
Abstract
Purpose
A fundamental understanding of plantar pressure distribution is important for prescribing an appropriate orthosis and applying nonoperative methods, such as stretching exercises, for the treatment of plantar fasciitis. Despite existing research on plantar pressure distribution, discrepancies between affected and unaffected sides in unilateral plantar fasciitis patients warrant further investigation. This study aimed to evaluate the plantar pressure distribution in patients with unilateral plantar fasciitis by comparing it with that on the contralateral unaffected side.
Methods
We retrospectively reviewed records from 20 consecutive patients diagnosed with unilateral plantar fasciitis, using the unaffected side as the control. The emed® pedobarographic system was used to measure the plantar pressure distribution during gait. The analysis was performed using a 4-mask configuration (toes, forefoot, midfoot, and hindfoot).
Results
Both sides showed no significant differences in radiographic parameters. The affected side showed a significantly higher contact area, maximum force, and force-time integrals in the midfoot. However, the unaffected side demonstrated significantly higher maximum force and force-time integrals in the hindfoot. There was no difference in the distribution of the peak pressure and pressure-time integrals between the two sides in all mask regions. The increased contact area and maximum force in the midfoot on the side with plantar fasciitis may result from heel pain-induced weight transfer from the hindfoot.
Conclusion
The findings of this study provide a basic understanding of plantar pressure distribution in the treatment of plantar fasciitis and highlight the importance of considering inter-side differences when designing treatment interventions or orthotic devices.
Introduction
Plantar fasciitis is a common cause of chronic pain in patients. 1 They often report heel pain upon first stepping out of bed in the morning, and in some cases, this discomfort extends along the plantar fascia to the midfoot and forefoot, with localized focal tenderness observed during physical examination.
The heel bears a substantial amount of weight during walking, 2 making discomfort a frequent complaint among patients while performing their daily activities. Although various treatments have been introduced with reports of excellent outcomes, there remains no consensus on the superior treatment method even in systematic reviews. 3 Therefore, nonoperative treatment methods are often preferred over invasive approaches, with orthoses and stretching exercises being the most common forms of treatment. 4
A fundamental understanding of plantar pressure distribution is essential for prescribing suitable orthoses and applying nonoperative treatments, such as stretching exercises. In our clinical experience, patients frequently experience satisfaction and improvement when heel cups are used to support painful areas. Previous biomechanical studies have shown that heel cups can reduce stiffness and increase the thickness of the heel pad while standing through confinement. 5 Despite this, fundamental research on the baseline status of plantar fasciitis by measuring plantar pressure is lacking. 6 Previous research has primarily focused on how treatments such as extracorporeal shock wave therapy (ESWT) affect changes in plantar pressure distribution before and after treatment.7,8 To the best of our knowledge, only one case series of 12 patients has compared the plantar pressure distribution of the symptomatic side to that of the contralateral asymptomatic side. 9
Therefore, this study aimed to compare the plantar pressure distribution on the symptomatic side in patients with plantar fasciitis with that on the asymptomatic side, serving as a control, using the emed® pedobarography platform. We hypothesized that the maximum force and peak pressure would be lower in the hindfoot area of the symptomatic side than on the asymptomatic side, as individuals tend to bear less weight to avoid pain. Furthermore, we anticipated that the contact area of the hindfoot would decrease on the symptomatic side.
Materials and methods
Study protocol
This retrospective level III comparative study received approval from our Institutional Review Board (IRB) and informed consent was obtained from all participants. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
We retrospectively reviewed the medical records of consecutive patients diagnosed with unilateral plantar fasciitis between July 2021 and December 2022. Inclusion criteria consisted of: (1) unilateral heel pain persisting for over 3 months, and (2) completion of a pedobarographic examination during the initial visit. Exclusion criteria included: (1) severe deformities potentially affecting abnormal plantar pressure, (2) recent trauma within the past 6 months, and (3) history of foot and ankle surgery. Ultimately, 20 patients were included in the analysis.
To minimize inter-individual variability, the unaffected side was designated as the control. Comparisons were performed to assess differences in radiographic and pedobarographic parameters between the affected and unaffected sides.
