
Abstract
Introduction
Patella fracture fixations were traditionally done using metal tension band wiring techniques. However, complications associated with metallic implants causing soft tissue irritation are not infrequent. Since 1998, there have been emerging case reports and series reporting the use of non-metallic implants, such as braided sutures, in the fixation of patella fractures 3. However, there is a limited clinical study on a direct comparison between metal and suture fixation in patella fractures. The aim of this study is to evaluate the outcome of all-suture fixation in patella fractures and to compare all-suture and metal fixation in mid-pole fractures.
Materials and method
A total number of 50 patients with operated fracture patella were retrospectively reviewed in a 2.5-year period. Primary outcomes included operation time, time for fracture union and postoperative knee function. Secondary outcomes include complications, need for secondary operations due to prominent implants, infection or loss of fixation.
Results
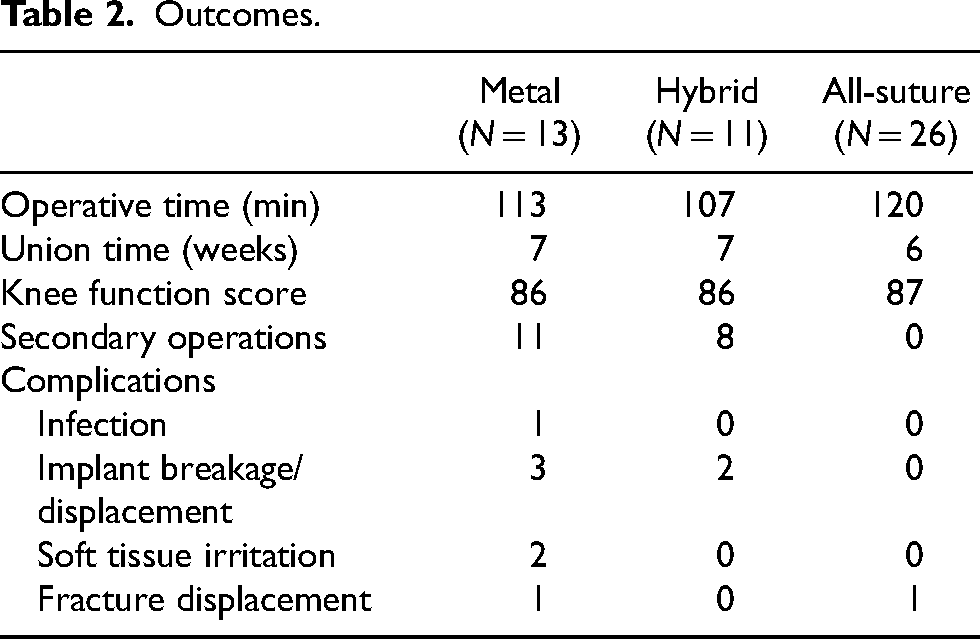
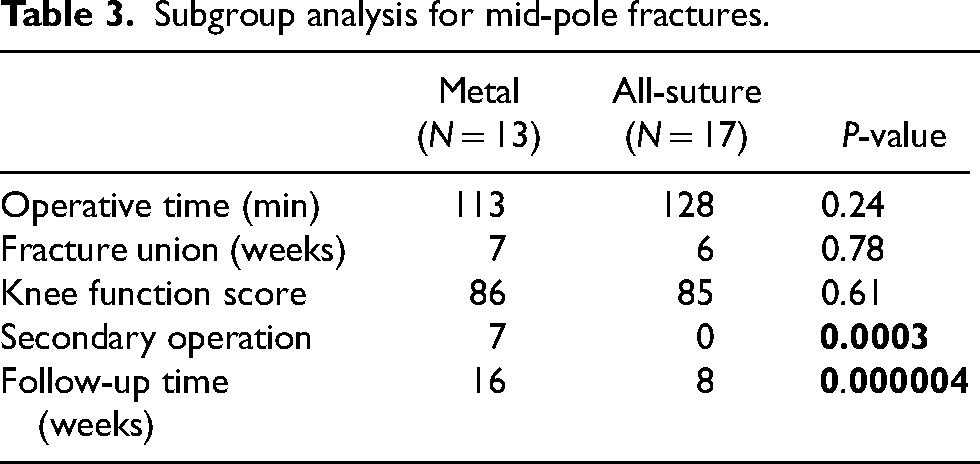
There was no statistically significant difference concerning time for fracture union, operation time and postoperative functional knee score between the three fixation methods. The rate of secondary operations was higher in the hybrid group (7 out of 11, 63.6%) and metal group (7 out of 13, 53.8%), and was lowest in an all-suture group (0 out of 28, 0%). Metal implant breakage and soft tissue irritation were the main reasons for secondary operations, which was significantly lower in the all-suture group (p < 0.0003). Subgroup analysis for mid-pole patella fractures showed similar results in which all primary outcomes showed no statistically significant difference, while the need for secondary operations was higher in the metal group (p < 0.003).
