
Abstract
Purpose:
Rotator cuff tears (RCTs) occur commonly, especially among certain groups of individuals. In this meta-analysis, we aim to identify risk factors for RCTs.
Methods:
We searched MEDLINE for 210 articles. Seventeen articles were selected for systematic review, of which 10 were eligible for meta-analysis. Data was analysed with Review Manager 5.3, using Mantel–Haenszel statistics and random effect models.
Results:
A total of 6653 individuals were analysed. The odds of sustaining a RCT on the dominant hand was 2.30 times more than the non-dominant hand (95% confidence interval (CI): 1.01–5.25, Z = 1.99, p = 0.05; Heterogenity: τ 2 = 0.38, χ 2 = 8.84, df = 2 (p = 0.01), I 2 = 77%). The odds of an individual aged 60 years and above sustaining a RCT was 5.07 times higher than an individual less than 60 years old (95% CI: 2.45–10.51, Z = 4.37, p < 0.001; Heterogenity: τ 2 = 0.47, χ 2 = 25.24, df = 3 (p < 0.001), I 2 = 88%). Female gender was not a significant association, with an odds ratio of 0.98 when compared to the male gender (95% CI: 0.66–1.45, Z = 0.09, p = 0.93; Heterogenity: τ 2 = 0.20, χ 2 = 44.24, df = 5 (p < 0.001), I 2 = 89%).
Conclusions:
Hand dominance and older age are associated with RCTs. More studies are required for further assessment of associations and risk factors of RCTs.
Keywords
Introduction
Rotator cuff tears (RCTs) are one of the more frequent pathologies within the shoulder girdle. 1 A significant number of such tears are asymptomatic. At any given time, the prevalence of asymptomatic RCTs is greater than that of symptomatic RCTs. 2 Many RCTs also cause restriction of shoulder function. 3 Epidemiologically, their prevalence increases with age, with 54% of asymptomatic patients aged 60 years and greater having sustained either a partial or complete RCT on magnetic resonance imaging. 4 Ultrasound (US) studies by Tempelhof et al. reveal that 13% of individuals in their fifth decade, 20% in their sixth decade and 31% in their seventh decade of life have RCTs. 5 From their study on 306 cadavers, Löhr and Uhthoff noted a 19% and 32% prevalence of full and partial thickness tears, respectively. 6 As the prevalence of RCTs is high within the general population, it is imperative to define risks and associations related to RCTs in the general population.
There have been various factors described to be associated with RCTs. The objective of this study is to synthesize the published literature regarding associations with RCTs in the form of a systematic review and meta-analysis. Where possible, we aimed to identify quantified overall estimates for associations with RCTs. This would provide an evidence-based foundation from which healthcare professionals can assess an individual’s risk of having an RCT at the point of consultation.
Methods
We searched Pubmed/MEDLINE (1956 to 11 February 2015) for publications in any language that recorded associations between identifiable risk factors and RCTs. Our search term was as follows: ‘(rotator cuff tear OR rotator cuff tendinopathy OR rotator cuff tendinitis) AND (risk factor)’. We also extracted and included the relevant citations of systematic reviews within our list for our review.
Out of the 210 studies we obtained, we selected all studies related to RCTs, rotator cuff tendinitis and their risk factors. We assessed the quality of these studies with a scoring system, adapted from Duckitt et al., 7 paying attention to participant selection (assessing the way in which participants were selected, comparing the potential extent of representation of study population to general population), comparability of groups being studied, study population size, study design and how the diagnosis of RCTs were made (Table 1). The maximum score a paper could obtain was 11 points. We excluded any study that failed our scoring system (< 6 points).
Rubric of assessment system.

Data analysis was carried out using Review Manager 5.3. 8 Where papers contained raw data, we calculated the unadjusted odds ratios (ORs) with 95% confidence intervals via Mantel–Haenszel statistics. We took into account random effects within our analysis model. For combined studies, we calculated the I2, statistic for combined studies, 9 which takes into account the proportion of total variation in study estimates as a result of heterogeneity of the studies included. For certain studies, we were unable to combine data. For such studies, we described the results from the studies along with their published ORs or relative risks (adjusted or crude). For factors in which data was combined from studies, Forrest Plots are displayed.
