
Abstract
The Manchester–Oxford Foot Questionnaire is a validated English 16-item patient-reported outcome measure for evaluating foot and ankle function. This study aimed to translate a Cantonese Chinese version of the questionnaire and evaluate its validity and reliability among patients with foot and ankle disorders. The translation and cross-cultural adaptation were conducted by forward translation, synthesis of translated versions, backward translation, review, and pre-testing by a panel of healthcare professionals. The test-retest reliability was conducted within 2–4 weeks. Internal consistency and construct validity were evaluated using the Visual Analogue Scale and Short-Form 36. 135 participants were recruited to complete the validation process. The overall reliability coefficient constituted 0.86 (intraclass correlation coefficient = 0.72–0.93). A strong, statistically significant correlation was found between the bodily pain subscale of Short-Form 36 and the pain subscale of the Cantonese Chinese-Manchester-Oxford Foot Questionnaire (r = −0.77, p < 0.001). This was similar to the pain subscale of the Cantonese Chinese-Manchester-Oxford Foot Questionnaire and visual analogue pain score (r = 0.77, p < 0.001). The overall score for the Cantonese Chinese Manchester-Oxford Foot Questionnaire between the healthy control group and the pathological group was statistically different (p < 0.001). A good consistency level was found in the questionnaire with a Cronbach's alpha coefficient of 0.78, 0.86, 0.78, 0.85 for pain, walking/standing, social interaction, and the overall domain of the Cantonese Chinese-Manchester-Oxford Foot Questionnaire, respectively. Therefore, this questionnaire can be adapted as a reliable clinical assessment and an outcome measure among the Cantonese Chinese-speaking population.
Keywords
Introduction
Patient-reported outcome measures (PROMs) are part of a patient-centred care model to provide a reliable and valid measure of a patient's symptoms, function and quality of life. 1 They are essential in evaluating the efficacy of orthopaedic treatment and healthcare outcomes in clinical trials. 2 In general, foot and ankle surgery still lacks a gold-standard self-reported instrument to evaluate the outcomes.3–7 Isolated use of clinical physical examination signs may not be comprehensive enough as it may not be able to accurately evaluate the patient's perceptions of outcome, i.e., their symptoms. 2
Currently, most self-reported outcome measures are designed in the English language; thus, it is required to translate, culturally adapt, and validate the questionnaire to a different language to suit the local context.8,9 Developed by a group of researchers from Oxford University, the Manchester-Oxford Foot Questionnaire (MOXFQ) is an internationally recognised 16-item PROM consisting of three different subscales, including pain, walking/standing and social interaction, with a summary index score (MOXFQ-Index). 10 The MOXFQ was first administered to postoperative hallux valgus patients and subsequently to a large cohort of 671 patients with different foot and ankle conditions.9,10,11 The MOXFQ displayed an advantage compared to other questionnaires in detecting chronological changes of an intervention. 12
The Chinese language is one of the six official languages in the United Nations and one of the most commonly used languages, with approximately 1.31 billion Chinese speakers accounting for 16% of the global population. 18 Although the MOXFQ has been translated into simplified Chinese, a Cantonese-Chinese version is still lacking.13–17 Specific language expressions and cultural differences exist between these dialects and Cantonese-Chinese, which is primarily used in Southern China and Hong Kong, just like the recently translated CAIT-HK version. 13 For instance, MOXFQ-CH translated “shooting pain” in Qn 12 as “闪痛” 14 which is a phrase that Cantonese-speaking individuals do not use. Therefore, a specific translated MOXFQ is required to evaluate its related symptoms for populations using Cantonese Chinese.
The study aims to translate the MOXFQ into the Cantonese-Chinese version through a cross-cultural adaptation process and verify this translation's validity and reliability among people with foot and ankle conditions.
Methods
This study is part of a randomised controlled trial and has been approved by CUHK-NTEC clinical research committee. The reference number is 2022.263-T. The data have not been communicated to a third party.
