
Abstract
Background:
Lateral elbow tendinopathy, also known as “tennis elbow” or “lateral epicondylitis,” is a common disease leading to pain in the lateral side of the elbow and disability during hand gripping. A counterforce brace is one of the most conventional treatments. However, its effects on outcomes remain inconclusive.
Objectives:
To investigate the effects of counterforce braces on pain in subjects with lateral elbow tendinopathy. Grip strength was reviewed as a secondary outcome.
Study design:
Systematic review and meta-analysis of randomized controlled trials.
Methods:
PubMed, Embase, Scopus, Web of Science, CENTRAL, PEDro, ProQuest, RECAL, and RehabData were searched from January 1, 1995, through June 15, 2019.
Results:
Seventeen studies were included with a total of 1145 participants. A small improvement in pain over the short term (standardized mean difference −0.02; 95% confidence interval: −0.85 to 0.80) and a moderate-to-large improvement in pain in subjects 45 years or younger (standardized mean difference −0.86; 95% confidence interval: −2.45 to 0.72) in favor of the brace versus physiotherapy interventions were found. In contrast, over the long-term physiotherapy interventions (standardized mean difference 1.17; 95% confidence interval: −0.00 to 2.34), wrist splint (standardized mean difference 0.35; 95% confidence interval: −0.07 to 0.76), and laser therapy (standardized mean difference 0.58; 95% confidence interval: −0.44 to 1.59) had better effects on pain improvement versus the brace.
Conclusion:
The results indicated that physiotherapy interventions compared to counterforce braces have better effects, especially over the long-term. However, counterforce braces may have better effects on pain in younger people (<45 years old) over the short term (<6 weeks).
Clinical relevance
The results suggest that counterforce bracing is a reasonable strategy to alleviate pain over the short term. However, the subgroup analysis suggests that factors such as age may have a role in their effectiveness.
Background
Lateral elbow tendinopathy (LET), also known as “tennis elbow” or “lateral epicondylitis” is a common disease leading to pain in the lateral side of the elbow and decrease in hand grip strength. 1 It is estimated that the prevalence of LET is 1.3% and 1.1% among men and women, respectively, 2 and 5%–10% among tennis players. 3 LET also reduces productivity, suggesting that it also has an economic impact. 4 Overload and repetitive excursion of the wrist extensor muscles, specifically the extensor carpi radialis brevis (ECRB) and the extensor digitorum communis (EDC), which originate on the lateral epicondyle of the humerus, are generally considered as the pathophysiology of LET.5,6
Although LET is commonly self-limiting and a wait-and-see policy is frequently adopted, 7 many treatment strategies, including physiotherapy exercises, acupuncture, extracorporeal shock-wave therapy (ECSW), laser therapy, dry needling, orthoses, injections, and surgery, have been used to relieve pain, alleviate inflammation, and improve grip strength.6,8,9 Conservative treatments result in clinical improvements in 75%–90% of subjects with LET. 10 A counterforce brace, which is also known as a “proximal forearm band” or “epicondylitis bandage,” is one conventional treatment.11,12 However, its effects on relevant outcomes remain inconclusive.
Two systematic reviews13,14 have been conducted with regards to the effects of orthoses in subjects with LET. Published in 2002 and 2004, these studies reviewed the available evidence qualitatively and reported inconclusive results based on the limited number of studies with heterogeneous methodologies. Since then, a number of randomized controlled trials (RCTs) have been published on this topic with more consistent methodologies.
To date, no systematic review and meta-analysis has been conducted on RCTs evaluating the effects of counterforce brace on pain in subjects with LET. The primary aim of this investigation was to determine the effects of counterforce braces on pain in subjects with LET. A secondary aim was to examine the effects of counterforce braces on grip strength.
Methods
This systematic review and meta-analysis was reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 15 Furthermore, the AMSTAR 2 appraisal tool 16 was used to promote the quality of reporting. The protocol for this review was registered in the PROSPERO database (registration number: CRD42019133024).
Search strategy
PubMed, Embase, Scopus, Web of Science (WoS), Cochrane Central Register of Controlled Trials (CENTRAL), Physiotherapy Evidence Database (PEDro library), ProQuest, RECAL database, and Rehab Data were searched from January 1, 1995, until June 15, 2019. Based on our preliminary findings, there are no relevant RCTs before 1995; therefore, we used 1995 as the search start date. The search strategy was developed using the population and intervention components of the PICO (Population, Intervention, Comparison, and Outcome) method. Medical subject headings (MeSH), free-text words, and the Emtree thesaurus were used to select the relevant terms. Search strings were first developed for PubMed (Supplemental Table 1) and then adjusted for use in the other databases. The search process was conducted by one reviewer (S.SH) with no language restriction considered. In addition, Google Scholar, OpenGrey, F1000Research, and registry databases such as World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP), ClinicalTrials.Gov, and ISRCTN.com were searched to find gray literature and unpublished data. Manual searching of key journals (Journal of Hand Therapy, Journal of Orthopaedic & Sports Physical Therapy, Journal of Shoulder and Elbow Surgery, Prosthetics and Orthotics International, and The American Journal of Sports Medicine) and the reference lists of relevant reviews and included studies was also conducted.
Eligibility criteria
The following criteria were used to determine study eligibility: (1) RCTs (either crossover or parallel designs); (2) adult subjects (greater than 18 years old); (3) reported pain scores in both intervention and comparison groups; and (4) studies in which subjects treated with a counterforce brace were compared to other interventions (physiotherapy interventions, other orthoses, laser therapy, or sham). Exclusion criteria were as follows: (1) clinical trials without a control group; (2) other study designs (observational studies, case series, case reports, trial protocols, abstracts, or theses with an insufficient description of findings); (3) in vitro studies; (4) evaluation of the effects of a counterforce brace on healthy subjects; (5) subjects who suffered from chronic, rheumatologic, or psychiatric diseases; (6) subjects with fracture or dislocation in the affected upper limb; and (7) subjects with a history of elbow surgery.
All of the search results were imported into EndNote X7 software (Thomson Reuters, New York, NY, USA). After removing duplicate references, two reviewers (S.SH and M.J.) independently screened the remaining studies based on titles and abstracts. After identifying potentially suitable studies, two reviewers (S.SH and M.J.) initiated the process of selecting eligible studies based on the predefined criteria. Any disagreement was resolved through discussion between the two reviewers (S.SH and M.J.) and consultation with the third reviewer (S.T.H.).
Data extraction
Data were independently extracted by two reviewers (S.SH and M.J.). Any disagreement was resolved through discussion and consultation with the third reviewer (S.T.H.). Data extracted from eligible studies included: (1) first author’s name; (2) country; (3) publication year; (4) study design; (5) mean age of each group; (6) gender of subjects; (7) sample size; (8) mean and standard deviation (SD) of outcomes of interest for each group; (9) disease duration; (10) type of intervention; (11) type of comparison; (12) follow-up duration; (13) outcomes and measurement tools, and (14) funding source. When the primary outcome data were not complete, the corresponding authors of those specific studies were contacted by e-mail to request the unpublished information. Furthermore, when two studies published information from the same population, we only considered the study with the data in which we were interested. If the data were expressed as figures or plots, WebPlotDigitizer ( https://automeris.io/WebPlotDigitizer/ ) was used to extract the outcome data.
