
Abstract
Background:
Syndesmotic instability is a significant concern in the management of unstable ankle fractures, occurring in approximately 10% to 13% of these cases. Early recognition and stabilization of syndesmotic injuries are essential to ensure optimal long-term outcomes. Several techniques are currently in use, often involving complex procedure and/or costly devices. Our study presents a syndesmosis fixation technique using K-wires that is both simple and cost-effective.
Methods:
This is a retrospective single-center case series. Three hundred seventy-seven ankle fractures with intraoperative syndesmosis instability and subsequent syndesmosis fixation with a K-wire were treated between 2002 and 2012. Of the 377 patients, 51 died and we were able to obtain long-term questionnaire completions from 94 patients (29% of presumed living patients), with a mean follow-up of 10.6 ± 3.0 years.
Results:
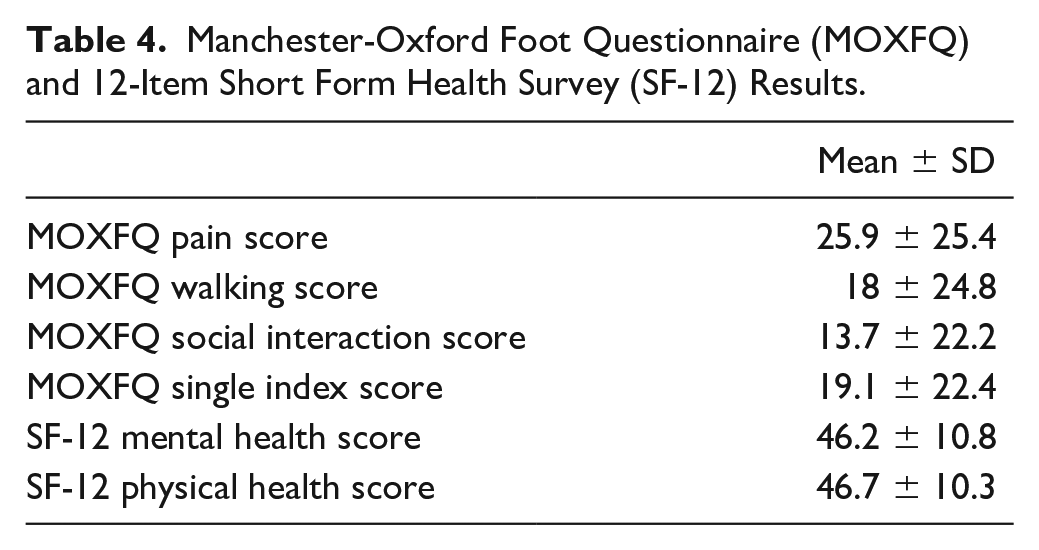
The mean age was 46.6 ± 18.5 years; 42% were Danis-Weber type B and 58% type C fractures. Syndesmosis fixation failure was observed in 9 (2%) patients, and 5 (1%) patients had K-wire displacement without loss of syndesmosis reduction. The Manchester-Oxford Foot Questionnaire (MOXFQ) was obtained 10±3 years after surgery. The mean MOXFQ pain score was 25.9 ± 25.4, the mean functional score was 18 ± 24.8, and the mean social score was 13.7 ± 22.2.
Conclusion:
We report long-term (10.6 ± 3 years) functional outcomes using a validated patient-reported questionnaire in patients who underwent syndesmosis fixation with 2 K-wires for unstable ankle fractures. In the subset of patients we were able to find in follow-up, we found low rates of syndesmosis fixation failure, low pain scores, and excellent functional outcomes. The availability and low cost of these implants make this technique an accessible and cost-effective solution to consider for syndesmosis fixation.
Level of Evidence:
Level IV, retrospective case series.
This is a visual representation of the abstract.