Radiographic measurement
Radiographic measurements were performed by a fellowship-trained orthopedic surgeon using picture archiving and communication system software (INFINITT Healthcare Co., Seoul, Republic of Korea). The lateral talo-first metatarsal angle, hallux valgus angle, and first-second intermetatarsal angle were measured on plain standing radiographs to mitigate the potential impact of severe foot deformities on plantar pressure. 10
Plantar pressure measurement and analysis
We used emed® (novel GmbH, Germany) to scan and record pressure distribution beneath the foot in dynamic conditions. The specifications included a sensor area of 475 mm × 320 mm, 6080 sensors, a resolution of four sensors/cm2, and an operating frequency of 100 Hz. Participants were instructed to walk barefoot along the platform at comfortable speeds. For the analysis, emed® CL (novel GmbH, Germany) was employed. Pedobarographs were segmented and masked into four areas (toes, forefoot, midfoot, and hindfoot) as previously described (Figure 1).
11
The contact area (cm2), maximum force (% body weight), peak pressure (kPa), force-time integrals (% body weight Four masks (toes, forefoot, midfoot, and hindfoot) used in this study.
Statistical analysis
All statistical analyses were performed using SPSS version 29 (IBM Corp., Armonk, NY, USA). Normal distribution of the data was evaluated using the Kolmogorov–Smirnov test. Continuous variables between the affected and unaffected sides were compared using the Wilcoxon signed-rank test, with statistical significance set at p < .05.
