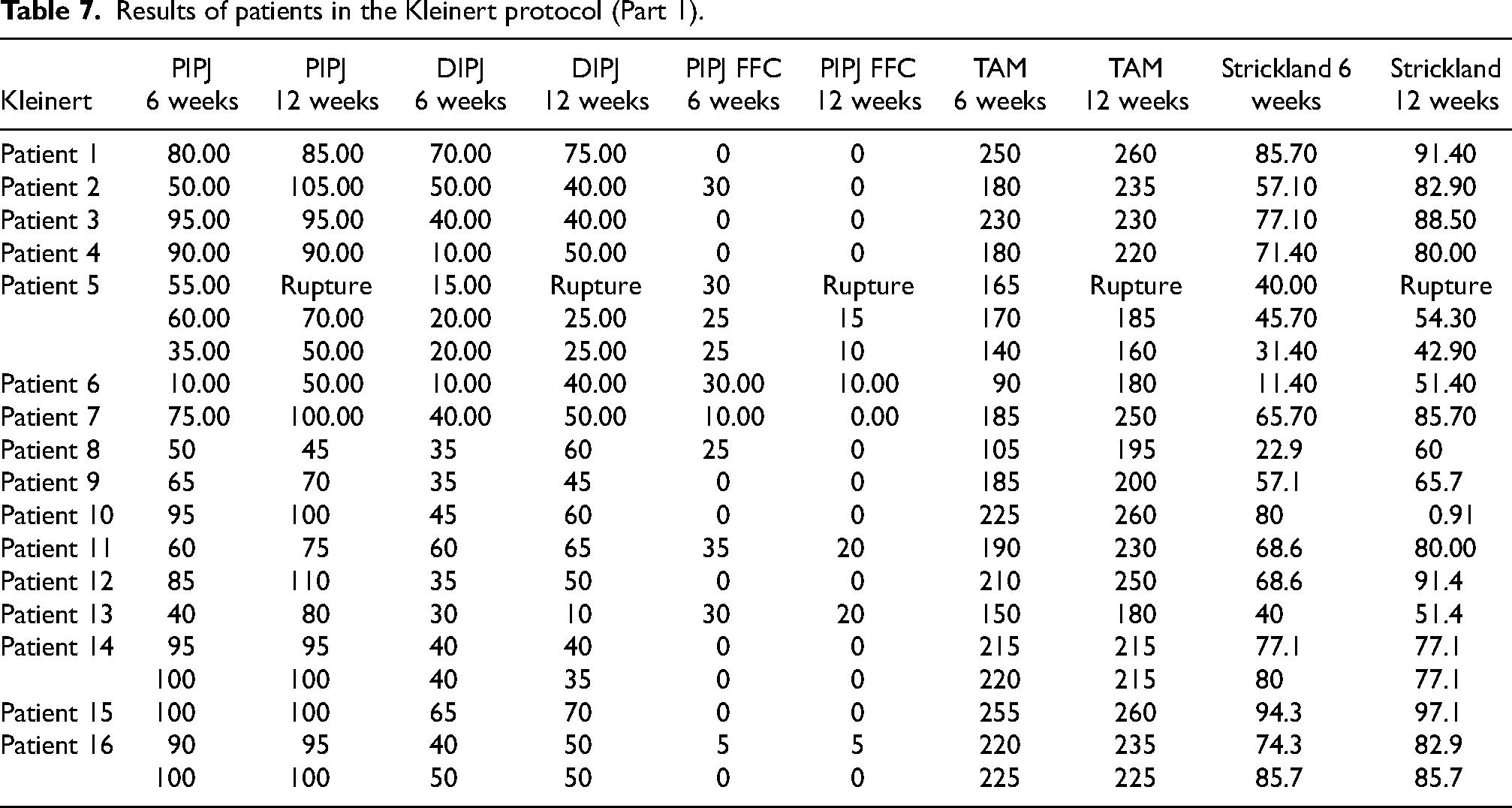
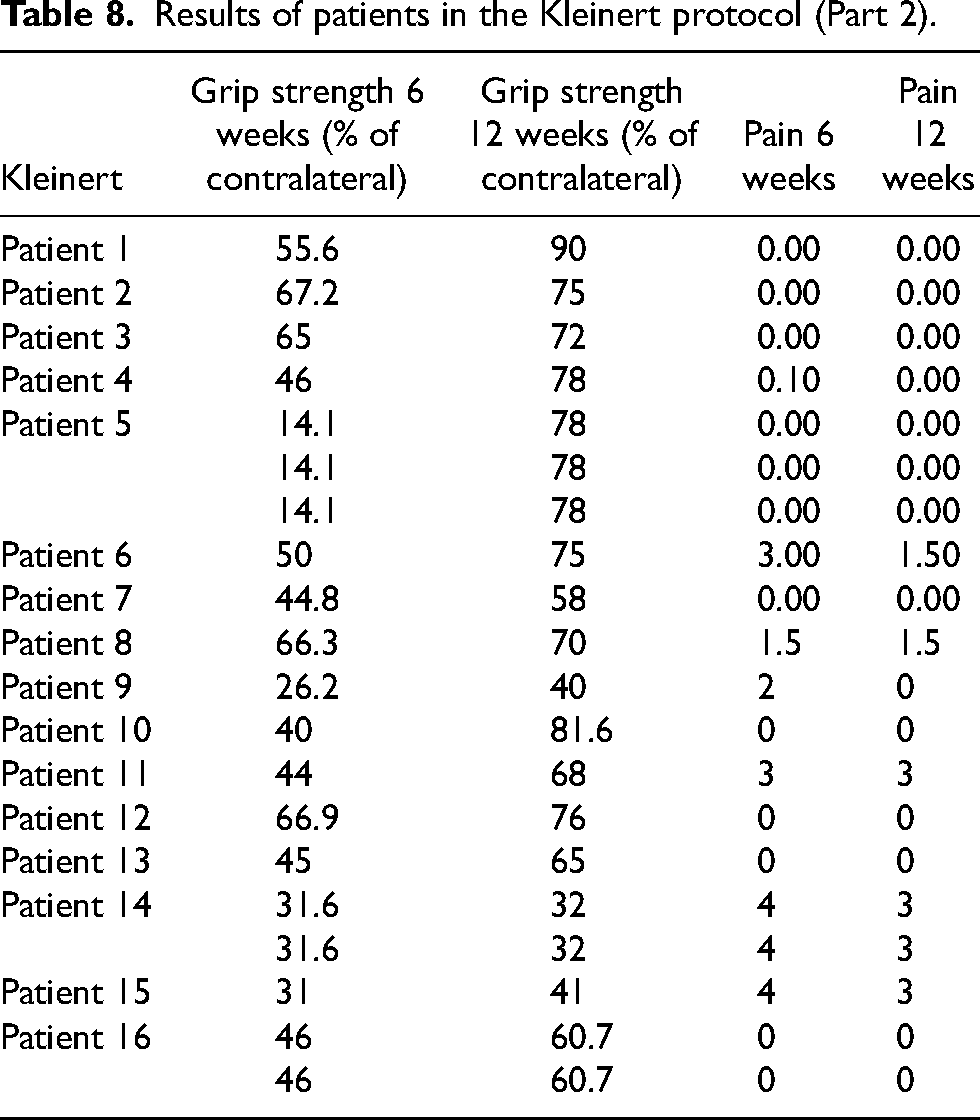
Detail results of flexor tendon repair rehabilitation in the two groups were charted in Tables 5 to 8.
Results of patients in the Saint John protocol group (Part 1).
Results of patients in the Saint John protocol group (Part 2).
Statistical differences in various parameters were summarized in Table 9.
Results of patients in the Kleinert protocol (Part 1).
Discussion
There has always been a debate with regard to the postoperative rehabilitation protocol for Zone I/II flexor tendon injuries. Initially, immobilization protocols were advocated. Nonetheless, poor results followed these programs. 13 Because of the poor results, other rehabilitation protocols were developed. Duran 4 reported the protocol which consisted of controlled passive motion to allow a certain degree of tendon excursion in order to decrease restrictive adhesions. Kleinert proposed his method based on active extension and passive flexion controlled by an elastic band. This protocol has been widely adopted and gained popularity due to the improved clinical results.
