
Abstract
Introduction
Tennis elbow (TE) or lateral elbow tendinopathy (LET) is one of the most common conditions that affect the muscles that originate from the lateral side of the elbow joint. It is also most common among tennis players; thus, it's a common name. It is also called lateral epicondylitis or lateral elbow joint pain.1,2 This condition typically arises from an extensor muscle overuse injury, which is typically brought on by excessive, rapid, repetitive motions of the wrist and forearm. 3 This fast contraction of these muscles causes micro-damages in their common origin, which leads to pain and local inflammation. 3 This pain may also extend to the posterior aspect of the forearm and hand, which affects grip strength. 4 The term LET is suitable for clinical diagnosis when this denotes a painful overuse of common extensor tendon disorder. It includes confined pain from the common extensor origin of the wrist muscles at the lateral epicondyle with pain during repetitive gripping activities. Activating factors for pain symptoms are variations of equipment, technique, or higher intensity in activity. 5 In several earlier investigations, female gender, dominant-side involvement, manual labor, ipsilateral rotator cuff tear, and positive and prior smoking history were thought to be related to lateral epicondylitis.6,7
Electromyography (EMG) is one of the functional tools that detect the muscle function or dysfunction. Assessing functional recovery in LET may be possible by tracking extensor carpi radialis (ECR) activity. 8 Firstly, most subjects identified as LET patients can be efficiently treated with traditional treatment, medication, and physical rehabilitation. 9 Sometimes, it is a self-control process in which more than 90% of subjects will recover within 1 year without surgical interference.10,11 The most efficient prescribed treatments by physiotherapists and occupational therapists are the discontinuation of activities that exacerbate this condition and the performance of a gradual home exercise routine. 12 In addition, physical rehabilitation programs, such as stretching, 4 deep friction massage, 13 strengthening exercises, and physic-thermal modalities,9,14 may have a satisfactory effect on the management of TE.
One of the novel techniques used for the rehabilitation of LET is the use of supportive devices like taping and bracing.4,15,16 The well-known mechanism of Kinesiotaping techniques (KTT) involves the support of the joint, muscle, and fascia at the site of inflammation and tends to improve the recovery of LET. This facilitates a pain-free range of motion (ROM). 17 It has been proposed that Kinesiotaping (KT) supports weak muscle groups, corrects joint abnormalities, improves blood and lymph circulation, delivers proprioceptive input, and decreases pain and muscle spasms. 18 In addition, kinesiotaping reduced pain intensity, restored grip strength, and improved functionality in subjects with lateral epicondylitis experiencing rehabilitation. 19 Furthermore, KT may be most effective when used as an adjunctive treatment, possibly by improving joint ROM, muscular endurance, and motor control. 20
The counterforce brace (CFB) is another new technique for managing LET.15,21 The CFB tends to reduce the amount of muscle tension at their insertion by moving the tension farther down the forearm. This tends to reduce muscle inhibition by pain and improve grip strength. 22 So, both the KTT and CFB are very effective in the management of LET accompanied by traditional physical therapy treatment, but there is limited literature concerning the more effective treatment methods for the improvement of pain and strength in subjects suffering from LET. Consequently, this study aimed to explore and compare the effect of the elbow CFB versus KTT on the degree of pain reduction and the electrical activity improvement of the dominant forearm muscles (wrist flexors and extensors) of females suffering from chronic LET. Our null hypothesis states that there was no statistically significant difference between the effects of CFB and KTT on pain intensity and wrist flexor and extensor myoelectric activities.
