
Abstract
Background/purpose
The relationship between a handball player's upper body posture, body weight distribution in relation to body height is poorly understood. So, this study explored the relationship between body height and sagittal spinal curvatures and plantar pressure distribution in handball players.
Method
According to handball player's body height, 63 male handball players were divided into two groups; group A (age, 23.54 ± 1.32 years) consisted of 30 handball players with body height above average, and group B (age, 23.40 ± 1.73 years) consisted of 33 handball players with body height below average. The thoracic and lumbar curvatures and trunk height were measured with the Formetric III 4D spine, and the DIERS Pedoscan device was used to assess the plantar pressure distribution for both groups.
Results
The thoracic kyphosis of group A was significantly higher than that of group B (p = 0.001), without a significant difference in lumbar lordosis (p = 0.086). Group A showed a significant increase in the forefeet pressure and a significant decrease in the rearfeet pressure compared to group B (p = 0.001). There was a high positive correlation between the body height and trunk length, and body height and kyphosis angle (r = 0.932, r = 0.665, respectively). There was a high positive correlation between the body height and forefoot plantar pressure (r = 0.665, p < 0.01).
Conclusion
The taller handball players have an increased thoracic kyphosis angle and forefeet pressure compared to shorter handball players.
Introduction
In many sports, the trunk asymmetries and disproportional muscle strength are often well-known; these may be caused by the non-uniform stresses applied to the spine or sport-specific unilateral muscle work, 1 which develops differences between both sides of the body. 2 The configuration of spinal anterior–posterior arches in handball, volleyball, and taekwondo athletes tend to be changed, where the degree of thoracic kyphosis angle was greater than the degree of lumbar lordosis angle, 3 where the largest values were noticed in the superior-thoracic region, whereas the lowest ones in the lumbar-sacral section.3,4
Athletes with segmental asymmetry may be more susceptible to injuries. 4 Handball which was considered as a unilateral loading sport, 5 affects the spinal anterior–posterior curvatures due to its training specificity and predominant forward flexion posture. 3 The taller the handball players, the greater the thoracic kyphosis, 6 and a lesser lumbar lordosis than the normal non-athletic subjects. 7 So, regular posture assessment is recommended during its practice. 8
The playing skill is significantly influenced by body anthropometry, and changes in the plantar pressure distribution can have an impact on athletes’ performance.9,10 The kyphotic posture of the handball players displaces the center of mass anterior,3,7 which disturbs the postural control, 11 plantar pressure distribution and foot loading patterns. 12 As a result, the kyphotic subjects preserve their anteroposterior equilibrium by increasing the heel contact duration. 13
Few studies have reported the impact of sagittal spinal curvatures, and body height on static foot plantar pressure distribution, which were conducted on patients or normal participants rather than athletic players.6,14 In addition, the relationship between a handball player's upper body posture, body weight distribution, and postural sagittal/frontal sway in relation to body height is poorly understood. 15
Some studies showed that the plantar pressure distribution provides useful information for exercise and rehabilitation to prevent body imbalance and injuries in sports.16,17 So, Esparza et al. 18 suggested further studies to investigate the changes in plantar pressure of different sports, rather than soccer and basketball players, as the lower extremity injuries caused by non-body contact are highly prevalent as the repetitive high loads on the foot could cause these injuries. Since the aforementioned studies showed that handball has a different specificity than other sports. This study, therefore, aimed to explore the relationship between the body height and sagittal spinal curvatures and plantar pressure distribution in handball players.
Methods
Participants
A total of 63 handball players participated in this cross-sectional study which was conducted between November 2021 and January 2022. The G*Power 3.1 software was used to calculate the sample size depending on a pilot study, which was done on ten participants (five subjects in each group) before starting the actual study to estimate the effect size. It was determined as 60 participants (30 in each group) according to effect size = 0.65, alpha = 0.05 and power = 0.80. So, the actual sample size was more than enough to conduct the study. The participants were divided into; group A consisted of 30 participants with body height above average, and group B consisted of 33 participants with body height below average. Their demographic data are presented in Table 1.
Demographic characteristics of the handball players.