Risk of bias assessment
Two reviewers (S.SH and M.J.) independently evaluated the risk of bias of the included studies using the Cochrane Risk of Bias Tool. 17 As with other steps, disagreements were resolved through discussion with a third reviewer (S.T.H.) if necessary. Risk of bias assessment was conducted based on six of the seven domains, specifically: random sequence generation; allocation concealment; blinding of outcome assessment; selective reporting; incomplete outcome data; and other bias. In orthotic interventions, it is typically difficult to blind the participants and personnel; thus, this domain of the tool was not considered relevant to risk of bias assessment. Moreover, the second question of the Verhagen quality assessment tool, 18 that is, “were the groups similar at baseline regarding the most important prognostic indicators?” was used instead of the “other bias” domain. 19 In each domain, the risk of bias was evaluated based on the criteria indicated in the Cochrane handbook, 17 and the response for every domain given as “high risk,” “low risk,” and “unclear risk” of bias. The overall methodological status of each study was as follows: “good,” one of the criteria was unclear; “fair,” one or two criteria were high risk; and “poor,” more than two criteria were unclear or high risk.
Statistical analysis
For quantitative analysis, the overall effect was calculated as the standardized mean difference (SMD) and 95% confidence interval (CI) between the counterforce brace and comparison intervention using a random-effects model with the DerSimonian and Laird method. 20 Due to the sample size in some studies being less than 20 in each group, SMD (Glass’s Δ) was used. 21 When the outcomes of interest were reported as a median and interquartile range (IQR), the mean and SD were calculated using the method proposed by Hozo et al. 22 To facilitate the interpretation of pooled estimates and to determine the minimal clinically important difference (MCID), effect sizes were described as small (up to 0.2), moderate (0.2–0.5), large (0.5–0.8), and very large (greater than 0.8). 23 Cochran’s Q-test and I2 statistics were used to assess statistical heterogeneity across studies, with values characterized as low (0%–25%), moderate (25%–50%), and high (50%–100%). 24 Subgroup analysis was used to explore the source of heterogeneity based on potential available variables such as: (1) age (⩽45 and >45); (2) random sequence generation (“low risk” and “high risk”); (3) allocation concealment (“low risk” and “high risk”); and (4) blinding of outcome assessment (“low risk” and “high risk”). Sensitivity analyses were used to evaluate the influence of each individual study on the pooled SMDs using the jackknife method (leave-one-out method). 25 Publication bias was investigated by the Begg and Mazumdar rank correlation test and Egger’s regression method. 26 In addition, the Duval and Tweedie “trim and fill” analysis was used to detect the potential influence of publication bias. 27 The funnel plot could not be used because the number of included studies was limited for each comparison (<10). All analyses were conducted using STATA 13.0 (StataCorp LP, College Station, TX, USA).
The GRADE approach
Overall evaluation of the evidence relating to the primary and secondary outcomes was conducted using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach. 28 The following six criteria were evaluated: publication bias, effect size, risk of bias, imprecision, indirectness, and inconsistency. GRADE ranking is categorized as very low, low, moderate, and high.
Results
Study selection
The PRISMA flowchart (Figure 1) summarizes the results of the search strategy and screening. The initial search strategy resulted in a total of 1224 studies; 429 studies remained for screening after removing duplicates. After screening based on title and abstract, 79 studies were selected for full-text evaluation. Finally, 17 RCTs3,29–44 were considered in the final synthesis. However, one study 3 was removed from the meta-analysis due to categorical data.
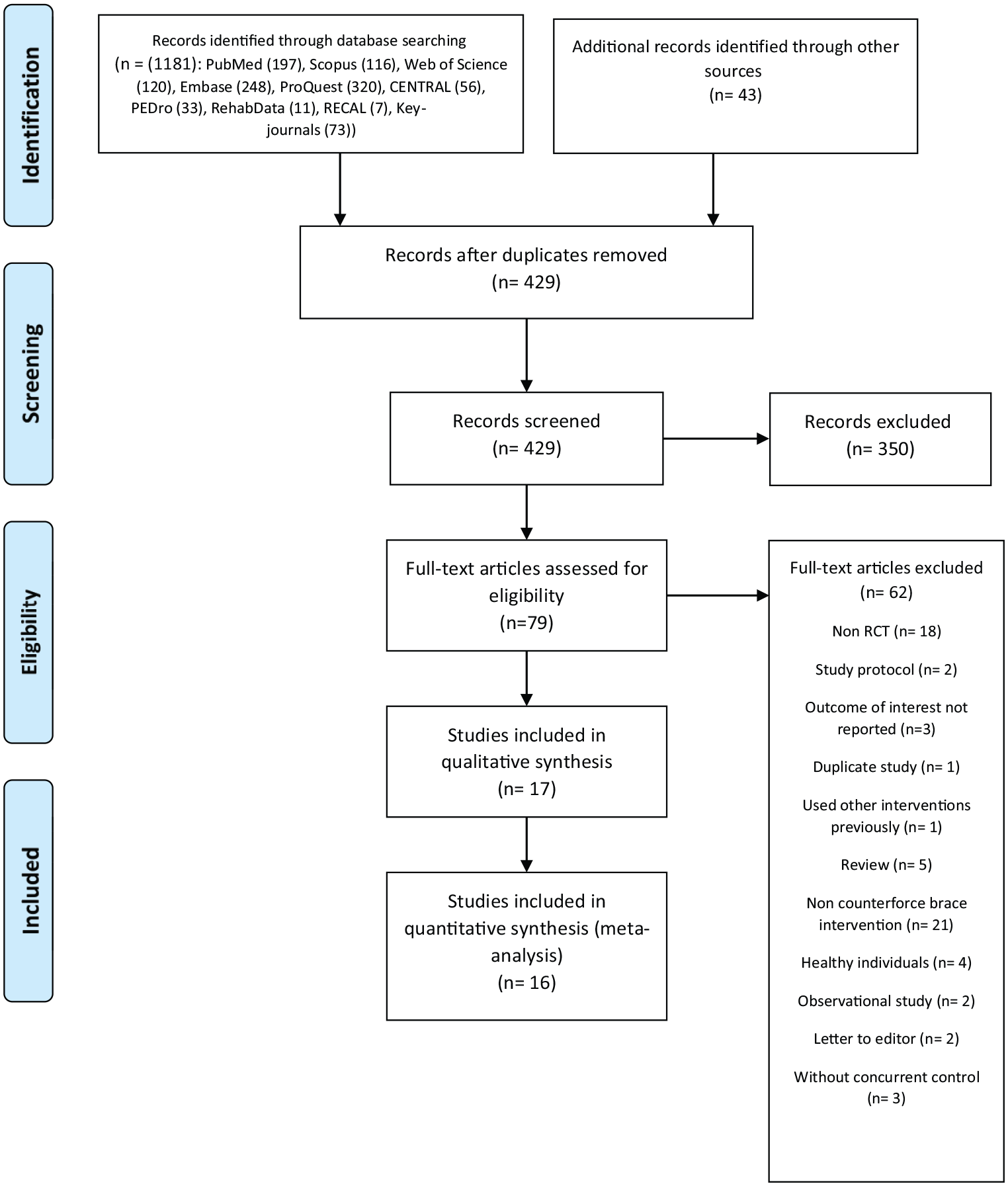
PRISMA flowchart.
Supplemental Table 2 lists the excluded studies alongside the reason for exclusion.