Participants and data collection
The data collection was conducted between August–November 2022, and 135 participants were recruited from patients and visitors at the Department of Orthopaedics and Traumatology at the Prince of Wales Hospital, Hong Kong. The inclusion criteria were age over 18 years old, no active cognitive/psychological impairment, and fluency in reading and understanding traditional Chinese (Cantonese) language. The first group were healthy subjects with no foot and ankle pathology, and the second group were patients clinically diagnosed with foot and ankle diseases.
Description of the Chinese-MOXFQ version
The validated Cantonese Chinese-MOXFQ includes 16 questions to measure patients’ health. The questionnaire is divided into three dimensions: walking/standing (seven items), pain (five items), and social interaction (four items). Each question is scored from 0 to 4, where 0 represents the best state of the symptoms, and 4 is the worst symptoms/most severe health state. The maximum potential sum is 64 (representing the greatest severity), and then transformed into a 0–100 scale, using the formula: (Summation/64)*100. 12
Translation adaptation
The translation of the English MOXFQ questionnaire to Cantonese Chinese was conducted based on internationally accepted guidelines.15,16 The translation process consists of five stages, mainly the forward translation by two independent translators, synthesis I (comparison of the two versions), blinded backward translation, synthesis II (comparison of the two back-translated versions), pilot testing and testing of the pre-final version of the translated instrument.15,16 These steps were supervised by a panel of medical professionals comprising physiotherapists and doctors. Firstly, the original English version of the questionnaire was forward-translated independently by two native translators into Cantonese Chinese. In the second stage, the two copies of the Chinese questionnaire were merged into one version. The merged version of the Cantonese Chinese MOXFQ was then back-translated into English to ensure that the meaning did not differ from the source document. In the fourth stage, the merged version of the Cantonese Chinese MOXFQ was reviewed and amended by an expert committee of healthcare professionals. In the final stage, a unified copy of the Cantonese Chinese MOXFQ was pre-tested in a group of 20 participants; amendments were made according to the focus-group feedback until the questionnaire achieved high acceptance and easy understanding by the participants.
Evaluation of the construct validity in Cantonese Chinese-MOXFQ
Participants had independently completed the Cantonese Chinese-MOXFQ, SF-36 and Visual Analogue Scale (VAS) pain score during the first time point. The SF-36 questionnaire is a health-related quality-of-life instrument comprising 36 questions relating to physical function, bodily pain, and general health. Cronbach's alpha coefficient will be calculated to evaluate internal consistency and measure the average correlation among items of one scale with another to determine whether the items are scored in the same direction. Cronbach's alpha coefficient between 0.80 and 0.90 is considered to be optimal. Values more than 0.7 are considered in an acceptable range.
Evaluation of the reliability test in Cantonese Chinese-MOXFQ
Reliability indicates the proportion of variability in each item or subscale that is due to true differences between individuals. It was assessed using the test-retest method. Participants completed the Cantonese Chinese-MOXFQ twice at two different time points. The interval between each time point was between two to four weeks to avoid memory bias response. All participants completed the questionnaire at the second time point without referring to the previous answers. Demographic factors such as age and gender were collected during the baseline measurement. Test-retest reliability was measured by using intraclass correlation coefficient (ICC).
Floor and ceiling effects of the Cantonese Chinese-MOXFQ
A ceiling effect is when a certain level limits measuring a variable above this level. A ceiling effect is when more than 15% of the questionnaires receive the highest possible score, while a floor effect is defined as when more than 15% receive the lowest score. When a ceiling or floor effect happens, it indicates a group of scores at either the questionnaire's upper or lower score limit. Concerning these effects, content validity will be assessed. 17
Statistical analysis
Construct validity was calculated using Spearman's correlation coefficient (r) between 16 items of the translated Cantonese Chinese-MOXFQ and validated traditional Chinese SF36. With a two-tailed significant level of p < 0.05, a correlation coefficient of ≥ 0.80 is considered a high correlation, 0.60–0.79 is considered a moderately high correlation, 0.40–0.59 indicates a moderate correlation, and 0.2–0.39 indicates a low correlation. 18 The difference between the healthy and pathological groups’ scores will indicate the group's validity. In addition, Mann–Whitey U test was performed to determine whether there was any statistical difference between the two groups. The significance level was set at P < 0.05. All statistical analysis was conducted using IBM SPSS Statistics version 26 (IBM® SPSS ® Statistics).