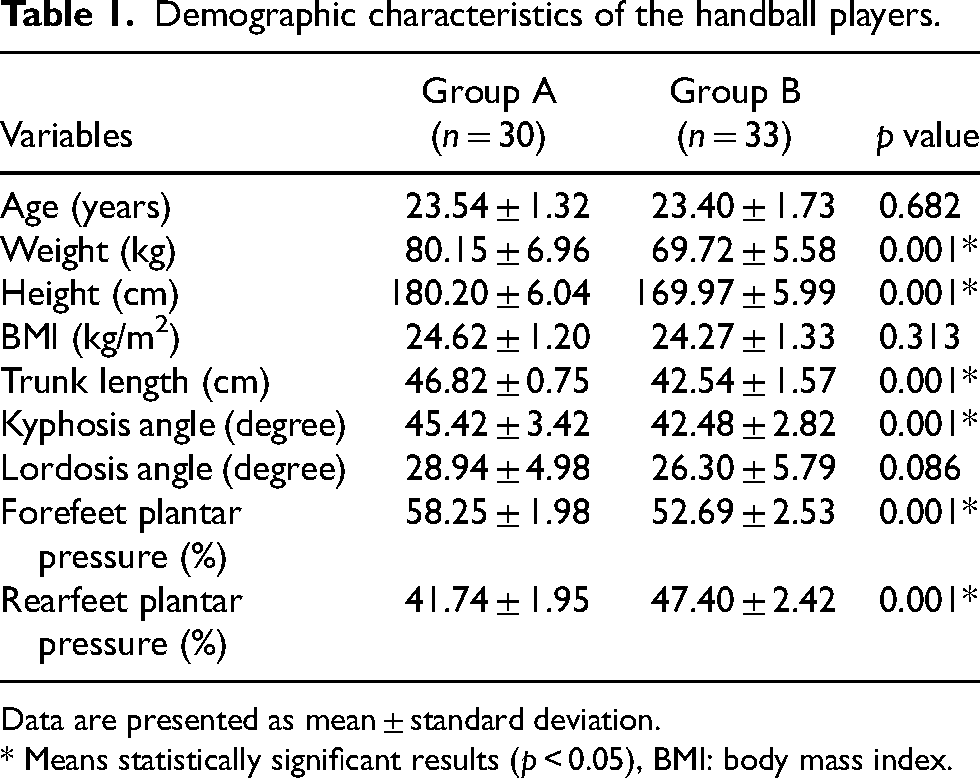
Data are presented as mean ± standard deviation.
* Means statistically significant results (p < 0.05), BMI: body mass index.
They were recruited from five different local clubs. Initially, 72 participants were screened for eligibility, nine did not undergo the inclusion criteria, which were; (1) attended 120 min training six times per week, and (2) their training duration ranged from 3 to 6 years. This information was obtained through a meeting before the conduction of the evaluation procedures. The participants were excluded if they had traumatic back injuries, were diagnosed with scoliosis, congenital spine abnormality, a history of neurological disorder or orthopedic surgery involving the back and lower extremities, balance disturbance, or any types of foot deformities, and participants who has tight tendo-achilles and prone to increase the forefoot pressure intrinsically. Each participant signed a written consent form and the research protocol was performed in agreement with the Declaration of Helsinki, and accepted by the ethics committee of the authors’ affiliated institutions (P.T.REC.012/003752).
Procedures
The DIERS Formetric (four-dimensions, International GmbH, Schlangenbad, model No. 1010112157, Germany) and DIERS Pedoscan (RS scan 1.0 m, International GmbH, Germany) were used for the optical measure of the spinal sagittal curvatures, trunk length, and plantar pressure distribution. The Formetric system provided four-dimensional images of the spine. It depends on the photogrammetric record of the spine with a rasterstereography procedure and DiCAM v2.2.0. The Pedoscan system (a 50 cm wide platform containing 4096 pressure sensors, and data gathering frequency was 300 Hz), delivered the percentage of plantar pressure distribution in four plantar areas (right forefoot, right rearfoot, left forefoot, and left rearfoot) during standing.6,14 The measuring data delivered an accurate three-dimensional model of the spine with a real-time foot pressure map. The feet static images are provided with a color representation of the feet and metrical information on the front-back and left–right pressure distribution in percentage.