Study characteristics
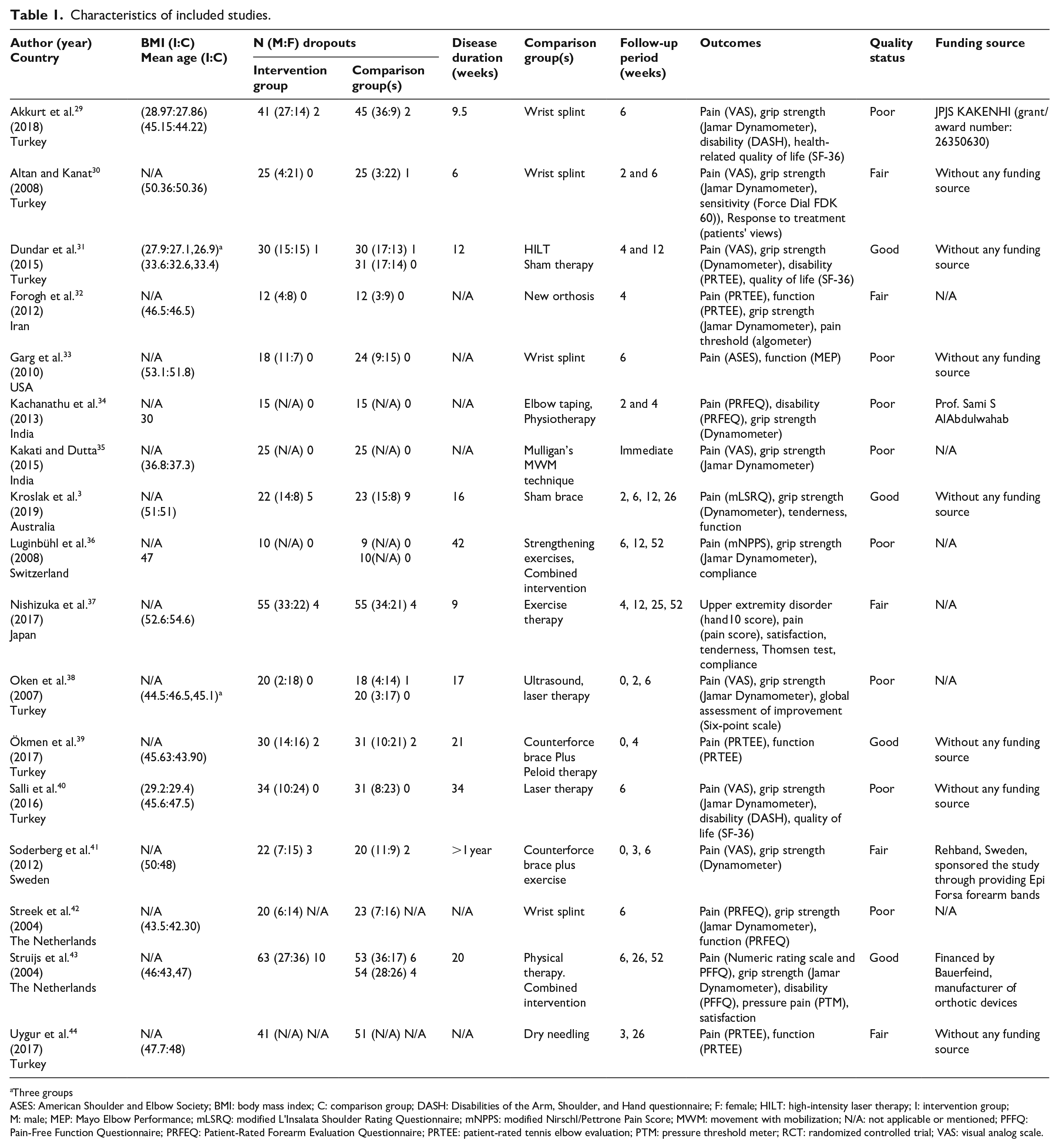
Characteristics of the included studies are outlined in Table 1. A total of 1145 subjects participated in the included studies, and 1086 (94.8%) subjects completed the trials. All of the included trials were parallel-design, and four trials31,36,38,43 had three groups.
Characteristics of included studies.
Three groups
ASES: American Shoulder and Elbow Society; BMI: body mass index; C: comparison group; DASH: Disabilities of the Arm, Shoulder, and Hand questionnaire; F: female; HILT: high-intensity laser therapy; I: intervention group; M: male; MEP: Mayo Elbow Performance; mLSRQ: modified L’Insalata Shoulder Rating Questionnaire; mNPPS: modified Nirschl/Pettrone Pain Score; MWM: movement with mobilization; N/A: not applicable or mentioned; PFFQ: Pain-Free Function Questionnaire; PRFEQ: Patient-Rated Forearm Evaluation Questionnaire; PRTEE: patient-rated tennis elbow evaluation; PTM: pressure threshold meter; RCT: randomized controlled trial; VAS: visual analog scale.
Risk of bias assessment
The risk of bias assessment is presented in Supplemental Figure 1. Most of the included studies considered randomization criteria, but only some of them3,31,34,37,39–41,44 described clearly the random sequence generation process. Furthermore, concealment of allocation was reported in only some trials.3,32,37,39,41–44 Disregarding these items can lead to selection biases and influence the internal and external validity of findings. 45 With respect to the third item, blinding of the outcome assessment, eight studies3,30–32,38,39,43,44 were judged as having a low risk of bias. Only six studies30,31,37,39,41,43 had a low risk of bias for the incomplete outcome data item. Ignoring this item results in attrition bias. According to the selective reporting of outcomes, all included studies had a low risk of bias. Finally, almost all of the studies had a low or unclear risk of bias regarding whether the groups were similar at baseline for the most important prognostic indicators, only one RCT was assessed as having a high risk of bias. 44 Overall, the quality of four studies3,31,39,43 was considered “good,” five studies30,32,37,41,44 were considered “fair,” and eight studies29,33–36,38,40,42 were considered “poor.” Supplemental Figure 2 presents the percentage of reviewers’ judgments for each risk of bias item. Information on funding source was identified where possible for included studies (see Table 1) to address agenda bias; however, this information was not reported in all studies.
Meta-analysis results of primary outcome: pain
Counterforce brace versus physiotherapy interventions; short-term follow-up (0–6 weeks)
The pooled estimate for six studies34,35,37,43,44,46 showed that a counterforce brace did not significantly relieve elbow pain versus physiotherapy interventions in subjects with LET (SMD −0.02 (95% CI −0.85 to 0.80) (Figure 2(a)). Statistical heterogeneity was high among the six studies (Heterogeneity χ2 = 69.36 (p < 0.001) I2 = 92.8%). Regarding the included trials in this category, the major limitation was small sample size leading to under-powering of the results.