Results
Patients
In total, 135 patients, including 55 healthy controls without foot and ankle problems and 80 individuals with foot and ankle pathologies, were recruited. The approximate time for them to fill the questionnaire was approximately 25 min, 10 min for the Cantonese Chinese-MOXFQ and 15 min for both SF-36 and VAS for pain score (Table 1).
Descriptive statistics of the total patients (n = 135).

Internal consistency
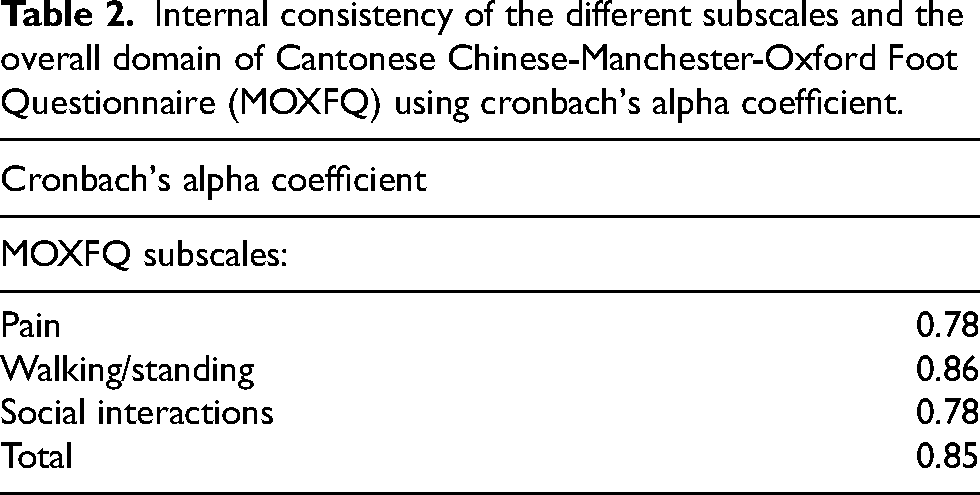
Cronbach's alpha coefficient for all three subscales was between 0.7 and 0.8, demonstrating good consistency across the items in each subscale. Moreover, Cronbach's alpha coefficient for the total Cantonese Chinese-MOXFQ showed good internal consistency across all items included in this instrument. Refer to Table 2 for more information.
Internal consistency of the different subscales and the overall domain of Cantonese Chinese-Manchester-Oxford Foot Questionnaire (MOXFQ) using cronbach's alpha coefficient.
Reliability
Test-retest reliability method was conducted over two time points using the ICC. All patients who had filled up the initial questionnaire were contacted, and 37 participants answered the Cantonese Chinese-MOXFQ for the second time. The ICC for all three subscales of pain, walking/standing, and social interaction were between 0.7 and 0.9 showing good reliability and reproducibility. The ICC for the total Cantonese Chinese-MOXFQ showed good reliability (Table 3).
Mean Manchester-Oxford Foot Questionnaire (MOXFQ) score and test-retest reliability of Chinese MOXFQ.