Conclusion
All-suture fixation for patella fractures is a feasible option not limited to distal pole fractures. In our series, this technique achieved similar outcomes when compared with traditional metal implants, with lower rates of secondary operations, and could be safely employed in mid-pole fractures as well.
Introduction
In healthy individuals, displaced patella fracture with a disrupted extensor mechanism is indicated for operative treatment. 1 The aims of surgery are the restoration of the articular surface, stable fixation to withstand the strong tensile force on the patella, and preservation of the extensor mechanism for early mobilisation. The most widely used method traditionally is the tension band wiring technique with stainless steel wires. However, the use of metallic implants for patella fracture is commonly associated with prominent hardware causing discomfort or skin impingement, hardware breakage or migration which requires another operation for removal. 2 The rate of removal of metal implants was reported to be as high as 40%. 3 Follow-up is often needed even after rehabilitation is completed to detect potential hardware problems. To remove the hardware, patients often needed to undergo another elective surgery under spinal or general anaesthesia, and sometimes a separate wound would be opened. There could be other problems associated with it, such as delayed wound healing, postoperative adhesions, knee stiffness, and prolonged work disability.4,5
To avoid frequent hardware complications and discomfort, over the past decade, there has been an increasing usage of non-metallic materials with modified methods of fixation. One of the techniques is based purely on braided sutures. 6 Non-absorbable braided sutures, for example, FiberWires, are shown to have comparable strength, if not superior, to stainless steel wires in both in vivo and cadaveric studies.7,8 It is a biomechanically suitable alternative for the fixation of patella fractures while avoiding metallic hardware complications. 9
Our centre has been operating on patella fractures with traditional metallic implants, all-suture and a hybrid of both methods based on fracture configuration. In view of emerging evidence on stronger suture material, reduced rate of implant-related complications and lower need for removal of implants, we had been switching from metal to all-suture techniques in fixing the majority of patella fracture cases in recent years, including mid-pole fractures.
We have retrospectively reviewed 50 cases of operated patella fractures in a 30-month period. A subgroup analysis to compare all-suture and metal fixation on mid-pole patella fractures was included.
Materials and methods
This is a retrospective review of all operated adult fracture patella cases in our centre from January 2020 to June 2022. The cases were identified through Clinical Data Analysis and Reporting System and Operating Theatre Management System. These were centralised hospital systems for charting all indexed operative cases.
Inclusion and exclusion criteria
All included cases were acute patella fractures with loss of extensor mechanism, in which the patients were physiologically fit to undergo operations for open reduction and internal fixation.
Patients with polytrauma, concomitant ipsilateral lower limb trauma, and previous ipsilateral knee surgery or revision cases were excluded.
Surgical techniques
Using an anterior midline approach, a fracture was exposed from the superior pole of the patella to the patella tendon. A full-thickness skin flap was elevated. The fracture was identified, with the hematoma cleared and irrigated thoroughly. The fracture was temporarily stabilised with bone clamps or K-wires.
In the metal group, fractures were fixed with the tension-band principle using 18G stainless steel wires. A cerclage and a figure-of-8 wire were placed around the patella, with the addition of intraosseous K-wires if needed.
In the hybrid method, which was used mainly in distal pole fractures, four-stranded Krachow sutures (2 runs of double loop, FiberWire#2) were applied. Three longitudinal transosseous tunnels were drilled over the proximal fragment. The sutures were brought through the intraosseous tunnel and tied over the superior pole of the patella. Protective figure-of-eight 18G stainless steel wire was placed through the tibial tuberosity and superior pole of the patella with the knee flexed at 90°.
In the all-suture technique, the suture we employed was FiberWire#2. Four-stranded Krachow sutures (2 runs of the double loop) were applied to the patella tendon. The sutures were brought through three longitudinal transosseous tunnels over the proximal fragment. The lateral and medial strands of sutures were brought through the lateral and medial bone tunnels respectively, while the middle two strands of sutures were brought through the middle bone tunnel. Each loop of suture was tightened with knots placed at the superior pole of the patella, as close to the patella bone as possible. Another FiberWire#2 was placed in a protective figure-of-8 configuration through tibial tuberosity and the superior pole of the patella with the knee flexed at 90°. Additional peri-patellar cerclage and figure-of-8 sutures might be placed to enhance the stability of the construct.