Results
Demographic data of the study participants.

Data are presented in mean ± standard deviation.
Study participants’ radiographic measurement data.

Data are presented in mean ± standard deviation.
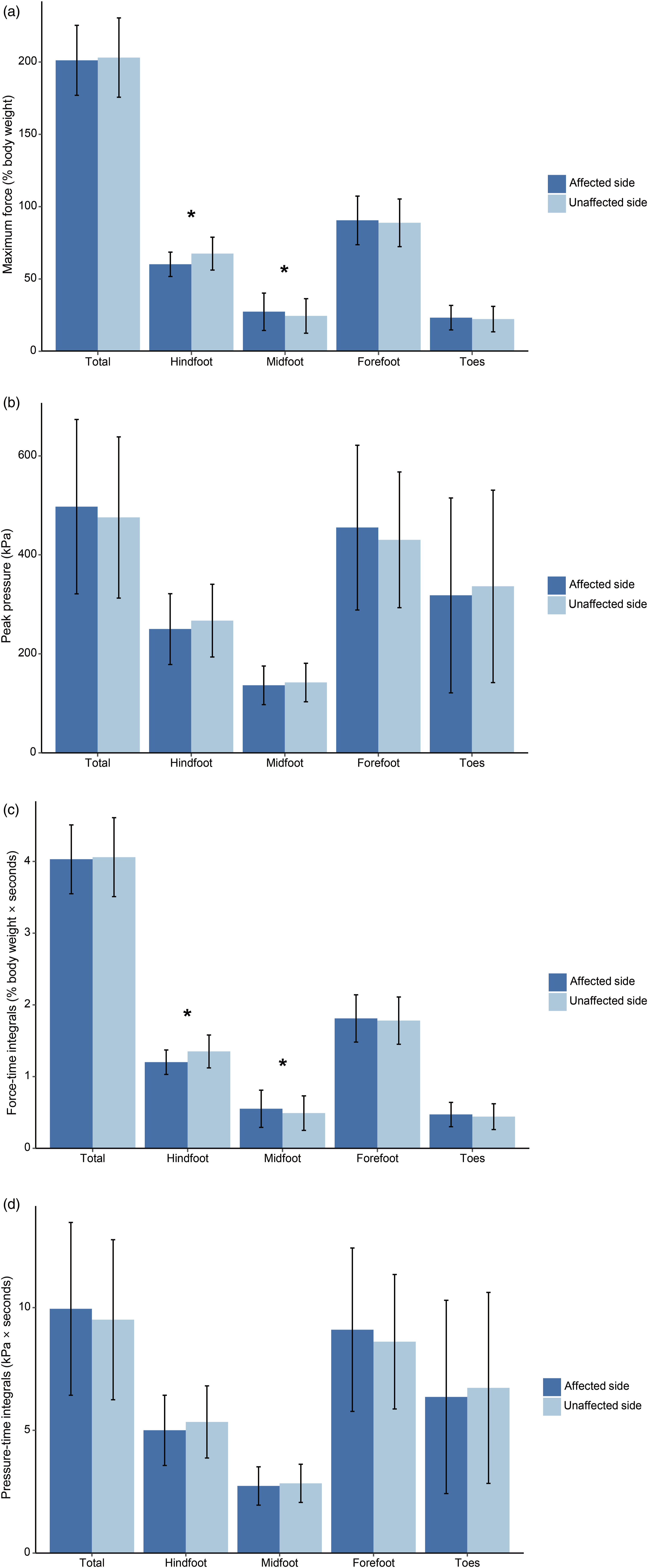
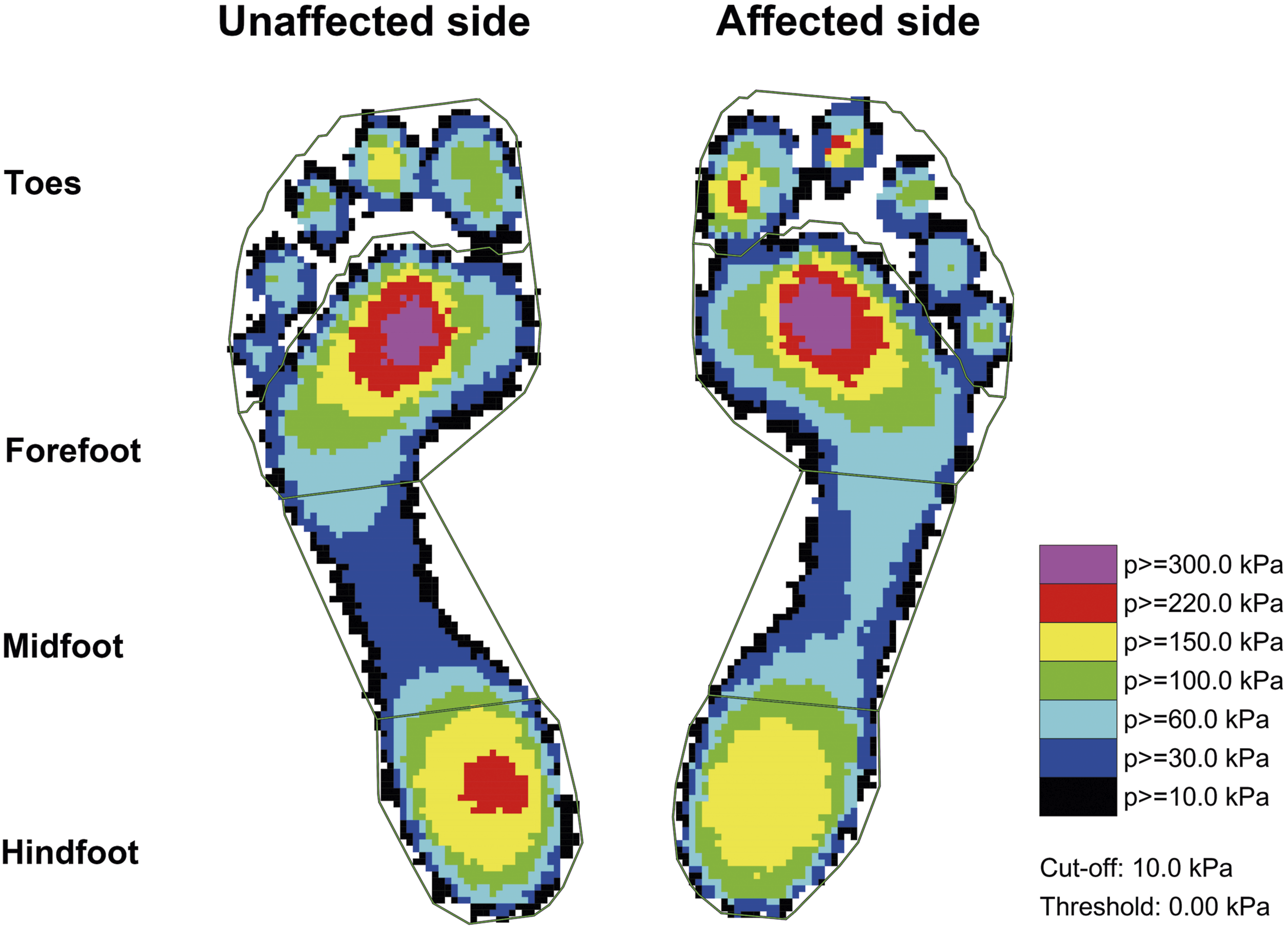
Regarding the recorded pedobarographic parameters, the contact area was significantly greater in the midfoot on the affected side compared to the unaffected side (28.9 ± 10.3 vs 26.3 ± 8.2, p = .007) (Figure 2 and Table 3). On the affected side, the maximum force was significantly higher in the midfoot (27.3 ± 12.9 vs 24.4 ± 11.9, p = .048), whereas on the unaffected side, it was significantly higher in the hindfoot (67.5 ± 11.4 vs 60.1 ± 8.4, p = .030) (Figure 3(a) and Table 3). However, there was no difference in peak pressure distribution between the two sides across all mask regions (Figure 3(b) and Table 3). Although force-time integrals were notably higher in the midfoot on the affected side (0.55 ± 0.26 vs 0.49 ± 0.24, p = .044), they were significantly higher in the hindfoot on the unaffected side (1.35 ± 0.23 vs 1.20 ± 0.17, p = .038) (Figure 3(c) and Table 3). This indicates a similar trend to that observed in maximum force. However, no significant difference in peak pressure was noted, attributed to the greater midfoot contact area on the affected side. Moreover, pressure-time integrals showed no significant difference between the two sides (Figure 3(d) and Table 3), aligning with the observed trend in peak pressure. Representative bilateral