Keywords
Introduction
Ankle fractures are a prevalent injury within the adult population. Syndesmotic instability is observed in approximately 10% to 13% of cases involving ankle fractures.23,27,28 Syndesmosis injuries are often associated with suprasyndesmotic fractures (44-C according to the AO-OTA classification or Danis-Weber C type), but it can also occur in transsyndesmotic fractures (44-B or Weber B type),6,9,23 as well as isolated and associated with proximal fibula fractures, such as the Maisonneuve fracture. 24 The most common mechanisms that produce syndesmotic instability are supination-external rotation (SER) and pronation-external rotation (PER).3,12
Early diagnosis of syndesmosis injury and adequate surgical stabilization are recommended to avoid the development of ankle instability, chronic pain, poor function, and early osteoarthritis in the ankle joint.5,26,34 Different techniques and materials are currently used, but may not be accessible in all health care settings, particularly in resource-limited environments. Trans-syndesmotic screw fixation is traditionally considered the gold standard, even if suture-button fixation is increasingly gaining popularity, 22 as recent studies have demonstrated noninferior functional results and even faster return to sports and lower complications rates.1,31,35 Nevertheless, alternative fixation methods have been described, such as elastic plates and K-wires.14,33 In 1994, Peter et al 16 described a technique for syndesmosis transfixation using 2 K-wires introduced obliquely across the tibiofibular joint. However, little is known about this technique as the available data are almost inexistent. To our knowledge, outcomes of syndesmosis fixation with K-wires in unstable ankle fractures have only been reported once by Missbach-Kroll et al 14 in 2003. In their study, syndesmosis K-wire fixation provided good to excellent outcomes with low complication rates. However, of the 50 included patients, only 36 were reviewed, and no validated outcome scores were used.
Our study aims to describe the surgical technique and report complication rates and long-term functional outcomes using the validated Manchester-Oxford Foot Questionnaire (MOXFQ) in patients treated with syndesmotic K-wire fixation for unstable ankle fractures. Although radiologic assessment remains a standard practice for evaluating the efficacy of syndesmosis fixation techniques, our study seeks to demonstrate that the ultimate measure of success is the functional recovery of the patient, and it can be achieved with a simple and cost-effective technique.
Material and Methods
Study Population
The local ethics committee approved this study. We performed an electronic chart review of all consecutive surgically treated rotational ankle fractures with intraoperative syndesmosis instability and subsequent syndesmosis fixation with K-wire in patients aged 18 years or older between January 2002 and December 2012. Data on baseline patient characteristics, including age, sex, comorbidities (American Society of Anesthesiologists score and diabetes), and lifestyle factors (body mass index and smoking status) were obtained from the anesthesia records. Mechanisms of accidents were obtained from the emergency reports. Bone quality was carefully considered in the selection of the fracture fixation method. However, for the purpose of evaluating syndesmosis fixation using K-wires, we intentionally employed a uniform technique across all patients, irrespective of bone quality or other potential confounding factors. Fractures were classified using the Danis-Weber classification in type A or infrasyndesmotic (AO/OTA 44-A), type B or transsyndesmotic (AO/OTA 44-B), and type C or suprasyndesmotic (AO/OTA 44C). 13 Fractures were further divided into unimalleolar, bimalleolar, and trimalleolar according to the number of fractured malleolus based on preoperative radiographs. 4 The first author reviewed all the radiographs, evaluating fracture patterns on the preoperative radiographs. A second independent analysis of 105 randomly selected cases was performed to assess the interobserver reliability of the classification system.
Complications and adverse events were classified into 5 categories: (1) wound problems with wound infection and skin necrosis; (2) syndesmosis fixation failure with loss of syndesmosis reduction; (3) fracture nonunion, defined as failure to consolidate more than 6 months after surgery; (4) presence of tibiofibular synostosis; and (5) K-wire displacement without loss of reduction. Radiographic parameters including clear medial space, tibiofibular space, and tibiofibular overlap were used to assess loss of reduction.7,20 Postoperative radiographs and clinical examination were performed at 6 weeks, 3, 6, and 12 months after surgery. Radiographs were reviewed for fracture and hardware-related complications, assessing syndesmotic and ankle joint congruity. Reoperations for partial hardware removal (K-wires only) and total hardware removal were noted. Exclusion criteria for this study included patients <18 years of age, polytrauma cases, patients with associated ipsilateral foot injuries, and patients without available postoperative radiographs or incomplete radiologic follow-up. A secondary analysis was conducted to assess the correlation between the syndesmotic loss of reduction and K-wire loosening and some demographic characteristics (age, sex, body mass index, diabetes, smoking status) assessed at the baseline.