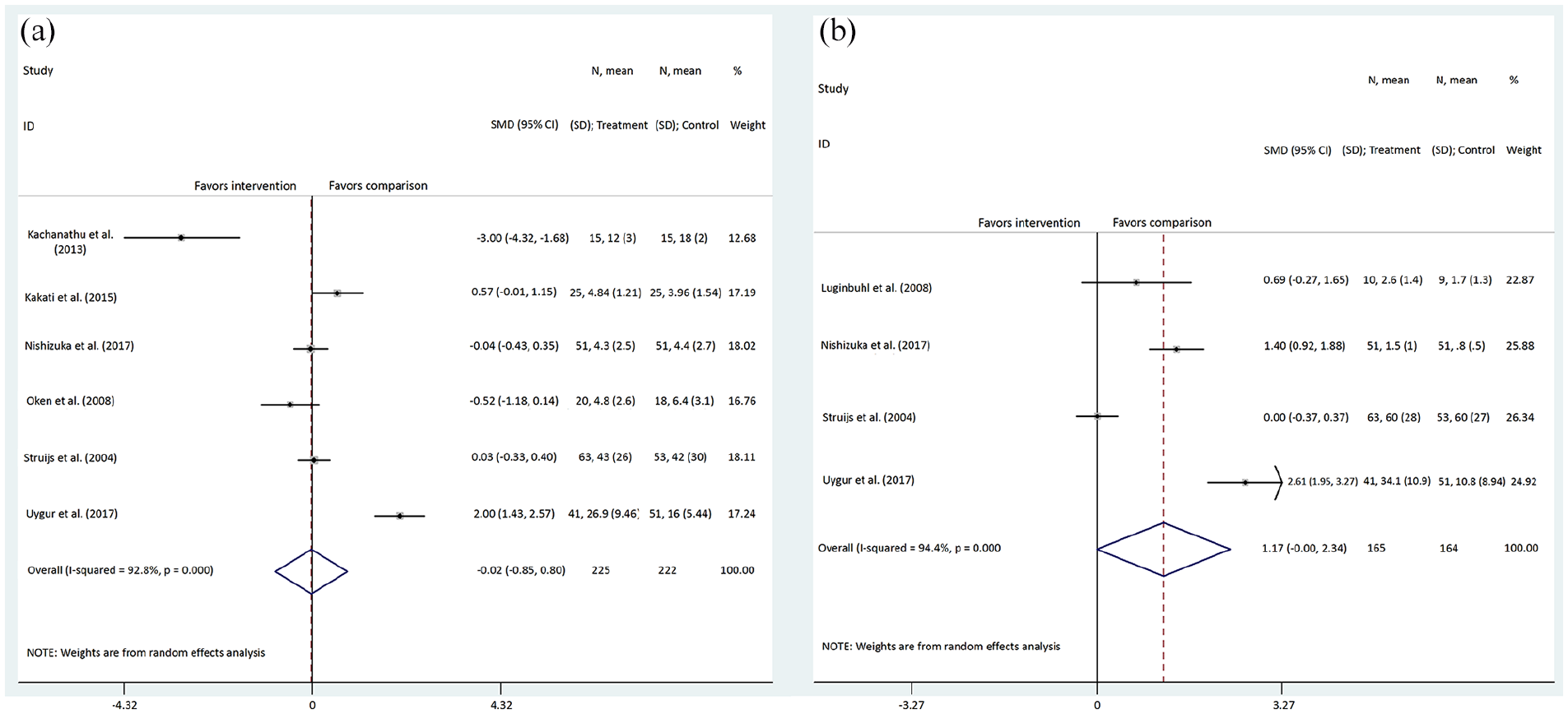
Forest plot comparing counterforce brace to physiotherapy interventions: (a) short-term follow-up and (b) long-term follow-up, primary outcome of pain.
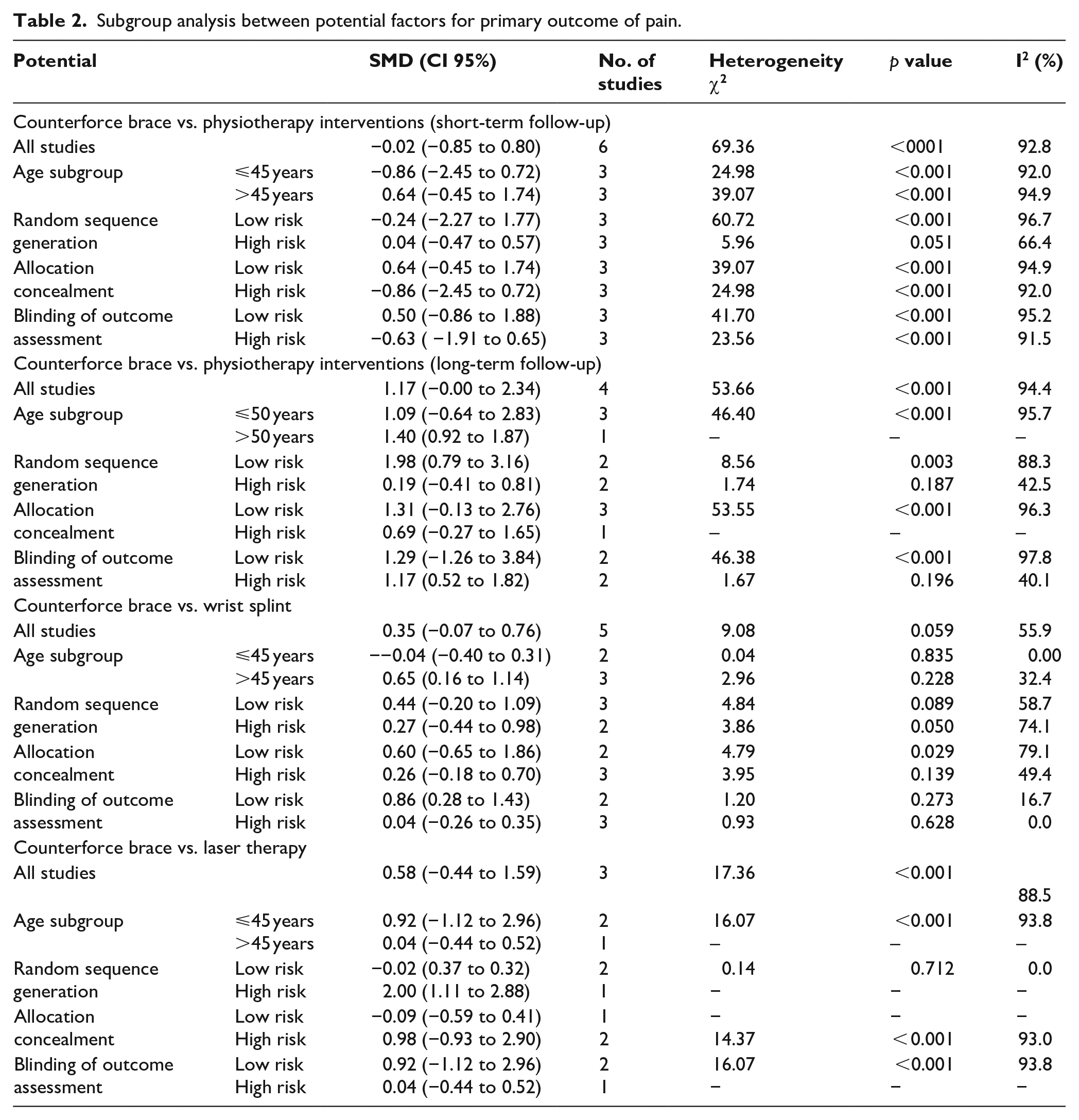
Supplemental Figure 3 shows the forest plots of the subgroup analysis of this category based on participants’ age (Supplemental Figure 3(a)), random sequence generation (Supplemental Figure 3(b)), allocation concealment (Supplemental Figure 3(c)), and blinding of the outcome assessment (Supplemental Figure 3(d)). Although the statistical heterogeneity results were not substantially different from the overall findings, pooled estimates were slightly different (see Table 2). Age subgroup analysis showed superior clinical effects of a counterforce brace on pain in subjects 45 years or younger (SMD −0.86; 95% CI −2.45 to 0.72). However, based on other factors, only high-risk bias trials showed better effects of a counterforce brace, which may reflect the impact of selection and detection bias.
Subgroup analysis between potential factors for primary outcome of pain.
Counterforce brace versus physiotherapy interventions; long-term follow-up (12–52 weeks)
The pooled estimate from four included studies36,37,43,44 revealed that other physiotherapy interventions in comparison with a counterforce brace decreased pain scores clinically (SMD 1.17; 95% CI −0.00 to 2.34), with significant statistical heterogeneity among the four trials (heterogeneity χ2 = 53.66 (p < 0.001) I2 = 94.4%). Body weight is shown by the forest plot in Figure 2(b). Although three studies36,37,44 showed that physiotherapy interventions had considerable effects on pain reduction, Struijs et al. 43 concluded that there was no difference between the two interventions, counterforce brace versus ultrasound, on pain at long-term follow-up (SMD 0.00; 95% CI −0.37 to 0.37). However, this comparison had limited studies with small samples resulting in inconclusive findings.
In the majority of subgroup analyses, there was no significant difference between the subsets of eligible studies when considering participants’ age, random sequence generation, allocation concealment, or blinding of outcome assessment (Table 2). Supplemental Figure 4 shows forest plots for these subgroup analyses.