The consistency of the measurements achieved with the Formetric spine-shape analysis has been verified by a comparison with digital and objective X-ray images. This device has a highly accepted validity compared with X-ray images, with excellent inter-and intra-rater reliability. 19 Furthermore, numerous research remarked on the Pedoscan's accuracy and reproducibility. 14
The stereographic projector/camera was calibrated by placing a flat whiteboard in the place of the contributor; the volume origin calibration was performed every day through the whiteboard image. Its height was modified according to the participant's body height. The cameras and their resultant strobes were adjusted to yield the best photographic resolution. The resistive measurement plate of Pedoscan is calibrated from time to time (every 2-3 months) to maintain its sensitivity. The participant was instructed to stand barefoot in a comfortable, erect posture on a fixed Pedoscan platform in a dark room. He should wear only his underwear (the area from the neck to two lumbar dimples is free from clothes), and his head should be directed forward with open eyes. 14
The trial was cancelled if the participant changed his position, talked or moved any body's segment. White light and parallel horizontal lines were seen on his back; these lines covered the whole length of the participant's back from the neck region to the lumbar dimples. The trunk length from C7-VP (VP; vertebral prominence) to the lumbar-DM (DM; point located on the back surface between the left and right lumbar dimples) was detected using the Formetric device. Moreover, the kyphosis and lordosis angles were measured with the reported precision of depth error (z-axis) < 0.25 mm and lateral error (x/y-axis) < 0.20 mm. 20 The image quality was enhanced by adjusting the contrast and brightness of the camera. The black and white positive images were scanned and cropped to decrease the size of the data. The three-dimensional model of the spine was created automatically to quantify the kyphosis and lordosis angles. For the four-dimensional average measurements, the presented image is the mean for all taken images. Consequently, the obtained result is only one image (Figure 1).
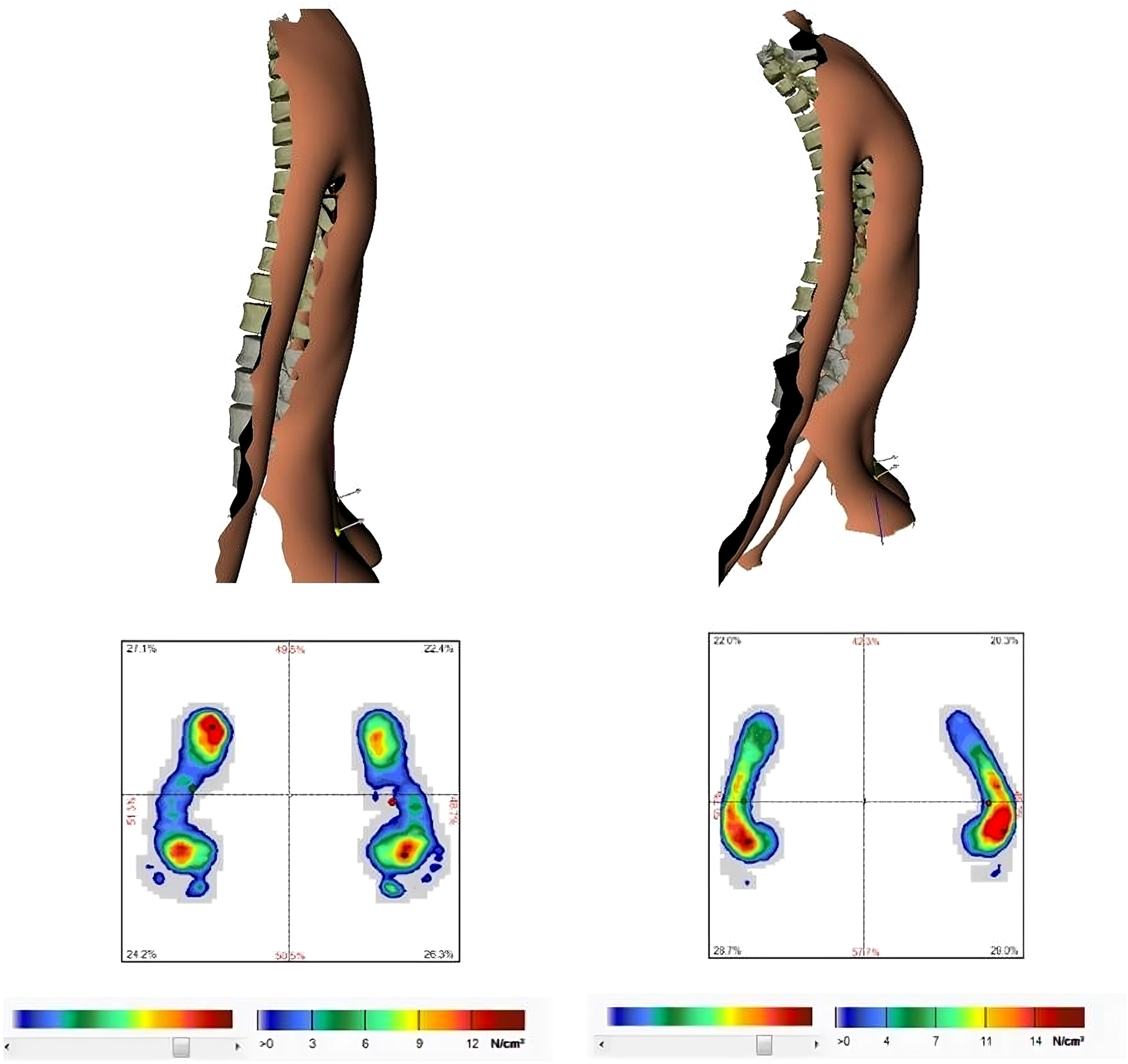
The percent of plantar pressure distribution of feet quadrants with a four-dimensional average of the spine.