Questionnaires
The questionnaires that were sent out to the patients included the MOXFQ and the 12-Item Short Form Health Survey. The MOXFQ is a patient-administered measure consisting of 16 items. The translated and validated French version was used. 29 The 3 domains (walking/standing, pain, and social interaction) were summed to provide a single summary index score. 15 The questionnaires were sent by mail to all eligible patients (patients still alive and with a known address) 10±3 years after surgery.
Surgical Technique
Open reduction and internal fixation of ankle fractures were performed according to the standard principles of the AO/OTA fracture fixation. 8 After fracture fixation, syndesmosis stability was tested under fluoroscopy using the modified Cotton or Hook test. In cases where syndesmosis widening was observed, further syndesmosis fixation was performed. Before fixation, syndesmosis was reduced under direct visualization and temporarily secured with a reduction clamp or K-wires. Once adequate reduction was achieved, definitive syndesmosis fixation was performed with K-wires.
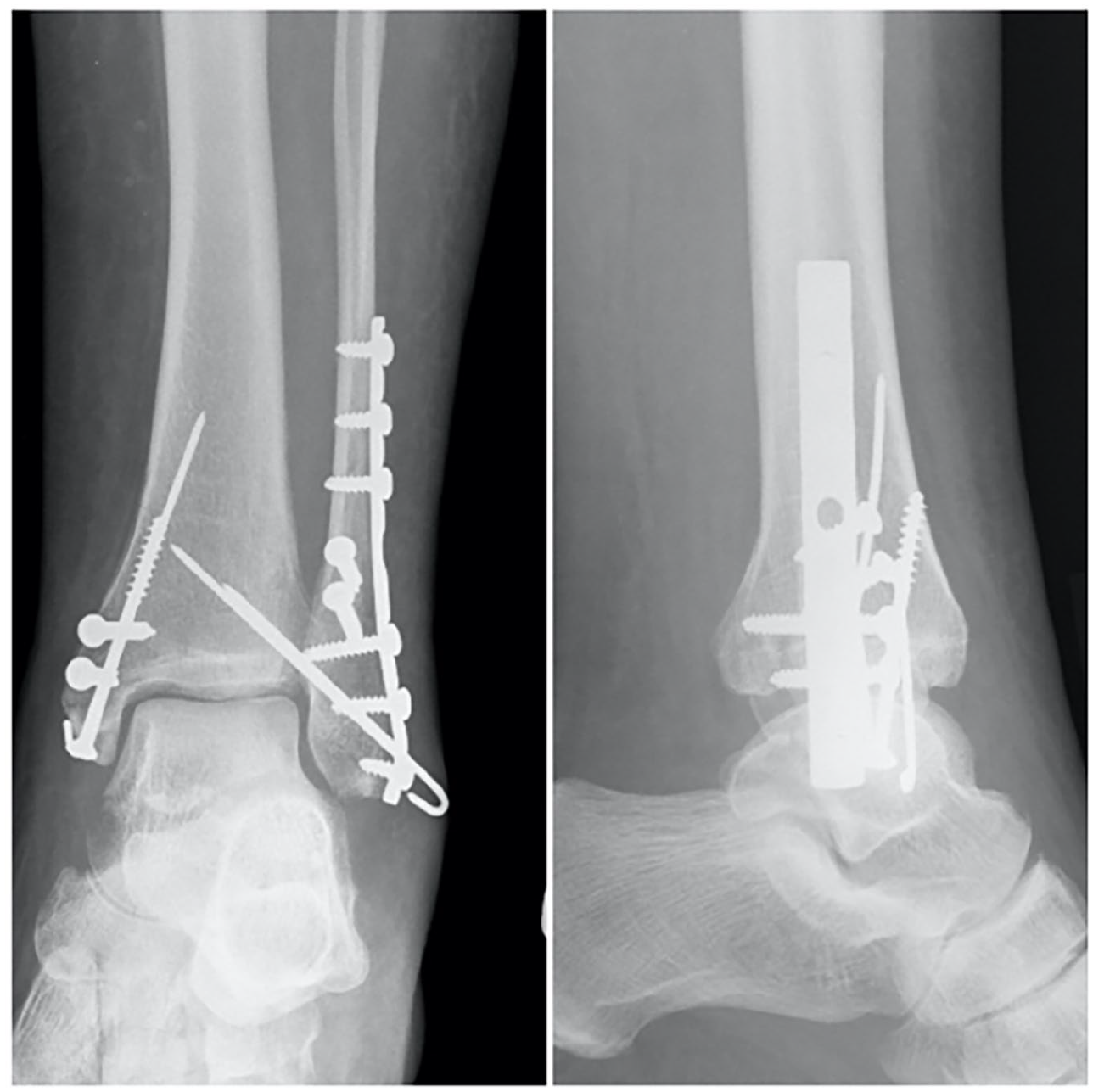
To perform this technique, two 1.6-mm Kirschner wires were inserted obliquely from distal to proximal and angled anteriorly (approximately 30°, along the intermalleolar plane) across the distal tibiofibular syndesmosis. The K-wire was then advanced to the medial tibial cortex and the distal end of the K-wire was cut, bent, and impacted on the fibula. A second K-wire was inserted parallel to the first, following the same steps. Figure 1 shows the radiographs of an ankle fracture with syndesmotic K-wire fixation. The final stability of the syndesmosis was assessed with the external