
Abstract
What is already known on this topic – Currently, there is no clinically validated return to activity tool following shoulder injury or surgery. Within the literature, rates of return to activity following injury/surgery vary significantly between different populations. The reason for this variation is poorly understood and may be a result of incomplete rehabilitation. The use of performance test batteries has been recently recommended as a tool to assist with return-to-activity decision-making.
What this study adds – Our study reports the reliability and psychometric properties of the first shoulder test battery that is inclusive of a psychosocial measure. The SIT-SAB is congruent with aspects of the 2022 BERN consensus statement on shoulder injuries and may be a useful tool in assisting return-to-activity decisions as it provides normative values for non-injured shoulders.
How this study might affect research, practice or policy – This study will pave the way for clinical validation of the test battery in a return to activity context. The findings from this study will contribute to the existing literature and could guide further investigation.
Background
Shoulder pain is one of the most common musculoskeletal complaints with a lifetime prevalence of up to 70%. 1 It is highly prevalent among athletes and the general population.2–4 It is associated with negative impacts such as absenteeism, productivity loss, impaired health-related quality-of-life and economic burden.4–6 A key goal of rehabilitation following shoulder injury or surgery is the resumption of physical activity or return-to-play (RTP). Return-to-play occurs along with a continuum which consists of three elements: return-to-participation, return-to-sports and return-to-performance. 7 The 2022 Bern consensus statement 8 suggested six domains to be considered for RTP criteria after a shoulder injury. This includes pain; active shoulder joint range of motion (ROM); strength, power and endurance; kinetic chain; psychological readiness; and sport-specific demands. Currently, there is no valid test for informing RTP decisions following a shoulder injury.8–11
In most cases, there is no clear rationale for relying on any test or criterion alone and no evidence to support their effectiveness in isolation. 11 This is due to the complexity of the shoulder and the many factors that can influence an athlete's readiness for RTP. This complexity makes it challenging to develop a single criterion or test that can be applied to all athletes. This is why there is a growing interest in using test batteries for shoulder post-injuries/post-surgeries and is also recommended by the 2022 Bern consensus statement.8,9 Compared to individual tests, a comprehensive test battery gives clinicians a better picture of the individual's physical capabilities as it assesses multiple domains and considers various factors allowing for a more informed and holistic evaluation of patient's readiness for RTP. 8
A battery of tests would provide an objective outcome measure, which would involve using standardised measurements and cut-off values to determine readiness for RTP. This would help to reduce subjectivity in the decision-making process and improve the quality of care for patients with shoulder injuries. Although several individual novel test batteries have been published, such as the Wilson et al. shoulder testing protocol, 12 Popchak et al. testing battery for shoulder 13 and the SARTs battery test, 14 none includes a psychosocial assessment. Furthermore, they have yet to be validated or widely adopted in clinical practice. 8 In addition, most RTP research focuses on elite athletes, limiting the translation of findings to the general population as studies have found differences in outcomes between elite and non-elite athletes after a shoulder injury. 15 Therefore, our Singapore Institute of Technology Shoulder Assessment Battery (SIT-SAB) is a novel RTP assessment for shoulder injury/surgery for the general population. It aims to look at patients holistically and may address the shortcomings of existing tests and help guide clinicians in the RTP decision-making process.
Clinicians need accurate and reliable information to make RTP decisions, which is why it is crucial to establish the psychometric properties of the test battery. 13 While several individual tests’ reliability and concurrent validity have been assessed, it is also essential to establish the reliability and validity of an entire battery of tests. This is because a battery of tests assesses multiple domains of muscular performance and considers the influence of factors such as fatigue and patient attention on the tests’ overall clinical utility and generalisability. It is also important to establish the normative data of the test battery so that clinicians have a reference point to compare patients’ performance. 16 Normative data can also be used to establish cut-off values or ranges of values for various tests that can be used to determine readiness for RTP. These are necessary steps to make the test battery robust and reliable for assessing an athlete's readiness to make an objective RTP decision for patients after shoulder injury/surgery. Hence, the primary aim of this study was to evaluate the intra-day reliability of the SIT-SAB, our novel shoulder battery and scoring system. The secondary aim is to provide normative data on the battery in the non-elite active population. We hypothesised that the battery and scoring system would show good to excellent test–retest reliability (International Consensus Criteria [ICC]- > 0.7–0.9).
Methods
Study design
We used a cross-sectional observational design to collect participants’ data over three weeks in November 2021 at SIT. We assessed participants according to the sequence of the Shoulder Battery Test, which was arranged in the order from least to most fatiguing tests.