Counterforce brace versus wrist splint
Five trials29,30,32,33,42 were included in this comparison. The meta-analysis (Figure 3(a)) showed a small-to-moderate improvement in favor of the wrist splint group on pain scores (SMD 0.35; 95% CI −0.07 to 0.76) with moderate statistical heterogeneity (heterogeneity χ2 = 9.08 (p = 0.059) I2 = 55.9%). However, only Akkurt et al. 29 showed a small improvement in favor of a counterforce brace group at six weeks (SMD −0.07; 95% CI −0.50 to 0.36). The trial by Forogh et al. 32 used a new orthosis with a covered forearm in the comparison group. Although the sample size in each group was very small (n = 10), the SMD was clinically and statistically significant in favor of the new orthosis group (SMD 1.30; 95% CI: 0.33 to 2.27). Based on available data, the subgroup analysis was used to find the source of heterogeneity (Supplemental Figure 5). The subgroup analysis by participants’ mean age (Supplemental Figure 5(a)) showed that the pooled effect size was in favor of the counterforce brace group in subjects 45 years or younger (SMD −0.04; 95% CI −0.40 to 0.31) with low statistical heterogeneity (heterogeneity χ2 = 0.04 (p = 0.835) I2 = 0.00%). Subgroup analysis among subjects >45 years was in favor of the wrist splint group (SMD 0.65; 95% CI 0.16 to 1.14) with moderate statistical heterogeneity (heterogeneity χ2 = 2.96 (p = 0.228) I2 = 32.4%). Table 2 outlines other subgroup analyses for this comparison.
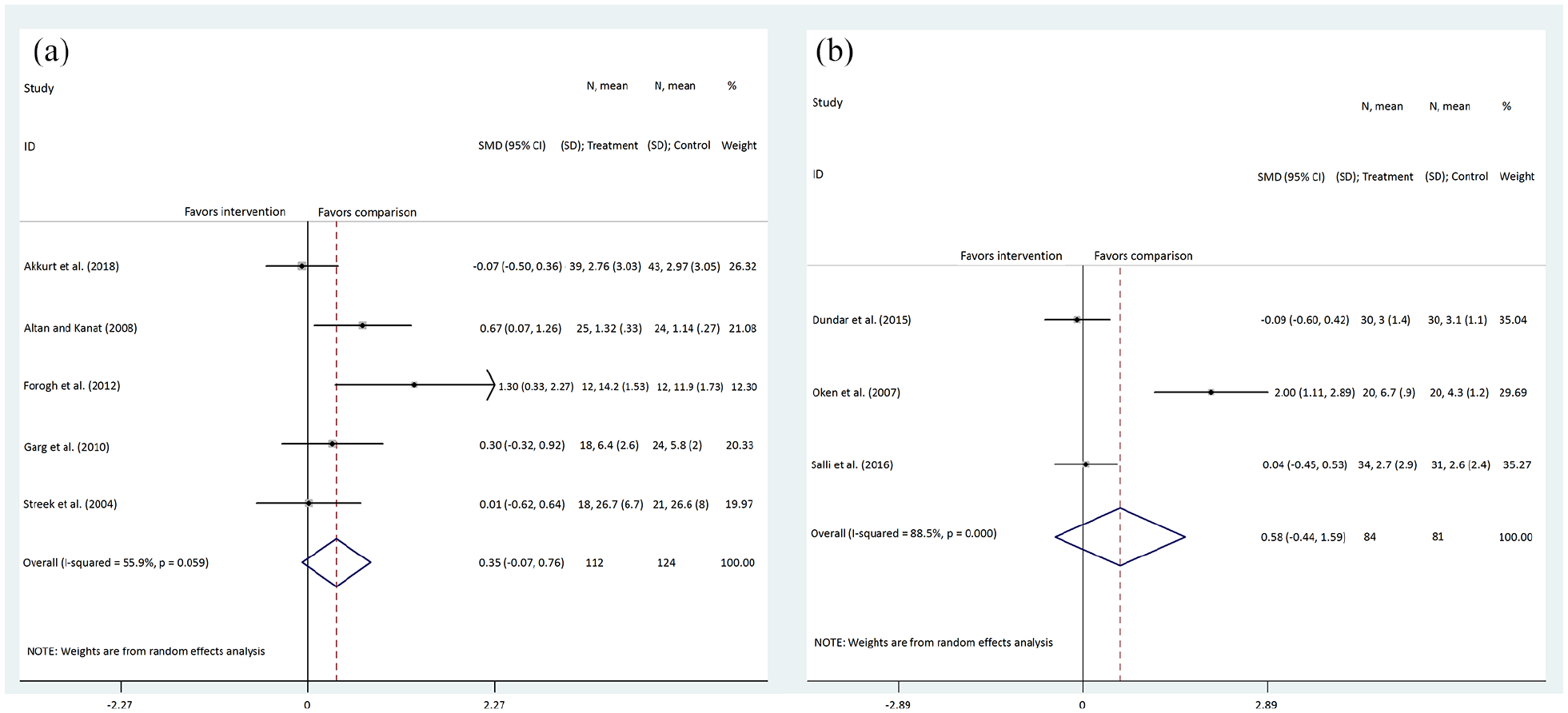
Forest plot comparing (a) counterforce brace to wrist splint and (b) counterforce brace to laser therapy, primary outcome of pain.
Counterforce brace versus laser therapy
Three studies31,38,40 showed a moderate improvement in favor of the laser therapy group (SMD 0.58; 95% CI −0.44 to 1.59), although between-study heterogeneity was significant (heterogeneity χ2 = 17.36 (p < 0.001) I2 = 88.5%) (Figure 3(b)). To investigate potential factors for heterogeneity, subgroup analyses were conducted (Table 2 and Supplemental Figure 6). Altogether, limited studies with small samples led to unreliable findings for this comparison.
Meta-analysis results of secondary outcome: grip strength
Counterforce brace versus physiotherapy interventions
Grip strength was reported in five trials.34–36,38,43 The pooled SMD showed a small improvement in favor of the physiotherapy group (SMD −0.12; 95% CI −0.43 to 0.20) with a low level of heterogeneity (heterogeneity χ2 = 5.51 (p = 0.239) I2 = 27.4%). Although three studies35,36,38 revealed moderate effectiveness in favor of physiotherapy, one study 43 showed a superior effect for the counterforce brace (SMD 0.21; 95% CI −0.15 to 0.58). Supplemental Figure 7(a) shows that all of the included studies have wide CIs reflective of their small sample size and insufficient statistical power. Supplemental Table 3 outlines the results of subgroup analyses, and Supplemental Figure 8 shows the body weights by forest plots.
Counterforce brace versus wrist splint
A comparison of grip strength between a counterforce brace and wrist splint was conducted in four studies29,30,32,42 (Supplemental Figure 7(b)). The pooled SMD demonstrated a small improvement in favor of the counterforce brace (SMD 0.37; 95% CI −0.12 to 0.86) but with large heterogeneity (heterogeneity χ2 = 7.74 (p = 0.052) I2 = 61.3%). All of the included studies favored the counterforce brace except one 32 that compared a new orthosis to a counterforce brace without covered forearm (SMD −0.53, 95% CI −1.36 to 0.30). Limited studies with low statistical power in this comparison resulted in inconclusive findings. The results of subgroup analyses are shown in Supplemental Figure 9.
Counterforce brace versus laser therapy
Three studies31,38,40 compared the effect of a counterforce brace to laser therapy on grip strength. The pooled estimation showed a moderate improvement in favor of laser therapy (SMD −0.48; 95% CI −1.46 to 0.50), although the between-study heterogeneity was considerable (heterogeneity χ2 = 16.69 (p < 0.001) I2 = 88.0%). For this comparison, a large and significant improvement in favor of laser therapy was shown by one of the studies 38 (SMD −1.79; 95% CI −2.64 to −0.95), while the other studies had contrary results (Supplemental Figure 10).