rotation stress test and the Hook test under fluoroscopy. After surgery, all patients were immobilized in a nonweightbearing lower leg cast or boot for 6 weeks. Weightbearing was allowed as tolerated at 6 weeks post-operatively, and ankle range of motion exercises were then initiated, starting at 6 weeks postoperatively.

Weightbearing anteroposterior (left) and lateral (right) ankle radiograph illustrating a unimalleolar Weber B fracture with 2 K-wires used for syndesmosis fixation.
Statistical Analysis
This is a descriptive study of a series of patients treated with a specific surgical technique and long-term follow-up. Baseline characteristics and outcomes were assessed by presenting means and SDs for continuous variables and totals and percentages for categorical variables. Baseline characteristics were assessed for all patients and for those who responded to the questionnaire at follow-up to detect significant (P < .05) discrepancies.
Results
A total of 377 ankle fractures with intraoperative syndesmosis instability and subsequent syndesmosis fixation with a K-wire were included. The mean age was 46 years (range, 18-90; SD 18.5) and 229 (60.7%) were male. Baseline characteristics of the patients are shown in Table 1. Injury characteristics and fracture types are shown in Table 2. The interobserver reliability of two independent examiners in classifying a random sample of 105 radiographs showed almost perfect agreement, with an ICC of 0.894 (95% CI 0.844 to 0.928).
Baseline Characteristics of All Patients and MOXFQ Respondents.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; MOXFQ, Manchester-Oxford Foot Questionnaire.
Fracture Characteristics and Accident Type for All Patients and MOXFQ Respondents.