Participants
From a convenience sample of college students, we recruited individuals 18 years or older with asymptomatic shoulders and normal shoulder mobility. Participants were excluded if they had a history of shoulder injury or surgery within the past 2 years, a musculoskeletal disorder in the cervical region or upper limb or reported shoulder pain or symptoms within the past 6 months. We gathered demographic and anthropometric information to identify potential risk factors that affect the SIT-SAB score. This includes data on age, gender, height, weight, BMI, dominant arm, history of shoulder injuries, activity level, type of sports and current level of play. To evaluate the inter- and intra-rater reliability of the SIT-SAB, we needed 19 participants to return for two additional sessions to assess test–retest reliability. This number of participants was chosen based on the recommendation of Carter et al., who suggested that a minimum of 19 participants would be needed to achieve an ICC score of 0.7, with a significance level of 0.05 and a power of 80%, for reliability studies involving two examiners.
Singapore Institute of Technology Shoulder Assessment Battery
The SIT-SAB includes six tests arranged in the order of increasing fatigability as follows: Firstly, the Hand-Behind-Back (HBB) test; followed by the Seated Medicine Ball Throw (SMBT) test; the Athletic Shoulder Test (ASHT); the modified Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Questionnaire (KJOC); the Isometric Shoulder External/Internal Rotation Strength (Iso-ER/IR) ratio test; and finally, the Posterior Shoulder Endurance Test (PSET) (Figure 1). Before starting the SIT-SAB, a standardised warm-up was performed involving three movements (Arm circles, Shoulder rolls, Alternating chest hugs) consisting of 10 repetitions each. We established the methodology of each test in the SIT-SAB based on the existing literature, which is summarised in Table 1. Based on each test's contributions to the assessment of shoulder function as determined by the team, as outlined in the brief descriptions below. Each test was given a score out of 15 or 20 (Figure 2), with a maximum total test battery score of 100. The scoring of each test corresponds to the performance on the test together with specific criteria outlined in Table 1.
We selected the HBB method as it is standard for assessing shoulder joint internal active ROM. 17 It is an important functional measure for the shoulder as it is related to activities of daily living (toileting, dressing)17,18 and serves as one of the early signs of shoulder pathology.17,18 Despite concerns about HBB's accuracy due to its susceptibility to various factors such as multiple-joint movement, spinal differences and obesity index, 19 its reliability has been confirmed to be clinically adequate. 20 We selected the SMBT as it is a functional assessment of upper body explosiveness and power that can be conducted on any population.21,22 It also has been demonstrated to have clinically acceptable reliability and a strong correlation to shoulder ER and IR strength. 23 Furthermore, as the throwing biomechanics requires a proximal-to-distal sequence of energy transfer along with the kinetic chain, 24 SMBT can assess the patient's ability to generate power through the kinetic chain. This would provide insights into any inadequate movement strategies adopted by the patient. We selected the ASHT as it is a reliable long-lever isometric strength test replicating shoulder muscle contraction typical to various sport-specific actions and daily functions. 25 It can also effectively assess the higher shear forces experienced by the shoulder, which the short-lever arm test may not adequately capture. 26
We selected the KJOC questionnaire as it can appropriately assess psychological factors. It looks at the perceived shoulder health in relation to activity and the psychological impact on their social well-being. It was also found to have high validity and sensitivity when used as a tool for screening. 27 Furthermore, the KJOC has demonstrated excellent reliability, can discern athletes with shoulder pain and has strong predictive ability. 28 We selected the Iso-ER/IR ratio test as it is a reliable assessment tool for rotator cuff strength and intermuscular balances.29,30 The function of the external and internal rotator muscles is an important factor in shoulder injuries, and a normal strength ratio should be maintained to improve shoulder function. 31 We selected the PSET as it is a test to measure muscular fatigue around the shoulder. Muscular fatigue may alter muscle activation patterns, force couples and kinematics, which is an important factor in shoulder injuries. 32 Furthermore, it is important in repetitive daily movement.
While all components of SIT-SAB have been shown to have clinical utility in making return-to-activity decision-making following a shoulder injury, we have given a higher weightage to HBB and KJOC. The HBB was given a higher weightage as loss of glenohumeral internal rotation has been demonstrated to be a risk factor for injury across a wide variety of sports. 33 A deficit can cause an alteration of joint kinematics making optimal internal rotation range an important determinant of shoulder functionality. 34 The KJOC was given a higher weightage as it is the only patient-reported outcome measure and negative psychological factors are associated with worse patient outcomes. 35 Higher levels of pain catastrophising have been shown to adversely impact the benefits derived from progressing in rehabilitative exercises, 36 making it a critical factor influencing the success of rehabilitation.