Methods
Participants
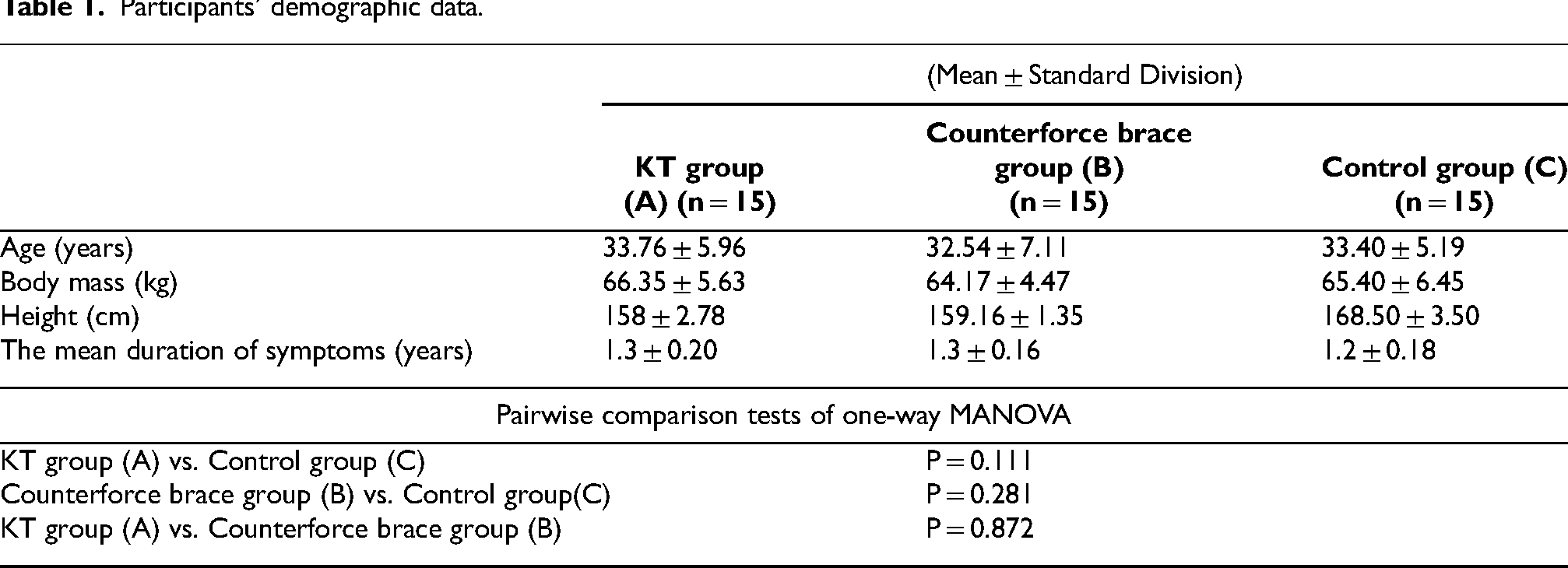
A total of 45 females clinically diagnosed as having chronic tennis elbow participated in the current study. All female subjects were assigned randomly into three groups of equal numbers (15 females in each group) using the sealed envelope method. Each patient selected a random envelope and handed it to the physical therapist. The demographic features of the three groups are shown in Table 1. All groups received a physiotherapy program for the forearm muscles for 12 sessions over 4 weeks.
Participants’ demographic data.
Experimental group A (KT Group) received the traditional physiotherapy program in addition to Kinesiotaping. Group B (CFB Group) received the physiotherapy program in addition to the counterforce brace. Group C (Control Group) received the physiotherapy program only. The inclusion criteria include; 1) Age was limited between 25 and 40 years. 2) All LET cases were diagnosed and referred by an orthopaedist. 3) Activities involving repeated wrist extension exacerbated their symptoms. 4) All cases did not demonstrate clinical signs or symptoms of a current elbow or wrist condition other than lateral epicondylitis. 5) The score of LET pain extended from 6 to 8 on the 10-cm VAS due to inflammation and microdamage of the tendons. 5) They were medically stable and did not take any medications or analgesics for at least the previous 3 months. 7) None of the female subjects engaged in any particular activity except ordinary household tasks.
The participant was excluded if there were any clinical signs and symptoms of evoked referred pain from the trigger point, proximal and distal joints or muscles, ligamentous injury, joint dislocation or subluxation, and latest fracture and surgery in the hand, forearm, or elbow. In addition, if the participants engaged in any specified physical activities other than household tasks, they were excluded. Pain intensity and EMG of patients’ wrist extensor and flexor muscles were measured for the three groups as study outcomes. All participants signed an informed consent form upon their agreement to participate in the study before testing and to publish these case details. The study was approved by the Research Ethical Committee of the Faculty of Physical Therapy, Cairo University (P.T.REC/012/004562).