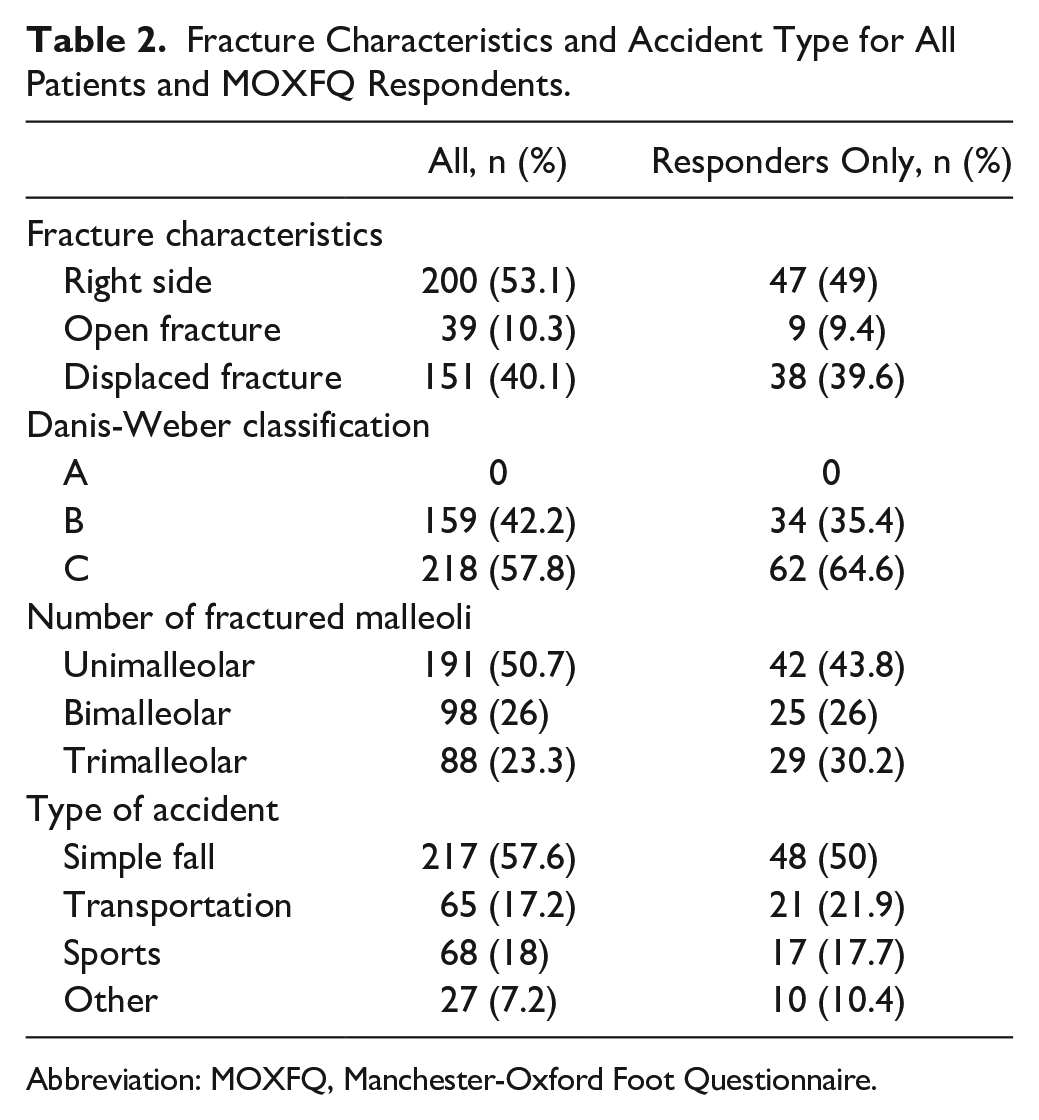
Abbreviation: MOXFQ, Manchester-Oxford Foot Questionnaire.
Complications
Acute syndesmosis fixation failure was observed in 9 patients (2%) at early stage of the follow-up at 6 weeks postoperatively in 5 cases and at 3 months in 4 cases. All had abnormal postoperative radiologic measurements, which were further confirmed by bilateral ankle CT. Seven of the 9 patients underwent revision syndesmosis fixation surgery. In 2 patients with radiographic evidence of loss of reduction, postoperative CT measurements of the syndesmosis showed an increased tibiofibular distance of 3 and 2.8 mm compared to the uninjured ankle. Revision surgery was not performed in these 2 patients. Five patients (1.3%) presented with K-wire-related complications, including 4 cases of K-wire displacement and 1 case of K-wire breakage. Of these, none presented with secondary loss of syndesmosis reduction and 4 patients underwent K-wire removal.