Regarding the plantar pressure distribution, the participant stood barefoot on the plantar pressure platform, 14 and the snapshot of percentage feet plantar pressure distribution was obtained through the pressure maps; total forefoot pressure (TFP) and total rearfoot pressure (TRP) were calculated. The measurement of each participant was repeated three times. The average and standard deviation (mean ± SD) values of the total percentage of forefeet and rearfeet plantar pressure were calculated (through the detection of the percentage of four-foot quadrants). The percentage of forefoot plantar pressure included the summation of the percentage of the right and left forefeet, while the percentage of rearfoot included the summation of the percentage of the right and left rearfoot.
Statistical analysis
IBM Statistical Package for the Social Sciences SPSS version 20 for Windows version 7 software was applied for the statistical analyses. The normality of the distributions was confirmed by the Shapiro-Wilk test (p > 0.05). The independent t-test was used to identify differences in anthropometric data, percentage foot plantar pressure, and spinal sagittal curvatures of both groups. Correlation analyses were applied to examine the potential effect of the body height and kyphosis angle on the percentage of total forefeet plantar pressure in both groups by conducting the Pearson correlation test (r). The significance level was set at p < 0.05.
Results
Regarding age and BMI the results showed no statistically significant differences between the above (group A) and below-average (group B) body-height handball players (p > 0.05), as shown in Table 1.
Group A showed a significant increase in thoracic kyphosis compared to group B (p = 0.001). There was no significant difference in the lordotic angle between both groups (p = 0.086). Statistically significant differences were detected in the percentages of total forefoot and rare foot pressure in group A compared to group B (p < 0.05), as shown in Table 1.
Regarding group A; there was a high positive correlation between the body height and trunk length; body height and kyphotic angle (r = 0.932, p = 0.001; r = 0.665, p = 0.001, respectively). There was a weak positive correlation between body height and lumbar lordosis (r = 0.376, p = 0.040). The body height showed a high positive correlation with the percentage of total forefeet plantar pressure (r = 0.665, p = 0.001), and the body height showed a high negative correlation with the percentage of rarefeet plantar pressure (r = 0.668, p = 0.001).
There was a moderate correlation between the kyphotic angle and trunk length (r = 0.522, p = 0.003), and a highly significant correlation between the kyphotic angle and body height (r = 0.665, p = 0.001). A high positive correlation between the kyphotic angle and percentage of total forefeet pressure and a high negative correlation between the kyphotic angle and percentage of total rarefeet pressure (r = 0.751, p = 0.001; r = −0.753, p = 0.001, respectively) were detected, as shown in Table 2.
Correlations among body height, trunk length, spinal curvatures, and the percentage of forefeet plantar pressure distribution.