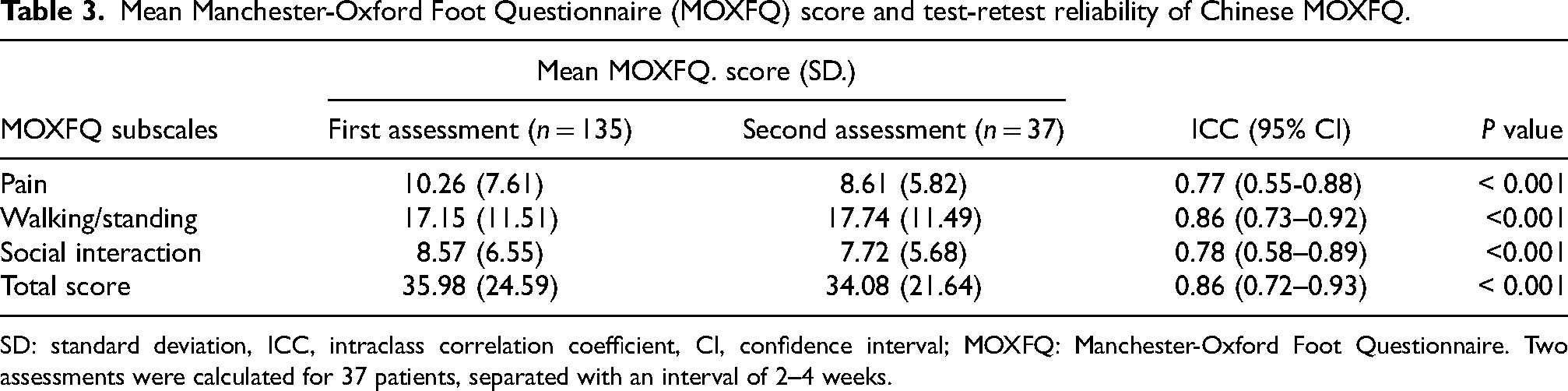
SD: standard deviation, ICC, intraclass correlation coefficient, CI, confidence interval; MOXFQ: Manchester-Oxford Foot Questionnaire. Two assessments were calculated for 37 patients, separated with an interval of 2–4 weeks.
Construct validity between Chinese-Sf-36 and Chinese-MOXFQ version
A moderate to strong correlation between the subscales of the Chinese SF-36 and the Cantonese Chinese-MOXFQ version confirmed the validity of this instrument. The strongest correlation was observed between the bodily pain subscale of SF-36 and the pain subscale of the Cantonese Chinese-MOXFQ (r = −0.77). This is followed by the physical function subscale in Cantonese Chinese-SF36 and the total score of Cantonese Chinese-MOXFQ (r = −0.75), the bodily pain subscale of Cantonese Chinese-SF36 and the social interaction subscale of the Cantonese Chinese-MOXFQ (r = −0.72), the physical function subscale in Cantonese Chinese-SF36 and social interaction subscale of the Cantonese Chinese-MOXFQ (r = −0.71), physical function subscale in the Cantonese Chinese-SF36 and walking/standing subscale of the Cantonese Chinese-MOXFQ (r = −0.71). The correlation coefficients for the other subscales of the Cantonese Chinese-MOXFQ version and the other domains of the Cantonese Chinese-SF36 were either moderately (r < 0.7) or poorly (r < 0.05) correlated, indicating an adequate divergent validity 19 (Table 4). No ceiling effects were found for the Cantonese Chinese-MOXFQ.
Construct validity results: Spearman correlation between mean preoperative scores for each of the Manchester-Oxford Foot Questionnaire (MOXFQ) and sf-36 subscales.