Statistical methods
Our primary outcome measure was the SIT-SAB's inter-rater, intra-rater and inter-day reliability. We compared the scores obtained between two different testers to test for inter-rater reliability. This was done using two examiners’ mean rating (k = 2) with a two-way random-effects ICC model. To test for intra-rater reliability, we compared the scores obtained by the same tester on a separate day. This was done using the absolute agreement with a two-way mixed-effects ICC model. Test–retest reliability was obtained by comparing the scores obtained across all 3 days. After calculating the ICC coefficients and the 95% confidence interval, we then classify the reliability of the battery into poor, moderate, good or excellent, corresponding with a value that is less than 0.5, between 0.5 and 0.75, between 0.75 and 0.9 and above 0.9, respectively. 37 We also looked for any possible risk factors that could affect the SIT-SAB score by comparing demographic and anthropometric parameters to the score of the battery. A paired t-test, Mann–Whitney U test and the Kruskal–Wallis H test were used to compare data that were normally distributed, non-normally distributed or had three or more categorical variables, respectively. Pearson's and Spearman's correlation coefficients were also used to evaluate the relationship between linear and ordinal variables. An alpha level of 0.05 was used to define statistical significance. Analyses were performed using SPSS statistical software (V.22.0, SPSS).
Results
Participants
One hundred and four participants were recruited for the study, and 19 returned for two additional trials. The participants had a mean age of 25.1 ± 4.4 years, and 91.3% (n = 95) were right-arm dominant. A total of 11 participants reported having a history of shoulder injury (more than 2 years history). The other demographic and anthropometric characteristics of the participants are shown in Table 2.
Singapore Institute of Technology Shoulder Assessment Battery
The mean score for the SIT-SAB is 87.3 ± 10.3 out of a maximum possible score of 100. The results of the descriptive statistical analysis of the SIT-SAB score are shown in Table 3. We found no statistically significant correlation to other demographic, anthropometric characteristics or other factors. Kruskal–Wallis H test showed no statistically significant difference in the SIT-SAB score between the sub-groups (p > 0.05). The test–retest reliability of the SIT-SAB score over three trials was excellent, with an ICC value of 0.89 [0.78, 0.96]. It also demonstrated good inter-rater reliability and intra-rater reliability with an ICC value of 0.81 [0.78, 0.93] and 0.97 [0.92, 0.99].
Discussion
We evaluated the intra-rater, inter-rater and inter-day reliability of our novel SIT-SAB and scoring system and found a good to excellent test–retest reliability. Both individual tests and the battery scoring system demonstrate good psychometric properties, which shows that this battery allows clinicians to obtain accurate information reliably. The normative values have also been established to give clinicians a reference point to compare patient performance. Therefore, we have demonstrated that this novel shoulder battery test is reliable for assessing an athlete's readiness to make an objective RTP decision for patients after shoulder injury/surgery.
In our SIT-SAB, we selected tests based on their ability to comprehensively evaluate patients’ shoulder function. Although the SIT-SAB was created prior to the publication of the Bern 2022 consensus statement, 8 it addressed the six domains of consideration for RTP outlined in the consensus statement (Table 4). This includes the psychosocial assessment many existing batteries lack. Whilst existing shoulder rehabilitation protocols focus on decreasing pain, working with kinetic chain and restoring ROM, strength, power and endurance, they lack specific interventions that address psychological readiness and sports-specific performance. This could be attributed to the need for such criteria to be used in RTP assessment. It has been established that psychological response is an important factor in the successful RTP.38,39 However, no specific protocol exists in the literature that addresses psychological readiness. Nonetheless, psychological readiness should be an important consideration during rehabilitation. Clinicians can utilise strategies such as positive self-talk, cognitive restructuring, goal setting, relaxation, guided imagery and creating a supportive environment to promote positive psychological responses. 40
Clinical implication
Return-to-play occurs along with a continuum involving progressive flow through three phases (return-to-participation, return-to-sports and return-to-performance), emphasising graded, criterion-based decision-making for progression. 7 Several published theoretical frameworks aid with RTP decision-making by establishing the various factors of RTP to promote consistency and transparency. 41 The most recognised framework, Strategic Assessment of Risk and Risk Tolerance (StAART), 42 involves a three-tiered decision-making process. However, there is little evidence regarding the physical RTP criteria. 43 Although the Bern 2022 consensus statement recommended six domains of consideration for RTP, 8 time is the most used criterion and is often used alone even though it is insufficient.9–11 Other criteria include strength, ROM, pain and sports-specific testing, although most were subjective in nature. 9 There is no protocol that uses criteria that look at the six domains, 8 which poses a challenge to clinicians making RTP decisions due to insufficient information. This could lead to premature RTP, which risks re-injury or a delayed RTP that will cost resources and impact performance. The SIT-SAB may represent a potential solution to standardise the quality of information available to clinicians during the RTP decision-making process and overcome the inadequate information clinicians use for RTP decision-making.