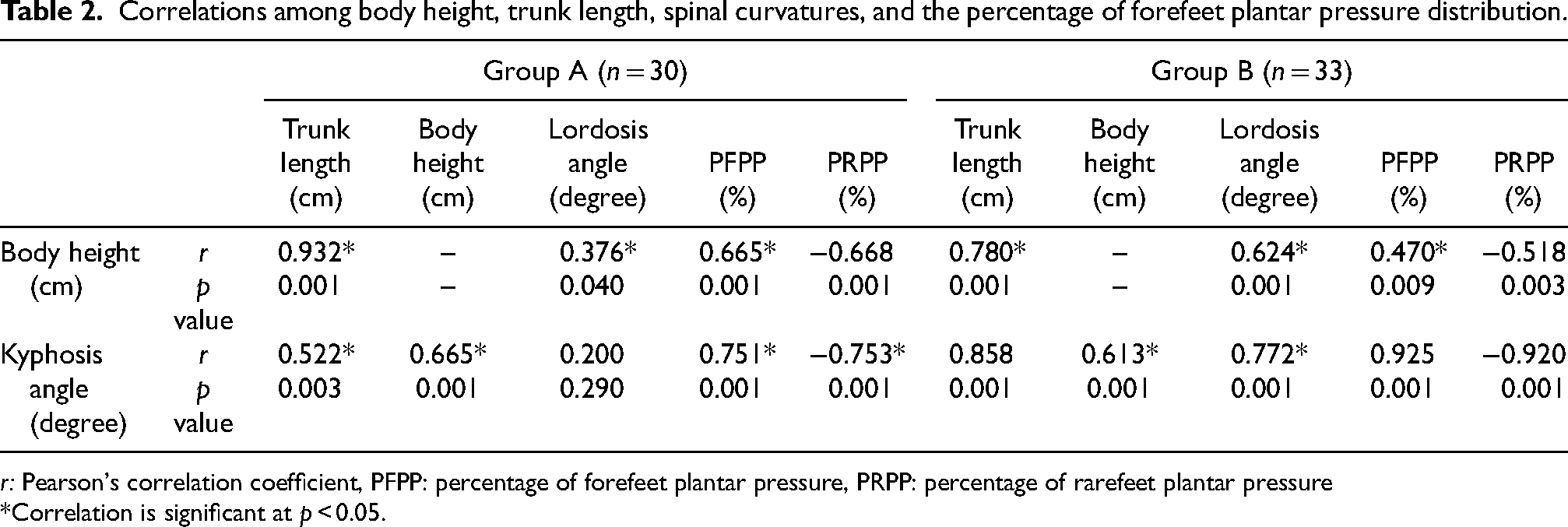
r: Pearson's correlation coefficient, PFPP: percentage of forefeet plantar pressure, PRPP: percentage of rarefeet plantar pressure
*Correlation is significant at p < 0.05.
For group B; there was a high positive correlation between the body height and trunk length; body height and kyphotic angle (r = 0.780, p = 0.001; r = 0.613, p = 0.001, respectively). Also, a high positive correlation was detected between body height and lordotic angle (r = 0.624, p = 0.001). A moderate correlation was detected between the body height and total forefeet pressure (r = 0.470, p = 0.009), and a moderate negative correlation between the body height and total rarefeet pressure (r = −0.518, p = 0.003).
There was a high positive in the trunk length and the kyphotic angle; body height and kyphotic angle (r = 0.858, p = 0.001; r = 0.613, p = 0.001). A high positive correlation was detected between the kyphotic angle and the percentage of TFP, while a high negative correlation was detected between the kyphotic angle and percentage of TRP (r = 0.925, p = 0.001; r = −0.920, p = 0.001, respectively).
Discussion
The current study demonstrated the relationship between body height and plantar pressure distribution in two groups of different body heights of handball players (above and below-average body height). The prevalence study of Hershkovich et al. 21 which was conducted on 829,791 subjects aged 17 years showed for all height groups, a correlation between height and the risk of spinal abnormalities with severity was discovered. Thus, the degree of spinal abnormalities is likewise positively correlated with body height. These results support the present findings which showed that the handball players with body height above average reported a significant increase in thoracic kyphosis angle compared to handball players with body height below average. However, there is no significant difference in the lordotic angle between both groups.
There was a high positive correlation between the body height and trunk length; body height and kyphotic angle, this indicated a great impact of body height on increasing the thoracic kyphosis, this result was consistent with the recent findings of Ohlendorf et al. 15 who confirmed that the male handball players with a body height above average have a larger kyphosis angle than smaller counterparts with the same training level.
Another study 22 conducted on volleyball players explained that kyphotic posture tended to be more and the lordotic one less frequent in volleyball players than in untrained subjects, the authors returned that finding to the typical volleyball posture consisting of a forward bend with a rounded back, the arms and shoulders protruding. Some authors point to the effect of body height on chest kyphosis which may be augmented in tall people. 23 Furthermore, it has been shown that handball players have deepened thoracic kyphosis, similar as volleyball players. 24 Wilczyński et al. 25 reported that the angle of thoracic kyphosis was reduced in 19% of handball players, while in 12%, it was enlarged. On the other hand, a reduction in the angle of lumbar lordosis, excessive lateral deflection, surface rotation, and deflection from the vertical position in the majority of handball players were detected.