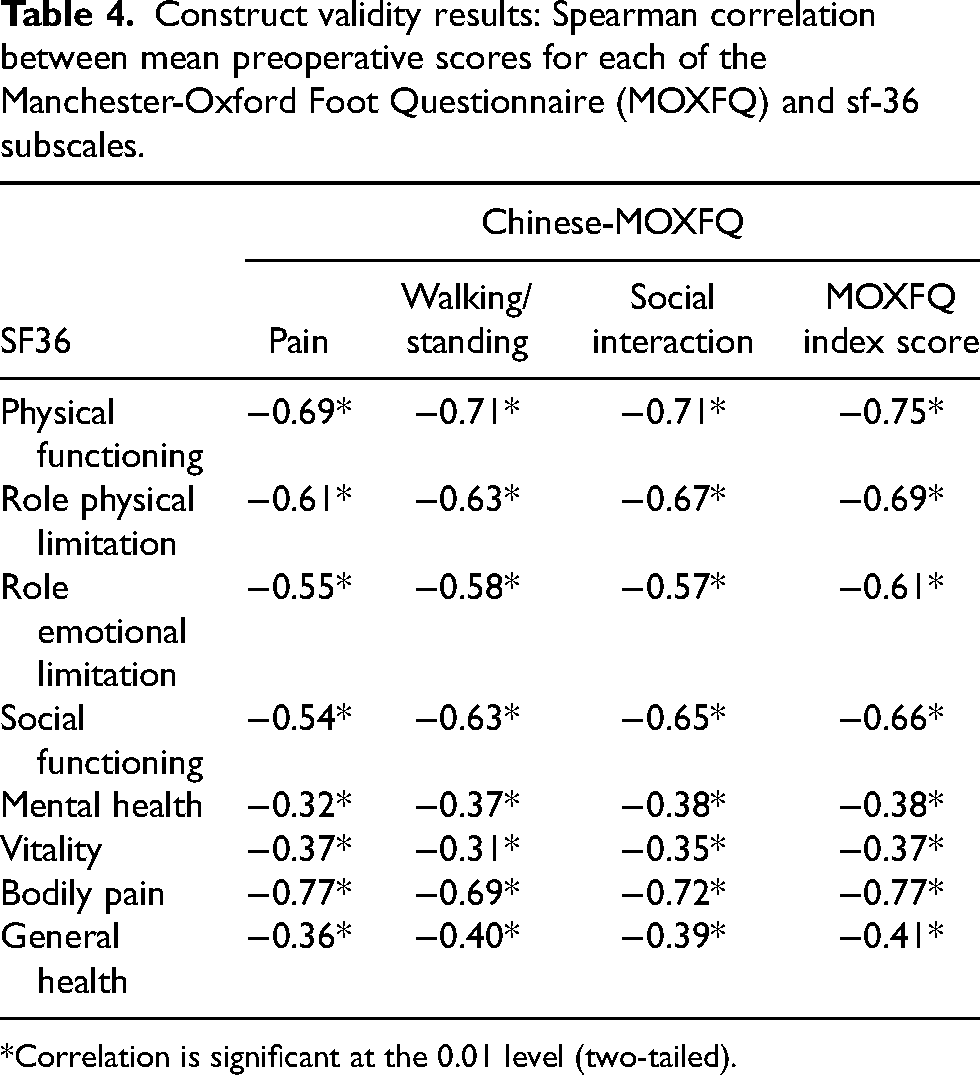
*Correlation is significant at the 0.01 level (two-tailed).
Construct validity between VAS pain score and Cantonese Chinese-MOXFQ version
A positive correlation between the total score of Cantonese Chinese-MOXFQ (16 questions of the MOXFQ) and VAS pain score was found (r = 0.71, p < 0.001). The pain subscale of the Cantonese Chinese-MOXFQ and VAS score for pain was found (16 questions of the MOXFQ, r = 0.71, p < 0.001; MOXFQ-pain, r = 0.77, p < 0.001) (Table 5).
Construct validity results: Spearman correlation between mean preoperative scores for the MOXFQ and VAS pain score.
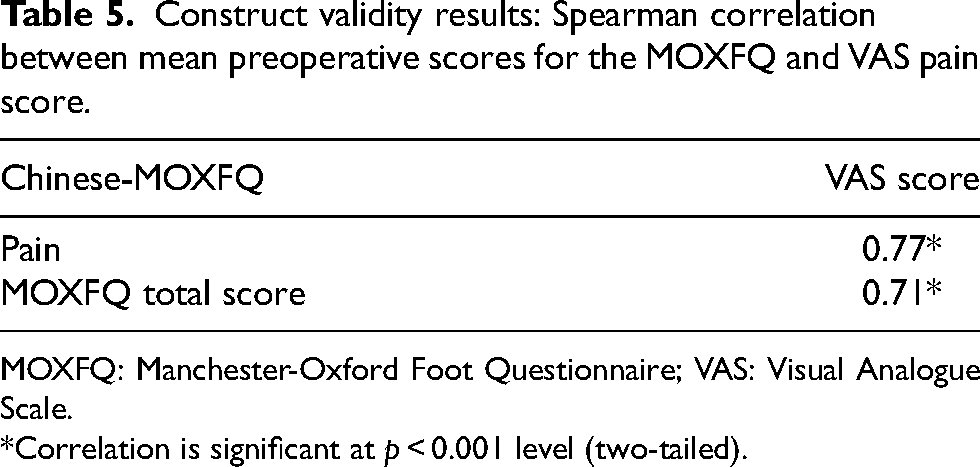
MOXFQ: Manchester-Oxford Foot Questionnaire; VAS: Visual Analogue Scale.