With advances in surgical repair techniques and better suture materials, the more secure tendon repair prompted surgeons to consider the idea of early active mobilization. In theory, early active mobilization could achieve better tensile strength, as well as better tendon gliding, hence fewer adhesions and leading to improved digit motion.
One of the earlier reports of early active motion protocol was the Belfast protocol, published by Small in 1989. 7 In the original article, a POP splint fitted with the wrist in flexion was used, and gradual increase in active flexion ROM of PIP and DIP joints within the splint were commenced. In the study, it showed that controlled early active motion can be successfully applied without an increase in the rupture rates while demonstrating favorable outcomes.
Another well-known early active mobilization protocol was the Indiana Protocol suggested by Strickland 14 in which a tenodesis hinge splint is utilized. The affected fingers are passively flexed while the wrist is extended. The patient then actively holds the flexed position for 5 s. The wrist is then flexed to extend the fingers as a tenodesis effect. This protocol is also well known as the “place and hold” protocol. It postulated that by such movement, one could achieve greater tendon excursion.
Peck et al. in 2014 advocated the use the Manchester short splint. This protocol is based on the idea that with the wrist in extension, the work of finger flexion can be minimized. Also if the wrist is allowed to move, there is increased passive flexor tendon excursion during wrist tenodesis. Their results of using the Manchester short splint demonstrates improved outcomes whilst preserving repair integrity.
Later Higgins and Lalonde 12 proposed the use of the Saint John protocol. This protocol allows the patient to perform active finger flexion within a forearm-based splint that places the wrist in extension for the first 2 weeks. They found that with the wrist extended and MCP joint flexed, there is the least tension in the flexor tendon, and hence it can optimize tendon relaxation during immobilization after flexor tendon repairs. After 2 weeks, a short Manchester splint is used and this facilitates the synergistic motion of wrist extension and finger flexion to further promote tendon excursions.
Despite the evolution of these flexor tendon protocols, however, in our locality, the Kleinert regimen remains the protocol of choice in many institutes due to its well established efficiency and acceptable rupture rate.
However, from our experience, the Kleinert protocol carries certain drawbacks, including the risk of joint flexion contracture and the complicated design of the splint. The risk of flexion contracture of the interphangeal joint has been documented in previous studies. Small et al. 7 suggested that the Kleinert splintage results in an increased risk to flexion contracture of the PIP joints due to the prolonged flexion of the digits in traction by the elastic band. Such flexion resting position of PIP joint leads to the contracture of the volar plate and loss of PIP joint extension. Moreover, the extension of fingers is totally dependent on the patients’ motivation and compliance to the regime, hence increasing the risk of such deformity, especially in the early postoperative period which there would be significant pain, swelling, and stiffness. Another drawback of the Kleinert splint is the complexity in fabricating the splint. It is also less comfortable for the patient to put on. Also the Kleinert splints may require more supervision, training from the therapist, as well as good understanding and patient compliance for the optimal result.
In view of the above mentioned drawbacks, the newer Saint John protocol has been introduced for use in our institute since November 2021. At the time of the writing of this article, there has been no publication on direct comparison between Kleinert splintage and the newer Saint John Protocol. Therefore, we thought it would be worthwhile to do a comparative study with this new cohort using the Saint John protocol with a historical control group that used the Kleinert protocol.
In comparison to the Kleinert protocol, a notable divergence observed in the Saint John protocol pertained to the utilization of two distinct types of splints. This divergence stemmed from the rationale that the forearm splint, employed during the initial 2 weeks, facilitated a more comfortable posture in the early postoperative phase, while concurrently enabling early finger mobilization to achieve optimal excursion of the repaired tendon. Subsequently, as the tendon progressively underwent healing beyond the initial 2-week period, the short arm Manchester splint was employed instead. This particular splint facilitated synergistic motion, involving wrist extension and finger flexion, thereby permitting a greater extent of tendon excursion.