The throwing sports develop spinal misalignment; Sliwa et al. 26 examined the changes of spinal curvature in volleyball players, who participated in the European junior volleyball championships. They didn’t confirm the relation between the degree of lumbar lordosis and body height. The current study showed that the handball players with a body height below average have a high positive correlation between their body height and lordotic angle, and handball players with a body height above average have a weak positive correlation between their body height and lumbar lordosis, this may return to the biomechanical compensation through increasing the thoracic kyphosis angle to gain a spinal balance. 27
In addition, a high positive correlation between body height and trunk length in both handball groups was confirmed by Alonso et al. 28 who noticed an increased trunk-cephalic length with increasing body height. Furthermore, a high positive correlation was detected between the trunk length and kyphosis angle, this relationship was reported by Ameer and Abdel-Aziem 7 who reported that the taller handball players have longer trunk length and greater thoracic kyphosis. Additionally, the observed changes in the shape of anteroposterior spinal curvatures might be related both to sports training and somatic parameters.22,27
In addition, the current study showed significant differences in the percentages of the total forefoot and rare foot pressure in handball players with body height above average (group A) compared to handball players with body height below average (group B); regarding group A, the body height showed a high positive correlation with the percentage of total forefeet plantar pressure, and the body height showed a high negative correlation with the percentage of rarefeet plantar pressure. While, group B showed a moderate correlation was detected between the body height and total forefeet pressure, and a moderate negative correlation between the body height and total rarefeet pressure. This indicated by increasing the body height, the percentage of total forefoot plantar pressure increases in comparison to the percentage of rarefeet plantar pressure, So, increasing the body height, and thoracic kyphosis tend to change the percentage of plantar pressure between the forefeet and rearfoot plantar regions.
These findings coincide with Pomarino and Pomarino 29 who confirmed that the increased percentage pressure distribution between the forefoot and rearfoot in normal adult subjects, whereby the distribution between the two sides of the body is almost balanced. Also, the handball players showed a greater laterality effect on their leading foot in comparison to the non-leading foot by changing the plantar pressure and force distributions between both feet. Also, the leading feet had greater plantar pressure, with more pressure concentration at the forefoot. 17
The taller handball players group has an increased thoracic kyphosis which was associated with the increase in the forefoot pressure and decrease in the rearfoot pressure compared to the shorter handball players group and no significant difference in lumbar lordosis of both groups concurs with the findings of Żurawski et al. 30 who found that in static settings, there was a positive correlation between the thoracic kyphosis degree and the percentage forefoot load. Moreover, they concluded that the distribution of ground reaction forces on the feet is influenced by the magnitude of lumbar lordosis and thoracic kyphosis, and there is a linear relationship between the percentage of forefoot and rearfoot loads and the lumbar lordosis.
The current study had many limitations, the study did not include handball players from both genders. Instead of focusing solely on the static condition, it is advised to examine both static and dynamic activities when examining how body height affects the plantar pressure distribution in handball players. Although being a unilateral sport, handball's impact on the spine's lateral alignment has not been studied. So, more research is required to determine whether handball players, especially the tallest ones, have spinal scoliosis. Moreover, the effects of team positioning (i.e. wings, pivots, goal, and rearward center) were not studied. It has been determined that each handball position requires physiological and physical characteristics specific to the player's position. More attention should be paid to research into how plantar pressure distribution affects players' performance and risk of injury in handball. Finally, a longitudinal study is necessary to determine the long-term implications of the body height of handball players on the development of spine and foot asymmetry over time.
Conclusion
The taller handball players have an increased thoracic kyphosis angle and forefeet pressure, and a decreased rearfeet pressure compared to shorter handball players. However, the body height has had no effect on the lumbar spine alignment. So, the tallest handball players should have regular assessments of posture and lower extremities by the handball coaches, and training sessions should include exercises that support proper upper body alignment and body weight distribution on the feet.
Footnotes
Acknowledgements
The authors are grateful for everyone's participation and tremendous efforts during the course of this study project.
Authors contributions
Amr Abdel-aziem and Mariam Ameer contributed to the conception of the study, analysis, manuscript preparation, data analyses, and writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This research has been approved by the IRB of the ethics committee of the Faculty of Physical Therapy, Cairo University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.