The secondary analysis conducted to assess potential correlations between the loss of syndesmotic reduction and/or K-wire loosening and demographic factors (age, sex, body mass index, diabetes, and smoking status) found no significant associations. An illustrative radiograph of 1 case of K-wire displacement is shown in Figure 2. A summary of complications and hardware removal rates is shown in Table 3.
Nonweightbearing anteroposterior (left) and lateral (right) ankle radiograph illustrating a bimalleolar Weber B fracture with K-wire loosening and secondary displacement.
Summary of Complications and Hardware Removal Surgery Rates.

Patient-Reported Outcomes results
Of the 377 patients, 51 died and 58 were lost to follow-up. A total of 268 patients completed a comprehensive 12-month radiographic follow-up and were eligible for questionnaire participation. Of the suspected still living patients, 94 patients (29%) completed the questionnaire, with a mean follow-up of 10.6 ± 3.0 years postsurgery (Figure 3). The 94 patients who completed the questionnaire did not differ significantly in baseline characteristics from the 377 consecutive patients operated on between 2002 and 2012. The results of the patient-reported outcome measures are shown in Table 4. The mean MOXFQ pain score was 25.9 ± 25.4, the mean function/walking score was 18 ± 24.8, and the mean social score was 13.7 ± 22.2. According to pain categories, 35 (37%) reported no ankle pain, 39 (42%) mild pain, 13 (14%) moderate pain, and 7 (7%) severe pain.

Flow chart of patients from enrolment to data analysis.
Manchester-Oxford Foot Questionnaire (MOXFQ) and 12-Item Short Form Health Survey (SF-12) Results.
Discussion
This study reports the long-term clinical results of syndesmosis fixation using 2 K-wires in patients with unstable ankle fractures in a subset of patients we were able to contact. Our results suggest that this technique provides good to excellent clinical and functional outcomes and is associated with low complication rates. To our knowledge, there is only 1 study reporting clinical outcomes and complication rates in patients with syndesmosis injuries and ankle fractures where the syndesmosis was fixed with K-wires. 14 Between 1988 and 1996, 50 patients undergoing this technique were reviewed with a mean follow-up of 8.3 years. Complications with secondary K-wire displacement were seen in 10% of patients. In our study, K-wire loosening and displacement were less common (1.3%). K-wire loosening may be explained by the fact that K-wires are flexible and the small amount of movement that occurs between the tibia and the distal fibula may cause K-wire loosening with consequent displacement. We believe that the use of quadricortical K-wires and their impact on the fibula may be helpful in preventing secondary displacement. In addition, the use of 2 K-wires provides additional stability and prevents potential loss of syndesmosis reduction in the event of K-wire loosening or breakage.
Fixation failure and loss of syndesmosis reduction can lead to widening of the mortise and further osteoarthritis. 25 Their incidence has been reported to be 10% to 16% after screw fixation and 0% to 5% after flexible fixation.10,30 Our study shows comparable results to other flexible techniques, with loss of syndesmosis reduction observed in 2.4% of patients. These results suggest that K-wires can provide stable fixation and maintain syndesmosis reduction throughout the healing process. This is supported by the biomechanical study by Peter et al 16 that compared the use of 2 K-wires inserted obliquely across the distal tibiofibular syndesmosis with the use of a 3.5-mm transverse screw. Distal joint motion and pressure contact characteristics were measured in injured and uninjured ankles. No significant differences were found between the 2 techniques, and the authors conclude that both techniques stabilize the injured syndesmotic joint equally well.