Sensitivity analysis
The results of sensitivity analysis based on the leave-one-out method showed that certain trials influenced the overall SMDs of the primary outcome (pain) over the short term, from −0.34 (95% CI −0.96 to 0.28) after removing the study by Uygur et al. 44 to 0.40 (95% CI −0.33 to 1.14) after removing the study by Kachanathu et al. 34 Furthermore, for the primary outcome over the long term, sensitivity analysis showed that certain trials also had a considerable effect on the pooled estimate. Supplemental Figures 11 and 12 show the results of sensitivity analysis for the primary and secondary outcome (grip strength), respectively.
Publication bias assessment
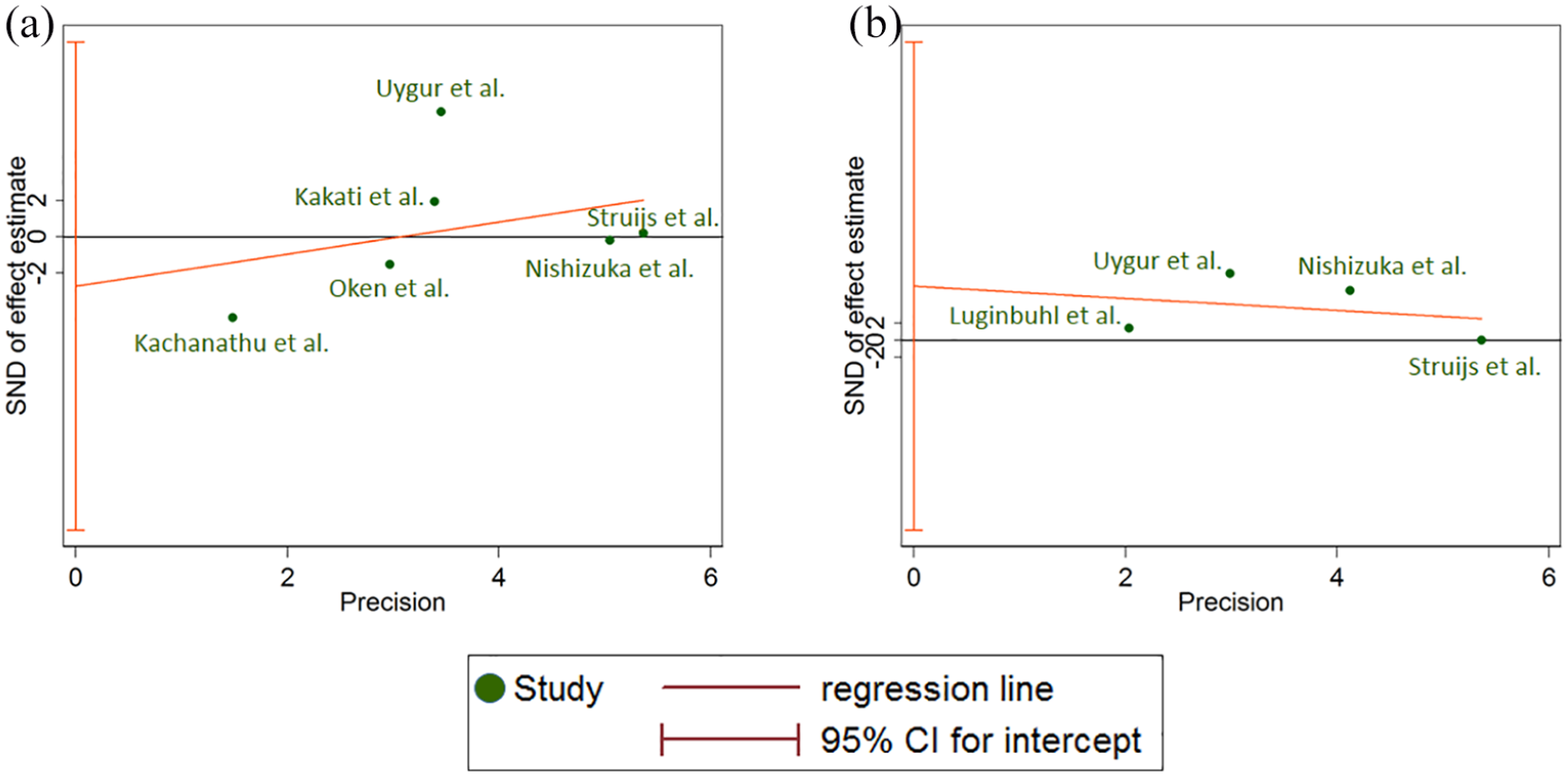
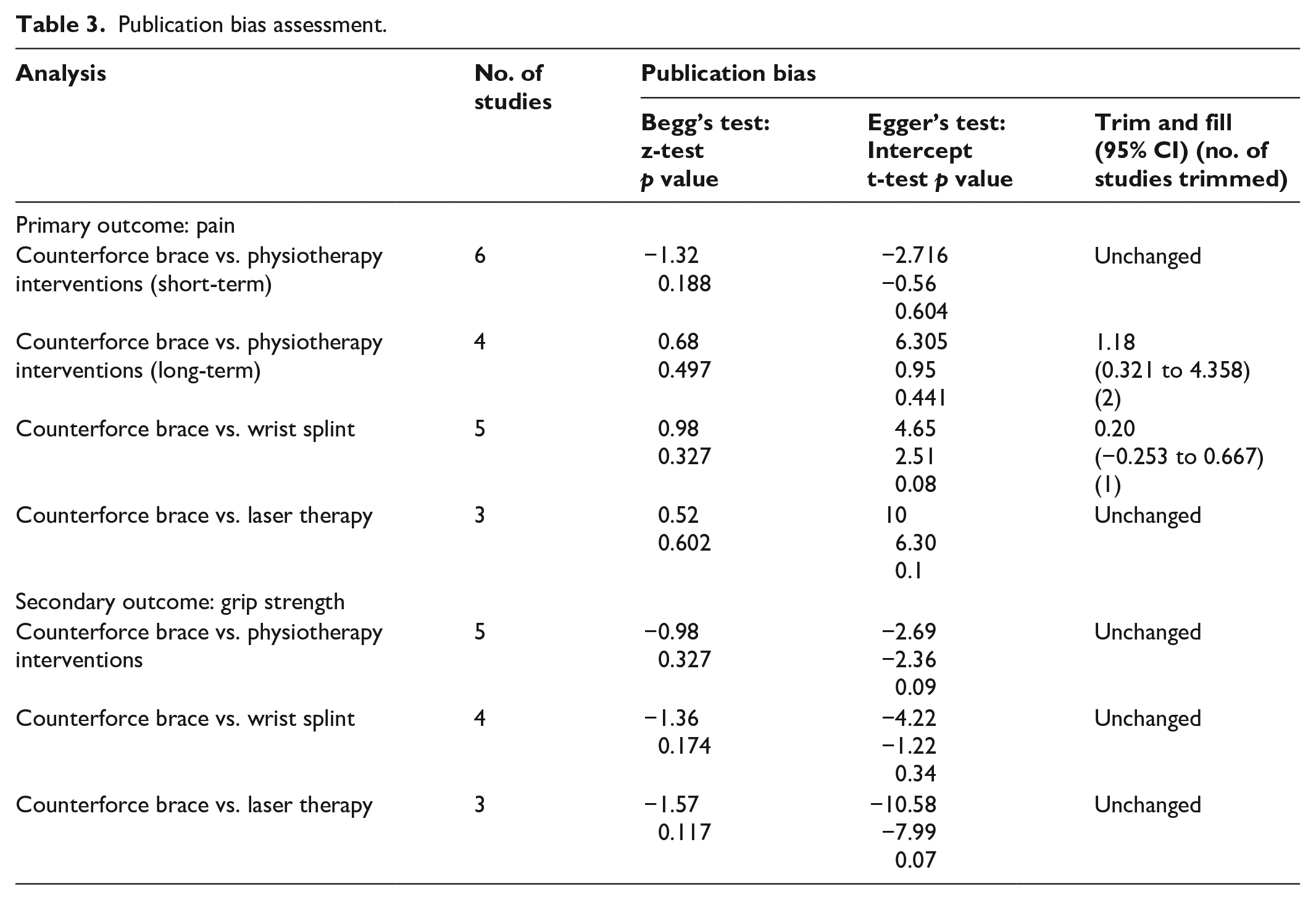
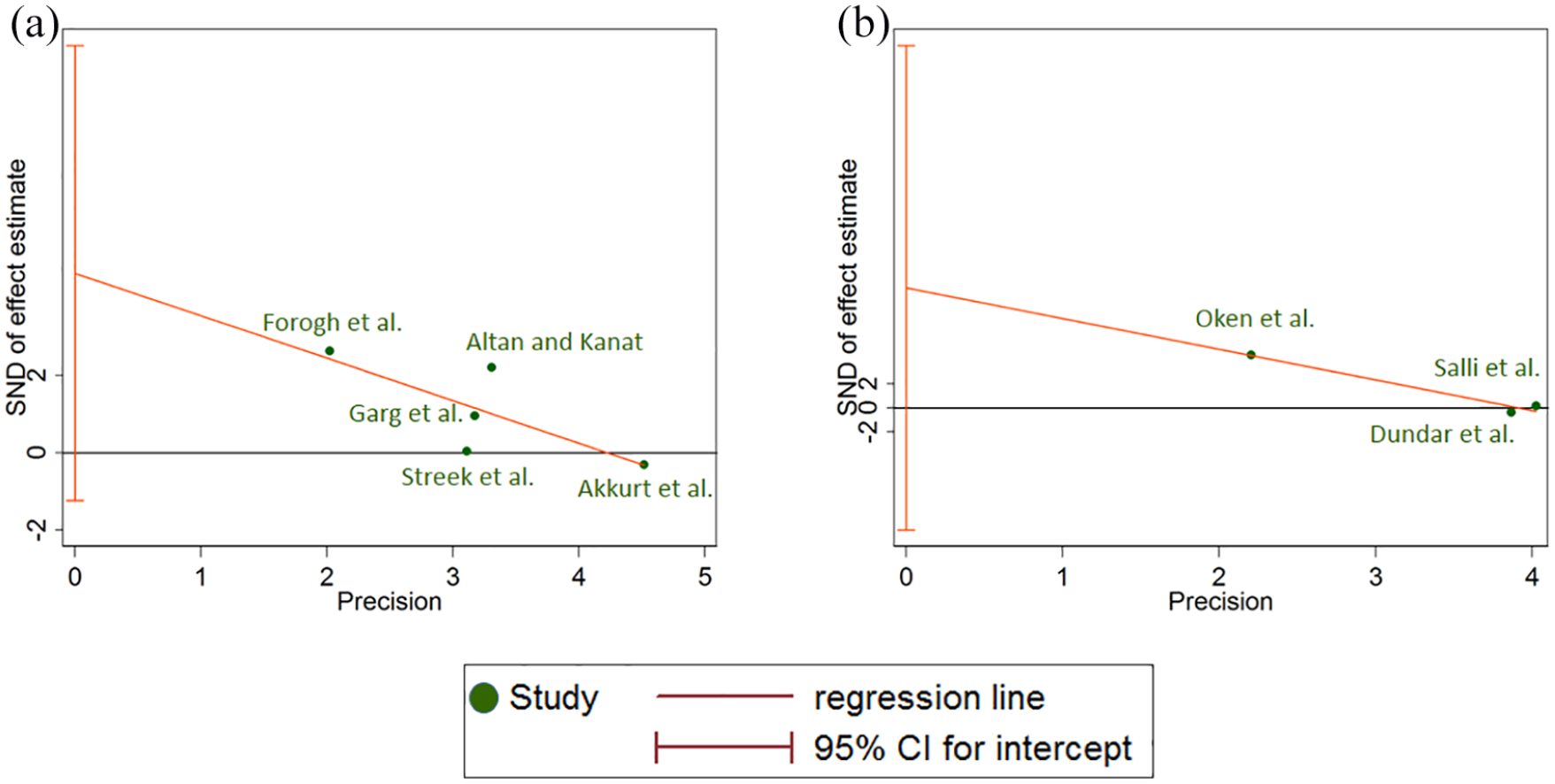
No potential publication bias was found for pain over short-term follow-up using Egger’s linear regression method (intercept = −2.716, standard error = 4.838, 95% CI −16.14 to 10.71, p = 0.604) and Egger’s graph (Figure 4(a)). The “trim and fill” method also did not find any missing studies. However, Egger’s linear regression (intercept = 6.305, standard error = 6.612, 95% CI −22.14 to 34.75, p = 0.441) showed that there is considerable publication bias for pain over long-term follow-up (Figure 4(b)). Using the “trim and fill” method, two potentially missing studies were identified in this meta-analysis. Inclusion for missing publications led to an adjusted SMD that was unchanged (Table 3). Egger’s linear regression also