The SIT-SAB overcomes these limitations in several ways. Firstly, results from this study show that the SIT-SAB is a reliable objective measure that different care team members can use. Secondly, the normative data established from this study can be used as a criterion for progression to start patients on the RTP continuum. This also provides objectivity to the criteria for RTP compared to traditional methods. Finally, the SIT-SAB assess the six domains of consideration, providing comprehensive information for clinicians to make better RTP decisions. Strategies used throughout the three RTP phases are highly interrelated due to the interrelationship between rehabilitation and RTP. 43
Overall, clinicians may utilise the SIT-SAB to assess patients who have completed a shoulder rehabilitation program to determine their readiness to progress through the three phases of RTP. The SIT-SAB can be used as a criterion for starting them on the RTP phase. In cases where patients do not achieve a score above the normative value, the SIT-SAB enables clinicians to identify functional limitations that require further attention and adjust the patient's program accordingly. After completing the adjusted rehabilitation protocol, patients may attempt the SIT-SAB test again to evaluate their progress and determine their suitability for RTP. Consequently, the test can be used to monitor patients’ progress throughout the rehabilitation process, reassess the patient's condition and be used to individualise patients’ rehabilitation programs based on their needs.
Limitations
The limitations of this study should be noted. Firstly, while the intent of our SIT-SAB is for the patient with a significant history of post-shoulder injury/surgery, the current study looked at a group of relatively healthy young adults who do not present with shoulder pathology or dysfunction. Therefore, the result of this study only demonstrates the reliability of SIT-SAB as a test and future studies are required to examine the validity of SIT-SAB in the patient population. Cut-off score and minimal clinically important difference (MCID) should also be established to help clinicians make sense