Study design
This pre-test, post-test control group study was conducted. The evaluators who gathered the data were blinded to the groups’ allocation. Participants in three groups were examined before and after 12 treatment sessions (according to the treatment type administered for each group) over 4 weeks to determine the pain level and myoelectric activity of wrist flexors and extensors.
Instrumentations
A Visual Analogue Scale (VAS) was used. VASs involve a line, usually 10 cm long, ranging from no pain or discomfort (zero) to the worst pain that one could feel (10). 23 The subject was in a relaxed position then he was given the appendix, which contains VAS. The subject was instructed to place a vertical mark on the line that indicated her pain. In addition, a computerized electromyography device, a two digital channel electro-myogram (EMG) instrument (Neuro-EMG-Micro, Neurosoft, Ivanovo, Russia), was applied to detect myoelectric signals from the forearm muscles (wrist extensors and flexors). The device consists of a screen, keyboard, printer, and computer processing unit. The device contains two electrically insulated amplifier networks with an impedance of fewer than 100 m ohms and a sensitivity of up to 4000 UV/0.5. The amplifier achievements of up to ten traces on display with firmness of 1000 points per trace were available.
Moreover, a ground electrode and two silver surface recording electrodes (active and passive) were used. Before the apparatus was used, the commissioned company calibrated all tested parameters. The BB kinesiotape (IC: 87683491, Made in Korea) is 100% cotton latex-free, hypoallergenic, non-restrictive, has a water-resistant coating, and is easy to apply. It is thin and has high elasticity, enabling the tape to extend to 20%–40% of its original length. The tape is 5 cm in width and 5 m in length. The sensitivity test was examined before applying kinesiotape.
Procedure
The study was conducted in the lab of the Faculty of Physical Therapy, Cairo University. in the period from 12/1/2021 to 20/2/2021. All patients received a short-lived orientation about the type and importance of the study, the devices used, and the tasks to be done. Each patient's body mass and height were recorded from the height and weight scale. Measurements were taken from the three groups before and 4 weeks after.
The subject was asked to sit in a comfortable position. The skin over the wrist and forearm was cleaned carefully using alcohol webs and dehydrated with clean, dry cotton. This method was repeated several times till the skin became red, aiming to decrease the skin impedance. Great attention was paid not to scratching the area of skin below the recording EMG electrodes. The measurement tape was used to detect the examined muscles’ motor points that were striking the skin with a marker with a non-permanent ink. The maximum isometric for each examined muscle contraction was necessarily detected for the normalization of EMG activities to compare the examined muscle contraction between the participants. To confirm that the maximum amount of effort was delivered through the total measuring process, verbal inspiration, and visual feedback were provided for each participant. The position of the electrodes was clearly defined using palpation while the subjects were instructed to extend and flex their wrists against manual resistance. The location of the wrist muscles’ motor point was detected and specified by Delagi and Perotto. 24 As the kinesiology and EMG association recommended, electrodes were located on the midpoint of the muscle belly with the recognition of the surface in the same orientation as the muscle fibers. The inter-electrode space between the electrodes was 2 cm.
For the placement of the electrodes on wrist extensors, a line was drawn from the lateral humeral epicondyle to the radial styloid process. 25 The ground electrode was placed at the radial styloid process. The active electrode was positioned over the muscle belly, mid-way between the motor point and the tendinous origin of the wrist extensors the following palpation during resisted wrist extension. The passive electrode was 2 cm from the active electrode (Figure 1).

The electrodes’ placement for wrist extensors.
On the other hand, a line was detected and drawn between the medial humeral epicondyle to the ulnar styloid process so that the electrodes were directed parallel to this line. The active electrode was placed over the most prominent part of the muscle mid-way between the motor point and the tendinous origin of the wrist flexors the following palpation during resisted wrist flexion. The passive electrode was 2 cm from the active electrode, 25 as shown in Figure 2.