One of the main hopes with the introduction of flexible syndesmosis fixation was to avoid the need for hardware removal and reduce revision rates. Reoperation rates are found to be most of the time higher in patients with screw fixation than flexible fixation. Recent systematic reviews and meta-analyses on the use of suture button or screw showed that screw systematic removal is progressively losing appeal, because of increasing evidence of non-inferiority of on-demand removal even in case of screw breakage.10,19,30
Although on-demand screw removal is gaining popularity, the reoperation rate due to local pain, skin irritation, or limited range of motion (ROM) remains around 23% for screws 19 and between 6% and 9% for suture button implants.2,11,17,21 In our cohort, K-wire removal was performed in 4.2% of patients. The decision to remove the hardware was entirely up to the surgeon. However, we hypothesize that patient complaints may be the main motive, suggesting that this fixation may be associated with low rates of discomfort.
Concerns have been raised about the economic burden of different techniques used for syndesmosis fixation. 32 At their median cost, suture buttons are likely to be cost effective over screws, at least for symptomatic screw removal rates greater than 17.5%. 18 It was not our aim to perform a cost analysis of the use of K-wires for syndesmosis fixation. However, apart from the low removal rate, K-wires remain a very inexpensive device, available worldwide, and almost unbeatable in terms of reducing health care costs compared to other devices currently in use. K-wire fixation is an excellent solution in situations where access to other implants is economically restricted, without compromising patient outcomes.
As mentioned above, long-term functional outcomes have been reported once by Missbach-Kroll et al 14 They reported good to excellent results in 81% of patients at 8.3 years of follow-up. However, no standardized outcomes or validated questionnaires were used. In the current study, clinical outcomes were assessed with the MOXFQ and 12-Item Short Form Health Survey scores, and results showed low pain scores and excellent functional outcomes at 10 ± 3 years after the initial surgery.
This study has several limitations, mostly inherent to his retrospective design. Firstly, syndesmosis reduction was only assessed by ankle radiographs, which may limit the true incidence of loss of reduction in our cohort. Second, the radiologic follow-up timeline ends at 1 year after the index surgical procedure, whereas the principal functional outcome timeline ends up to 10 ± 3 years after surgery. Third, the high patient mobility in our urban area and the fact that our hospital is a referral trauma center in a tourist area may have contributed to the 29% response rate among suspected living patients to our questionnaire. We acknowledge that the relatively young age of our cohort of patients representing the study population, a mean of only 46 years, may make it difficult to generalize our findings to the general population, even though the technique has been used in much older patients, up to 90 years of age, and no statistically significant correlation was found between age and comorbidities and the occurrence of K-wire loosening/syndesmosis reduction loss. Moreover, the retrospective nature of the study and the lack of a control group also contribute to a lower level of evidence. Regarding the secondary analysis, which found no significant correlations between the loss of syndesmotic fixation or K-wire loosening and demographic factors, the strength of the evidence is inherently limited because of the small number of events. Further research comparing this technique with more traditional fixation techniques is warranted.
Conclusion
This is the first study to report long-term functional outcomes using a validated patient-reported questionnaire in a large series of patients with syndesmosis fixation using 2 K-wires for unstable ankle fractures. In the subset of patients we were able to contact in long-term follow-up, this technique was associated with apparent low rates of syndesmosis fixation failure, low pain scores, and very good functional outcomes at follow-up. Furthermore, the availability and low cost of these implants make this technique a cost-effective solution for syndesmosis fixation without compromising stability and patient outcomes.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241310425 – Supplemental material for Long-term Clinical Outcomes After Syndesmosis Fixation With K-wires in Ankle Fractures With Syndesmotic Instability
Supplemental material, sj-pdf-1-fao-10.1177_24730114241310425 for Long-term Clinical Outcomes After Syndesmosis Fixation With K-wires in Ankle Fractures With Syndesmotic Instability by Diogo Vieira Cardoso, Filippo Pierobon, Anne Lübbeke-Wolff and Victor Dubois-Ferrière in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the local Ethics Committee. Informed consent was obtained from all subjects.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.