pedobarographs of the participant with plantar fasciitis are shown in Figure 4. Comparison of contact area between affected and unaffected sides. Asterisks denote significant difference between the sides. Study participants’ pedobarographic data. Data are presented in mean ± standard deviation. Bold values denote p < .05. Abbreviations: BW, body weight; s, seconds. aNormalized by body weight. Comparison of (a) maximum force, (b) peak pressure, (c) force-time integrals, and (d) pressure-time integrals between the sides. Asterisks denote significant difference between the sides. Representative pedobarographs of the participant with plantar fasciitis.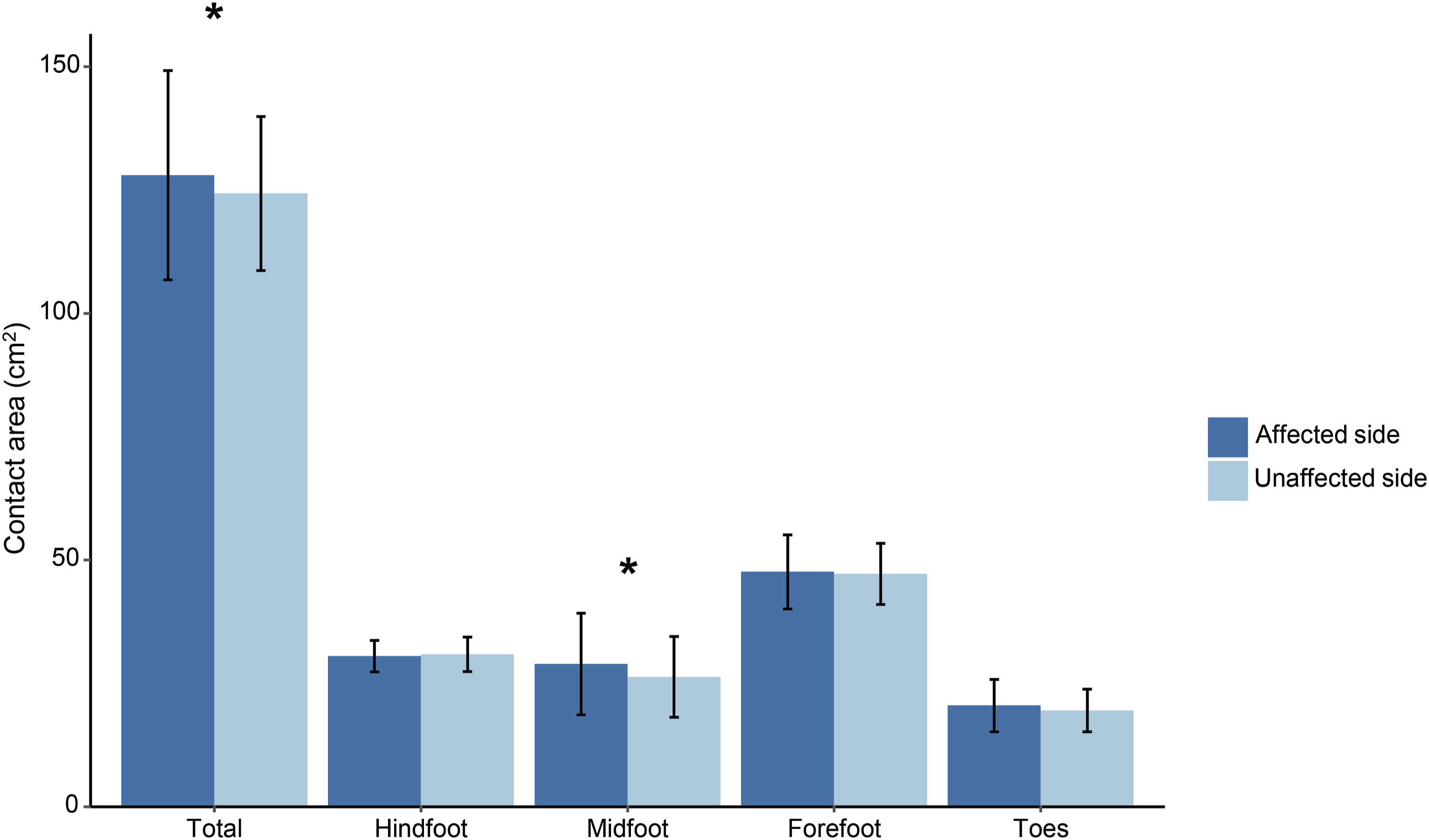

Discussion
In this study, we evaluated patients with unilateral plantar fasciitis who had experienced heel pain for an average of approximately 3 years and conducted a dynamic plantar pressure analysis to investigate the differences in plantar pressure distribution between the affected and unaffected sides.
The primary finding of this study was an increase in contact area and maximum force in the midfoot areas on the side with plantar fasciitis, which can be interpreted as the result of weight transfer from the hindfoot to the midfoot due to heel pain. A previous study reported that patients with plantar fasciitis made gait adjustments that resulted in a reduced ground reaction force beneath the rearfoot. 