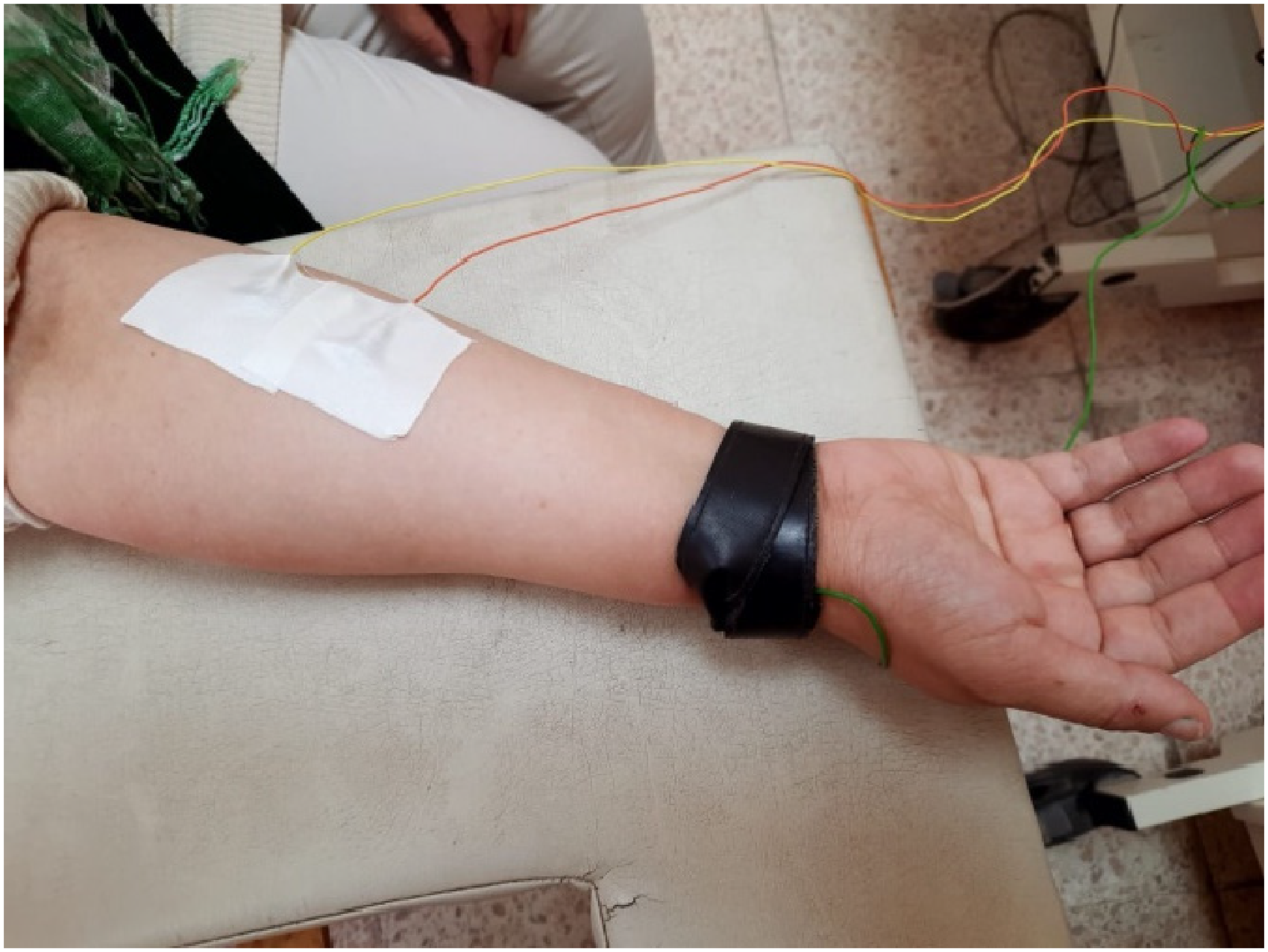
The electrodes’ placement for wrist flexors.