*Correlation is significant at p < 0.001 level (two-tailed).
Discriminant validity of the Cantonese Chinese-MOXFQ
The results demonstrated that healthy participants obtained low average scores while participants with pathological foot and ankle pathologies scored a high average score. The mean score for pain, walking and standing, and social interaction of the Cantonese Chinese-MOXFQ subscales and the Cantonese Chinese-MOXFQ total score in the healthy control group was 12.38 (95%CI 11.07–13.70), 20.82 (95%CI 18.63–23.00), 10.06 (95%CI 8.80–11.32), and 43.26 (95%CI 38.91–47.61), respectively. The scores were significantly higher compared to the pathological group. On the contrary, the scores for the foot and ankle pathological group constituted 4.86 (95%CI 3.13–6.59) for pain, 11.90 (95%CI 8.82–14.98) for walking/standing, 5.20 (95%CI 3.74–6.66) for social interaction and 21.96 (95% CI 15.99–27.93) for the total score of the Cantonese Chinese-MOXFQ. A statistical difference (p < 0.001) was found between the foot and ankle pathological group and the healthy control group regarding the mean scores of the pain, walking/standing, social interaction subscales and the overall score of Cantonese Chinese-MOXFQ.
Discussion
MOXFQ is one of the well-designed, disease-specific PROMS developed by Dawson et al. 20 that can provide reliable and valid measures of health-related issues to the patients, such as pain, function, mobility, and health-related quality of life. The MOXFQ is currently used as a PROM for both clinical trials of surgery and non-surgical treatment.21–23
In the current study, we sought to develop a Cantonese Chinese version of the MOXFQ, namely, Cantonese Chinese-MOXFQ, through translation and cultural adaptation based on the international guidelines and the described psychometric testing.15,16 The key phrases were carefully translated to ensure compatibility of the Cantonese Chinese version with the original version. This is also the first study to evaluate the content validity and reliability of the translated Cantonese Chinese version of the MOXFQ among patients with foot and ankle conditions against a healthy control group. The patients easily comprehended the Cantonese Chinese version of the MOXFQ; no missing data and major drawbacks occurred during the cross-cultural adaptation procedure. Our results demonstrated good reliability, which aligned with other studies.20,24,25 The ICC for the three domains, pain, walking/standing, and social interaction, was 0.77 (0.55–0.88), 0.86 (0.73–0.92), and 0.78 (0.58–0.89), respectively. The overall ICC of the overall domain of the Cantonese Chinese MOXFQ was also high, constituting 0.86 (0.72–0.93). Hence, this has affirmed its’ appropriate use in the Cantonese-speaking population. Simultaneously, the assessment of the internal consistency using Cronbach's alpha coefficient also expressed a good consistency level over each subscale and the overall domain of the MOXFQ. In comparison to the other translated versions of the questionnaire, for instance, the English 12 and the Italian 26 versions, our depicted results (i.e., 0.78 for pain, 0.86 for walking/standing, 0.78 for social interaction, 0.85 for the total score of MOXFQ) were found to be similar. No floor or ceiling effects were observed in this study, as no participant obtained the maximum score and vice versa.