1 In other words, to reduce pain during walking, it can be said that the strategy involved minimizing the contact area of the heel, which corresponds to the hindfoot, and avoiding bearing weight on it. Meanwhile, increasing the contact area in the midfoot region and transferring the force facilitated the forward movement. The lack of significant difference in the peak pressure and pressure-time integrals between the two sides can be attributed to the definition of pressure, which is the force divided by the area. Therefore, even if the force increased, the peak pressure did not increase as long as the contact area increased. The results of this study differ markedly from those previously published by Hsu et al., 9 who analyzed plantar pressure distribution in 12 patients with plantar fasciitis and compared the symptomatic and asymptomatic sides before and after the application of ESWT. They found that after 3 weeks of ESWT treatment, there was a significant increase in the forefoot peak contact pressure, a significant decrease in the contact area of the digital area on the symptomatic side, and a significant reduction in the total foot impulse. However, at baseline before the ESWT intervention, there was no significant difference between the symptomatic and asymptomatic sides in any foot region (including the hindfoot, midfoot, forefoot, and digital) in terms of peak pressure, contact area, impulse, and contact duration. The discrepancy between the results of the present study and those of Hsu et al. may be attributed to the small sample size used in their research. In contrast, our study involved a larger group of 20 participants, providing more robust results than those in the existing literature.