Results
We identified 230 studies. After screening titles, we read 92 abstracts. We subsequently excluded 48 further studies as they were cadaveric studies, had no data analyses regarding rotator cuff tendinopathies, had poor or no data analysis techniques or were not written in English. We read 44 full-text articles, of which 5 were removed as they were either systematic reviews or meta-analyses.
We scored the remaining 39 articles based on our adapted assessment system. Details of our scoring system can be found in Table 1. The maximum number of points a paper could score was 11 points. Sixteen articles were removed as they failed our scoring system (<6 points). Details regarding the individual scores of the 39 papers can be found in Table 2.
Score breakdown for selected studies based on selection criteria.

Six other articles were removed as there was no analysis regarding RCTs (i.e. only other forms of rotator cuff tendinopathies, such as rotator cuff tendinitis, were discussed). A total of 17 articles were available for our qualitative synthesis, of which, 10 articles were used for the meta-analysis. Details regarding the included studies can be found in Table 3. A list of excluded studies is available upon request. The Prisma diagram in Figure 1 summarizes the article selection process for the systematic review and meta-analysis.
Characteristics of included studies.
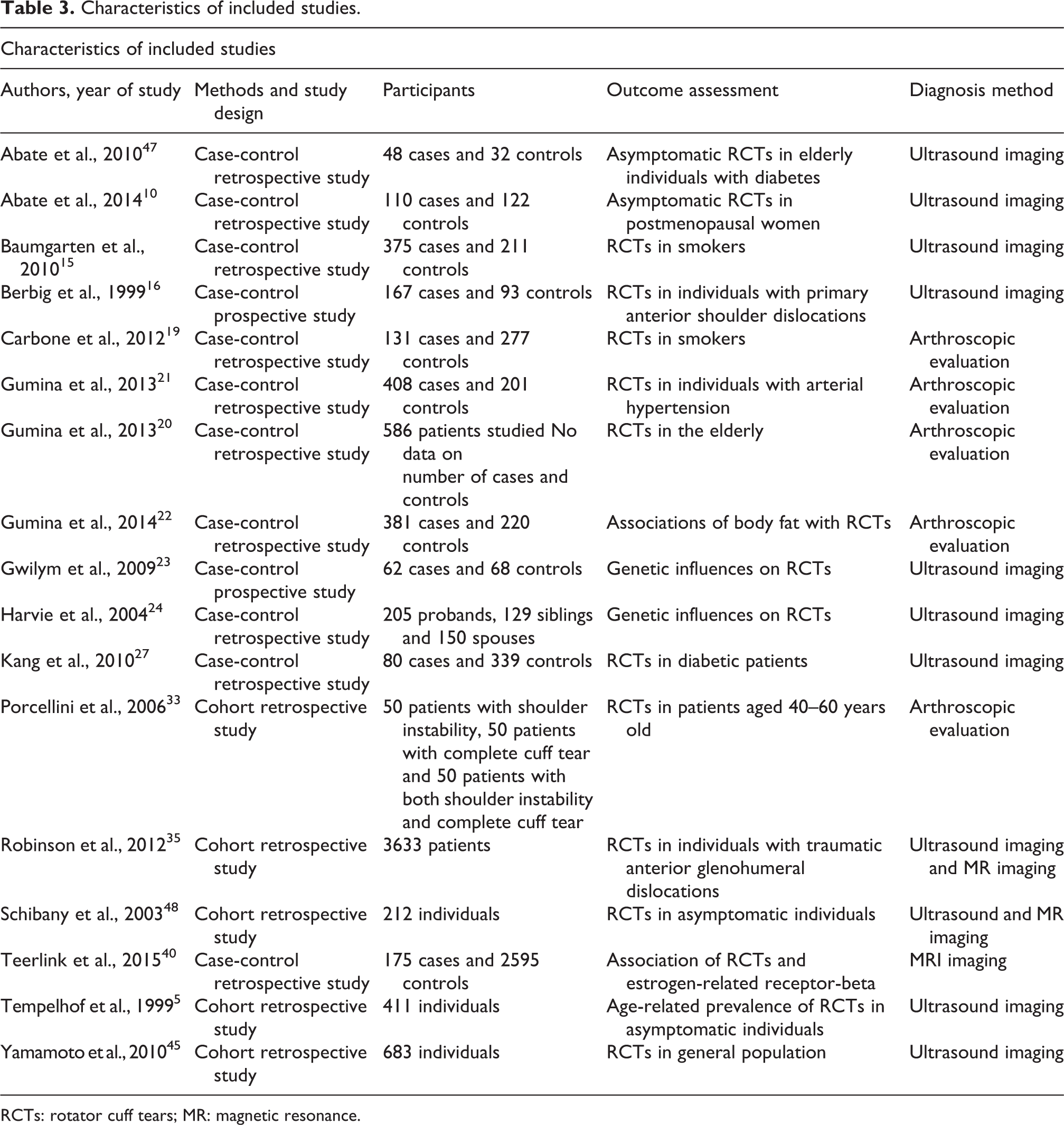
RCTs: rotator cuff tears; MR: magnetic resonance.