of collected data and track significant progress.44,45 Secondly, as most patients experience unilateral shoulder pathology, clinicians may find that SMBT may not be as relevant as a bilateral functional performance test. Although unilateral tests like the seated single-arm shot-put test might be more appropriate, SMBT allows us to assess the patient's ability to develop overall upper body power and coordination. Clinicians can identify any potential compensatory muscle activation pattern by studying the movement along the kinetic chain. Moreover, as a part of a test battery, other tests such as ASHT, ER/IR and PSET have already assessed the arm individually. Therefore, SMBT can provide valuable information regarding the patient's overall function as part of a comprehensive battery of tests. Finally, while we have established normative data for SIT-SAB in the healthy young adult population, it might not reflect other populations such as the adolescent, elderly or elite athlete population. Further studies looking at specific populations will be needed to ensure the robustness of our novel test battery.
Conclusion
The SIT-SAB is a novel test battery that can be used to assess a patient's physical status after a shoulder injury/surgery. The SIT-SAB demonstrated good inter-rater, intra-rater and inter-day reliability and has a normative value of 87 in the healthy adult population. Following further research, the SIT-SAB has the potential to inform clinicians in guiding RTP decisions. It assesses the domains for RTP criteria after a shoulder injury as suggested by the Bern 2022 consensus statement. 8 This study confirms the reliability of SIT-SAB as a test battery. We have also established the normative data to provide a reference point for clinicians to compare their patient's performance. Further studies looking at the validity, MCID and a cut-off point would be needed to increase the value of our novel test battery.
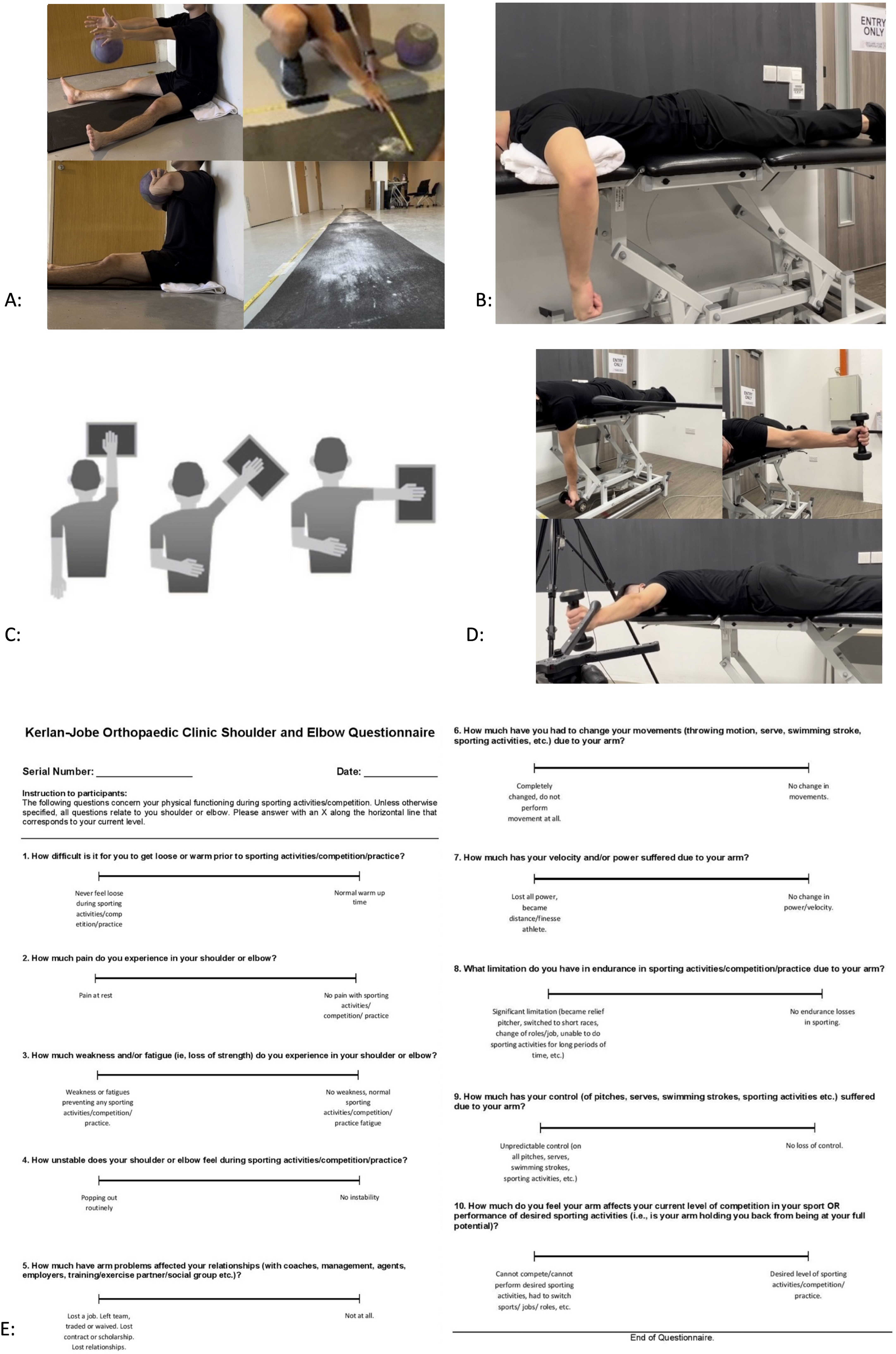
(a) Seated medicine ball throw, (b) ER/IR ratio, (c) ASH, (d) PSET and (e) KJOC.
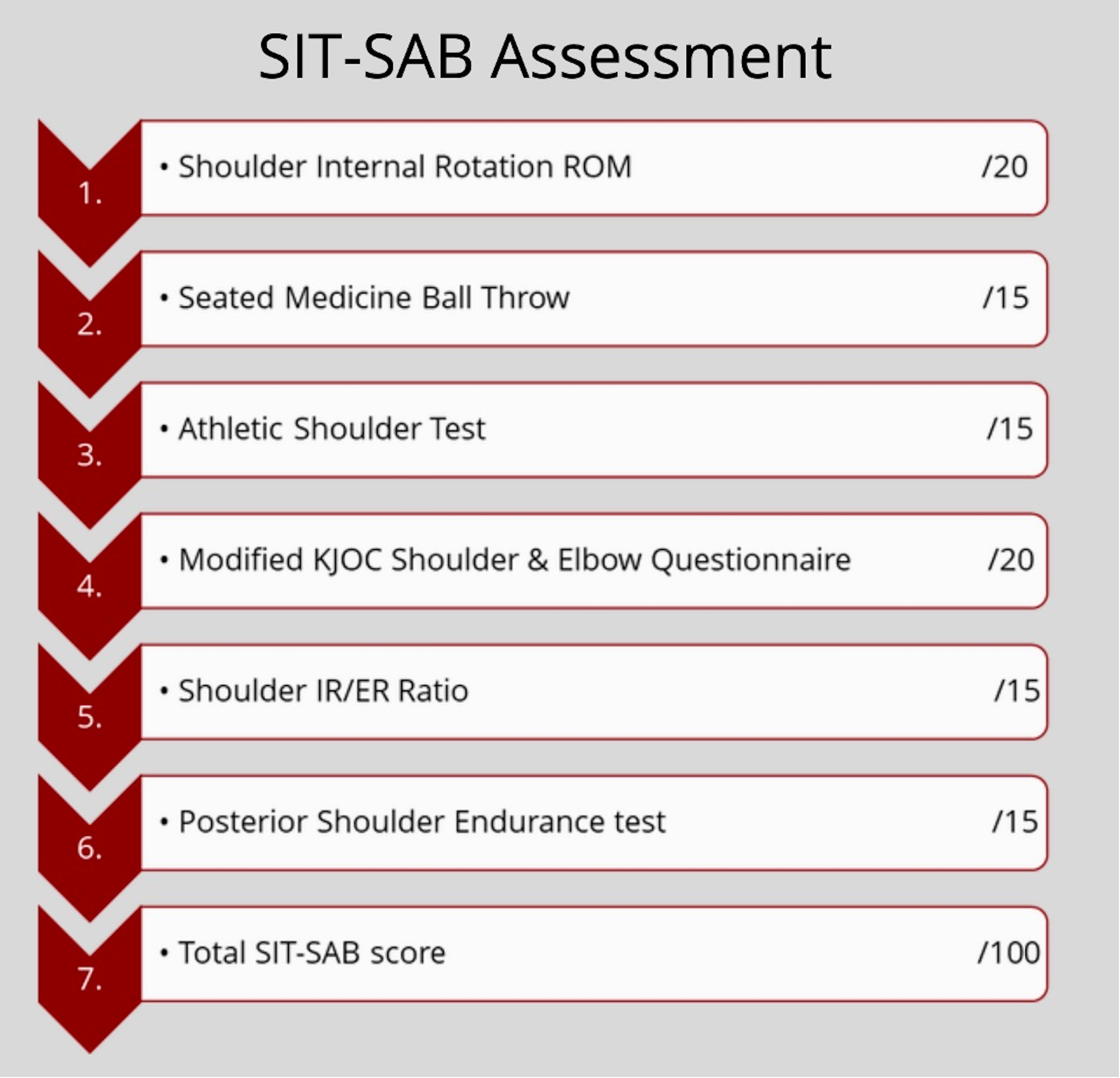
SIT-SAB outline and individual test’s contribution to the assessment.