Lastly, the construct validity of the Cantonese Chinese MOXFQ version using spearman correlation showed a strong association between some subscales of the MOXFQ and SF-36. Our results were found to be similar to the original MOXFQ with respect to foot and ankle conditions. 20 In their results, a strong to moderate association was found between the walking/standing subscale of the MOXFQ and all the parameters of the SF-36. In addition, the pain subscale of MOXFQ was strongly correlated with the bodily pain of the SF-36. In accordance with their results, our study has depicted that the pain subscale of the Cantonese Chinese-MOXFQ and the bodily pain subscale of the SF-36 (r = −0.77, p < 0.001) had the strongest association. This is followed by the social interaction subscale of the Cantonese Chinese-MOXFQ and bodily pain subscale of the SF-36 (r = −0.72 p < 0.001), the walking/standing subscale of the Cantonese Chinese-MOXFQ and the physical functioning subscale of SF-36 (r = −0.71, p < 0.001), and the social interaction subscale of the Cantonese Chinese-MOXFQ and physical functioning of the SF-36 (r = −0.71, p < 0.001). A strong correlation was also found between the pain subscale of the Cantonese Chinese-MOXFQ and the VAS pain score(r = 0.77, p < 0.001), suggesting a predictable and consistent relationship between the VAS for pain and the pain subscale of the Cantonese Chinese-MOXFQ. On the contrary, our study also showed a poor association between each subscale of the Cantonese Chinese-MOXFQ with the mental health and vitality subscale of the SF-36, similar to Dawson et al.. 20 This is not unexpected since the development of the Cantonese Chinese-MOXFQ was not intended to measure the patient's mental health and vitality as outcome measures.
Overall, the results of the current study demonstrated that the translation of the MOXFQ into Cantonese Chinese would not lose the psychometric properties of the original meaning in English. Hence, adopting the Cantonese Chinese-MOXFQ is more effective than developing an entirely new scale for Cantonese Chinese patients with foot and ankle pathologies. Compared to the VAS, a commonly used tool to evaluate pain intensity, the Cantonese Chinese-MOXFQ version can reflect the impact of a foot and ankle condition on the individual's daily activities associated with pain. Moreover, a standardised set of questions allows cross-cultural comparison of studies between different countries and increases the robustness of any research studies. Therefore, the Cantonese Chinese-MOXFQ version is a reliable and valid questionnaire to assess the severity of the symptoms in Cantonese-speaking patients with foot and ankle pathologies and can be recommended to be used in clinical and research settings.
The limitation of the study was the lack of comparison between the Cantonese Chinese-MOXFQ with other disease-specific reported outcome measures, such as the Cantonese Chinese-Foot and Ankle Outcome Score (FAOS). 9 Although this was not achieved in this study, a strong correlation between the MOXFQ (walking/standing) subscale and FAOS (activity daily living) subscale, the MOXFQ (pain) subscale and FAOS (pain) subscale and the total domain of MOXFQ and FAOS (quality of life) subscale was established by Arab et al.. 27 Therefore, it is safe to assume that both the original version of MOXFQ and FAOS have acquired comparable psychometric properties. Future studies can integrate FAOS or another foot and ankle-specific PROM to test for the construct validity with the Cantonese Chinese-MOXFQ version. Another potential limitation would be the self-reporting bias from the patients who took part in the study. The convenience sampling method was also introduced due to the limited resources. Patients with pathological foot and ankle conditions were only recruited at a single centre, where they were selected based on proximity and availability. Therefore, this may not fully represent the entire Cantonese-speaking population with foot and ankle pathologies. Nonetheless, based on our results, the representativeness of our sample can be given considerable confidence where the Cantonese-Chinese MOXFQ was semantically equivalent to the original version and evaluated in the different regions of the foot and ankle condition.
Conclusion
In conclusion, the Cantonese-Chinese MOXFQ can be considered a reliable and valid patient report outcome measure for various foot and ankle problems. It can be recommended to grade disease severity and monitor treatment efficiency for foot and ankle pathologies.
Footnotes
Acknowledgements
The authors wish to thank all the patients who participated in the study and the team's research assistant in assisting the data collection.
Author contributions
CSMC and LPH have contributed substantially to the conception, design, analysis, interpretation of the data, and manuscript drafting. LCBC has contributed to the translation of the questionnaire and VKMC, HX have critically revised the intellectual content. LKKS and YSHP supervised the study. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.