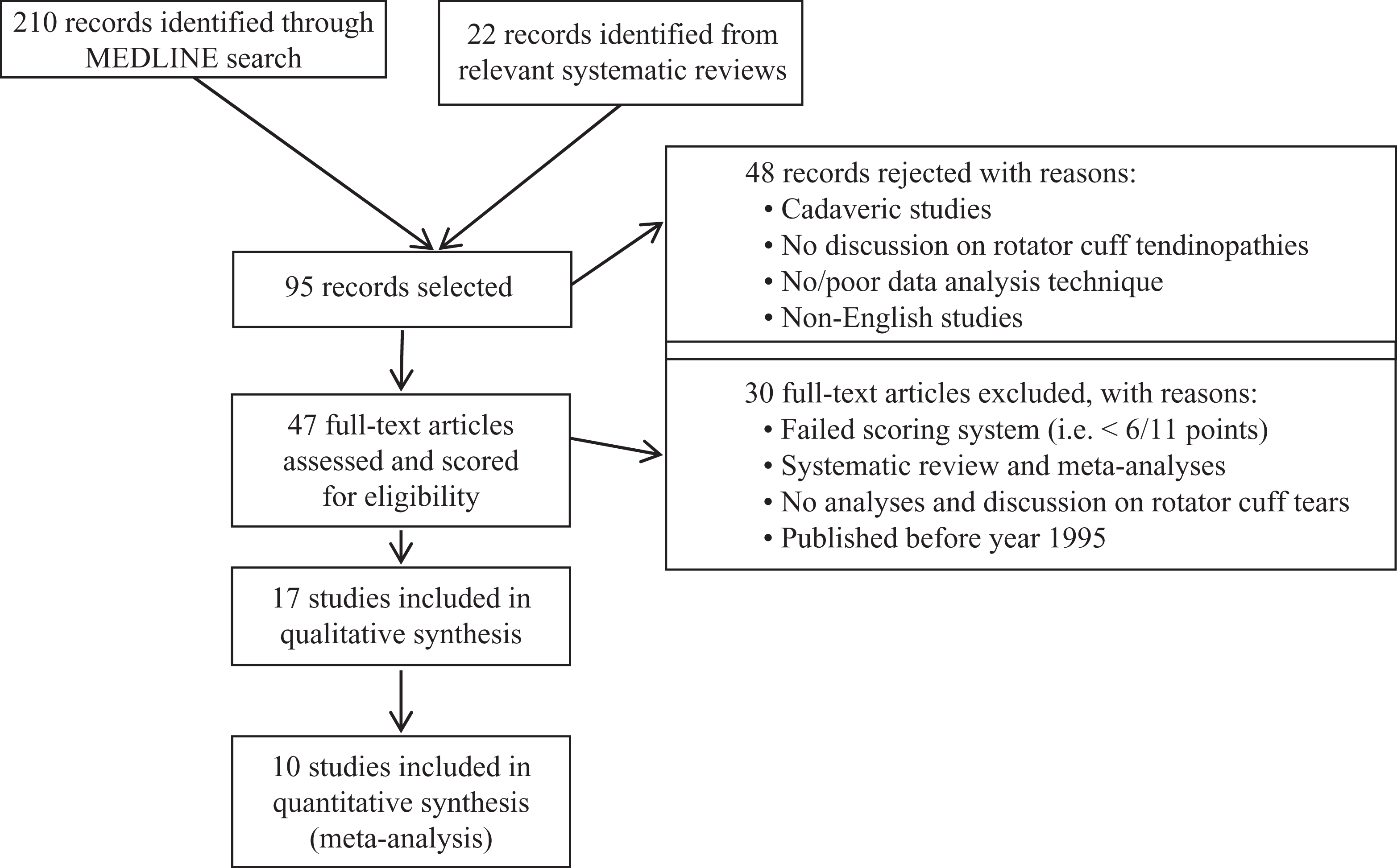
PRISMA diagram outlying flow of article selection.