A previous study demonstrated that combining Achilles tendon stretching with plantar fascia stretching led to superior clinical outcomes. 12 Other studies have reported a relationship between plantar fascial thickness and Achilles tendon pathology. 13 In patients with plantar fasciitis, it is not uncommon for the Achilles tendon to be tight. 14 This tightness can hinder ankle dorsiflexion, leading to plantar flexion of the foot upon contact with the ground. As a result, loading may shift towards the midfoot or forefoot, exacerbating pain in the sole of the foot. Therefore, stretching of the Achilles tendon is necessary to prevent weight transfer from the original hindfoot to the midfoot or forefoot. One might be concerned that stretching the Achilles tendon by increasing the maximum force and contact area in the hindfoot could conversely exacerbate symptoms in patients with heel pain. However, the results presented in this study indicate that concerns may be unwarranted, as the maximum force on the hindfoot of the asymptomatic unaffected side is higher than that on the affected side. In addition, it is physiologically normal for the heel area to bear more weight during gait. 2
The significance of this study lies in the fact that understanding plantar pressure distribution is crucial for the nonoperative treatment of patients with plantar fasciitis. However, there has been a lack of research on this basic aspect. In addition to the study by Hsu et al., 9 two other studies compared plantar pressure distribution in asymptomatic healthy individuals as the control group. Kanatli et al. hypothesized that loss of heel pad elasticity was related to heel pain, affecting heel pressure distribution; however, they found no relationship between heel pad compressibility and peak pressure at heel strike. 15 Kelly et al. also reported no significant difference in either contact duration or peak pressure under the heel between subjects with and without heel pain. 16 Nevertheless, our study holds significant value in that we compared both sides in patients with unilateral plantar fasciitis to reduce inter-individual variability and included five major pedobarographic parameters.
Our study had several limitations. Firstly, it was retrospective, and only unilateral patients who underwent plantar pressure measurements were included, resulting in a small sample size. However, this may be attributed to our study’s focus on symptomatic diseased participants. This is because conducting pedobarographic or gait studies in a diseased state presents challenges. Therefore, we only performed pedobarographic analysis in the initial state. A follow-up study that compares these measurements after the participants have recovered from plantar fasciitis would also be valuable. Secondly, our findings indicated that the maximum force on the hindfoot of the unaffected side tended to exceed that on the affected side. However, it remains to be confirmed whether this increase is significant compared to the normal group, or if the affected side is significantly reduced compared to the unaffected side. Therefore, a comparison between the affected and unaffected sides, along with an asymptomatic control group matched for age and sex, would have provided more informative results. Lastly, gait analysis using reflective marker sets was not performed. However, it is worth noting that our study measured plantar pressure distribution dynamically during walking, rather than statically. In future studies, evaluating changes in heel strike duration due to heel pain or investigating kinematics across intersegmental motion of the foot and ankle regions would be beneficial.
Conclusion
Our study could serve as a useful reference for explaining the plantar pressure distribution in patients with chronic heel pain in outpatient clinics. Understanding the biomechanical alterations associated with plantar fasciitis can guide the development of targeted exercise regimens aimed at addressing specific pressure points and optimizing foot function during daily activities. In addition, the findings of this study could aid in effectively prescribing appropriate orthoses for patients with plantar fasciitis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2016R1D1A1B02009379) and in part by SNUH Research Fund (grant No. 0420212120). The funding source did not have a role in the study design, in the collection, analysis, and interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for publication.
Ethics approval statement
This research ethics was approved by Seoul National University Hospital Institutional Review Board (IRB number: H-2105-067-1218). All research protocols were carried out in accordance with the ethical standards of the Institutional Review Board and with the Declaration of Helsinki.