detected a publication bias in the meta-analysis assessing the effect of counterforce brace versus wrist splint on pain (intercept = 4.656, standard error = 1.854, 95% CI −1.24 to 10.55, p = 0.087) (Figure 5(a)). The “trim and fill” method identified a missing study and, therefore, changed the pooled estimate (SMD 0.20; 95% CI −0.253 to 0.667). Although Egger’s linear regression showed a suspected publication bias for the fourth comparison, counterforce brace versus laser therapy (intercept = 4.656, standard error = 1.854, 95% CI −1.24 to 10.55, p = 0.087), the “trim and fill” method did not identify any missing study for this comparison with limited trials (Figure 5(b)). Table 3 and Supplemental Figure 13 show the results of the publication bias assessment for the secondary outcome.
Egger’s graphs for primary outcome of pain: (a) counterforce brace vs. physiotherapy interventions, short-term follow-up and (b) counterforce brace vs. physiotherapy interventions, long-term follow-up.
Publication bias assessment.
Egger’s graphs for primary outcome of pain: (a) counterforce brace vs. wrist splint and (b) counterforce brace vs. laser therapy.
“Trim and fill” plots for pain and grip strength are shown in Supplemental Figures 14 and 15, respectively.
Quality of evidence
Table 4 shows the GRADE evidence profile. The quality of evidence was evaluated as low and very low in both of the outcomes because of limited sample size, high level of statistical heterogeneity, publication bias, and small effect sizes.
GRADE evidence profile.