The procedures of the different test included in the SIT-SAB.
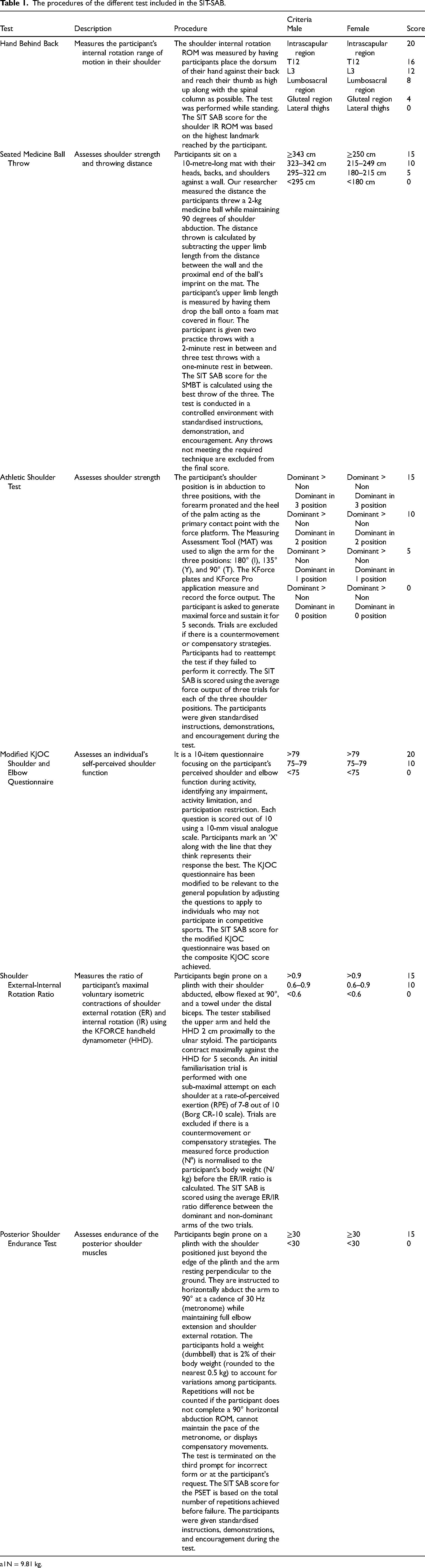
1N = 9.81 kg.
Descriptive characteristic of participants, mean ± SD or N (%).