The EMG responses were visually checked using an amplitude-time display of the EMG recordings to ensure that obvious artifacts were excluded. Motion artifacts or electrode noise were subtracted before quantification of EMG variables. 26 Data was tested at 1000 Hz and cleaned with a 20–450 Hz band pass filter. The peak amplitude value was detected from the three trials of wrist extensor and flexor contraction against maximum resistance. The average peak amplitude of the three trials of maximum isometric contraction for wrist flexors and extensors was then detected and normalized as stated by the following equation:
Subjects in Group A were fastened with KT in return to Kenzo Kase's Kinesiotaping Manual. 27 The tape was extended from the elbow joint to the wrist joint. The strip was applied from the origin to the insertion of the examined muscles while the muscle to be taped was put in a stretched position. One knowledgeable physiotherapist who successfully completed a Kinesio tape application training course applied the tape in all cases. From the origin (2 cm above the common extensor and flexor origins) to the level of the radial and ulnar styloid processes, the tape was applied as shown in Figure 3. The beginning of KT was fixed at the origin of the muscles in the relaxed state. The tape was rubbed in the stretched muscle position with 10% tension above the belly of the muscle to the muscle insertion at the wrist. Over the course of 4 weeks, a single-colored KT roll with the same tension was used and replaced in the same way every 48 h unless it was necessary to change it. For taping, each patient's forearm was placed in a relaxed position while resting it on a taping table, as shown in Figure 3.

KT positions for wrist flexors and extensors.
Moreover, a commercially available elbow counterforce brace was used with subjects in Group B. It was made of an adjustable high-score closed-cell neoprene sponge enclosed with high elastic polyester fibers on each side. Also, it had a strap fitted on the wrist muscles’ muscle belly. The physiotherapy program was given for the three groups, which consisted of ultrasonic with an intensity of 0.8 W/cm2 applied over the common wrist extensor tendons in a circular movement for 7 min, which helps for pain reduction 28 ; superficial heating was done using infrared radiation as a source of superficial heating for 20 min, 29 deep friction massage over the extensor tendons for 10 min, 30 and exercises were in the form of active flexion and extension of the elbow for five sets of ten repetitions. 31 The physical therapy program was conducted three times per week for 4 weeks.
Data analysis