Methods of fixation
Methods of fixation were determined by surgeons according to fracture configuration (Figure 1). Distal pole fractures were treated with either hybrid or all-suture, which involved transosseous sutures, with an addition of anterior figure-of-8 banding passing through tibial tuberosity and superior pole of the patella using metal or sutures. Simple transverse, mid-pole, stellate or comminute fractures included in this study were fixed with metal or all-suture techniques.
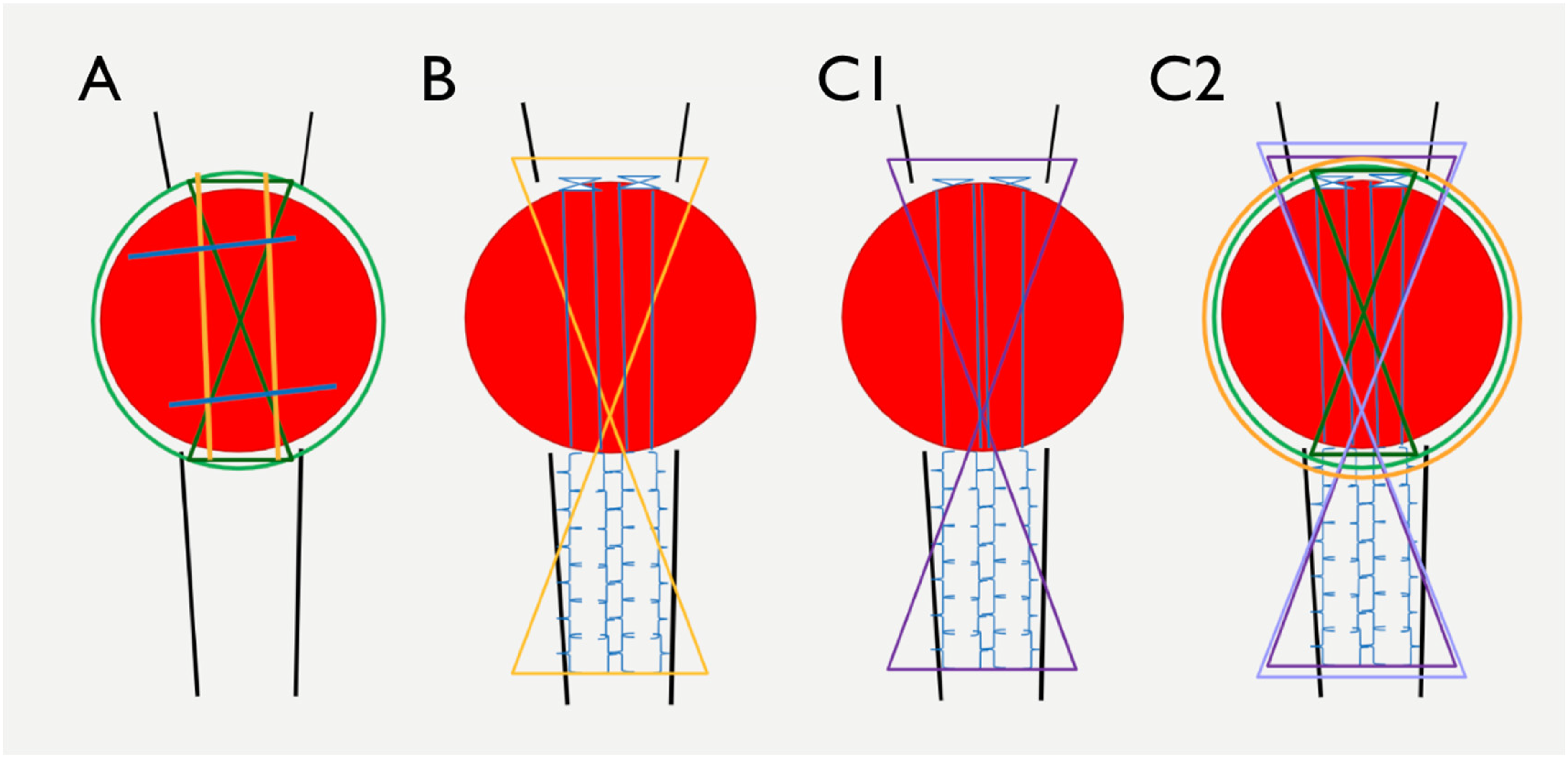
Schematic diagram of the three fixation methods. (A) Metal fixation. Peri-patellar cerclage and figure-of-8 wires with 18G stainless steel wire loops, addition of intra-osseous K-wires may be used. (B) Hybrid method. Four strands of Krackow sutures were placed at the patella tendon with FiberWire#2, followed by a protective figure-of-eight 18G metal wire passing through the tibial tuberosity and superior pole of the patella. (C1) Basic all-suture technique. Four strands of Krackow sutures are placed at the patella tendon, followed by a protective figure-of-eight suture passing through the tibial tuberosity and superior pole of the patella using FiberWire#2. (C2) Stability enhancement for all-suture technique. Addition of peri-patellar cerclage and figure-of-eight sutures with FiberWire#2.