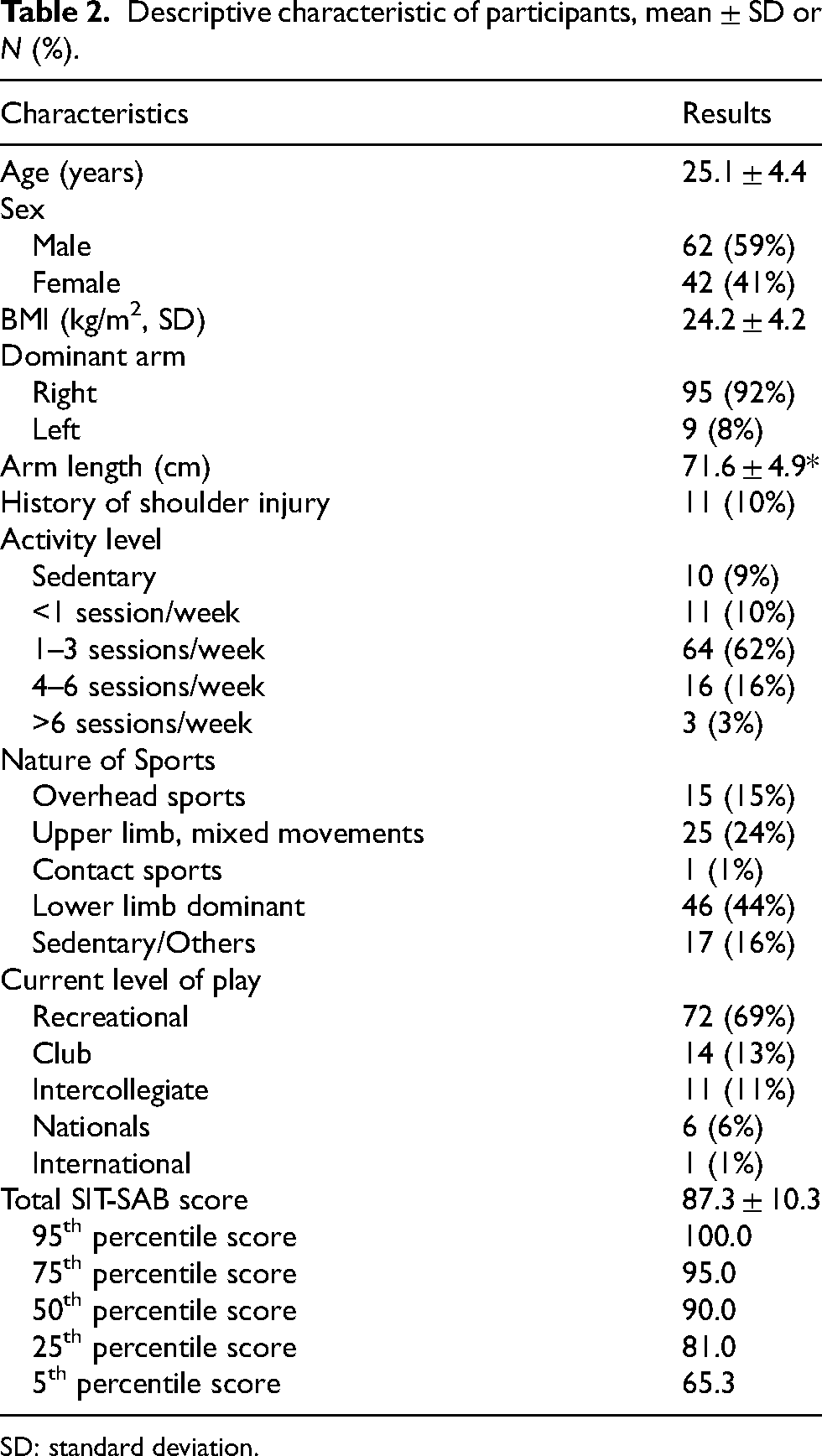
SD: standard deviation.
Descriptive characteristic of the SIT-SAB results, mean ± SD or N (%).
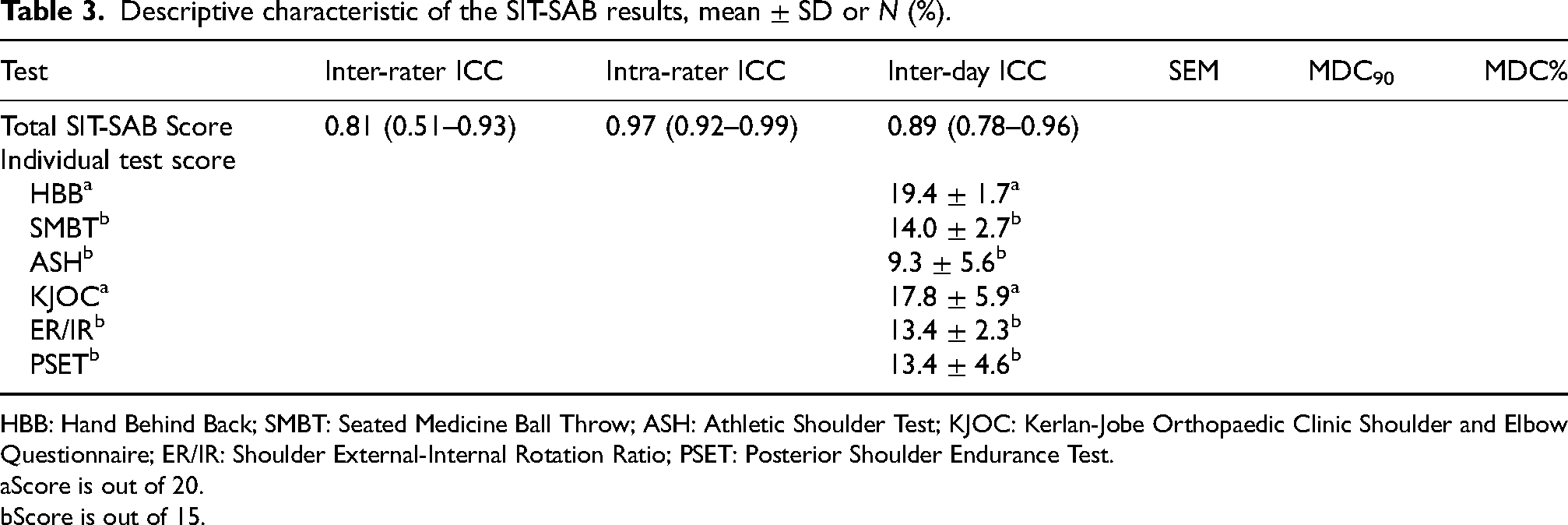
HBB: Hand Behind Back; SMBT: Seated Medicine Ball Throw; ASH: Athletic Shoulder Test; KJOC: Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Questionnaire; ER/IR: Shoulder External-Internal Rotation Ratio; PSET: Posterior Shoulder Endurance Test.