First, a pilot study on three patients was done, and its data were used to calculate the required sample size through the power analysis equation. The required sample size was calculated using G*Power software 3.1.9.2 with a confidence level of 95%, a power of 80%, and a moderate effect size of 0.3. The primary outcome measures were the pain level and EMG peak amplitude of the wrist extensor and flexor muscles. The result of the sample size calculation detected that the least sample size of 40 contributors was essential for the current study. Data for the 45 women who accomplished the study to the end were then analyzed. Figure 4 is a flow chart of participants’ involvement in the study.
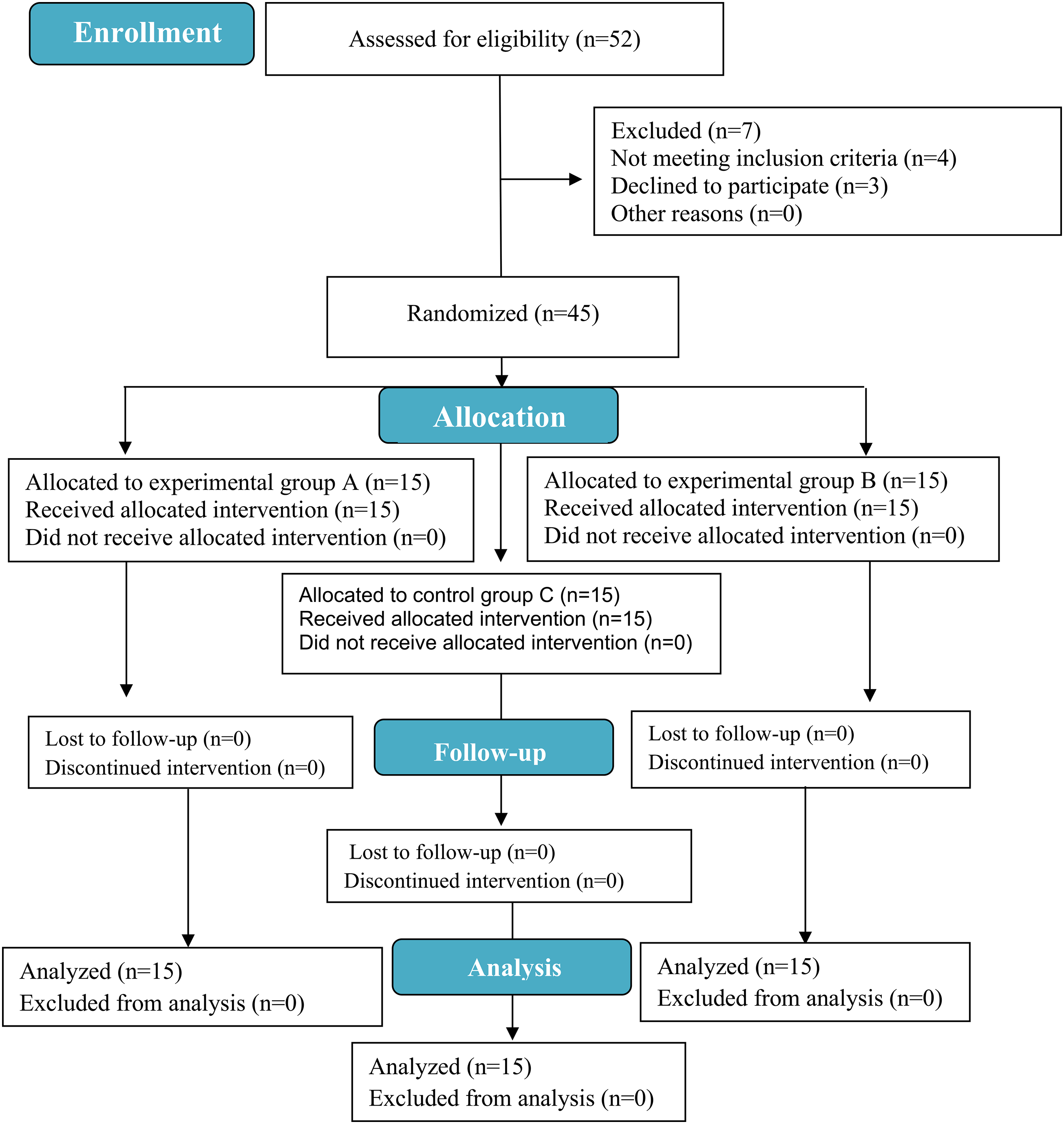
Flow chart of the participants’ involvement.
A 3 × 2 mixed design MANOVA was used to evaluate the effect of KT versus counterforce brace on pain level (measured by VAS) and EMG peak amplitudes of wrist flexor and extensor muscles in patients with tennis elbow. The study involved two independent variables. The one independent variable was the examined groups (between participant factors) which included three groups; experimental group A (KT group), experimental group B (counter force brace group), and control group C. The other independent variable was the examination time (within participants’ factor with two examination times); examination before intervention (pre-testing) and examination after intervention (post-testing). The three dependent variables were scores of the VAS scale and EMG peak amplitudes of wrist flexor and extensor muscles. All statistical measures were done using IBM statistical package for social sciences (SPSS) version 20. The significance level for all statistical tests was set as P < 0.05.
Results
A total of 52 women with tennis elbows were assessed for eligibility. Seven participants were excluded from the study; four women did not meet the inclusion criteria, and three withdrew from the study. After excluding patients dropping out and those who did not meet the inclusion criteria, 45 subjects were included in the study. They were assigned to three equal groups of 15; tested group A (n = 15), tested group B (n = 15), and the control group C (n = 15). The normality test (Shapiro-Wilk test) showed no statistically significant difference in participants’ demographic data (age, body mass, and height) in the three groups. Also, Levene's test of equality of variance showed no statistically significant differences. The mean and standard divisions of demographic variables were detected for each group, and the Pairwise comparison tests of one-way MANOVA showed no statistically significant differences in demographic data among the three groups, as shown in Table 1.
The 3 × 2 mixed design MANOVA showed statistically significant differences in pre-post examinations (within subjects’ comparisons) for each group in the VAS and myoelectric activity of wrist flexors and extensors. The mean values of pain levels were significantly reduced in the two experimental groups, while they increased in the control groups. On the other hand, the mean values of the pre-test and post-test myoelectric activities of wrist flexors and extensors tend to increase in each tested group.