Rehabilitation
Wound condition was monitored on day 1. Postoperative radiographs were taken (Figure 2). Patients were given a knee–extension brace for 2 weeks while allowing full-weight bearing walking. Isometric quadriceps muscle exercise was commenced. After a satisfactory level of ambulation and self-care was achieved, patients would be discharged from a hospital. From weeks 3–6, they were given a hinged knee brace with a gradual increase in the degree of flexion from 0° to 90°. They would be followed up at 3 weeks for assessment of wounds and fracture fixation. Knee braces were removed at 6 weeks. Patients were then followed up every 6–8 weeks for monitoring of fracture union and functional status.
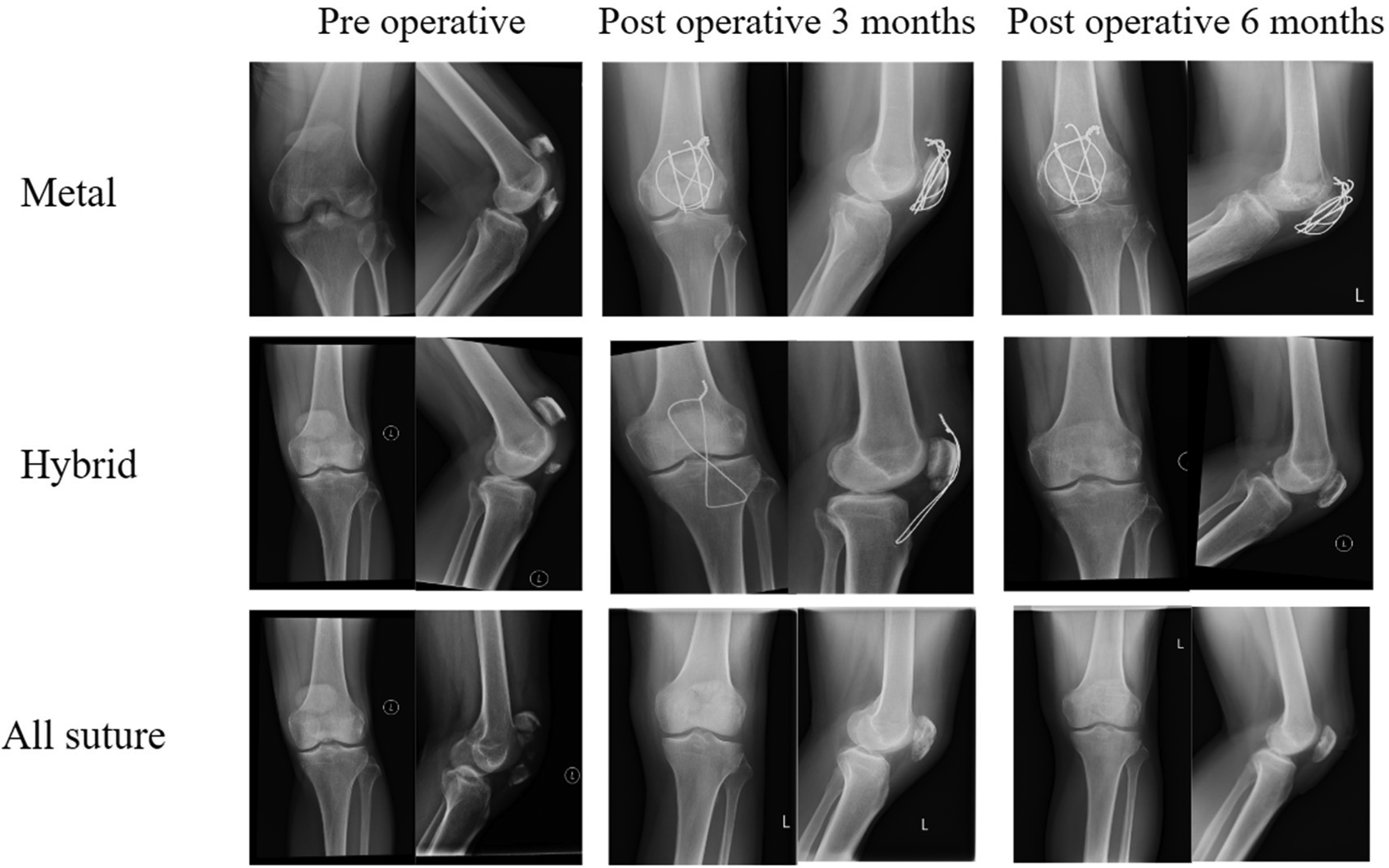
X-ray images of patella fixation. There were no quadriceps or patella tendon rupture, or loss of extensor mechanism observed. All fractures were healed. No fixation failure was evident. No cut-out of bone by sutures or wires was seen. No patella baja was demonstrated.