Score is out of 20.
Score is out of 15.
Comparison of the six domains of consideration as suggested by the Bern 2022 Consensus Statement and the tests included in the SIT-SAB.
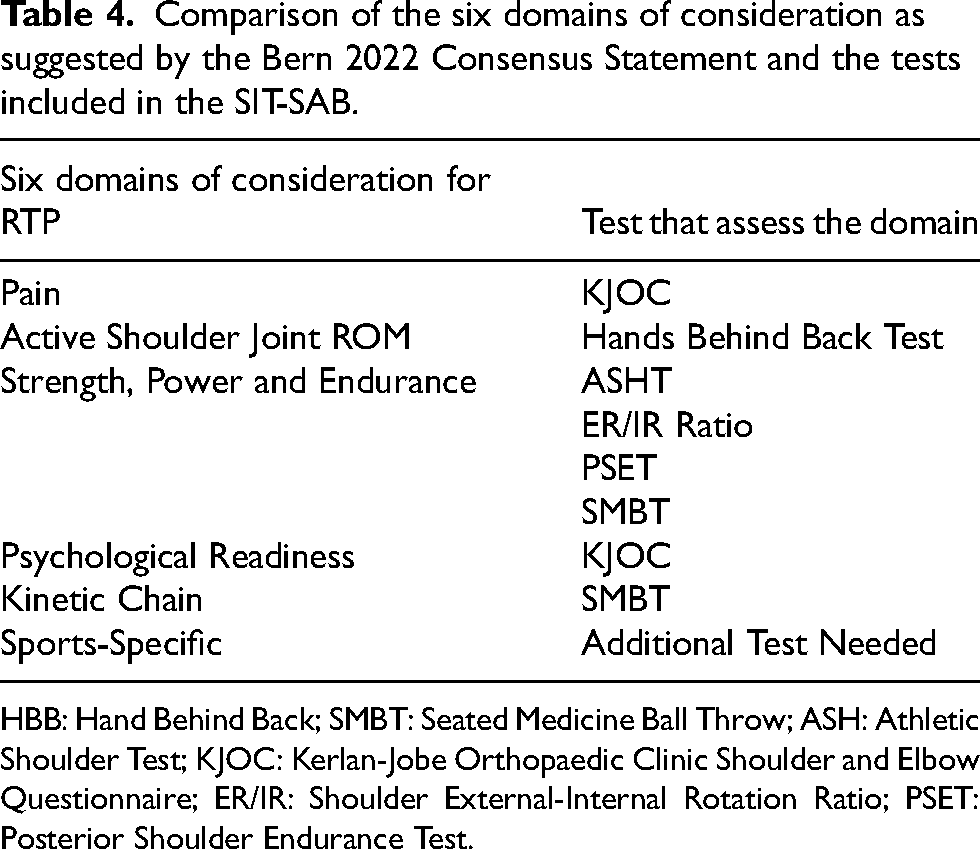
HBB: Hand Behind Back; SMBT: Seated Medicine Ball Throw; ASH: Athletic Shoulder Test; KJOC: Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Questionnaire; ER/IR: Shoulder External-Internal Rotation Ratio; PSET: Posterior Shoulder Endurance Test.
Supplemental Material
sj-pdf-1-otr-10.1177_22104917231225969 - Supplemental material for A novel return-to-play battery for shoulder injury/surgery: Normative values and psychometric properties
Supplemental material, sj-pdf-1-otr-10.1177_22104917231225969 for A novel return-to-play battery for shoulder injury/surgery: Normative values and psychometric properties by Kieron Phillips, Jun Xiang Ng, Tarek Abdelkader and Alex Wirianski in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Contributorship
Phillips K. was the lead contributor to this study through conception, design and data collection. Phillips K. and Ng J. X. contributed to the data analysis and drafting of this article. Wirianski A. and Abdelkader T. contributed to the structure design, supervision, provided resources and revised the manuscript. Wirianski A and Phillip K. contributed to the critical revision for important intellectual content. The authors read and approved the final manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Approved by the ethics committee of the Singapore Institute of Technology, project number 2021055.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.