The apparent smaller number of cases recruited for the Kleinert protocol arm was due to the fact that some of the cases were excluded due to incomplete documentation or those did not attend physiotherapy and occupational therapy more than 3 months. However, it was important to note that only cases that completed a minimum of 3 months of follow-up with comprehensive assessments were included in the study. No cases were excluded due to selection bias. Another noteworthy point was that we successfully recruited a comparable number of patients for the Saint John protocol within a shorter timeframe. This achievement could be attributed to our proactive approach of contacting patients who had missed a follow-up appointment, effectively reducing the rate of defaults.
There are several advantages of the Saint John protocol over the conventional Kleinert protocol as shown in our study. One of the most important advantages was less fixed flexion contracture over the PIP joint. This was also shown in previous study by Small et al. 7 It could be explained that when one is undergoing the Saint John protocol, the PIPJ and DIPJ were resting in extension instead of a flexed position in the case of the Kleinert splinting due to the traction of the elastic band. As a result, the IP joints were not subjected to constant flexion during resting. Hence they would be less likely to develop fixed flexion contracture as the tendon heals.
Moreover, the total active motion at 12 weeks in the Saint John group was superior compared to the Kleinert group (229° vs 220°). However, the results are not statistically significant.
Another advantage of the Saint John protocol from our study is that there is much less pain in the early postoperative period up to 6 weeks. This might be related to the less complicated design of the splint and the hand and fingers are positioned in a more physiological and functional position.
Another major superiority of the Saint John protocol was faster return to work. It could be explained by the fact that the patients experienced less pain, better ROM and less complicated rehabilitation protocol. As a result, patients would be more motivated to participate in the journey of recovery, and later feeling more confident to return to work.
The clinical outcomes of the Saint John protocol in our study were slightly better than other protocols published in previous studies in terms of total active motion (Table 10).
Results of patients in the Kleinert protocol (Part 2).
Statistical significant differences in parameters between Kleinert Protocol group and Saint John group.
Clinical outcomes of previous studies comparing different flexor tendon rehabilitation protocol for zone I/II flexor tendon repair.
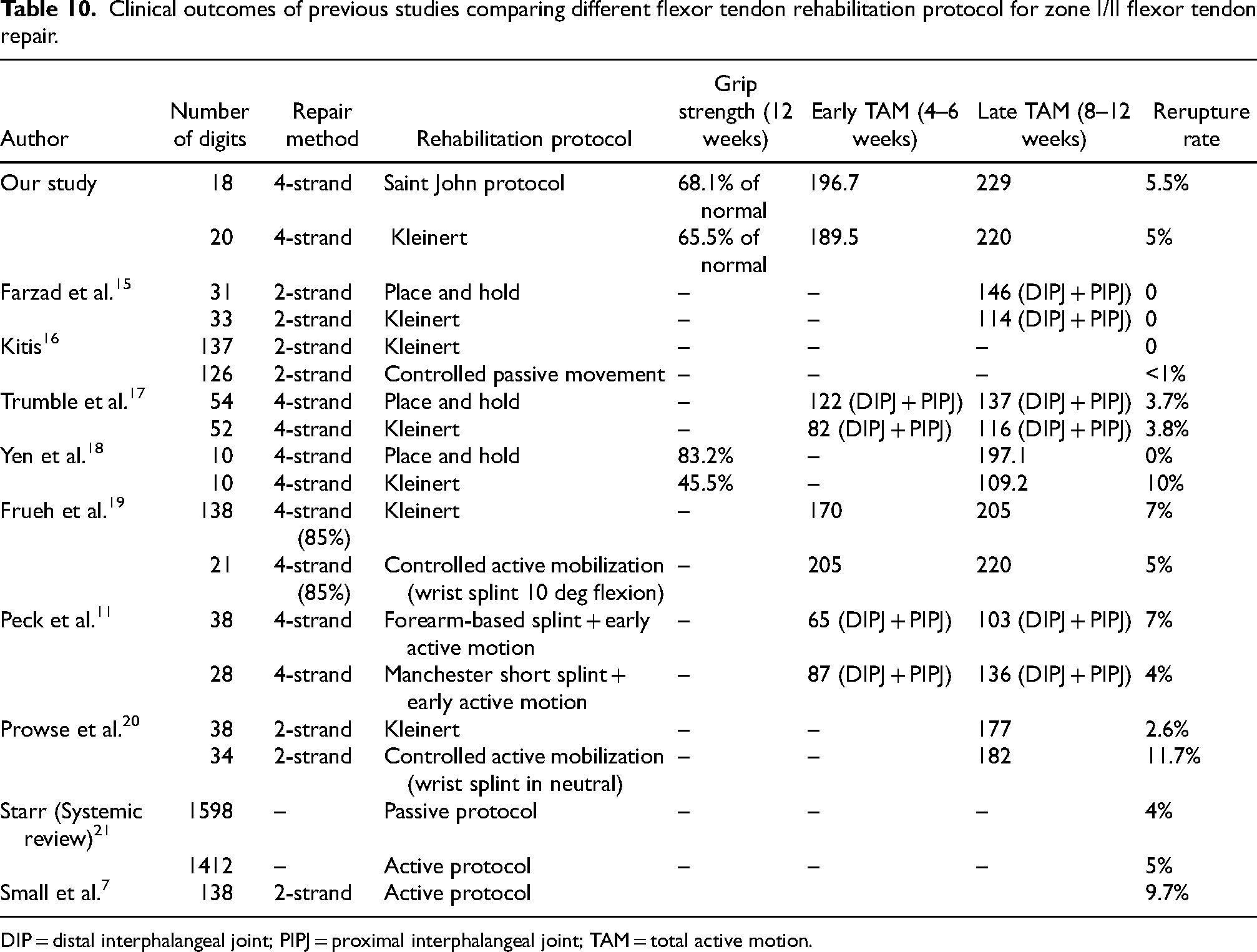