For patients with metal protective wire placed through the tibial tuberosity and superior pole of the patella in the hybrid group, elective removal of the protective wire was routinely arranged.
Data analysis
Analysis with statistical comparison was made with a one-tailed t-test with a significance threshold set at p < 0.05.
Ethics approval
The Research Ethics Committee of our hospital's cluster approved the conduct of this study (Ref.: KC/KE-22-0049/ER-4).
Outcome measures
Clinical data such as patients’ demographics, age, and surgical techniques were collected from the electronic patients’ records.
Primary outcome measures collected were operative time, time for fracture union, and knee function, which was quantified by Lysholm knee score.
Secondary outcomes included were occurrence of any postoperative complications such as infection, loss of fixation, prominent implants or breakage, soft tissue irritation, and if secondary operations were required. Elective removal of the implant was also considered a secondary operation.
Results
Two patients who were lost to follow-up at three months were excluded from the study. Two patients who received fixation methods other than those described above were also excluded. A total number of 50 cases were suitable for analysis (Figure 3).
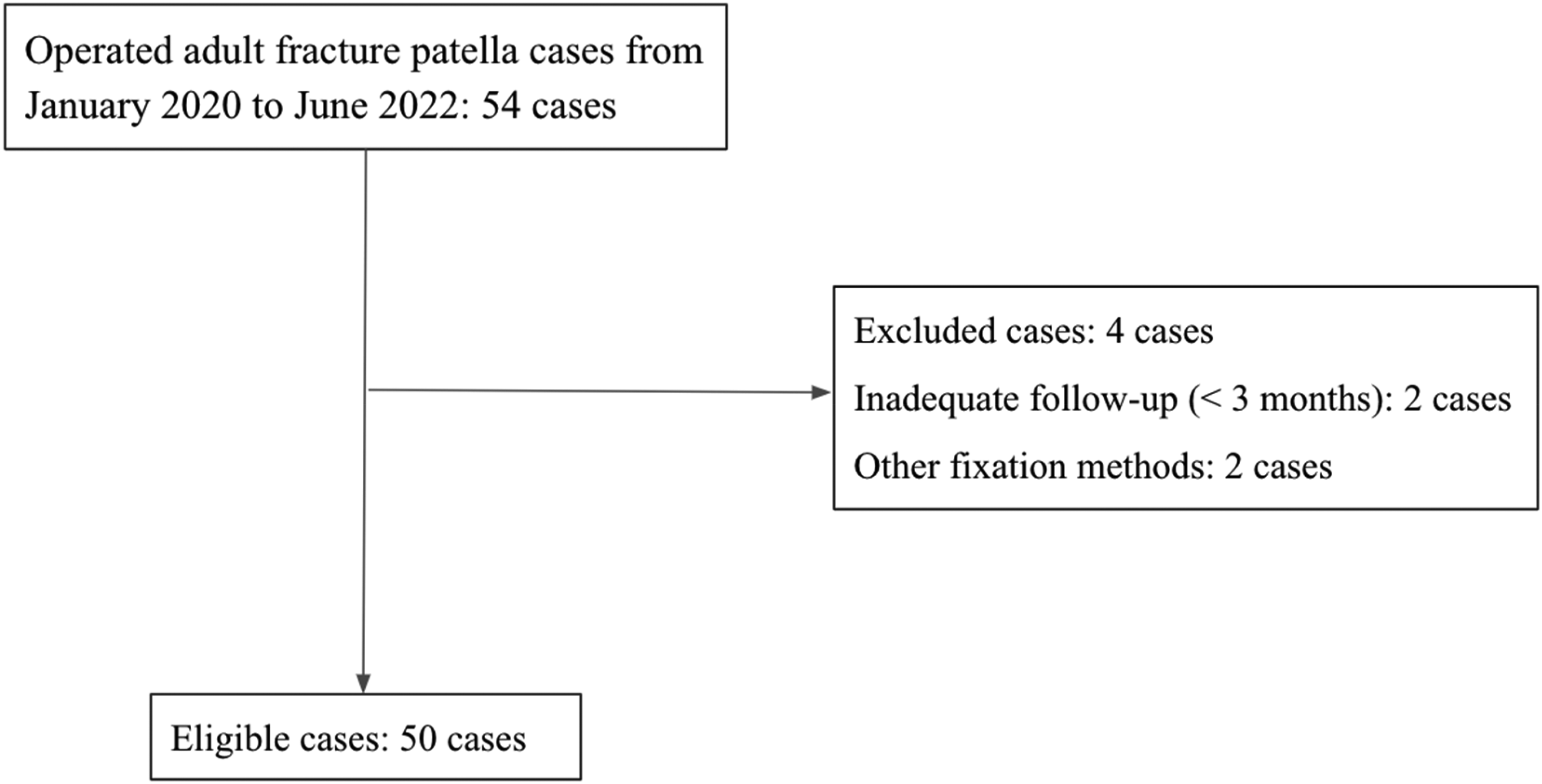