Furthermore, the 3 × 2 mixed design MANOVA showed no statistically significant differences in the pre-treatment intervention among the three groups, while the post-treatment intervention showed a statistically significant difference in VAS between the experimental groups’ A and C in favor of group A, and there were no significant differences in the myoelectric activities of wrist flexors and extensors between these groups. On the other hand, there were statistically significant differences in post-treatment intervention in the VAS and the myoelectric activities of wrist flexors and extensors between groups B and C in favor of group B. Finally, there were statistically significant differences in post-treatment intervention in the VAS, the myoelectric activities of wrist flexors, and extensors between groups A and B in favor of group B (Table 2).
Results of the visual analogue scale (VAS) and wrist flexors᾿ and extensors᾿ EMG peak amplitudes among the three tested groups.
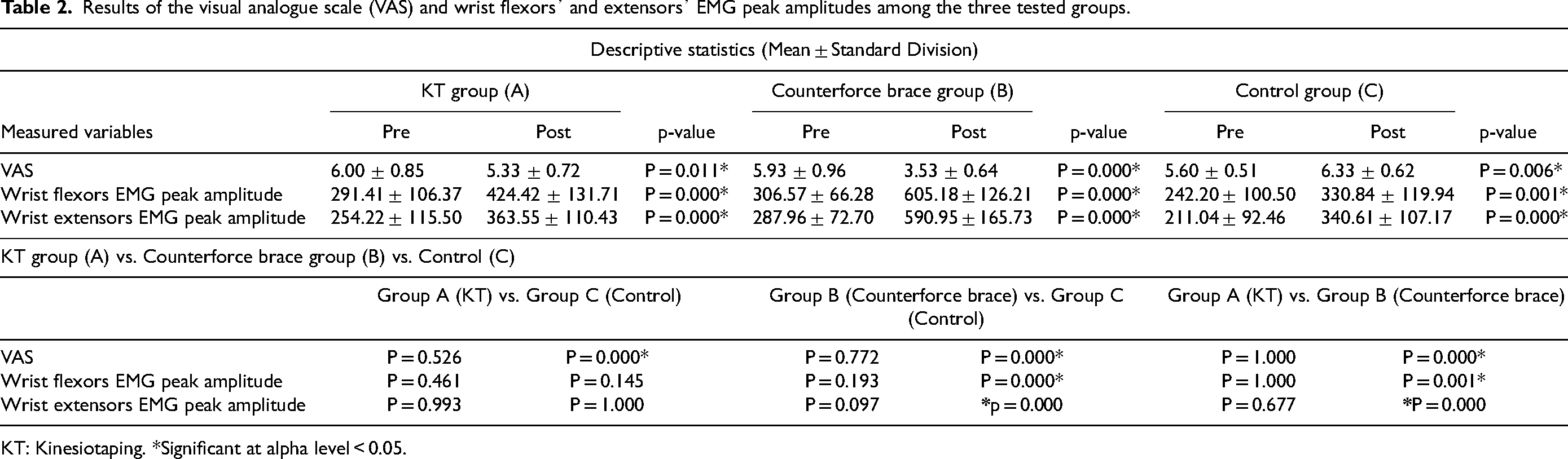
KT: Kinesiotaping. *Significant at alpha level < 0.05.
Discussion
The results of the current study show statistically significant differences in the pre-post intervention in the three groups. Moreover, a statistically significant reduction of pain was detected in groups B and A compared to group C and between groups B and A in favor of Group B. In addition, statistically significant increases in the myoelectrical activity of wrist flexor and extensor muscles were detected between groups B and C and between groups B and A in favor of group B. This indicated the superiority of using the counterforce brace to reduce the pain level and increase the myoelectrical activity of wrist flexors and extensors in tennis elbow pathology in comparison with using KTT. The results of this study agree with the result of a study conducted by Shaheen et al., 32 which proves that KT is better in the treatment of tennis elbow than the conventional therapy treatment in male and female patients suffering from lateral epicondylitis (LE). In addition, a study conducted by Schneider and Rhea 33 and applied to 14 healthy tennis players showed improvement in the muscle strength of forearm extensors. Several previous studies have confirmed the importance of KTT along with exercise in the management of lateral epicondylitis,34–36 although other studies reported a lack of strong evidence underlying the mechanism of KTT in relieving the symptoms of LE and there is still debate regarding the effect of KTT in the treatment of LE.37,38
Moreover, a study performed on 45 subjects with tennis elbows using the forearm brace and elbow taping with conventional physical therapy programs reported the potential effect of the forearm brace with conventional physical therapy programs relative to elbow taping in reducing pain, improving the grip strength, and enhancing functional performance. This result supports the results of the current study, in which the counterforce brace in the current study shows a superior effect to the KTT in reducing the pain and increasing the myoelectrical activity of wrist flexors and extensors. 39
Also, a systematic review confirmed that orthotics could be acceptable for treating the signs and symptoms of lateral epicondylitis, such as reducing pain and improving grip strength, ROM, and proprioception. 40 Besides, the study's results on patients with tennis elbows using the CFB and placebo groups showed greater pain reduction (pain frequency and intensity) and overall elbow functional activities after using the CFB. 41
On the other hand, Shamsoddini et al., 15 using the tapping technique and CFB, report results that conflict with those of the current study, while the results of this study showed greater improvement in pain reduction through the use of the tapping technique than the CFB, but no significant difference in grip strength or wrist extension force between both methods. Shamsoddini et al. 15 used the hand-held dynamometer for evaluation instead of EMG, as done in the current study. In addition, adhesive and non-elastic taping were used in this study instead of KTT. Otherwise, a study conducted by Phadke and Desai 42 reported an equal effect of KTT and CFB in the management of LE through reducing pain, improving grip strength, and reducing disability.