A summary of our systematic review findings can be found in Table 4. From our systematic review, we noted that there were only five factors, which had a statistically significant calculated ORs, namely age above 60 years (OR = 5.07, 95% CI: 2.45–10.51), dominant hand (OR = 2.30, 95% CI: 1.01–5.25), overweight body mass index (BMI) (OR = 2.35, 95% CI: 1.65–3.40), tobacco smoking (OR = 1.74, 95% CI: 1.25–2.43) and hypertension (OR = 1.93, 95% CI: 1.36–2.74). However, for most of the parameters, there are insufficient populations being studied to make a synthesized conclusion of their extent of effect towards contribution to RCTs.
Summary of results from systematic review.a

BMI: body mass index; CI: confidence interval.
a I 2 for overweight BMI, tobacco smoking, hypertension and diabetes mellitus were not applicable as there was only one study within our included studies that analysed each factor. Hence, there was no heterogeneity of studies to be assessed.
From the systematic review, we further analysed the age of patients (Table 5), hand dominance (Table 6) and gender of patients (Table 7) in relation to their influence on RCTs. In all, taking into consideration random effects, females had an OR of 0.98 (95% CI: 0.66–1.45, Z = 0.09, p = 0.93) revealing that gender may not be a significant parameter for RCTs based on the current data. However, hand dominance and the age of patient were revealed to be significant factors with respect to sustaining RCTs. Total OR for dominant hand was 2.30 (95% CI: 1.01–5.25, Z = 1.99, p = 0.05). A significant level of inter-study heterogeneity was noted (τ 2 = 0.20, χ 2 = 44.24, df = 5 (p < 0.00001), I 2 = 89%). A more substantial relationship was noted between a greater age of patient and RCTs. The total OR for individuals aged 60 years and above sustaining an RCT was 5.03 (95% CI: 2.45–10.51, Z = 4.37, p < 0.0001). A significant level of inter-study heterogeneity was also noted (τ 2 = 0.47, χ 2 = 25.24, df = 3 (p < 0.0001), I 2 = 88%).
Forest plot synthesizing overall odds ratio for RCT in individuals aged 60 years and above.

CI: confidence interval; M–H: Mantel–Haenszel. Heterogeneity: τ2 = 0.47; χ2 = 25.24, df = 3 (p < 0.0001); I 2 = 88%. Test for overall effect: Z = 4.37 (P < 0.0001).
Forest plot synthesizing overall OR for RCT in dominant hand.

OR: odds ratio; RCT: rotator cuff tear; CI: confidence interval; M–H: Mantel–Haenszel. Heterogeneity: τ2 = 0.38; χ2 = 8.84, df = 2 (P = 0.01); I 2=77%. Test for overall effect: Z = 1.99 (P = 0.05).
Forest plot synthesizing overall OR for RCT in Female Gender.

OR: odds ratio; RCT: rotator cuff tear; CI: confidence interval; M–H: Mantel–Haenszel.