Eligible cases after exclusion.
Demographics
There were 17 male and 32 female patients of the total number of 50 cases (Table 1). One female patient has bilateral patella fractures. The average age was 62.4 years (19–82 years). The number of patients who received metal fixation, hybrid and all-suture are 13, 11 and 26, respectively. The average follow-up time was 13 months. For mid-pole fracture subgroup analysis, the number of cases receiving metal fixation and all-suture techniques was 13 and 17, respectively, with an average age of 63.3 years (45–88 years).
Demographics.
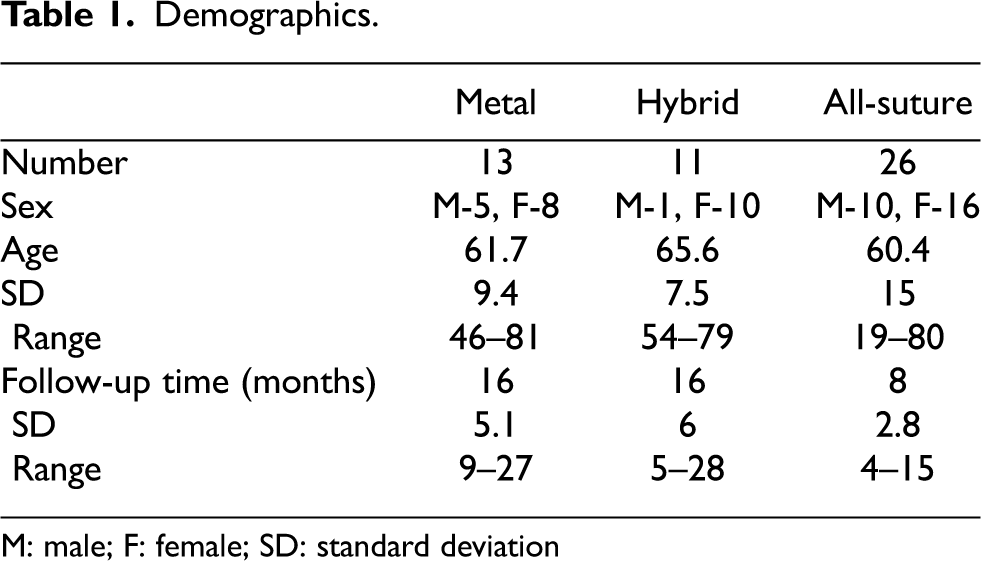
M: male; F: female; SD: standard deviation
Operative time and time for fracture union
The mean operative time for all-suture, metal and hybrid groups showed no statistical significance (p = 0.22–0.75). Moreover, no significant difference was observed between metal and all-suture groups for mid-pole fractures (p = 0.24). The mean time for fracture union for all-suture, metal and hybrid groups was 6 weeks, 7 weeks and 7 weeks, respectively. There were no cases of fracture non-union. Subgroup analysis for mid-pole patella fracture comparing all-suture and metal groups revealed that the time for fracture union was 6 and 7 weeks, respectively, and the difference was not shown to be significant (p = 0.78; Tables 2 and 3).