DIP = distal interphalangeal joint; PIPJ = proximal interphalangeal joint; TAM = total active motion.
Concerning the safety of the Saint John protocol, the flexor tendon rerupture rate was 5% in our study, which was comparable to the published ruptures rate of various studies ranging from 0 to 11.7% associated with early active motion rehabilitation protocols (Table 10). Hence this protocol did not sacrifice tendon integrity for better clinical outcomes. We believe that a four-strand repair with proper tension is adequate in preserving the integrity of the repaired tendon.
However, it is important to acknowledge certain limitations associated with the Saint John protocol. Firstly, patients in the Saint John group are required to possess a higher level of education and compliance in order to fully leverage the benefits of this more advanced protocol, in contrast to the traditional Kleinert protocol. Additionally, the warm-up exercises in the Saint John protocol involve passive movement of the injured finger using the contralateral hand. Consequently, patients with bilateral injuries may encounter challenges in adhering to the Saint John protocol.
Limitations
This study has a few limitations. Firstly, it is a retrospective study, which may have introduced selection bias. Secondly, the surgery was performed by different surgeons. However, the repair technique was unified with four-strand core sutures. Thirdly, differences in patient compliance and motivation with the rehabilitation regime cannot be controlled, which might affect the clinical outcomes. Additionally, the sample size was relatively small, which may have limited the statistical power to detect significant differences in some outcomes. Further studies with larger sample sizes and prospective designs are needed to confirm these findings.
Conclusion
We compared the outcomes of patients with uncomplicated Zone I/II flexor tendon repairs who had been rehabilitated using either the Kleinert or the Saint John protocol. From our findings, the Saint John protocol demonstrated noninferior result compared with the well-established Kleinert protocol. The Saint John protocol showed potential advantages including: (a) less pain at 6 week, (b) less flexion contracture at the PIPJ at 6 weeks, and (c) better total active range of motion at 12 weeks (although not statistically significant). Rupture rates between the two groups were similar as well. Lastly, the simplicity of the design of the splint also makes it an attractive option from the therapists’ and patients’ point of view. However, further randomized control trial is warranted to validate these results and determine the long-term effects of the Saint John protocol.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.