Heterogeneity: τ 2 = 0.20; χ 2 = 44.24, df = 5 (p = 0.00001); I 2 = 89%. Test for overall effect: Z = 0.09 (P = 0.93).
Discussion
The results in our study conclude that both the dominant hand and older age are associated with higher odds of sustaining an RCT. Within our study, factors such as a high BMI, hypertension and smoking were not considered to be associations with RCTs as they were only reported in one article each and hence could not be generalized sufficiently to the rest of the international population.
Benson et al. 49 discuss that the aetiologies of RCTs are multifactorial. The aetiologies for RCTs revolve around both homeostasis of normal tissue and elimination pathways for damaged and superfluous cells. Any disruption in such homeostasis and elimination pathways can result in rotator cuff tendon degeneration. It extreme cases, this tendon degeneration can present as RCTs. Disruptions in homeostasis, from the pathophysiological perspective, result in excessive apoptosis within the tendon itself. Case in point, the number of apoptotic cells in the torn aspects of the rotator cuff tendons has been shown to be double that of normal tendons. 50 The role of apoptosis has also been proven by animal studies revealing apoptotic gene upregulation and eventual increased apoptosis upon high strain and overuse. 51,52 Apoptosis in itself is a process of programmed cell death. 53,54 It is prompted by a variety of chemical signals, such as glucocorticoids, growth factor withdrawal, reactive oxygen species and cytokines. 55
Hand dominance and older age were both noted to be significantly associated with RCTs. The dominant hand had more than double the odds of sustaining an RCT as compared to the non-dominant hand, while an individual aged 60 years or above was approximately at a five-time higher odds of sustaining an RCT as compared to an individual less than 60 years old. Both these observations can be explained by the increased apoptotic activities observed under such circumstances. The dominant hand tends to be utilized more than the non-dominant hand and hence tends to be placed under higher stress. This increases apoptosis at the sites of increased stress. RCTs predictably will occur at the site of highest stress.
Tendons in the elderly have a significantly compromised microvascular system making the patient more prone to degeneration, microtears, calcification, fibrovascular proliferation and general insult. All these pathways place the elderly at higher risk of sustaining RCTs. 56,57 A study performed by Milgrom et al. revealed that the prevalence of both partial- and full-thickness RCTs increased markedly after 50 years of age and that these findings were present in more than 50% of dominant shoulders in the seventh decade of life and in 80% of participants over 80 years of age. 28 Yamaguchi et al. 58 noted that the average age for an individual without an RCT was 48.7 years, 58.7 years for those with a unilateral tear and 67.8 years for those with a bilateral tear. Moreover, further logistic regression analysis revealed a 50% likelihood of a bilateral RCT at 66.0 years of age (p < 0.01).
Factors such as diabetes mellitus, hypertension, smoking and older age prompt such chemical signals, induce excessive apoptosis and consequently impede current elimination pathways via poor vascularity, alterations in material properties as well as matrix composition changes and consequently. Although we did not consider a high BMI, hypertension, diabetes mellitus and smoking as associations with RCTs within our analysis due to insufficient reporting of these factors within the current literature, patients with such factors potentially are at a higher risk of RCTs. 59 –61 Furthermore, such interference with elimination pathways can potentially prolong the healing process of these patients.
The data for gender association with RCTs was equivocal as well, with a total OR of 0.98 (CI: 0.66–1.45). This may indicate that the homeostasis of natural tissue and elimination pathways as well as the extent of apoptosis is similar in both the male and female genders.
Conclusion
In conclusion, our meta-analysis revealed that both hand dominance and older age are associated with RCTs. Although we revealed that a higher BMI, a history of hypertension and history of smoking are associated with RCTs within our systematic review, these associations cannot be generalized to the entire international population as it strong data was only presented in one study. Future studies should focus more on strengthening the literature for the association between RCTs and factors such as diabetes mellitus, hypertension, smoking and BMI. Studies should also explore other novel risk factors as well as basic sciences explaining the underlying basis for the association between each factor and RCTs. It is hoped that with such information, treatment options can be improved, thus influencing management protocols and patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.