Outcomes.
Subgroup analysis for mid-pole fractures.
Knee function
The Lysholm knee score was utilised for objective measurement of knee function post-operatively. The scoring system takes account of the presence of knee pain, limping, swelling, locking, instability, the need for support during ambulation, ability to manage stairs and squatting. Out of a score of 100, eight questions concerning knee symptoms and ambulation status were included, where higher scores indicated a better knee function. Scores were categorised as excellent (95–100), good (84–94), fair (65–83) and poor (<65). Knee scores were comparable among all groups with mean scores of 87, 86 and 87 for all-suture, metal and hybrid groups, respectively. Subgroup analysis for mid-pole fractures also showed comparable results with a mean score of 85 in the all-suture group and 86 in the metal group (p = 0.61).
Implant complications and secondary operations
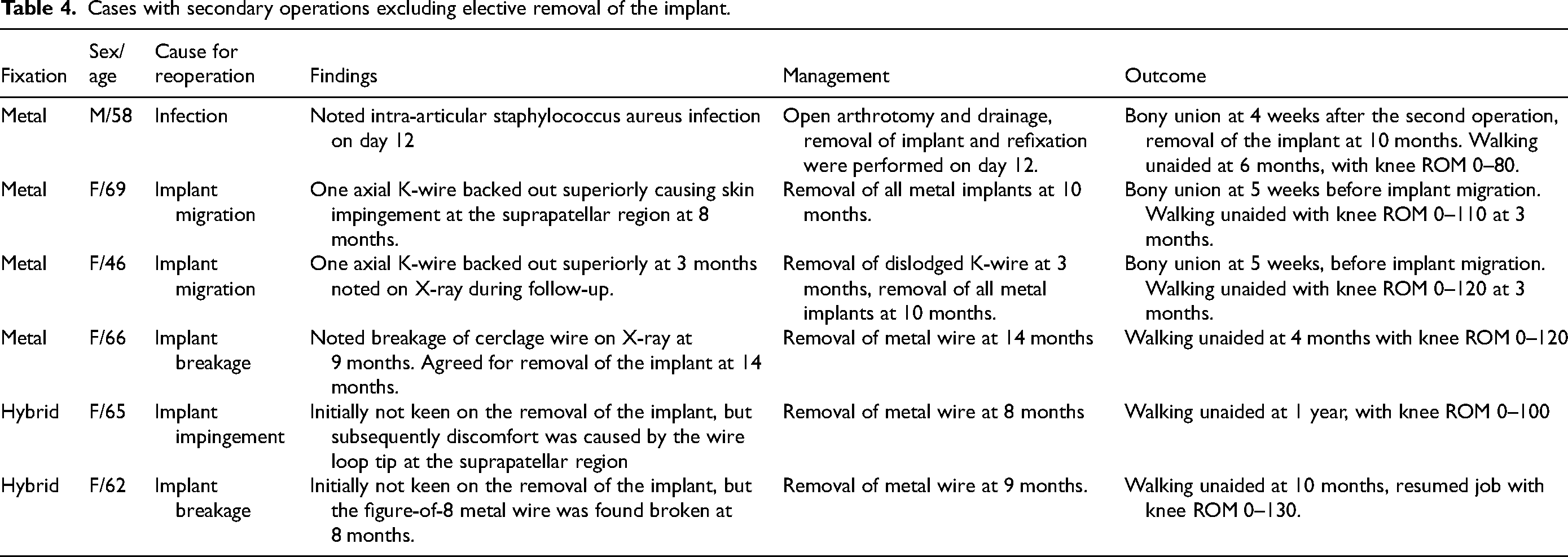
Soft tissue irritation by implants was found in two of the cases in the metal group, and both patients received secondary operations for the removal of implants. Skin impingement by wire at the upper lateral corner of the patella occurred in one case, while in the other case, an axial transosseous K-wire was dislodged superiorly causing impingement. Breakage of metal wires was noted in two cases in the hybrid group and one case in the metal group. Secondary surgeries for the removal of implants were done for eight patients in the hybrid group and 11 patients in the metal group. No implant or suture-related complications and secondary operations were found in the all-suture group (Table 4). The reasons for secondary operations were infection, implant breakage/displacement, soft tissue irritation and patient's request.
Cases with secondary operations excluding elective removal of the implant.