The most surprising result in our study was the control group with physiotherapy alone, without the use of a KTT or counterforce brace, resulted in a statistically significant increase in the VAS rather than a decrease in pain, although the myoelectrical activity of wrist flexor and extensor significantly increased. This suggests that continuing a physiotherapy program without using any supporting devices (supports the elbow muscles while moving, reducing stress and soreness as a result), like a KTT or counterforce brace, may have no or adverse effects, particularly with regard to pain exacerbation. 43 Additionally, the elbow joint's biomechanical stresses are decreased by using supporting devices when the extensor carpi radialis brevis muscle is being unloaded and restrict the patient to avoid the activities that cause pain. 44 Although physical therapy may have the potential to decrease pain immediately after treatment (short-term pain relief), there is insufficient data to support any long-term clinical effects of physiotherapy alone.45,46 Rehabilitation should take a multimodal approach in order to fulfill individual requirements and achieve long-term goals. 22 Furthermore, the lack of patient education regarding joint protection strategies and lifestyle changes to avoid painful activities from our study may have had an impact on the findings. 47 Further investigation is needed to clarify this point as there is still a definite need for evidence-based recommendations for physiotherapists treating lateral elbow tendinopathy.
According to the results of the current study and earlier research, it can be hypothesized that the CFB has a superior effect in reducing pain and improving the electrical activity of wrist flexors and extensors than the KTT in the cases of lateral elbow tendinopathy. Also, CFB and KTT were better than the conventional physical therapy treatment alone for tennis elbow cases. Our study has some obvious limitations. As the current study only included a small sample of female subjects, our findings could not be generalized to males. Furthermore, long-term studies are required to confirm the treatment interventions’ true effectiveness because the treatment interventions’ duration was short in the current study (only 1 month). In addition, further research studies are required to determine the hand grip strength and functional score in improving the functional performance in addition to the myoelectrical activities of wrist flexors and extensors following the use of supporting devices in conjunction with conventional physiotherapy programs. Additionally, the Patient-Specific Functional Scale was not used in the current study to assess the patient activity level, hence it is advised that similar scales or questionnaires should be used in future studies to determine the patient's activity level. Moreover, the physiotherapy program should incorporate instructions on self-joint protection techniques.
Conclusion
Although there were statistically significant improvements in wrist flexors and extensors in the control group due to the physiotherapy treatment program, we detected statistically significant better pain reduction and increased muscle activities of wrist flexors and extensors when using the CFB or KTT compared to the traditional physical therapy treatment alone. Also, the patients with lateral elbow tendinopathy might experience a superior result from the CFB when compared to the KTT if combined with a physical therapy program in terms of pain relief and improved muscular activity of wrist flexors and extensors. Therefore, for better treatment outcomes, we recommend adding CFB to traditional physical therapy treatment to manage tennis elbow cases.
Footnotes
Acknowledgments
The authors appreciate the great efforts exerted by all participants during the conduction of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.