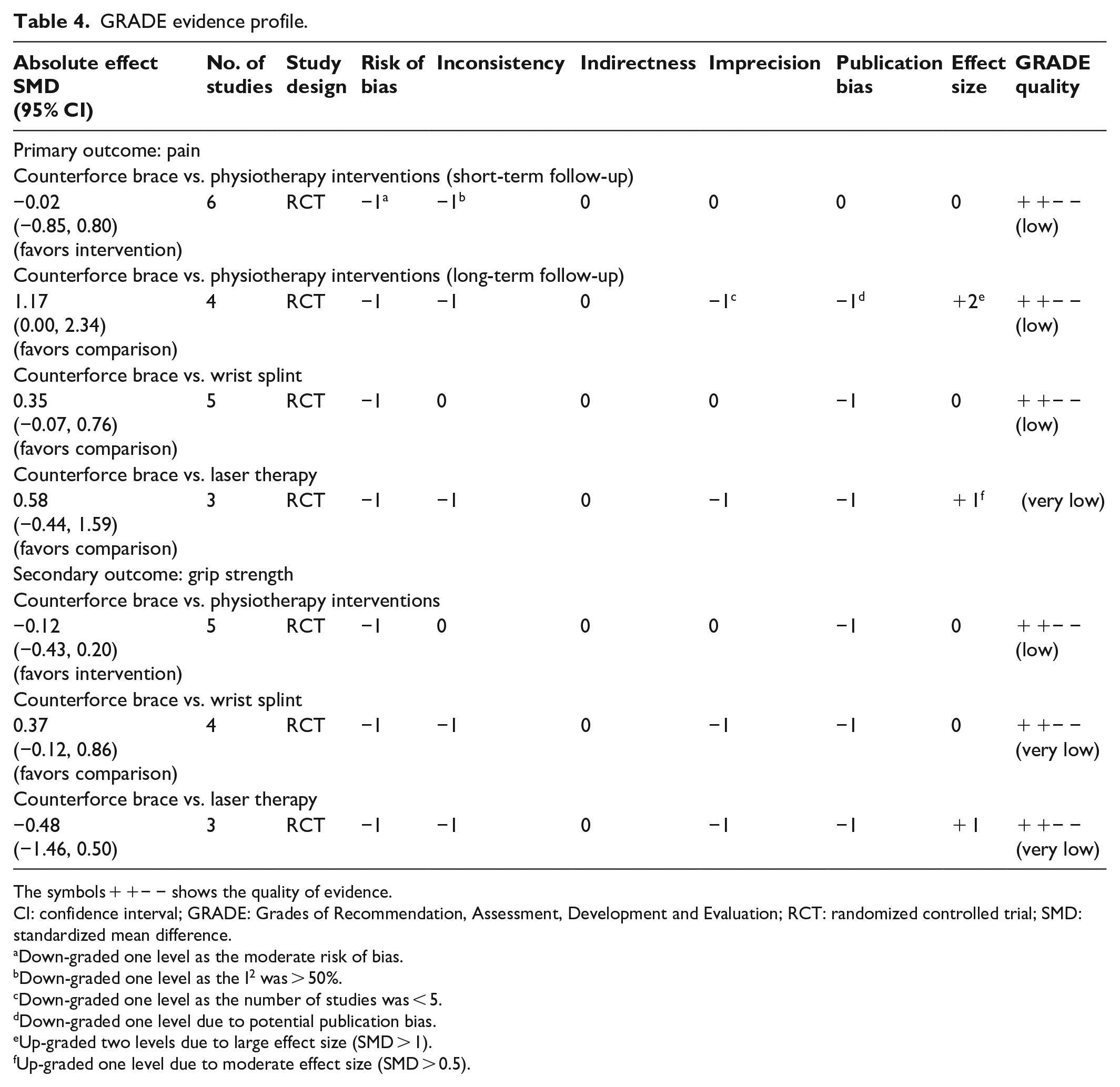
The symbols + +− − shows the quality of evidence.
CI: confidence interval; GRADE: Grades of Recommendation, Assessment, Development and Evaluation; RCT: randomized controlled trial; SMD: standardized mean difference.
Down-graded one level as the moderate risk of bias.
Down-graded one level as the I2 was > 50%.
Down-graded one level as the number of studies was < 5.
Down-graded one level due to potential publication bias.
Up-graded two levels due to large effect size (SMD > 1).
Up-graded one level due to moderate effect size (SMD > 0.5).
Discussion
To our knowledge, this is the first, comprehensive, systematic review and meta-analysis about the effects of a counterforce brace on pain and grip strength in subjects with LET. The results of our review suggest that use of a counterforce bracing compared to physiotherapy interventions did not demonstrate any superior effect on pain scores over the short term. However, physiotherapy interventions compared to counterforce bracing showed improvements in both pain and grip strength over the long term. A comparison of a wrist splint to a counterforce brace showed that improvements in pain favored the wrist splint and improvements in grip strength favored the counterforce brace. Our review also indicated that the quality of evidence was low and very low for most of the comparisons, due to high risk of bias, statistical heterogeneity, and publication bias.
Effects on pain
Counterforce braces may have mechanical 47 and neuromuscular effects 48 on elbow proprioception. Since motor control is reduced in older adults, 49 it is not surprising that our review suggested that the effects of the brace decline with age. While this may be a notable finding, due to the limited number of trials in each subgroup, it should be considered with caution. Counterforce braces prevent extensor muscle expansion, creating a new extensor origin and giving the soft tissue time to heal.8,50 It is possible that the better effect of the counterforce brace on pain in younger adults be the result of better remodeling capability of their musculoskeletal system in comparison to older adults. However, the effect of potential confounding variables like chronicity, the extent of intrasubstance damage, the severity of pain, and the extent of pressure on the tendon from the counterforce cuff should not be underestimated. For example, although theoretical, for a counterforce brace to work based on the new origin theory, 51 a snug enough strap must be provided, which was not measured or reported in the reviewed studies. A previous study reported a positive correlation between strap tension of the counterforce brace and pain. 52 By comparison, physiotherapy modalities theoretically work based on mechanisms of action like increased blood flow, softening scar tissue, and maintaining mobility within soft tissue. 53 Therefore, physiotherapy modalities may be a more effective mechanism for healing compared to counterforce braces. It is possible that the combined effect of physiotherapy and a counterforce brace may be worth consideration. Regardless, according to GRADE findings, quality of evidence was low to very low; therefore, conducting high-quality studies is necessary to arrive at more conclusive results. In addition, economic evaluation studies (cost-effectiveness, cost–utility, and cost–benefit analyses) should be undertaken to help health insurers and health policy-makers to determine the most cost-effective intervention. 53
Effects on grip strength
This review included trials evaluating the effects of counterforce braces compared to physiotherapy interventions on grip strength as a secondary outcome. The pooled estimate showed a small and nonsignificant improvement in grip strength favoring physiotherapy interventions. Although the between-study heterogeneity was low, wide CIs around the point estimates did not engender confidence in the robustness of the findings. GRADE assessments were low and very low for this outcome. Thus, future trials should consider the MCID criteria to calculate a sufficient sample size to arrive at more conclusive results.
Study limitations
This review had a few limitations. First, some of the comparisons and subgroups included a limited number of studies with high levels of statistical heterogeneity. Second, most of the included studies had low methodological quality due to the inability to blind completely. Third, due to a lack of data in most of the included studies, we could not consider other potential confounding factors such as body mass index (BMI), duration of disease, and physical activities.
Conclusion
Despite the limitations of this systematic review and meta-analysis, the results indicated that physiotherapy interventions compared to counterforce braces may have better effects, especially over the long term. However, counterforce braces may have better effects on pain in younger people (<45 years old) over the short term (<6 weeks). Furthermore, counterforce braces were slightly superior to wrist splints in grip strength improvement.
Supplemental Material
10.1177_0309364620930618_Supplemental_material – Supplemental material for The effects of counterforce brace on pain in subjects with lateral elbow tendinopathy: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, 10.1177_0309364620930618_Supplemental_material for The effects of counterforce brace on pain in subjects with lateral elbow tendinopathy: A systematic review and meta-analysis of randomized controlled trials by Saeed Shahabi, Kamran Bagheri Lankarani, Seyed Taghi Heydari, Maryam Jalali, Sulmaz Ghahramani, Mojtaba Kamyab, Reza Tabrizi and Mostafa Hosseinabadi in Prosthetics and Orthotics International
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Trial registration
The protocol of this study has been registered in the PROSPERO database (registration number: CRD42019133024).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.