Infection
There was one case of infection in the metal group, which requires open arthrotomy and drainage on day 12. Implants were taken down for the prevention of biofilm. Thorough lavage of the joint and refixation with metal wires was performed. The fracture healed at 7 weeks and the patient was able to walk without aid eventually (Table 4).
Fracture displacement
In this series, no cases of fracture non-union or fixation failure requiring reoperation were found among all fixation methods. There were, however, two cases of initial fracture displacement, but eventually, both resulted in bony union and comparable functional outcomes. The extensor mechanisms for both cases were intact throughout. One of the cases was in the metal group, where a 3 mm anterior gapping of fracture was noted at postoperative 3 weeks. A bony union was observed without intervention. Another case was in the all-suture group, in which a 3 mm anterior gapping of fracture was noted at postoperative 10 weeks. An extension knee brace was prescribed and the bony union was observed afterwards.
Discussion
This study is the first local series on an all-suture transosseous technique with direct comparison to metal on mid-pole patella fractures alone. In our series, time for fracture union for all-suture and metal groups showed no statistical significance and was comparable to the literature. 10 Among cases in the all-suture group, no complications such as infection, irritation by sutures and revision were found. Knee function was also comparable for all-suture and metal groups.
The use of FiberWire in stabilising patella fractures was shown to be a feasible option in recent literature. 11 Although the loss of reduction was found in one case for all-suture fixation, no revision surgery was needed to achieve bony union. There was a significantly lower rate of hardware complications and secondary surgeries when compared with other fixation methods.10–12 Similar results were found in our study.
A common question regarding suture fixation is the biomechanical strength of sutures. Wright et al. 7 concluded that FiberWire#5, single or double-stranded, was more resistant than 18G stainless steel wires when used in simple transverse fractures with the same implant configuration in a biomechanical study. In our study, we extrapolated the results and used FiberWire#2, due to its availability in our centre, cost, and less degree of soft tissue irritation and knot prominence. FiberWire#2 and #5 differ in their diameter (three metrics and seven metrics), and therefore, our fixation was augmented by transosseous tunnels to achieve a stable fixation in different patterns of patella fractures. No fixation failure or patella baja was found in our series. The consideration of using double-stranded FiberWire#2 without transosseous tunnels could be the direction for our future clinical studies.
The mean follow-up time for the all-suture group was found to be 8 months, while that of the metal group was 16 months in the subgroup analysis. Patients in the metal group generally needed longer follow-up duration due to implant impingement causing soft tissue irritation, breakage and scheduled implant removal. In general, the need for serial radiological monitoring was observed to be higher in the metal group.
One of the strengths of this study is the analysis of a separate entity of mid-pole fractures, in contrast to other studies that included one general analysis for more heterogeneous fracture patterns, for example, a mixture of distal poles and mid-poles. We also documented the postoperative knee function with a validated functional scoring system, which offered a subjective assessment of our patient's knee function.
Limitations of this study include a relatively small sample size in a single centre, and being a retrospective review. Due to the switch of fixation method from metal to all-suture techniques, the follow-up time for the all-suture group was shorter. Potential complications for all-suture techniques might not be observed in this study due to the relatively short follow-up time in which suture material could also cause irritation, allergy and migration into the joint if broken. Future studies could be done to address the potential long-term complications for all-suture techniques. There could also be a potential information bias and inaccuracy of medical records. In addition, fracture patterns were never homogeneous. Even within the subgroup of mid-pole patella fractures, not all mid-pole fractures were identical. There were variations in fracture patterns which might result in a difference in surgical method and final outcomes. Rehabilitation protocol and the adherence of patients varied, which might affect end functional outcomes such as range of motion. Finally, time for the union was determined radiologically during follow-up, which was limited by how often radiographs were taken, that is, follow-up frequency.
Conclusion
To conclude, the all-suture transosseous tunnel method is a safe and effective technique for patella fracture fixation to achieve sufficient stable osteosynthesis, even for mid-pole patella fractures. In our series, all fractures using all-suture fixation healed without complications such as infection, symptomatic suture knots, soft tissue irritation, or revision surgery. The rate of secondary operations and follow-up time was demonstrated to be statistically less when compared with metal fixation in mid-pole fractures. The knee scores showed good results. The time to fracture union was 6 weeks. We could take this as a reference to further fine-tune future rehabilitation protocols for patella fractures fixed with this method. The all-suture technique should be considered a good alternative in treating not just a distal pole, but also mid-pole patella fractures.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.